
Abstract
Abstract
Background:
The 2010 Cochrane Collaboration Review reported laser acupuncture as being effective in depression. The treatment was on LR 8, LR 14, CV 14, and HT 7 over 12 sessions within a 2-month period.
Objective:
The aim of this study was to investigate the biological plausibility of low-intensity laser acupuncture as an antidepressant treatment.
Design:
Randomized stimulation with a fiber-optic infrared laser on these acupoints and KI 3 acupoint. We used a blocked design, alternating laser and placebo laser/rest blocks, while the blood oxygenation level-dependent (BOLD) fMRI response was recorded from the whole brain on a 3T MRI scanner.
Setting:
This study took place at the research institute.
Subjects:
Ten subjects were studied, as confirmed by the Hamilton Depression Rating Scale (HAM-D17).
I
Main outcome measures:
Significant brain patterns for each acupoint greater than the other acupoints and placebo.
Results:
Each acupoint laser stimulation condition resulted in a different activation size and pattern of neural activity. Regions with significantly increased activation and deactivation compared to placebo included fronto-limbic-striatal brain regions. There was no significant activation or deactivation with KI 3. Blinding was afforded with the block design and the infrared laser.
Conclusions:
There is positive biological evidence to support the empirical evidence for laser acupuncture in the treatment of depression. With its minimal adverse effect profile and ease of application, laser acupuncture should be included in depression management strategies.
Introduction
The first foray into the use of acupuncture in the treatment of depression was the investigatory work on electroacupuncture.6,7 These earlier studies were followed by clinical studies from 1998 when the use of manual needle acupuncture in depression was revisited. 9 In a randomized controlled needle acupuncture study using acupoints relevant to mood, as well as secondary acupoints tailored to individual subjects, it was found that acupuncture in depression was better than placebo. However, the effect was transient, with depression recurring at 6 months. 10 Needle acupuncture was as good as pharmacotherapy, albeit with a better adverse effects profile.7,8 Adverse effects are the main reason for patients' noncompliance, and the recent literature reflects this, with only 7.7% of patients benefiting from pharmacotherapy. 14 The fact that acupuncture has fewer adverse effects is indeed encouraging, and further investigation is needed to consider it as another treatment option for depression, alongside pharmacotherapy, cognitive behaviour therapy, and supportive counselling. Three systematic reviews on acupuncture in depression were inconclusive on the efficacy of needle acupuncture in depression.15–17 By 2010, enough literature had accumulated for the Cochrane Collaboration to review all acupuncture studies on depression. 4 All except one were needle acupuncture studies, with one double-blind, controlled study that examined laser acupuncture reporting a highly significant positive effect of the treatment. 11 The Cochrane review concluded that there was insufficient evidence for the use of acupuncture in depression. It is noteworthy that none of the studies reviewed was supported by neuroimaging.
If acupuncture is to be established as an evidence-based treatment for depression, it is necessary to document that acupuncture results in brain effects in regions considered important in the regulation of emotion. We recently reported on the brain effects of low-intensity laser stimulation of four acupoints, traditionally used in Traditional Chinese Medicine (TCM) for the treatment of depression, in a sample of healthy subjects. We showed that such stimulation did lead to activation of brain regions that made it biologically plausible as an antidepressant treatment. 18 In this paper, we extend these findings to a depressed group. We also included the acupoint KI 3, frequently used for anxiety, insomnia, and fatigue in TCM, since these symptoms are often present in depressed patients. We used laser rather than needle acupuncture for this investigation because of the greater acceptability of the former by patients, and the ease of blinding with laser stimulation because of the lack of a skin sensation in laser acupuncture.
Methods
Ethics Statement
Sydney and Illawarra Area Health Service and participants provided written informed consent before participation.
