
Abstract
Background and Aims:
Bariatric surgery is considered the only long-lasting treatment for morbid obesity. Techniques and procedures have changed dramatically. We report on some of the major changes in the field.
Materials and Methods:
We reviewed some of the major changes in trends in bariatric surgery based on some landmark paper published in the literature.
Results:
We identified three major phases in the evolution of bariatric surgery. The pioneer phase was mostly characterized by discovery of weight loss procedures serendipitously from procedures done for other purposes. The second phase can be identified with the advent of laparoscopic techniques. This is considered the phase of greatest expansion of bariatric surgery. The metabolic phase derives from the improved understanding of the mechanisms of actions of the bariatric operations at the hormonal and molecular level.
Conclusions:
Bariatric surgery has changed significantly over the years. The safety of the laparoscopic approach, along with the better understanding of the metabolic changes obtained postoperatively, has led to a more individualized approach and also an attempt to expand the indications for these procedures.
Introduction
It has been almost three decades since the National Institutes of Health (NIH) consensus conference has established that bariatric surgery is the only long-lasting treatment for morbid obesity (1). Since then, bariatric surgery has undergone exponential growth, demonstrating superior long-lasting results when compared to other interventions, resulting in wide recognition and becoming a specialty of its own.
Many factors contributed to this unique escalade or growth trajectory. Undoubtedly, the main cornerstone of the rise in popularity was the ability to perform such procedures with minimal morbidity and mortality due to the introduction of laparoscopic techniques in 1994 (2). Although initially lengthy and challenging, the laparoscopic operations were always characterized by decreased wound infections, bleeding, and ventral hernias, as well as shorter hospital stay while achieving comparable weight loss results. This is especially true in a group of patients in whom open operations had a high rate of short- and long-term complications.
The confidence and popularity reached by the laparoscopic bariatric surgeons was such that even the nonbariatric and nonlaparoscopic procedures benefited from the change in management of the postoperative period (abolition of nasogastric tubes, early feeding after anastomosis, early ambulation and discharge). This steep evolution would have not been possible without the advancement in laparoscopic technologies, in particular the introduction of ultrasonic energy and sophisticated cutters and stapling devices.
Material and Methods
We reviewed some of the most important papers in bariatric surgery in order to identify the historical and current trends of bariatric surgery. We describe some of the most important changes in the concepts of techniques, mechanism of action, and popularity of the different bariatric operations over the years. The choice of the paper reviewed was based on the need to highlight some of the major changes occurred in the acceptance of the different procedures and beliefs during the history of bariatric surgery. This is not meant to be a comprehensive review of all the landmark scientific papers in the bariatric surgery literature.
Results
Based on the review of the literature during the evolution of the bariatric specialty, we can arbitrarily identify several phases:
The pioneer phase;
The laparoscopic phase;
The metabolic phase.
The Pioneer Phase
Initially, the serendipitous evidence that either removing or bypassing the intestine would determine weight loss leads to the development of the first bariatric procedure, the jejunoileal bypass (JIB), by Kremen et al. (3, 4). Although very effective for weight loss, and in spite of variations such as the jejunocolic bypass (JCB), the significant postoperative morbidities related to diarrhea, electrolyte disturbances, vitamin deficiency, and liver failure lead to the abandonment of such procedures (5). While Mason continued to propose procedures that combined restriction and malabsorption, describing the modern Roux-en-Y gastric bypass (RYGB), the idea of simply restricting the gastric volume continued to flourish.
Among the several gastroplasties described in an effort to reduce the gastric volume, the vertical banded gastroplasty (VBG) deserves special attention, as this was the procedure with the overall longest longevity and wider application. First described by Mason (6) in 1982, VBG consists of the creation of a long narrow gastric pouch based on the lesser curvature with a banded narrow outlet. In spite of the respectable weight loss results (excess weight loss (EWL) up to 68%), the long-term complications of band erosion and weight regain from a gastro-gastric fistula are such that this procedure is now considered virtually of historic interest (7).
The idea of reducing the gastric volume by simply placing an extrinsic nonadjustable band was developed by Wilkinson in 1978 and applied more extensively by Molina (8) in 1980. It was in 1985 in Sweden by Hallberg and Forsell, and in 1986 in the United States by Kuzmak, that the modern era of adjustable gastric band began, initially with open techniques and then laparoscopically (9, 10). The placement of an adjustable band below the esophagogastric junction allows for the creation of a small gastric pouch of approximately 15 cm3. Since then, laparoscopic adjustable gastric banding (LAGB) increased in popularity on a yearly basis, while the gastric bypass remained the gold standard of bariatric operations.
