
Abstract
Background:
Nonsuicidal self-injury (NSSI) affects many autistic individuals, and has been linked to suicidality in this group. It has been closely linked to difficulties with intrapersonal emotion regulation, but a role of interpersonal emotion regulation processes in NSSI has been underexplored. Empathic disequilibrium is a state of imbalance between a person’s cognitive empathy (CE) and emotional empathy (EE). We recently found that autistic people exhibit heightened EE relative to CE, consistent with their firsthand reports of hypersensitivity to the emotions of others. Because this kind of empathic imbalance is associated with hyperarousal and emotional reactivity, we hypothesized that it might increase the risk of NSSI, which often occurs as a means of trying to regulate overwhelming or distressing emotions.
Methods:
We measured CE, EE, emotional reactivity, and NSSI behaviors in 304 autistic and 289 nonautistic participants, and used polynomial regression with response surface analysis to examine empathic disequilibrium as a predictor of emotional reactivity and engagement in NSSI.
Results:
Replicating previous research, individuals with an autism diagnosis were more likely to show a pattern of EE-dominance (OR = 4.51 [2.66, 7.63], p < 0.001), although they did not differ significantly in overall empathy levels. While empathic disequilibrium was associated with NSSI in autistic and nonautistic people, the nature of these pathways differed between groups. In autistic people, empathic disequilibrium toward EE-dominance was associated with a higher incidence of NSSI through emotional reactivity. In contrast, for nonautistic individuals, the incidence of NSSI was associated with overall empathy and, when accounting for emotional reactivity, with empathic disequilibrium toward CE dominance.
Conclusions:
While future studies should investigate the direction of relationships with longitudinal designs, these findings highlight different mechanisms for NSSI in autistic and nonautistic people. They corroborate growing evidence that the relative imbalance between empathic abilities may be relevant for meaningful outcomes, such as psychopathology.
Community Brief
Why is this an important issue?
Autistic people have told us that they feel the emotions of other people strongly. Indeed, our group has found that being autistic is associated with having relatively higher emotional empathy (EE) than cognitive empathy (CE). EE is the ability to share the emotional states of others. CE is the ability to identify how someone else is feeling. When your EE is stronger than your CE, you can be easily overwhelmed by the emotions of other people. This is because normally, your CE acts as a kind of regulatory force to dampen down your emotional response to the emotions of others.
It is extremely important that we correct the stigmatizing myth that autistic people lack empathy. It is also important to look at negative outcomes that could be related to feeling the emotions of others so strongly. One such outcome might be self-injury, which often occurs when people are trying to manage overwhelming emotions. This is a common behavior in autistic people and is associated with suicide, so it is important to understand it.
What was the purpose of this study?
We wanted to see whether we could replicate the same pattern of empathic disequilibrium, specifically higher EE than CE, in autistic people. We also wanted to see whether this pattern was associated with self-injury, and whether this was because people with higher EE tend to be emotionally reactive (experience emotions strongly).
What did the researchers do?
We conducted an online survey of 304 autistic and 289 nonautistic people. They completed questionnaires measuring EE and CE, emotional reactivity, and self-injury. We then performed an analysis to see whether relatively higher levels of EE than CE could predict emotional reactivity, and through that, self-injury.
What were the results of the study?
We found that being autistic was associated with having relatively higher EE than CE, but not having lower empathy overall. This state of EE-dominant empathic disequilibrium was related to being more emotionally reactive, and through this, with greater incidence of self-injury in autistic people. Interestingly, these relationships seemed to work differently in nonautistic people, who might have different risk factors for self-injury.
What do these findings add to what was already known?
These findings confirm that autism is not characterized by lower empathy, but by relatively higher EE than CE. They corroborate firsthand reports from autistic people who express how unpleasant it can be to experience other people’s emotions so strongly. Our findings suggest that this pattern of higher EE to CE may be associated with negative outcomes related to emotional dysregulation, such as self-injury.
What are potential weaknesses in the study?
We cannot confirm the direction of relationships between the variables in our study. Our sample is not representative of all autistic people.
How will these findings help autistic adults now or in the future?
These findings challenge the myth that autistic people lack empathy: in fact, they are hyperresponsive to the emotions of others, and this may be bad for their mental health.
Background
Nonsuicidal self-injury (NSSI, also known as self-harm) is the deliberate infliction of pain and/or injury on the body through behaviors such as cutting, biting, or burning. While not driven by suicidal intent, it is robustly associated with psychopathology and suicide risk. Autistic people are at higher risk of engaging in NSSI, yet little is known about the psychological mechanisms that underlie this link. One possible mechanism is empathic disequilibrium, a term reflecting the imbalance between the emotional and cognitive aspects of empathy (see Table 1). Most notably, imbalance toward emotional empathy (EE) is associated with autism and autistic traits, and with greater emotional reactivity.1–3 As emotional reactivity and dysregulation are closely linked to NSSI,4–6 we examined the links between empathic disequilibrium and NSSI in autistic and nonautistic individuals and examined the role of emotional reactivity as a possible mediator of this relationship.
Glossary of Terms as Used Herein
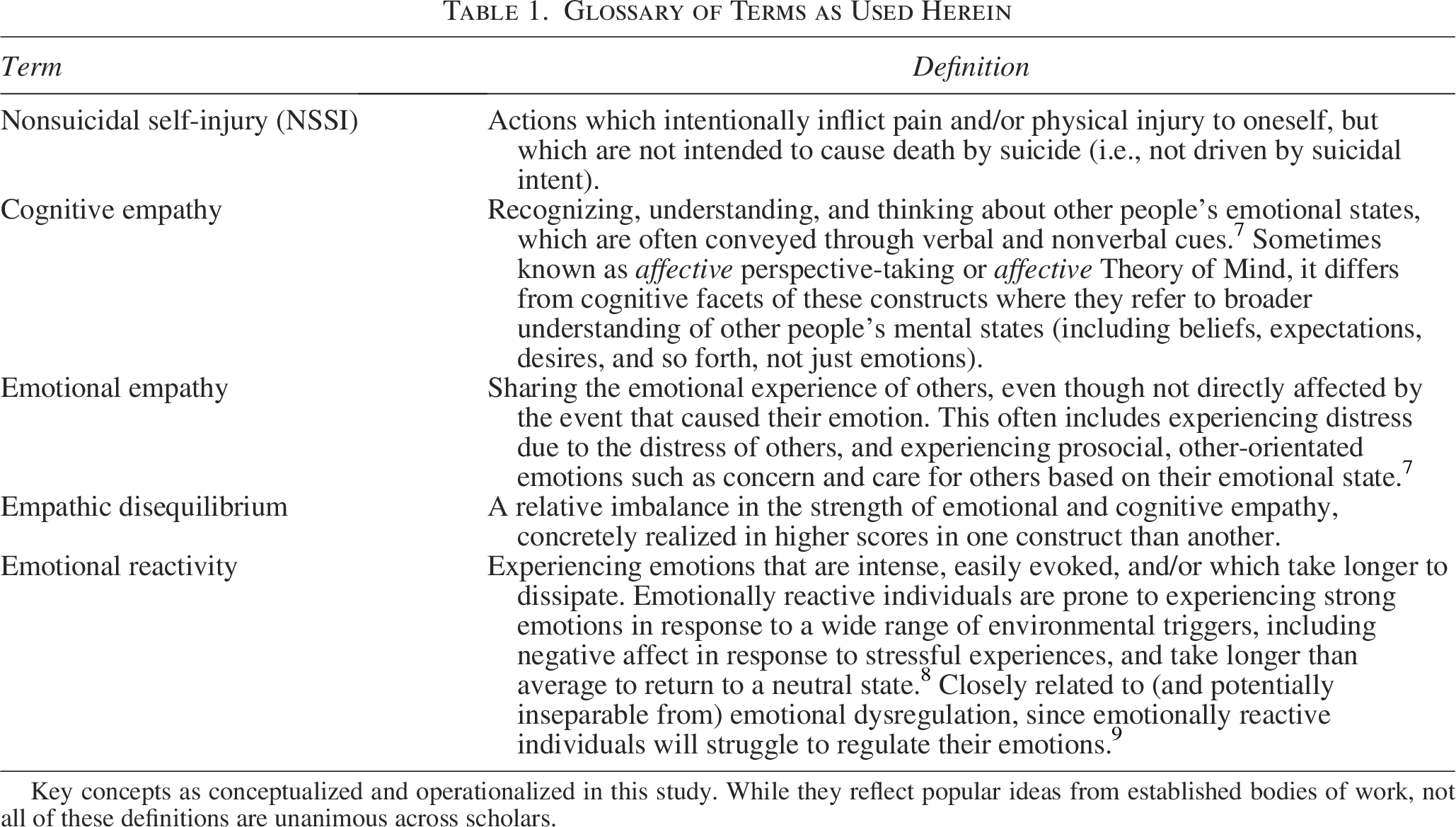
Key concepts as conceptualized and operationalized in this study. While they reflect popular ideas from established bodies of work, not all of these definitions are unanimous across scholars.