Subjects
Subjects aged 18–50 years were recruited by online advertisement at the University of New South Wales and Prince of Wales Hospital Randwick and by paper notice at the private clinic on the North Shore in Sydney over a 3-month period. Inclusion criteria were that patients should meet the DSM IV criteria for major depression; 19 have scores of >12 on the self-reporting Beck Depression Inventory (BDI); 20 have scores of >14 on the clinician-rated Montgomery and Asberg Depression Rating Scale (MADRS); 21 have scores of >10 on the Hamilton Psychiatric Reporting Scale (HAM-D); 22 have suffered from depression for less than 2 years; and be able to give informed consent. The potential subjects underwent the self-reporting BDI first prior to clinician interview by IQS and/or PS. Inter-rater reliability was estabished at the commencement of the study. All subjects were right-handed. Exclusion criteria were a history of alcohol abuse; psychotropic medication or mood-related herbs such as St John's Wort taken within the previous month; presence of neurological or other major physical illness; or diagnosis of another psychiatric disorder. Any contraindications to MRI (pacemaker, ferromagnetic implants or foreign body, claustrophobia) were exclusionary.
Sample Size
The sample size was set at n=10 subjects comparative to our healthy subjects LA and fMRI study. 18
Choice of Acupoints
The acupoints were selected for their relevance to mood disorders according to TCM. 23 These acupoints lay on the classically named Liver (LR), Heart (HT), and Conception Vessel (CV) meridians. The selected points, labeled LR 8 on the left, LR 14 on the right, HT 7 on the left, CV 14 in the midline, and KI 3 on the right, are shown in Figure 1. LR 8 is in the left medial knee region, between the insertions of the sartorius and semitendinosus muscles. LR 14 is in the vicinity of the right 6th intercostal space on the mid-clavicular line. HT 7 is at the left wrist crease, in the vicinity of the radial side of the flexor carpi ulnaris. CV 14 is in the anterior midline, approximately 5 cm below the xiphisternum. KI 3 is located midway between the centre of the right medial malleolus and the Achilles tendon. 24
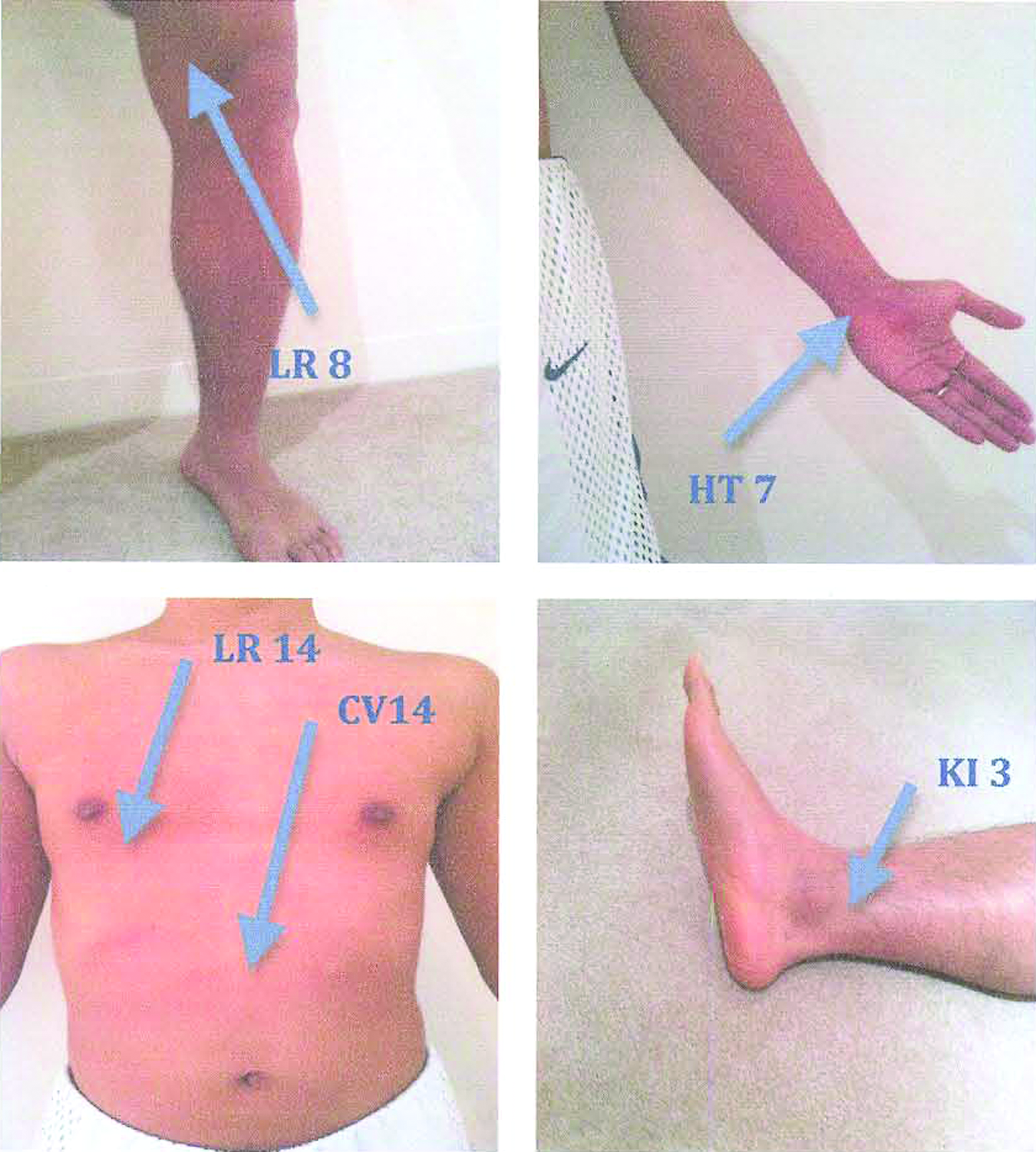
Location of acupoints.