During the gastric bypass, a small (15–30 cm3) gastric pouch is created by completely dividing the proximal portion of the stomach from the rest. It is fundamental to completely exclude the more stretchable fundus of the stomach and basing the gastric pouch on the stiffer lesser curvature. The jejunum is then divided at a variable distance of 40–60 cm from the ligament of Treiz. The reconstruction is performed in a typical Roux-en-Y configuration with the jejuno-jejunostomy done at a distance between 100 and 200 cm to determine malabsorption. Although originally the belief was that the mechanism of action of the RYGB was based on the restriction and malabsorption created, several other potential changes seem to contribute to the overall effect of the procedure. Some of these changes will be discussed later on in “the metabolic phase” section of this article.
The Laparoscopic Phase
As previously mentioned, the description of the first laparoscopic RYGB by Wittgrove et al. (2) in 1994 was one of the most important contributing factors for the sudden increase in popularity of bariatric surgery as well as the advancement of laparoscopic gastrointestinal procedures. The increased demand for bariatric surgeons caused the sprouting of a myriad of training programs and teaching courses. With the inevitable spike in popularity soon followed worrisome increase in complications, mostly due to the increased number of patients/cases.
The need for standardization and uniformity of techniques and protocols led to the rise of “Centers of Excellence” (COE) in the United States. This need for organization was not limited to the technical aspect of the surgeries, but also encompassed the multidisciplinary support system for patients in both the preoperative and postoperative periods.
The combination of structured training programs, standardization of techniques, advances in technology, and the organizational and reporting requirements of COE designation leads to the achievement of excellent results. In fact, the complication rates from each procedure became almost negligible (leak rate from gastric bypass of <1%) (7).
During this time, LAGB gained significant popularity. Factors contributing to the widespread popularity of LAGB were the remarkable clinical results (initially in Europe, Australia, and Israel), the paucity of complications (especially early on), and the technical ease of the procedure itself (11). LAGB gained in popularity to the degree that between 2008 and 2010, it became the most commonly performed bariatric procedure worldwide (12). LAGB was performed on an outpatient basis, and often was performed in freestanding surgery centers. Multiple “adjustment clinics” were opened in order to satisfy the increasing patient demand.
Unfortunately, the challenges in obtaining and maintaining weight loss, the intensity of the required follow-up and, most importantly, the publication of poor long-term results that resulted in high explantation rates caused an inversion of the trend in the choice of procedures. Multiple reports of high reoperation rates secondary to long-term complications (slippage, pouch dilatation, dysphagia with megaesophagus, and, in less percentages, erosion) started to appear in the bariatric literature (13). More recently, the drop in popularity and demand of LAGB has caused some experts to question its role in the future of bariatric surgery.
At around the same time when the LAGB started to lose popularity as the preferred bariatric approach, a new procedure, the laparoscopic sleeve gastrectomy (LSG) described by Ren et al. (14), was poised to take the lead (Fig 1). The LSG was initially described as a first-stage operation for very-high-risk patients undergoing biliopancreatic diversion with duodenal switch (BPD-DS) (14). The concept was to perform a simpler and safer operation to achieve initial weight loss. After 6–12 months later, the now healthier patients would undergo the completion BPD-DS to achieve the beneficial metabolic effects of malabsorption. It was soon obvious that LSG itself was providing significant and long-lasting weight loss and that the second-stage completion BPD-DS was only rarely necessary (only 6% of patients required it) (16). The idea behind the LSG is to create a narrow gastric conduit based on the lesser curvature around a calibration tube of 35–45 Fr, by removing in its entirety the fundus and the majority of the body. Typically the majority of the antrum is spared as the resection of the stomach starts between 5 and 7 cm from the pylorus. As a result, the procedure provides significant mechanical restriction, although important changes of the hormonal and entero-insular axis fundamentally contribute to the efficacy of the procedure, as discussed in “the metabolic phase” section.