Self-injury is highly prevalent in autistic people, with an estimated 42% of the autistic population affected. 7 Autistic people are three to five times more likely to engage in self-injury * than are nonautistic counterparts,8,9 with risk slightly higher in adults. Indeed, while NSSI typically peaks in adolescence and then declines in nonautistic people, 10 self-injurious behavior appears to remain prevalent in autistic adults, including possibly autistic older adults in the 55–70 age range. 11 Relatively little is known about NSSI in autistic people, but their reports suggest that it resembles nonautistic NSSI in age of onset and functional purposes.12–14 In autistic and nonautistic populations alike, NSSI has deleterious consequences on confidence, self-worth, and relationships.13,15,16 Further concern about it is warranted, however, by relationships demonstrated, in the general population, between NSSI and poor psychosocial outcomes,17,18 and the development and exacerbation of psychopathology.19,20 In addition to increasing suicide risk via effects on psychopathology, 21 NSSI is itself robustly associated with later suicidality.22,23 While the evidence base is scarcer, these relationships appear to operate similarly in autistic people, where NSSI is likewise associated with psychopathology, 13 and appears to contribute to the heightened suicide risk seen in this group.24–26 Given that autistic people have higher rates of psychopathology 27 and suicidality, 25 it is imperative to better understand the risk factors associated with NSSI, how best to prevent it, and support individuals who desire recovery, to ameliorate these kind of debilitating and devastating outcomes.
While emotion regulation appears to be a principal function of NSSI for autistic12–14 and nonautistic people alike,28,29 the initiation and maintenance of NSSI have been linked to difficulties with emotion awareness and regulation, as well as emotional reactivity (being more prone to experience strong and perseverative emotions from a range of stimuli).4–6 However, another facet of emotion processing remains underexplored as a risk factor for NSSI in autistic and nonautistic people: the interpersonal dimension of emotions, as is fundamentally reflected in our abilities to understand and to share the emotions of others. These two abilities, termed cognitive empathy (CE) and EE, are considered aspects of empathy that are genetically, developmentally, and biologically distinct.30,31 The former describes the ability to understand the emotional states of others, closely corresponding to affective aspects of Theory of Mind. 32 The latter describes an individual’s sensitivity to and sharing of other people’s emotional states, while maintaining a self-other distinction. The neural substrates that support recognizing and responding to others’ emotions are, to a large extent, those that support recognizing, and regulating one’s own33–35 ; as such, being able to identify and regulate one’s own emotions are closely related to an individual’s ability to recognize and respond emotionally to others.36–38 The same appears to be true in autistic people, where levels of alexithymia (difficulty identifying and describing one’s emotional state) are strongly predictive of empathic processes.39,40
Differences in CE and/or EE have long been linked to the development of psychopathology,41,42 but a new mechanism through which empathic processes might affect mental health was recently proposed. Shalev, Uzefovsky 2 emphasized the importance of considering, beyond the overall levels of CE and/or EE, the relative strength of each process compared with the other. Given the complexity and ambiguity inherent to social interaction, they suggest that the interplay of these two processes, which can influence and regulate one another, is essential for adaptive and flexible social responses. In this scenario, an individual whose EE is relatively stronger than the CE is likely to experience overarousal in response to others’ emotions, since a corresponding level of CE is needed to regulate an individual’s own affective response to others’ emotions. Consequently, this imbalance of empathic processes might be experienced as distress or discomfort, reflecting higher emotional reactivity to the emotions of others as well as one’s own. 1
There is precedent for the idea that autistic people might show relative differences in empathic processes, but theoretical accounts have thus far unfortunately tended to be deficit-based. In the empathy imbalance hypothesis, 43 Smith proposed that autistic people might exhibit “a deficit of CE but a surfeit of EE.” He suggested difficulties with CE would make it difficult to channel empathic concern for others into an adaptive response, and the emotional arousal might be experienced as highly distressing (as per Rogers et al. 44 and Dziobek et al. 45 ); accordingly, Smith posited that “impaired” CE in the presence of “enhanced” EE would give rise to “a confusing and aversive experience” wherein the individual’s “sense of self would easily be permeated by other people’s emotions” (pp.494). The empathic imbalance hypothesis was coached in terms of deficits (impaired CE and enhanced EE), and subsequent literature has failed to reliably reproduce this pattern in autistic people. There have also been important developments in recent work that recognizes that difficulties establishing an empathic connection may originate from the different communication styles of neurotypical and neurodivergent individuals, rather than impairments in either party. 46 Consequently, criticism and doubts have been raised regarding the validity of delineating empathy into discrete components in the context of autism. 47 Nevertheless, in so far as it relates to intraindividual cognitive processes and their ramifications for the individuals and their social world, Shalev and colleagues showed, across several samples, that the relative imbalance between CE and EE—specifically, a pattern of stronger EE than CE, rather than deficits or enhancements in either—was predictive of autistic features (particularly social differences) and an autism diagnosis, while overall empathy levels were not.1–3
Deficit-focused approaches to empathy have been a source of stigma for autistic people, who have reported that they feel the emotions of others to an intense, sometimes incapacitating extent.47–50 This new empathic framework thus seems timely, and appears capable of explaining this aspect of the autistic social experience: EE-dominant empathic disequilibrium would indeed be characterized by hyperreactivity to the emotions of others without the same extent of CE downregulatory control. 1 EE-dominant empathic disequilibrium might, subsequently, leave individuals particularly prone to poor mental health, and hence explain another aspect of the autistic experience. Given the relationship between NSSI and the way people experience their emotions, we query, for the first time, whether autistic and nonautistic individuals with a greater extent of empathic disequilibrium between EE and CE may be more likely to turn to NSSI to regulate the overwhelm associated with experiencing other people’s emotions.
The present study constitutes a preliminary test of the above hypothesis while testing the replicability of previous observations. Specifically, we suggest that as per previous studies,1–3 autistic people are likely to be characterized by a greater EE than CE. Given the role of CE and EE in exerting regulatory balance over one another in social interactions, and in line with previous findings, 1 we secondly suggest that empathic disequilibrium toward EE will be associated with greater emotion reactivity. Mediated by this heightened emotion reactivity, we thirdly suggest that individuals with greater empathic disequilibrium may have a greater likelihood of engaging in NSSI.