Liver (LR) channel is used for internalized emotions, frustration, and depression. It is also useful for increasing vitality in fatigue patients. Liver Qi Stagnation and Liver Fire are two likely TCM diagnoses for depression. As the depression progresses, Liver Qi deficiency sets in. LR 14 is the front mu or alarm point of the Liver channel, which is used when rapid recovery is required. LR 8 is the water point of the Liver channel and is helpful to quell Liver Fire.
CV 14 is the front mu or alarm point of the Heart (HT) channel (i.e., the emotional heart in TCM). It is a sedating or calmative point. It is also useful in noncardiac pectoral pain and other somatic changes with depression that involve the chest and abdomen.
HT 7 is the sedation point of the Heart (HT) channel. It is often used for patients in distress to calm them down, for example to help them to drop off to sleep at night. It is used in depression, mood swings, indifference, or amotivation.
KI 3, the source point of the Kidney channel, was included to manage fatigue likely to be secondary to sleep disturbances, and also any anxiety component from the depression.
fMRI design
A block design (Active-Sham-Active-Sham) was used, with each block being of 24 seconds duration during which the subject received either laser stimulation (switched on) or placebo stimulation (switched off) at one acupoint. The 24 seconds included 2 seconds built-in time delay for laser safety, 2 seconds TR or rest time, and the actual active laser stimulation or sham laser (laser switched off) block of 20 seconds. The infrared laser was held with a light touch on the skin surface by the acupuncturist. Since the low-intensity laser produces no sensation, it was possible for the subject to be kept blind to the phase of stimulation. The on–off cycle was repeated four times for each acupoint (LR 14, LR 8, CV 14, HT 7, KI 3). Eleven runs were performed, with the five acupoints being tested twice in random order after a dummy run. Subjects were told to relax and keep their eyes closed whilst in the scanner.
Laser Stimulation
A Moxla® prototype fiber-optic infrared light laser (Euryphaessa AB, Stockholm, Sweden; 808 nm) with 25 mW capacity and a fiber-optic arm was developed for use in the scanning room. The laser parameters were similar to the one used in our previous fMRI study. 18 The acupoints were carefully circled with a skin-marking pencil (circumference slightly larger than the laser probe) prior to entry into the scanning room. A stably held laser was applied to the skin by the acupuncturist (IQ-S) who moved it from point to point according to the time signal. The switching on and off was achieved with a computer signal time-locked to the MRI acquisition. In the first round, each run had 25 mW×20 seconds of laser energy delivery (0.5 J) and each acupoint received four active laser runs (0.5 J×4=2 J). In the second round, the procedure was repeated (another 2 J). The total energy delivered was 4 J per acupoint per subject.