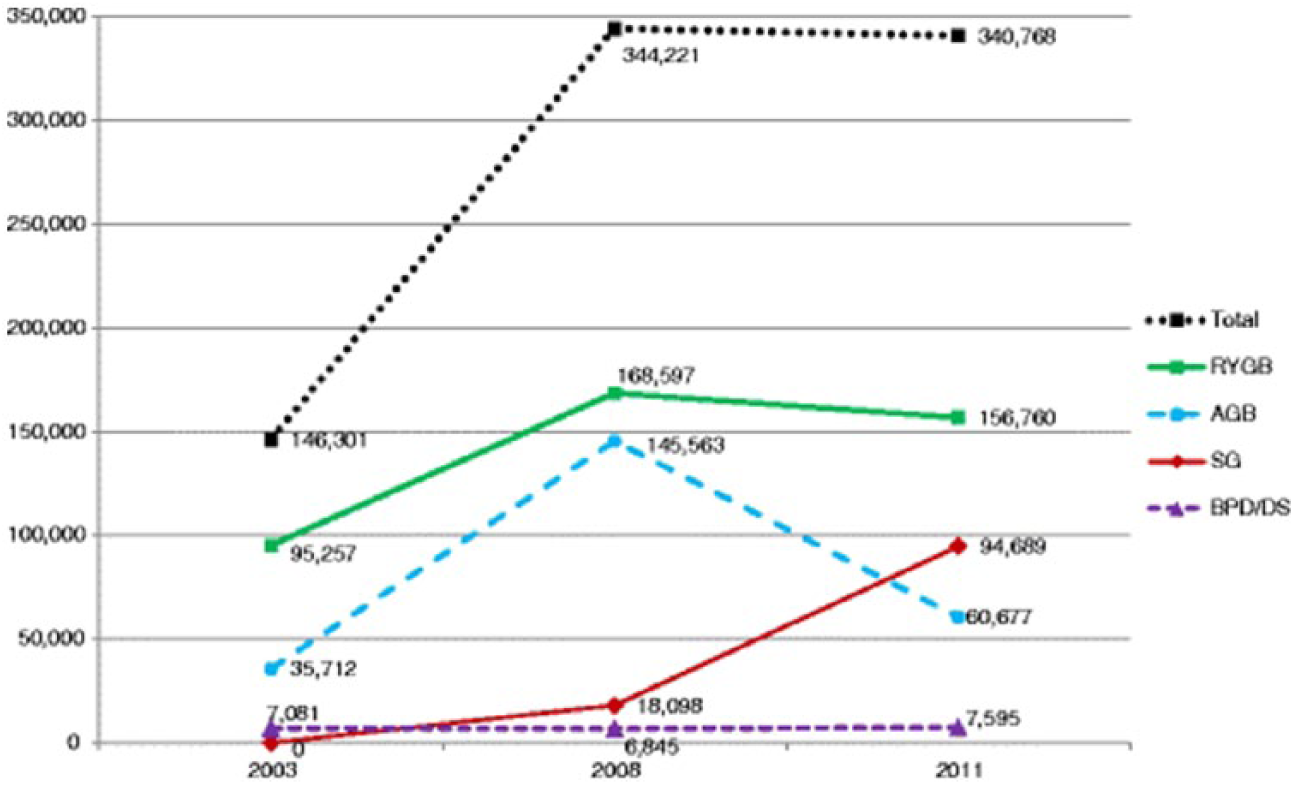
Change in the number of bariatric operations over the years.
Initially, a significant variability in the technique was reported, to the point where several consensus conferences were called in an effort to standardize the procedure and the results (17). Accordingly, and due to a larger body of literature collected since its introduction in 2004, as well as longer follow-up data becoming available, LSG has confirmed its efficacy over time. In fact, in recent data reporting seven or more years of follow-up, LSG had a 55% EWL with minimal short- and long-term complications (18).
In a retrospectively collected series from the American College of Surgeons-Bariatric Surgery Center Network (ACS-BSCN), Hutter et al. (19) positioned the LSG between the LAGB and RYGB when looking not only at efficacy, but also at morbidity and mortality. However, in one of the largest publications comparing morbidity-related procedures, Fridman et al. (20) demonstrated that LSG is not only as efficacious as RYGB, but also has the lowest incidence of complications and reoperations when compared to any other bariatric procedure, including LAGB.
The incidence of staple line disruption after LSG is low at 1.2% (21). However, it is difficult to manage this unusual complication that can result in chronic fistulous tracts and the need for complex reoperative procedures. Several factors contribute to this phenomenon. First of all, the LSG results in increased intraluminal pressure as the diminished volume is created, maintaining an intact outlet valve (the pylorus). Furthermore, two anatomic angles of the newly created sleeve can be critical areas for the development and persistence of a staple line leak. The proximal one at the level of the angle of His is the so-called angle of ischemia. This is the most common location of a leak. Some authors speculate that the dissection close to the esophagogastric junction, along with the division of the short gastric vessels in an area of transition of the blood supply from the distal esophagus to the proximal stomach, can determine a relative ischemia more prone to leak (22).