Methods
Participants
This study was advertised as a study on empathy and mental health. Our autistic adult sample (n = 304) was recruited through contacting participants from previous research by our UK-based group,26,51 and through use of Prolific, a site for research participation. Participants from our previous work constituted 44% of the sample; we invited back only those who lived in the United Kingdom (approximately 350, giving a response rate of about 38%). We obtained the other 56% from Prolific, where we advertised for participants diagnosed as autistic, older than 18, fluent in English, and living in the United Kingdom. Of the whole autistic sample, just under half (144) had been assigned male at birth; of these, 94% identified as cisgender men, 3.5% as nonbinary, and the remainder chose not to report their gender. Of the 160 participants who reported having been assigned female at birth, 86.9% identified as cisgender women, 9.4% as nonbinary, and 0.6% as transgender men, with the remainder choosing not to report their gender. We applied inclusion criteria where inclusion in the study was on the basis of self-reporting a formal autism diagnosis. Most participants were diagnosed as adults (average age 28.6 [SD: 13.3] and 28.2 [SD: 17.2] in people assigned male and female at birth, respectively). Altogether, 203 autistic (66.8% of the autistic sample) reported some lifetime experience of NSSI † . Of these, 61.8% were assigned female at birth.
We recruited autistic participants between January 2022 and July 2022, and began recruiting age- and sex-matched nonautistic participants on Prolific when 74% of the autism data were collected, in the period between May and July 2022. Initially, we advertised for cisgender UK-based men and women who had never received a diagnosis of autism or ADHD. When we had recruited 76% of the nonautistic group, we implemented a change in recruitment strategy. We did this because a high proportion of the autistic group reported recent and/or sustained engagement in NSSI, while only 19% of nonautistic people recruited at that point endorsed any experience of NSSI. To create more equivalent groups, we purposively screened for nonautistic men and women with some experience of NSSI. The final group comprised 289 nonautistic participants. Of them, 147 indicated they had been assigned male at birth (with 146 cisgender, and 1 participant nonbinary). All 142 participants who indicated they had been assigned female at birth identified as cisgender. Of the nonautistic group, 113 (39.1%) reported some lifetime experience of NSSI; of that 113, 50% had been assigned female at birth.
We conducted a power analysis, using the simr v1.0.5 package (53) and based on 5,000 Monte Carlo simulations, which showed that 280 in each group would provide sufficient power (1-β ≥ 0.85, α = 0.05) to detect effects of even small sizes (r = 0.1). The demographic information of the groups is shown in Table 2, along with their scores in major study variables.
Participant Demographics and Scores in Major Study Variables
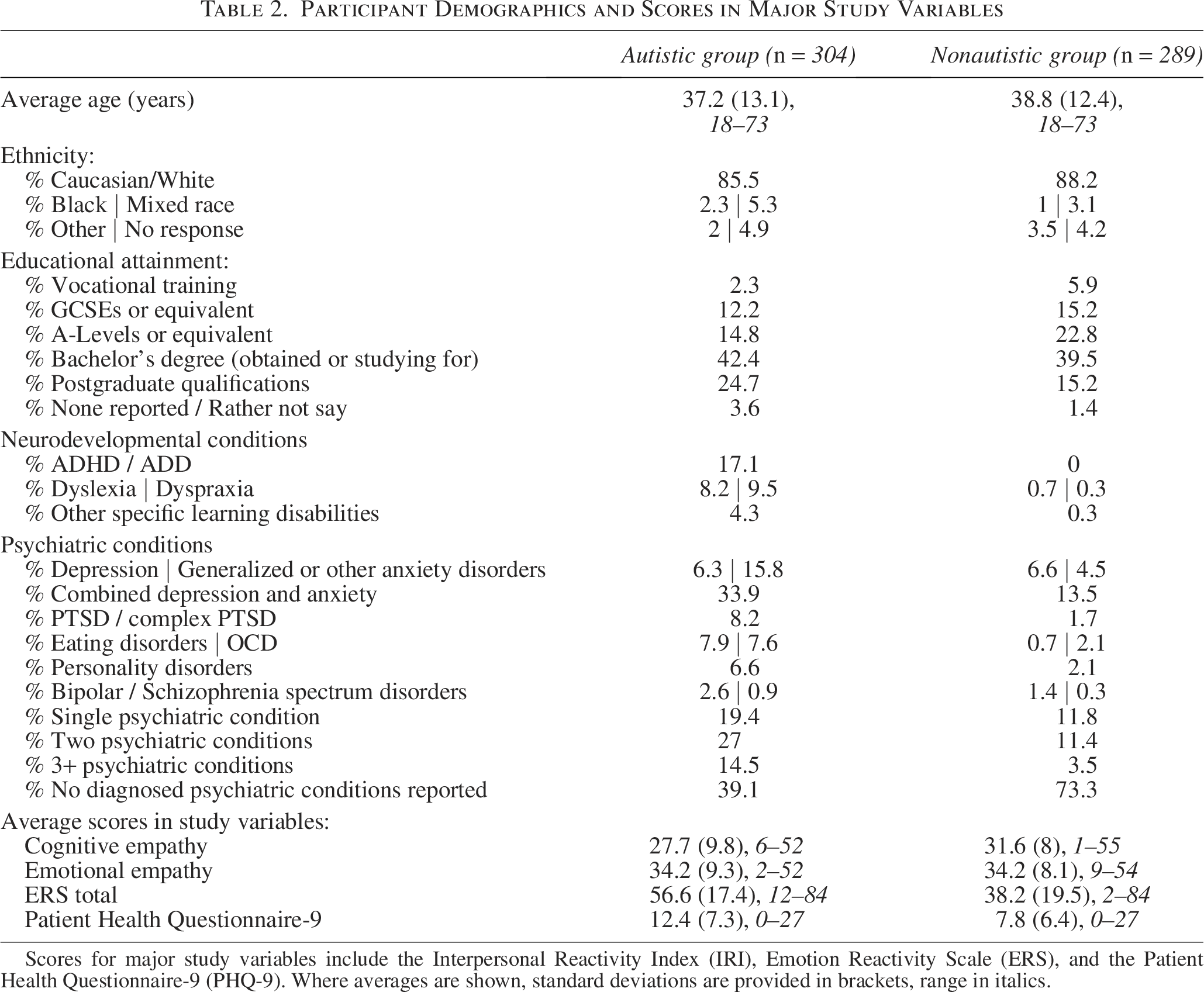
Scores for major study variables include the Interpersonal Reactivity Index (IRI), Emotion Reactivity Scale (ERS), and the Patient Health Questionnaire-9 (PHQ-9). Where averages are shown, standard deviations are provided in brackets, range in italics.
Materials and Procedure
The study was approved by the Ethics Panel of the Faculty of Science and Technology at Bournemouth University (ID 39520). All participants provided fully informed consent to take part, and for their anonymous data to be published. After consenting to participate, participants completed an online survey (approximately 30 minutes), which comprised the following:
Interpersonal Reactivity Index
The Interpersonal Reactivity Index (IRI)52,53 is a popular multidimensional measure of empathy. The four 7-item scales reflect the tendency to be emotionally affected by fictional characters and situations (Fantasy); the tendency to imagine other people’s perspectives, regardless of accuracy (Perspective-Taking); the tendency to feel “other-orientated” emotions such as concern, sympathy, or compassion in response to others’ distress (Empathic Concern); and the tendency to experience “self-orientated” distress, anxiety, or discomfort in response to others’ distress (Personal Distress). On a 5-point Likert scale, higher scores reflect higher tendencies in each subscale. In accordance with bidimensional conceptions of empathy, 54 researchers often aggregate Fantasy and Perspective-Taking scales as a measure of CE, and Empathic Concern and Personal Distress to reflect EE (e.g., Fan et al. 55 and Gabay et al. 56 ). As per previous reports, 57 these aggregations of CE and EE had high internal consistency in our samples (for autistic and nonautistic participants, respectively, α = 0.83 and 0.82 for CE; and 0.83 and 0.82 for EE). While the literature base on assessment of empathy in autistic populations is inadequate, the IRI emerges as superior to some contemporaries in what little psychometric information is available. 58
Before analysis, to make our results more comprehensible in terms of population norms, we standardized CE and EE (dividing CE and EE by the standard deviation of the sample, and centering them based on the mean of the nonautistic group ‡ ). Since we assume patterns of empathy to differ in autistic versus nonautistic people, centering by the mean of the nonautistic group makes it easier to interpret these differences on a scale of all participants. This resulted in standardized scores for CE and EE that are relative to the mean of the nonautistic group.