fMRI
Imaging was performed on a 3T Philips Intera MRI scanner (Philips Medical Systems, Best, Netherlands) for both T1-weighted 3D structural and BOLD contrast functional MRI. The 3D structural MRI was acquired in sagittal orientation using a T1-weighted TFE sequence (TR/TE=6.39/2.9 ms; flip angle=8; matrix size=256×256; FOV=256×256 mm; slice thickness=1.0 mm), yielding sagittal slices 1.0 mm thick and an in-plane spatial resolution of 1.0 mm×1.0 mm, producing an isotropic voxel of 1.0 mm×1.0 mm×1.0 mm. A gradient echo-planar imaging (EPI) technique (TR/TE=2000/40 ms; matrix size=128×128; FOV=250 mm×250 mm; in-plane pixel size 1.953×1.953 mm) was used to acquire T2-weighted BOLD contrast fMRI in axial orientation. The whole brain was covered using 21 slices at 5.0 mm slice thickness and 0.5 mm gap for each volume. Each session of 96 volumes were collected at the rate of 2 s/volume.
Image Preprocessing and Statistical Analysis
Imaging data were analyzed using statistical parametric mapping (SPM2; Wellcome Department of Cognitive Neurology, London, UK) implemented in Matlab R2007b (Mathworks Inc., Natick, MA). All volumes were realigned spatially to the first volume and the time-series for voxels within each slice realigned temporally to acquisition of the middle slice. Resulting volumes were normalized to a standard EPI template based on the Montreal Neurological Institute (MNI). The normalized images were smoothed with an isotropic 8 mm full-width half-maximal Gaussian kernel. The time-series in each voxel were highpass-filtered to 1/120 Hz to remove low-frequency noise.
Statistical analysis was performed in two stages, assuming a random effects design. Each stimulation site was compared to the placebo (laser off) condition for first level analysis. The BOLD response to the laser acupuncture stimulation was modeled by a canonical hemodynamic response function (HRF), which is the mathematical derivative of the change in cerebral blood flow as measured by the Blood Oxygen Level Dependent (BOLD) signal as a response to the laser acupuncture intervention. The second level analysis (ANOVA) used each individual subject's contrast images, which were effectively the statistical parametric maps of the t-statistics for each voxel. The data had a threshold of P<0.001 with a spatial extent of 15 contiguous voxels.
Results
The Sample
Ten subjects were recruited (five women, five men). Their mean age was 43.7 years. Mean scores for the psychological measures were HAM-D (18.5), MADRS (21.0), and BDI (22.8). Six subjects were acupuncture naïve, and the other four had had needle acupuncture previously but not in the last 3 months. None had ever had laser acupuncture.
Individual Analysis (Level One)
There was much inter-individual variability for all the acupoints. HT 7 classically is an important acupoint in treating emotional distress. We observed that HT 7 stimulation resulted in wide brain regions' activation and deactivation in some subjects who had the TCM tongue diagnostic sign of “heart fire” (very red tip of tongue) likely as a brain response to this emotional distress. This was not found in the other subjects.
Group Analysis (Level Two)
At the group level, there were significant increases (activation) in BOLD levels in brain regions for each acupoint (LR 8, LR 14, CV 14, HT 7) when compared to all the other acupoints (verum laser per point>all others acupoints, P<0.001; Table 1). Further, there were also significant decreases (deactivation) in BOLD levels for each acupoint compared to all the other points (all other acupoints>verum laser per point, P<0.001; Table 1).
x,y,z coordinates, KE, and Zscore for the depressed subjects are also displayed.
LR 8
The right frontal cortex (precentral gyrus), right parietal cortex (postcentral gyrus), left temporal cortex (middle temporal cortex), and occipital cortex (bilateral lingual gyrii, right cuneus) were activated. Deactivation was at the frontal cortex (left inferior and middle frontal gyrii), temporal cortex (left middle temporal gyrus), and left subcortical lentiform nucleus (globus pallidus; Fig. 2).