The second angle of concern is by the incisura angularis on the stomach, where the transection of the stomach too close to the intraluminal sizer (usually a bougie) can determine narrowing or angulation, causing distal outlet obstruction. Since most of the back pressure is then applied to the angle of His, the leaks will manifest in this area and will perpetuate despite patients being nil per os (NPO) for a prolonged period of time. Unfortunately, contrary to what was seen in RYGB, the presence of chronically elevated intraluminal pressure determines a persistence of the leak, often refractory to less than radical interventions.
One of the changes in trend over the last several years has been the almost complete transition to offering LSG as the bariatric procedure of choice (Fig 1). The apparent technical simplicity of the procedure, coupled with the excellent mid- and long-term results, has contributed to the rapid acceptance of LSG. Unfortunately, although apparently technically simple, LSG presents several potentially devastating complications if the previously mentioned technical pitfalls are not carefully evaluated. It is certainly a concern that in the United States, the Centers for Medicare and Medicaid Services, following some isolated single-state data (Michigan Bariatric Surgery Collaborative), have decided to “liberalize” the use of LSG to any center, even those without “Center of Excellence” accreditation (23).
In fact, an increased number of reports describe the difficulty in treating chronic leaks after LSG. Almost invariably, these refractory leaks call for potentially morbid reoperations. The most popular approaches include the use of a Roux limb anatomized directly to the area of chronic fistula, and the conversion to a RYGB with a radical proximal gastrectomy (24, 25). The latter approach has been the authors’ first choice for chronic proximal leak after LSG. In a recent published experience, we reported 15 patients treated with a proximal gastrectomy and Roux-en-Y reconstruction with excellent results (6.6% re-leak, and 6.6% of other minor complication) (25).
Another changing trend we are witnessing with the prevailing of LSG over the other bariatric procedures is the increasing number of long-term reports of worsening, or de novo development, of gastroesophageal reflux disease (GERD) (26). Many factors have been attributed to this surge of GERD cases after LSG. Certainly the dissection at the level of the angle of His with the disturbance of the anatomic anti-GERD mechanisms (i.e. sling mechanism at the angle of His, phrenoesophageal membrane) plays a key role in the development of this potentially debilitating complication (26). Also, the previously mentioned increased intraluminal pressure created by the reduction in volume and the maintenance of an intact pylorus contributes to GERD. More evidence now exists on the misdiagnosis and under-treatment of small and often asymptomatic pre-LSG hiatal hernias (27). As part of consensus criteria, these hiatal hernias are more aggressively sought after and treated (27). Treatment of the GERD cases refractory to medical therapy is usually conversion to RYGB.
Given the always complex geography and now-changing ability to access health-care resources, and similar to what has already been seen with other bariatric operations, long-term follow-up and compliance remain a great challenge to North American bariatric surgery. Contrary to the well-established and more uniformly accessible socialized health-care European systems (Scandinavia in particular), the dropout rates in mid- to long-term follow-up remain a worrisome consideration in North America (28). It is not uncommon to encounter 33% follow-up rates at the 9-year follow-up (28). Obviously, this massive loss in follow-up rates translates to worse results and potentially higher numbers of complex revisional operations (28).
The Metabolic Phase
Finally, another trend in bariatric surgery over the last decade or more that has developed is the increased understanding of the mechanism of action of bariatric procedures. The original attempts to obtain weight loss via restriction, malabsorption, or a combination of both have now been completely translated into the physiologic changes post-procedure (3). One of the first to recognize the metabolic implications of bariatric surgery was Pories, who described the beneficial metabolic effects of RYGB in type II diabetes, with resolution rates of 83% for the diabetic patients and 91% for those with impaired glucose tolerance preoperatively (29). Although weight loss plays a significant role in the resolution of the diabetes, additional mechanisms have been demonstrated. In fact, the profound metabolic changes occurring after bariatric surgery (especially RYGB, BPD-DS, and LSG) are often evident shortly after the procedures, before any significant weight loss. Since then, a massive body of literature has shown some of the changes occurring after bariatric surgery. These changes are very complex and go beyond the scope of this article. With the significant variation among its different types, bariatric surgery causes a great deal of molecular, metabolic, and hormonal changes (3). Some of the commonly accepted metabolic and entero-hormonal changes are summarized in Table 1. Most of these changes are still topics of active research and controversy. Theories on the different changes continue to evolve, some of which attribute changes to either the bypass of the upper intestinal tract (proximal gut hypothesis) or the quicker delivery of nutrients to the distal portion of the intestine with the active secretion of several gut hormones (distal gut hypothesis) (30).
Common entero-hormonal changes after bariatric surgery.