Emotion Reactivity Scale
The 21-item Emotion Reactivity Scale (ERS) 59 captures an individual’s tendency to experience emotions frequently and easily (Sensitivity, 8 items), strongly (Arousal/Intensity, 10 items), and for prolonged periods (Persistence, 3 items). Higher scores reflect high emotion reactivity. The scale has strong psychometric properties and convergent and criterion-related validity with related scales and physiological measures. 60 It has been robustly used in research on NSSI and suicidality (e.g., Hamza et al. 61 ) although has not yet been validated in autistic samples. We used the total score, which had high internal consistency in autistic and nonautistic groups (α = 0.94, 0.96, respectively).
Non-Suicidal Self-Injury Assessment Tool
The Non-Suicidal Self-Injury-Assessment Tool (NSSI-AT) 62 is a comprehensive battery that assesses the type, frequency, recency, severity, and functional purpose of self-injurious behaviors. From this we derived the primary variable of our analysis, lifetime incidence of NSSI, which we coded so that scores ranged from participants having never engaged in NSSI (0), having tried it once (1), to having engaged in NSSI 2–3 times (2), 4–5 times (3), 6–10 times (4), 11–20 times (5), 21–50 times (6), >50 times (7). The NSSI-AT, while popularly used in autism studies interested in differentiating between suicidal and nonsuicidal self-injury,13,14,25,26 has not been validated in autistic people.
Patient Health Questionnaire-9
Because depression is a robust correlate of NSSI and was observed to be associated with empathic disequilibrium, 1 we controlled for depressive symptoms so as to isolate relationships between the other two. Scores for the Patient Health Questionnaire-9 (PHQ-9) 63 range between 0 and 27, with 8 the recommended cutoff for major depressive disorder 64 : 205 autistic and 117 nonautistic participants scored at or above the cutoff. The PHQ-9 has recently been validated in autistic people 65 ; internal consistency was equally high in autistic and nonautistic participants (α = 0.91).
Analysis
Only three participants did not complete the PHQ and the ERS. The remaining participants completed all primary variables, resulting in a very small amount of missing data, which we replaced by calculating the sample mean of these variables. We undertook an initial descriptive analysis (Supplementary Data S1) to characterize the features of NSSI, and relationships between these features, in just those participants who endorsed some lifetime history of NSSI.
As per previous research on empathic disequilibrium,1,3 we used polynomial regression with response surface analysis (PRRSA), a means of estimating the similarity and dissimilarity between two variables of interest (in this instance, equilibrium and disequilibrium between CE and EE) and an outcome variable. 66 We describe the results of the PRRSA by four parameters that estimate the linear (a1 = CE + EE) and nonlinear (a2 = CE2 + CE × EE + EE2) association of overall empathy and the outcome; and the linear (a3 = CE − EE) and nonlinear (a4 = CE2 − CE × EE + EE2) association of empathic disequilibrium with the outcomes. Accordingly, a negative correlation with a3 suggests a tendency toward EE-dominance to be related to the outcome, while a positive correlation with a3 suggests a tendency toward CE-dominance to be related to the outcome.
To initially test whether previously reported associations between autism and empathic disequilibrium 3 could be replicated, we conducted a logistic PRRSA with autism diagnostic status as a binary outcome. We were not focused on sex or gender differences, but as these factors were found to be related to empathic disequilibrium,1–3 it was important for us to examine whether the polynomial regression differed between people assigned male or female at birth. § As this previous work suggested an autism diagnosis to be related to EE-dominance, 1/OR is reported for a negative association with empathic disequilibrium, allowing for easier interpretation of the results.
Next, we tested the hypotheses that empathic disequilibrium would be associated with emotional reactivity, and through this mediator, lifetime incidence of NSSI. We conducted multigroup analyses to examine whether these models differed by group (autistic/nonautistic people), or by sex assigned at birth. We examined any models that statistically differed by group and/or by sex assigned at birth separately. To account for the possible relationship between depression and NSSI, we controlled for PHQ scores in all analyses.
To examine the mediation, we followed the guidelines proposed by Yzerbyt, Muller, Batailler, and Judd. 67 Specifically, we examined the significance of the association between the PRRSA parameters and emotional reactivity (path A) and the association between emotional reactivity and NSSI (path B). We used the product of paths A and B to estimate the indirect path (path AB), with 95% confidence intervals calculated using the Monte-Carlo resampling of 10,000 samples. We performed all analyses in R v4.1.2. 68 We used lavaan package v0.6.9 69 to assess the PRRSA parameters, conduct the mediation analyses, and perform the multigroup analyses; the Monte-Carlo CI function of the semTools package v.0.5-5 for resampling 70 ; and the plotRSA function of the RSA package v0.10.4 71 to plot the response surfaces. Data, codes, and materials are available on request. Notedly, where we use conventional statistical language of prediction in the above analyses, our cross-sectional design means that relationships reflect associations rather than implying causal directionality.
Results
We display the lifetime incidence of NSSI in autistic and nonautistic participants with experience of NSSI, the types of NSSI engaged in, and the recency of last NSSI incident, in Figure 1. Findings from our initial descriptive analysis (see Supplementary Data S1) gave the impression that autistic self-injury, in particular, might occur with increased variability and unintended severity, indicative of emotional dysregulation.