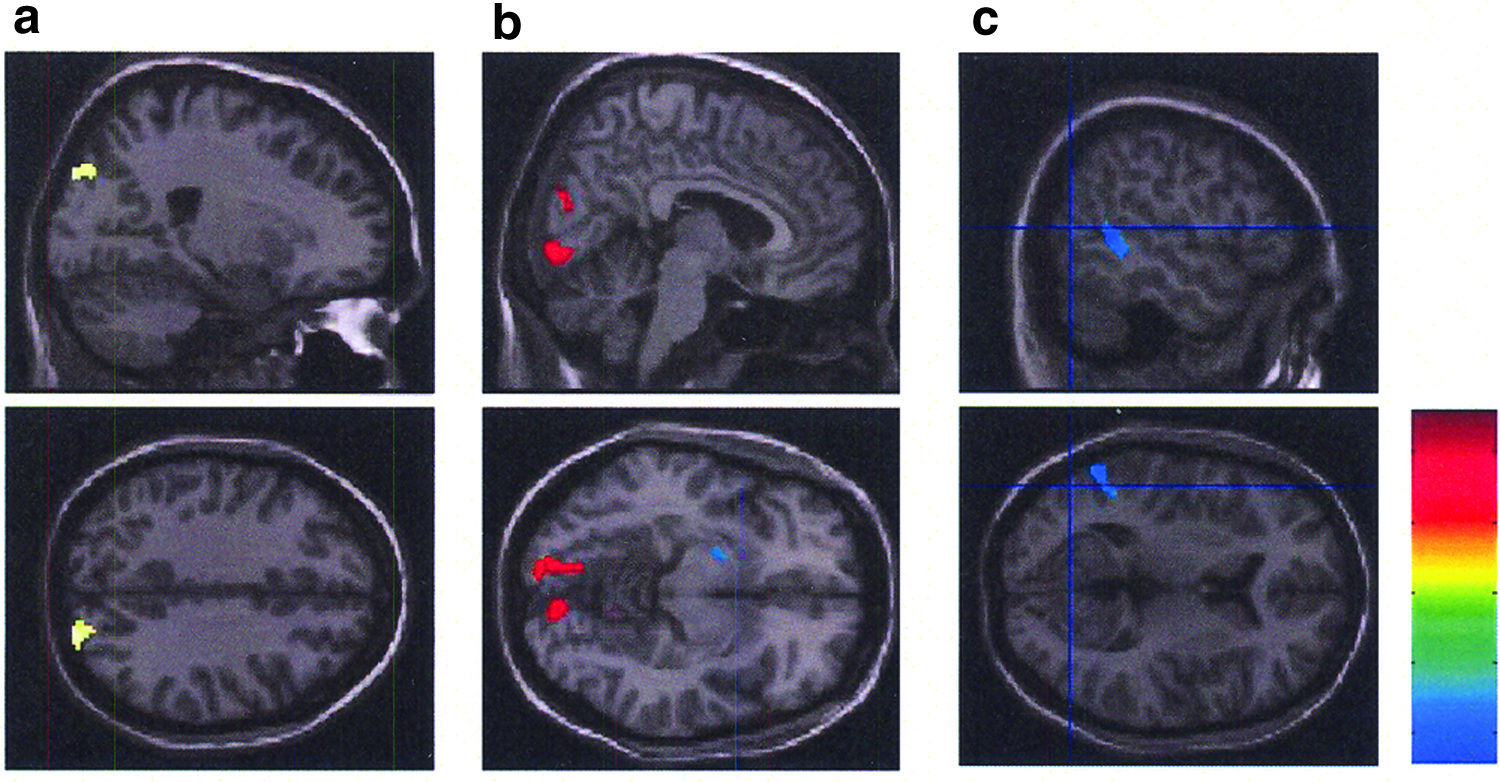
LR 8 brain patterns during laser acupuncture on LR 8 in major depressed subjects. (
LR 14
The temporal cortices (right superior temporal gyrus, left inferior temporal gyrus), frontal cortex (left middle frontal gyrus) and right parietal cortex (inferior parietal lobule) were activated. Deactivation was at the temporal cortex (bilateral superior temporal gyrus) and limbic cortex (left cingulate gyrus; Fig. 3).