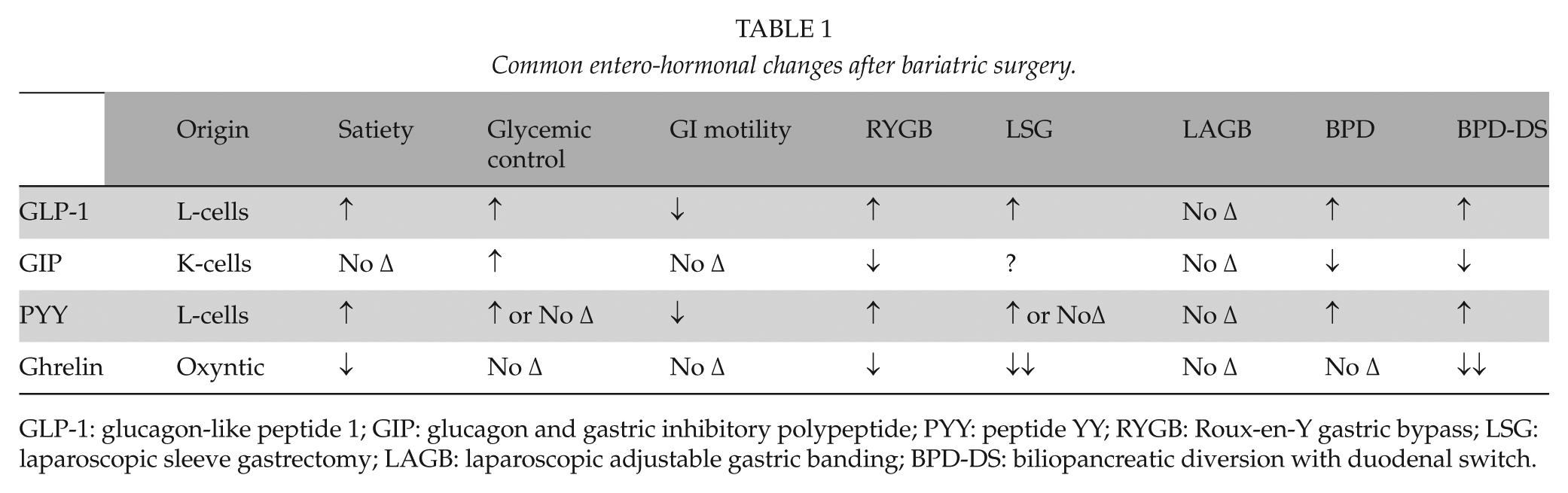
GLP-1: glucagon-like peptide 1; GIP: glucagon and gastric inhibitory polypeptide; PYY: peptide YY; RYGB: Roux-en-Y gastric bypass; LSG: laparoscopic sleeve gastrectomy; LAGB: laparoscopic adjustable gastric banding; BPD-DS: biliopancreatic diversion with duodenal switch.
It is likely that multiple factors contribute to the efficacy of such procedures. Factors include changes in caloric requirements, alteration of gut hormones, alteration of the bile acids and their metabolism regulated by binding to the nuclear receptor farsenoid-X receptor (FXR, also known as NR1H4), changes in the production of inflammatory markers and hormones from the adipose tissue, and finally alterations of the gut microflora (31). Furthermore, increased circulating bile acids, as well as associated changes to gut microbial communities, has been recently shown in animals to be fundamental for the effectiveness of the sleeve gastrectomy procedure (31). In fact, in the animal model, when the nuclear receptor FXR of the bile acid is disrupted, the vertical sleeve gastrectomy loses its efficacy (31). The recognition of such changes and the potential ability to predict the efficacy of obesity-related disease may eventually lead to the individualization of the procedures based on the unique individual metabolic pedigree, likely based on several serologic criteria (3).
As a consequence of these new discoveries, it has become more appropriate to describe the bariatric procedures as “metabolic” and move away from the traditional classification of restrictive, malabsorptive, and combined (3).
Conclusion
Bariatric surgery has undergone several key changes in the last decade. Besides world recognition of bariatric surgery as a subspecialty of its own, and the understanding and acceptance of the need for a multidisciplinary approach to the morbidly obese patient, several shifts in preferred procedure have occurred. Alongside a dramatic fall in popularity of LAGB, an increased interest in LSG has occurred. Its apparent simplicity should not, however, be associated with indiscriminate application by the nonexperts.
Finally, the continued recognition of new mechanisms of action in bariatric surgery will likely lead to more precise indications and individualization of the different procedures in order to achieve the best results.
Footnotes
Declaration of Conflicting Interests
None of the authors have any conflict of interest pertaining to this manuscript.
Funding
No funds were received for this manuscript.