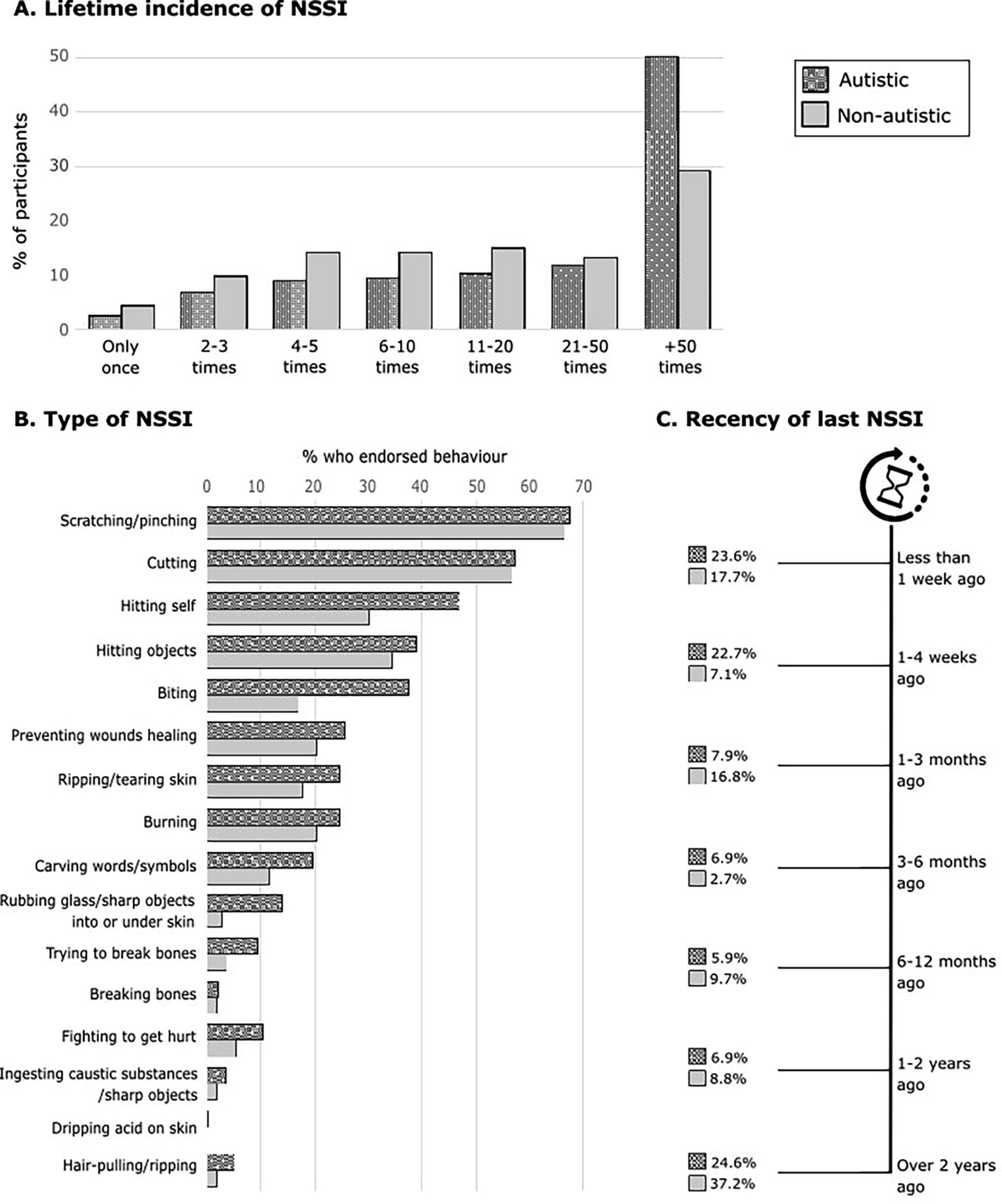
Features of NSSI in autistic and nonautistic participants. Part A depicts the lifetime incidence of NSSI in those participants with any history of NSSI engagement (66.8% of autistic, 39.1% of nonautistic participants). In this same group, Part B depicts the percentage of participants who endorsed ever having engaged in the listed behavior; all behaviors listed are categories in the NSSI-AT with the exception of hair-pulling/ripping, which was entered in a free-text box by a number of participants. Part C depicts the recency of NSSI behavior in those with any history of NSSI; note that 1.5% of autistic participants declined to answer this question. Throughout, autistic participants are represented by patterned/textured bars/boxes, nonautistic participants by plain gray. NSSI, Nonsuicidal self-injury; NSSI-AT, Non-Suicidal Self-Injury-Assessment Tool.
Empathic disequilibrium as a predictor of autism
We found that the overall model predicted autism diagnostic status (Nagelkerke R2 = 0.26, p < 0.001), as shown in Figure 2. As we hypothesized, empathic disequilibrium toward EE-dominance was linearly related to autism diagnostic status (1/OR = 4.51, 95% CI = [2.66, 7.63], p < 0.001). We did not find any curvilinear association with empathic disequilibrium (OR = 1.66, 95% CI = [0.86, 3.17], p = 0.19). Nor did we find any relationship between overall empathy and autism diagnostic status, in either linear (OR = 0.76, 95% CI = [0.55, 1.05], p = 0.13) or nonlinear associations (OR = 1.26, 95% CI = [0.97, 1.63], p = 0.10). We found no differences related to sex assigned at birth [χ2 (5, N = 593) = 8.34, p = 0.14], so we did not include this variable in any further analyses.
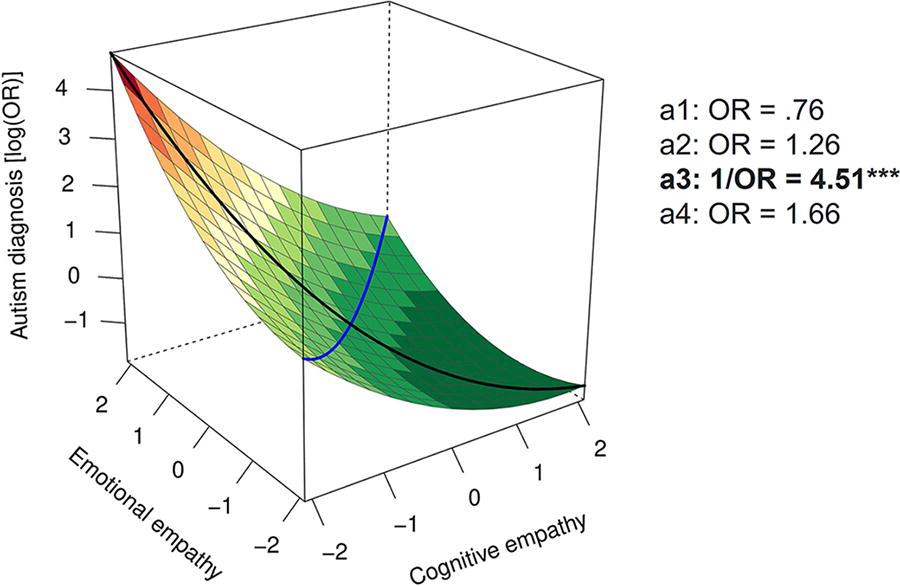
Polynomial regression plot predicting autism diagnostic status. The black line shows the projection of the empathic disequilibrium line and the blue line shows the projection of the overall empathy line. Moving away from the center along the black line toward the left corner corresponds to surfaces of emotional empathy dominance, while moving toward the right corner corresponds to cognitive empathy dominance. Likewise, moving up along the blue line represents areas of higher overall empathy. The log(OR) of an autism diagnosis is represented by colors, with green indicating a lower probability and red indicating a higher probability. ***p <0.005.
Empathic disequilibrium as a predictor of NSSI via emotional reactivity
We next aimed to assess the mediation model. For convenience and transparency, we describe unstandardized estimates (b), their confidence intervals, and full p-values of the surface parameters within the text as well as all parameters of the mediation analyses (AB path). We display standardized estimates (β) in the corresponding figures. We found no differences in the mediation pathway between people assigned male and female at birth [χ2 (1, N = 590) = 2.98, p = 0.08]. Yet, as we observed different pathways for autistic and nonautistic people [χ2 (2, N = 590) = 20.11, p < 0.001], we analyzed the mediation model separately for autistic and nonautistic people. We display the parameters of the polynomial regression for all models in Supplementary Data S1.
Autistic participants
The mediation model in autistic people had excellent fit indices, χ2 (1) = 1.02, p = 0.312; χ2/df = 1.02; normed fit index (NFI) = 0.99; comparative fit index (CFI) = 1.00; root mean square error of approximation (RMSEA) = 0.009. We display a summary of the results in Figure 3.