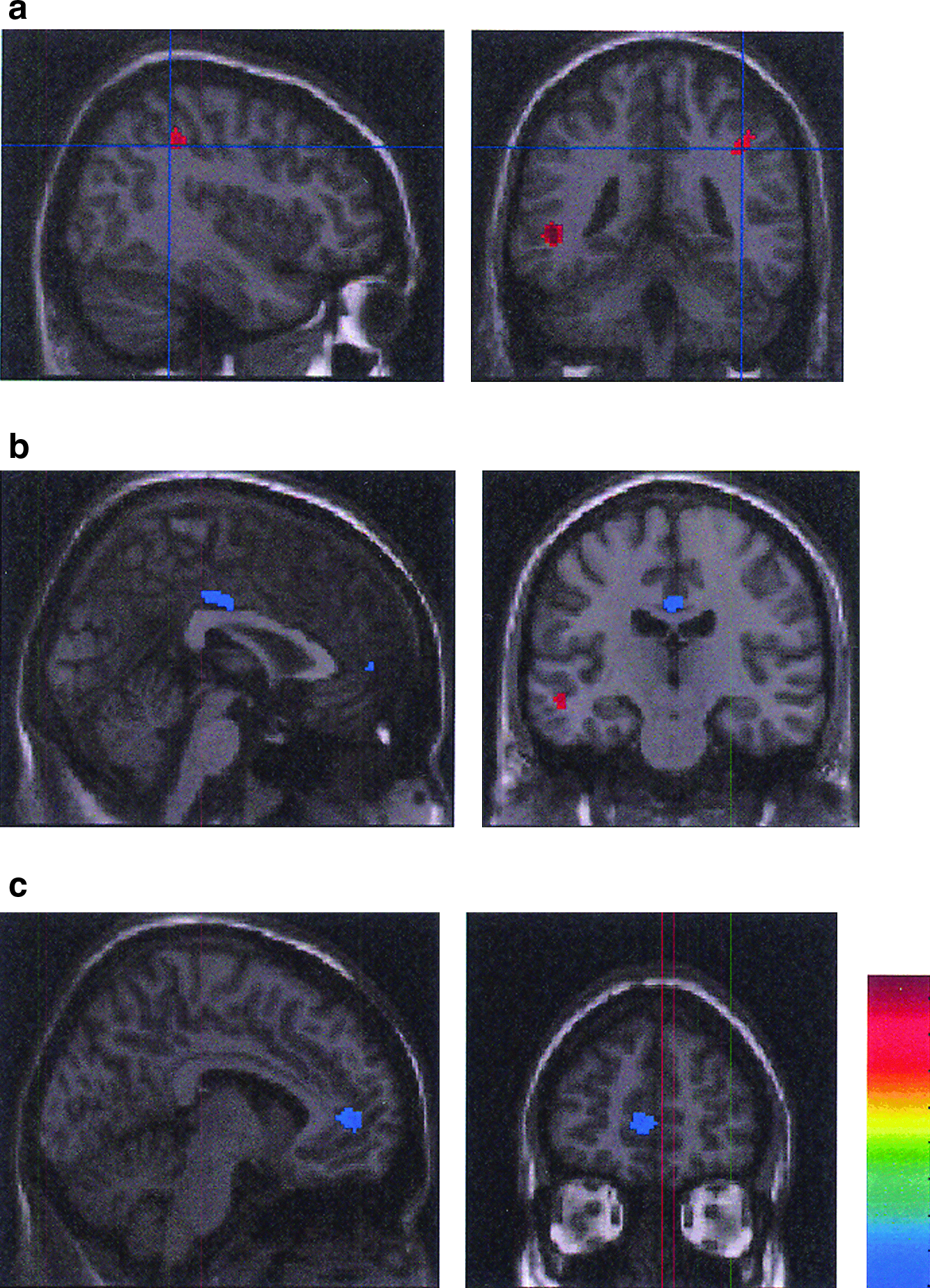
Brain patterns for laser acupuncture on LR 14 in major depressed subjects. (
CV 14
Activation was at the temporal cortex (bilateral middle temporal gyrus, right superior temporal gyrus), limbic cortex (right parahippocampal gyrus), and cerebellum (left culmen). Deactivation was at the temporal cortex (left inferior temporal gyrus; Fig. 4).
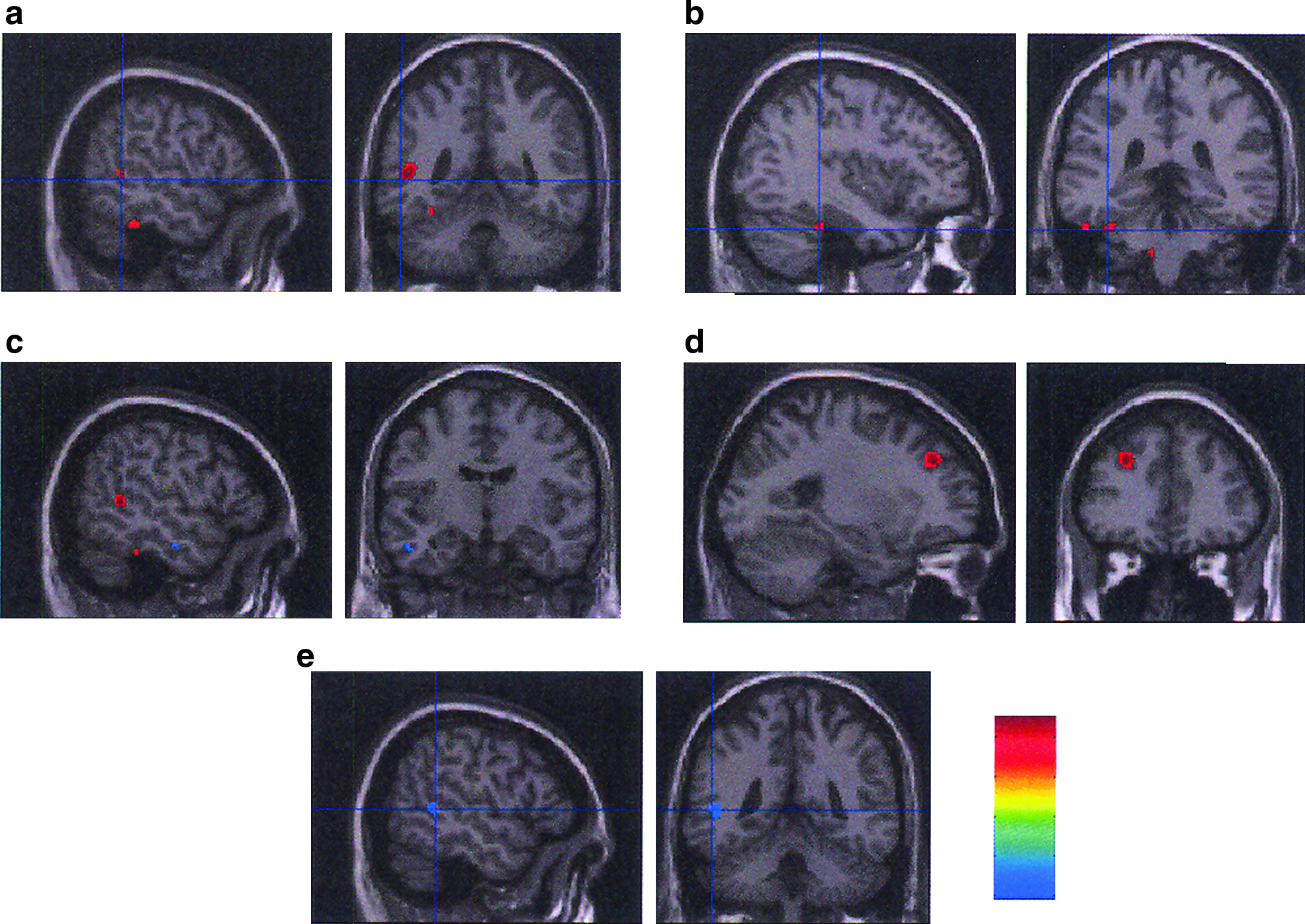
Brain patterns for laser acupuncture on acupoints CV 14 and HT 7 in major depressed subjects. (
HT 7
HT 7 activated the frontal cortex (left middle frontal gyrus). Deactivation was at temporal cortex (left middle temporal gyrus). Activity was ipsilateral (Fig. 4).
KI 3
There was no significant activation or deactivation.
Sensorimotor Cortex and Laterality of Cerebral Activation and Deactivation
There was activation of contralateral postcentral gyrus and precentral gyrus, that is, the sensorimotor cortex, with stimulation at LR 8 but none of the other acupoints. LR 8 and HT 7 were the only limb acupoints to produce brain effects. Laser stimulation at acupoint LR 8 caused bilateral activation and ipsilateral deactivation. Activation and deactivation with stimulation of HT 7 at left upper limb were both ipsilateral. There was no significant activation or deactivation with stimulation of the right lower limb acupoint KI 3.