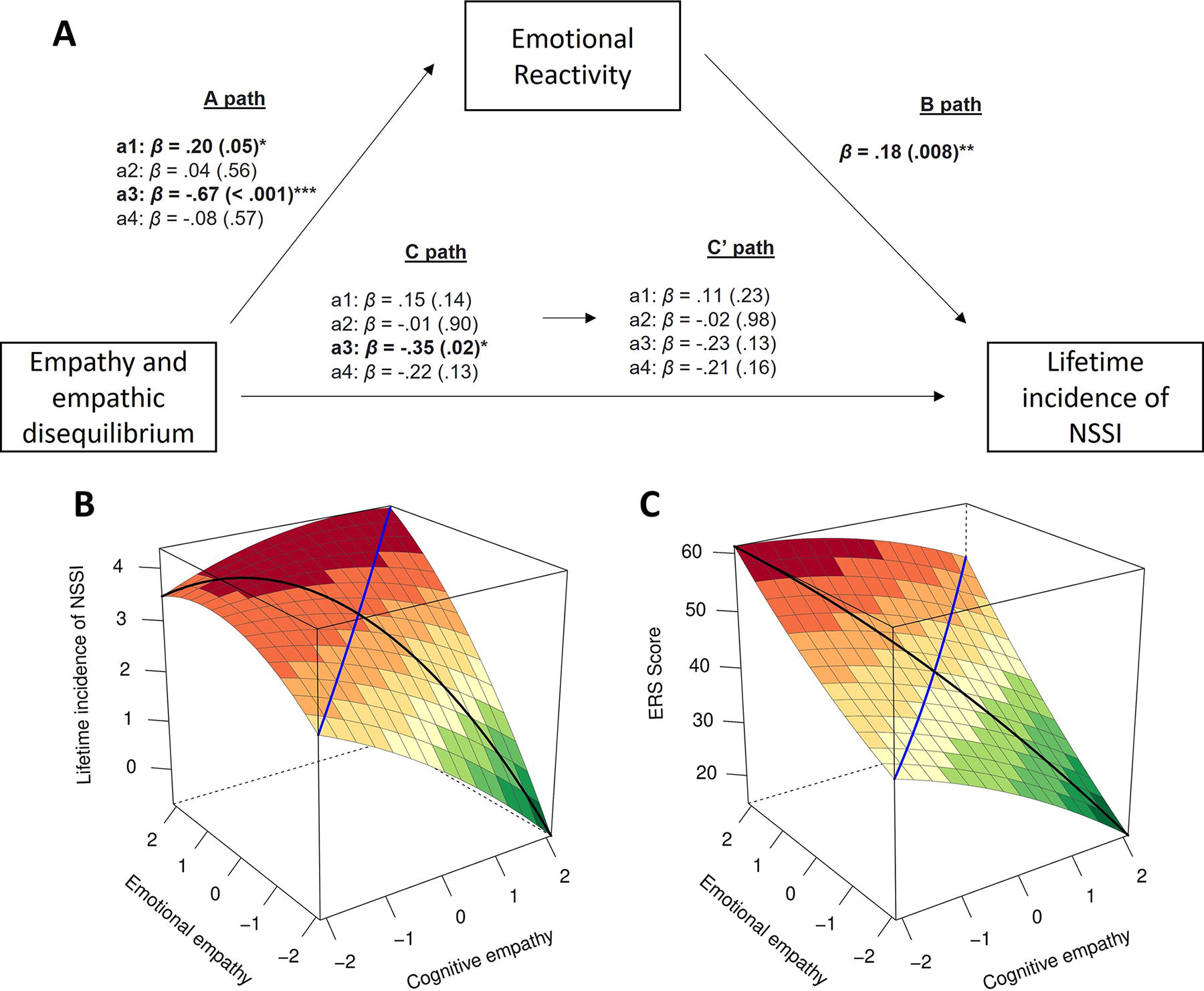
Mediation model predicting lifetime incidence of NSSI in autistic people. Part A depicts a plot of the association between the response surface parameters and lifetime NSSI and its mediation by emotional reactivity in autistic people. The reported parameters represent the linear
First, we found the total effect (without controlling for emotional reactivity; C path in Fig. 3A, and Fig. 3B) of empathic disequilibrium (toward EE-dominance) to be linearly related to lifetime incidence of NSSI (ba3 = −0.990, 95% CI [−1.81, −0.17], p = 0.02). We found no linear association between overall empathy and lifetime incidence of NSSI (ba1 = 0.41, 95% CI [−0.13, 0.95], p = 0.14), and no nonlinear association for either overall empathy or empathic disequilibrium.
We found that empathic disequilibrium with a tendency toward EE-dominance was also linearly related to emotional reactivity (b = −11.09, 95% CI [−16.16, −6.02], p < 0.001; Fig. 3A—A path, and Fig. 3C), which was associated with lifetime incidence of NSSI (b = 0.031, 95% CI [0.01, 0.05], p = 0.008; Fig. 3A—B path). As suggested by the indirect effect, the association between empathic disequilibrium and NSSI was fully mediated by emotional reactivity (βAB = −0.12, AB estimate = −0.34, 95% CI [−0.70, −0.07]), and became nonsignificant after controlling for emotional reactivity (ba3 = −0.65, 95% CI [−1.50, 0.19], p = 0.13; Fig. 3A—path C’).
Nonautistic participants
The mediation model in nonautistic people also revealed excellent fit indices, χ2 (1) = 0.40, p = 0.52; χ2/df = 0.40; NFI = 1.00; CFI = 1.00; RMSEA = 0.0001. We display a summary of the results in Figure 4.
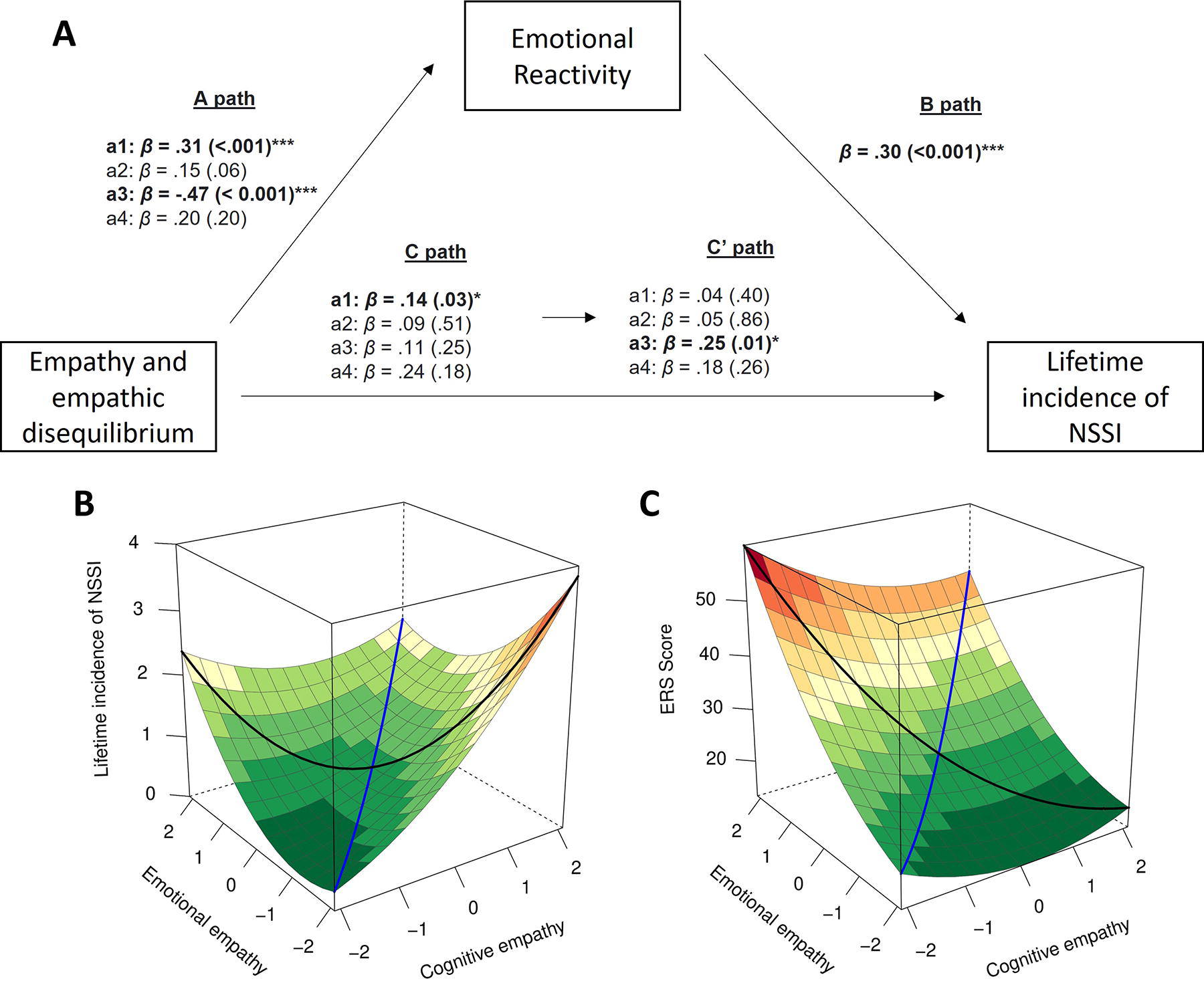
Mediation model predicting lifetime incidence of NSSI in nonautistic people. Part A shows a plot of the association between the response surface parameters and lifetime NSSI and its mediation by emotional reactivity in nonautistic people. The reported parameters represent the linear
Unlike the model for autistic people, without controlling for emotional reactivity (C path in Fig. 4A and Fig. 4B), we found that empathic disequilibrium was unrelated to lifetime incidence of NSSI either linearly (ba3 = 0.36, 95% CI [−0.26, 0.97], p = 0.25) or nonlinearly (ba4 = 0.55, 95% CI [−0.25, 1.36], p = 0.18). In contrast, greater overall empathy was linearly associated with higher lifetime incidence of NSSI (ba1 = 0.43, 95% CI [0.03, 0.82], p = 0.03). We found no nonlinear association for overall empathy (ba2 = 0.11, 95% CI [−0.21, 0.43], p = 0.51).
Greater overall empathy was also related to greater emotional reactivity, which in turn was associated with greater lifetime incidence of NSSI (b = 0.04, 95% CI [0.02, 0.06], p < 0.001; A path in Fig. 4A, and Fig. 4C). Emotional reactivity fully mediated the association between overall empathy and lifetime incidence of NSSI (βAB = 0.09, AB estimate = 0.43, 95% CI [0.04, 0.81]), which became nonsignificant after controlling for emotional reactivity (ba1 = 0.16, 95% CI [−0.21, 0.54], p = 0.40; path C’ in Fig. 4A).
Although we did not find a significant total effect between empathic disequilibrium and lifetime incidence of NSSI, empathic disequilibrium was linearly related to emotional reactivity as we previously saw for autistic people (ba3 = −10.23, 95% CI [−13.73, −6.72], p < 0.001; path A in Fig. 4A and Fig. 4B). After controlling for emotional reactivity (path C’ in Fig. 4A), a linear association emerged between empathic disequilibrium toward CE-dominance and lifetime incidence of NSSI (βAB = −0.14, AB estimate = −0.41, 95% CI [−0.66, −0.20]; ba3 = 0.77, 95% CI [0.16, 1.38], p = 0.01).
Discussion
In the present study, we aimed to investigate empathic disequilibrium as a predictor of emotional reactivity, and through that, NSSI in autistic and nonautistic people. We first replicated previous findings of high incidence of NSSI in autistic individuals7,14; an association between EE-dominant empathic disequilibrium, but not overall empathy, with being autistic 3 ; and an association between EE-dominant empathic disequilibrium and emotional reactivity. 1 We further found that in autistic people, empathic disequilibrium was related to greater lifetime incidence of NSSI through emotional reactivity. While these relationships must be interpreted cautiously given their cross-sectional nature, we did not observe this pathway in nonautistic people.
In this study, we replicated the finding that the likelihood of a self-reported autism diagnosis linearly increased with greater imbalance of EE over CE. 3 This corroborates numerous accounts of autistic people telling of empathic emotions that are overwhelming and incapacitating.47,48 As a concept, empathic disequilibrium opposes traditional academic approaches to empathy in autistic people, who have historically been assumed to exhibit impaired CE (the status of EE being more variable). This literature is dogged with inconsistencies across studies and measurement tools, 72 but has unfortunately translated into the common and stigmatizing belief that autistic people lack empathy.48,50 The growing body of literature on empathic disequilibrium challenges this myth, as does our finding that autistic people did not differ, that is, showed no deficits, in overall empathy. Rather, an autism diagnosis was predicted by experiencing the emotions of others to an intense, potentially distressing extent.
Broadening our understanding of the links between empathic disequilibrium and autism, we observed that in autistic people, empathic disequilibrium toward EE-dominance was associated with greater emotional reactivity. This finding, recently seen in nonautistic people, 1 is reflective of the typical dynamic interplay between empathic processes during social interaction. Where cognitive understanding of another’s emotions serves to down- or upregulate an empathic emotional response to said emotion,37,38 this regulatory process would be less effective in individuals with stronger EE than CE, who regardless of their empathy levels might instead experience hyperarousal due to the relatively lower cognitive understanding of those emotions. In this regard, reflecting the imbalance between EE and CE, empathic disequilibrium may be an index of empathic emotional reactivity and/or dysregulation, as indeed suggested by previous studies linking empathic imbalance and functional underconnectivity with anxiety.1,73
While these findings are preliminary, it may be possible to gain additional insights into potential mechanisms underlying NSSI in autistic people through the link between empathic disequilibrium and emotional reactivity. Specifically, we showed that imbalance toward EE-dominance was, through heighted emotional reactivity, associated with greater lifetime incidence of NSSI. It is possible that difficulties with empathic emotion regulation, as seemingly manifested here in empathic disequilibrium, are a reflection of general difficulties with emotion regulation, which have been linked with NSSI in autistic people. 13 However, it is also possible that empathic emotion regulation difficulties compound or are additive to effects of interpersonal emotion regulation difficulties on mental health. Another step in a causal chain may lie in the difficulties in interpersonal situations, which can arise as a result of the hyperarousal associated with EE-dominance.2,3 While there are still few firsthand accounts of NSSI in autistic people, we know that interpersonal conflict and the person’s perception of having made interpersonal faux pas can be close proximal triggers for NSSI in nonautistic people. 74
Interestingly, we found that a different model emerged in nonautistic people, suggesting differences in the mechanisms leading up to NSSI. While EE-dominant empathic disequilibrium was associated with emotional reactivity as in autistic people, this was also true of the overall empathy in nonautistic people: moreover, in this group, only overall empathy, not EE-dominance, was indirectly associated with NSSI through the mediator of emotional reactivity. While empathic disequilibrium showed no direct association with NSSI in nonautistic people, controlling for emotional reactivity as a mediator revealed an additional effect, though, where empathic disequilibrium toward higher CE was directly associated with NSSI. We showed in previous research that empathic disequilibrium toward CE was associated with cognitive autistic features (such as detail orientation),2,3 to depression, and to psychopathic traits. 1 Interestingly, a similar relationship between CE-dominance and psychopathic traits was masked or suppressed by emotional reactivity, 1 just as controlling for emotional reactivity in the present data revealed the relationship between CE-dominance and lifetime NSSI in nonautistic people. This suggests that for nonautistic people, experiencing understanding of others’ emotions accompanied by a dampened emotional response might be related to distress and feelings of disconnectedness, which may act as an alternative pathway to engaging in NSSI. While this explanation requires further investigation, it would appear consistent with associations observed between feelings of loneliness, desire to avoid social contact by being alone, and NSSI.18,75
While they might shed light on precipitating or risk factors for NSSI in autistic and nonautistic people, these preliminary findings and interpretations require replication and extended exploration in longitudinal designs, particularly given that NSSI can itself exacerbate psychopathology, emotion-related and interpersonal difficulties.5,76 However, our findings invite broader speculation on how empathic processes, most notably interpersonal emotion regulation, might relate to NSSI and possibly to other aspects of psychopathology traditionally linked to intrapersonal emotion regulation, such as disordered eating and substance use.4–6,77 They are supportive of previous suggestions that the way autistic people experience their own emotions has important clinical implications,78,79 and suggest this importance is extended to the way autistic people experience other people’s emotions, too. This has important social implications, too, in challenging the idea that autistic people are not affected by those around them.
Limitations and future directions
While we relied on theoretical considerations when modeling the relationship between empathic disequilibrium and NSSI through emotion reactivity, cross-sectional data cannot point to causal pathways or infer directionality. Therefore, future research would benefit from using longitudinal designs and/or examining how interventions to reduce empathic disequilibrium may ameliorate NSSI. While we attempted to capture empathic processes via self-report, there are many open questions in terms of how these processes operate in real-time. For autistic people, for instance, it is unclear how EE-dominance might manifest: for instance, whether EE processes are faster and/or more automatic than CE processes, and how this might manifest physiologically (for instance, in heart rate and neural activity) and in subjective awareness (e.g., feelings of distress or exhaustion). In addition, our assessment of empathic disequilibrium using current CE and EE measures necessitated relying on nonautistic individuals as a population norm, potentially limiting our inferences. This underscores the need for designing direct measures of empathic disequilibrium. Experimental approaches might also afford better understanding of the dynamic interaction between empathic processes in day-to-day, ecologically valid interpersonal contexts. Qualitative, creative, and/or participatory approaches, too, would afford understanding of the phenomenological experience of having relatively stronger EE than CE. While empathy has been a topic of considerable discussion within the autism and autistic community,47–50 what it feels like to experience another person’s emotions and the perceived impact and repercussions of that experience have not been the focus of targeted investigation. Such an investigation should be coproduced from origin, since autistic perspectives would inform how best to access the inner experiences of autistic people.
As pertains to the operationalization of our key variables, only the PHQ-9 has been validated in autistic people. 65 While there is little psychometric information about the IRI’s properties in autistic people, a recent COSMIN review suggests the measure emerges as superior to other commonly used scales in this population. 58 The ERS has not been validated in autistic people, and there is theoretical debate with regard to the separability of emotion reactivity and emotion (dys)regulation. 80 Similar to other scholars, we adopt a theoretical stance where being emotionally reactive is synonymous to being emotionally dysregulated (and hence pertinent to the literature connecting NSSI and emotion regulation), but we did not measure emotion regulation or attempt to differentiate the two. Moreover, the ERS provides an index of general emotional reactivity across contexts, while we link empathic disequilibrium, conceptually, to interpersonal emotional reactivity (and regulatory processes). At present, there is no validated means to operationalize empathic emotion reactivity and/or regulation, or to distinguish these interpersonal from intrapersonal processes; their relationship to one another is a critical query for future research.
In relation to NSSI, we used the NSSI-AT, a scale derived from bibliographic review and interviews with self-harming individuals and experts. While it has not been validated in autistic people, there has been a broader lack of focus on validating instruments to assess NSSI, with the same true for this scale. 81 This issue may be particularly pertinent to sections of the NSSI-AT not used in this study, such as the section assessing the functional purpose of NSSI behaviors. In relation to this, our index of lifetime incidence incorporated all lifetime NSSI behaviors, regardless of their functional purpose. Our model, in contrast, approached NSSI through the lens of emotional mechanisms. While our findings are supportive of emotion regulation as a major driver of NSSI,28,29 there are other motivations for NSSI and hence some forms of NSSI where the reported relationships may not apply. There is need to develop rigorous means of assessing the forms and functional purposes of NSSI in autistic people, a need that highlights how little we still know.
Unfortunately, we were unable to confirm or validate diagnoses in our autistic sample. Certain individuals within the autistic community were excluded, most notably those who self-identify but are not yet diagnosed, those with severe intellectual and/or communication impairments, and those with low computer-literacy and/or who did not have had access to electronic devices to complete the study (also excluded from the nonautistic group). Certain minorities were underrepresented, including autistic people of color, nonbinary, and transgender people; indeed, we did not try to understand empathic differences that might exist between autistic people of different sexes and genders. Our autistic sample was highly qualified, as is typical of sampling from online channels but not highly representative of the whole autistic community. 82 In that most autistic participants were diagnosed as adults, their profile was likely that of individuals with fair-to-strong camouflaging abilities, those who often exhibit higher than population average executive function and language skills. 83 While there is evidence to suggest that NSSI may be particularly common in late-diagnosed autistic people, 84 our findings concerning NSSI in these participants may not generalize to NSSI, which occurs in other autistic people.
Our nonautistic participants were well-matched to autistic participants for age and sex, but there were several potential confounding variables that might have contributed to differences between groups. While we controlled for depression, we did not control for other psychiatric conditions that might have affected the empathic processes or contributed to differences between autistic and nonautistic people. Although a form of neurodivergence rather than a psychiatric condition, ADHD has also been linked with empathic differences. 85 Given the high co-occurrence of ADHD and autism, we screened out nonautistic participants with diagnosed ADHD so that we might reduce the likelihood of including undiagnosed autistic people in our “nonautistic group”; in not applying the same exclusion criteria to the autistic group, we may have introduced an uncontrolled difference between groups that could have influenced the findings.
In general, differing recruitment approaches to autistic and nonautistic groups should be avoided. While Prolific compares favorably with other online platforms,86,87 our nonautistic participants might not represent random sampling from the general population, especially given our partial use of a purposive approach for individuals with experience of NSSI. While we did manage to recruit a small proportion of nonautistic individuals who engaged in NSSI through general advertising, the purposive approach seeking NSSI experience would be expected to draw participants with more extreme forms of NSSI, who would accordingly be expected to have greater lifetime psychopathology and suicidality. Within a bimodal nonautistic self-harming group, purposively recruited individuals could hence bear greater resemblance to autistic participants in NSSI behavior and correlates of the same. That we still observed different relationships between NSSI and empathic processes in autistic and nonautistic groups suggests that the presence of two subgroups within the nonautistic group did not affect these main findings, but we cannot rule this out.
Finally, we were unfortunately unable to implement a more participatory design due to funding and time constraints. While the research team did include autistic people, future research in this area should ideally be collaborative and coproduced with autistic people from more diverse backgrounds.
Conclusions
Our study investigated the links between empathic disequilibrium and NSSI in autistic and nonautistic people. The findings suggest that there are different mechanisms underpinning NSSI in autistic and nonautistic people, although the findings require replication in directional designs. Nonetheless, these findings challenge the stereotype of autistic people as unempathetic, suggesting instead that autistic people experience emotional hyperarousal in response to the emotions of others; moreover, that the greater the empathic imbalance toward emotional empathy, the more hyperaroused they are and through that more vulnerable to engaging in self-injury. Given the paucity of empirical literature concerning the way that autistic people experience the emotions of other people, our findings suggest this may be of relevance to psychopathology in this as well as other groups. More broadly, they corroborate the importance of emotion processes, which are typically only considered through an intrapersonal lens, to psychopathology in autistic and nonautistic people. Interpersonal emotion processes may bear relevance not only to NSSI but also to other difficulties associated with emotional dysregulation.
Footnotes
Acknowledgments
The authors gratefully thank the participants for their time, and thank the institutions for the internal funding that made this work possible.
Author Disclosure Statement
R.L.M. is a deputy editor at Autism in Adulthood. Otherwise, the authors have no financial or nonfinancial competing interests.
Funding Information
The study received internal institutional funding granted to R.L.M. and F.U.
Authorship Confirmation Statement
All four authors contributed to the conceptualization of and resources for the study and reviewing and editing the article. I.S. and F.U. developed the methodology and I.S. was responsible for software and programming. R.L.M., F.U., and I.S. were responsible for investigation and visualization of results. R.L.M. and I.S. curated the data, conducted formal analysis, and wrote the original draft. R.L.M. and F.U. were responsible for funding acquisition and project supervision and administration. All authors read and approved the final article. The article has been submitted solely to Autism in Adulthood.
Availability of Data and Materials
Participants did not provide consent for data to be hosted in publicly available repositories. However, data, codes, and materials are available on reasonable request.