Discussion
In this study, we examined the brain effects of laser acupuncture on our selected suite of acupoints that follow TCM principles and which have also been empirically tested in our depression and laser acupuncture pilot study. 11 We demonstrated that stimulation of acupoints LR 8, LR 14, and CV 14 activated and deactivated many brain regions, including those that are known to be involved in the regulation of mood and which are putative targets in any antidepressant treatment. 18 In particular, these regions were the cingulate gyrus, the parahippocampal gyrus, and the striatum. We also found that laser acupuncture modulated activity in brain regions involved in the default mode network (DMN) also known as resting state network (RSN).
DMN or RSN are the brain regions that are prominent when the brain is not performing a particular task (which is known as task positive, e.g., writing this article or reading this article) but is at rest (also known as task negative). The DMN or RSN is important, as in this “quiet time” much is done within the individual to regulate and coordinate complex neural cascades that also involve the affective (emotional) cortex or so called limbic or paralimbic systems.25–30 Lou et al. referred to these phenomena as “yoga lessons for the brain,” as this DMN or RSN time facilitated regulation of the autonomic nervous system and other neural networks, similar to the whole yoga experience where various postures in yoga lead up to meditation. 30
We have previously reported similar findings in a group of healthy individuals. 18 Table 1 summarizes the findings from the two studies, with the caveat that the two studies, while using the same methodology, were performed at different times, and the comparison is qualitative and not statistical. What is noteworthy is the more extensive network of brain regions affected with acupuncture in depressed patients, including activation of bilateral lingual gyrus and right cuneus with LR 8 and activation of left culmen by CV 14. Highly differentiated cognitive aspects of emotion involving the cuneus and lingual gyrus have been previously explored 31 and attest to the relevance of these findings. That the pattern of activation and deactivation is different in depressed subjects may be related to the baseline state-dependent level of activation. Functional brain imaging studies, while not consistent in their findings, reveal a network of brain regions that are hypoactive at rest, such as the middle frontal gyrus, superior temporal gyrus, anterior cingulate, insula, and cerebellum, and show increased activation with antidepressant treatment.32–35 On the other hand, certain brain regions such as the medial and inferior frontal gyrus, basal ganglia, and possibly the amygdala and thalamus are overactive at rest and showed reduction in activity with treatment. Activation patterns also appeared to be altered in the middle temporal gyrus, posterior cingulate, and cerebellum, but not consistently. The depressed participants in our study showed deactivation in the medial frontal gyrus, the superior temporal gyrus, and the globus pallidus, which is consistent with the likely effects of an antidepressant treatment. While healthy subjects showed activation of the cingulate gyrus, including the posterior region, with acupuncture, depressed patients showed a deactivation of the cingulate gyrus.
While the main regions modulated by acupuncture in both healthy and depressed patients are in the frontal and temporal lobes, depressed patients showed changes in other regions as well. The inferior parietal lobule was activated with the LR 14 acupoint in depression. Altered parietal activation at rest has been reported in some studies of depression. 36 Modulation of activity in the cerebellum with acupuncture on CV 12 and LR 8 acupoints in depressed patients in our study is noteworthy. The cerebellum is considered to be important for the regulation of mood and the perception of emotional stimuli,37,38 and its activation with acupuncture may have relevance to the potential antidepressant effects of this intervention. Moreover, the cortical-cerebellar system had been suggested to be central to the development of neural models important in the longer-term effects of acupuncture on cognitive processes.39–44 If this is the case, our findings suggest a biological mechanism by which acupuncture could produce long-term brain effects.
There may be concerns regarding the small sample sizes in both our fMRI studies. However, sample size is not the only way to increase power. The quality of the data attained, including the signal-to-noise ratio (both temporally and spatially) of the imaging data acquired and noise associated with movement and artifacts and so on, are also very important. The scanning was performed on a 3T scanner with very good spatial signal-to-noise ratio (∼80). Further, thresholding was performed at a cluster level of 15 voxels, which is a common conservative method.
We demonstrated in our 2010 study that control (non-acupoint) points are not inert, and the selected control point significantly activated the right cingulate gyrus and deactivated the left parahippocampus. In extending these findings to a depressed group, our primary investigation was to test significant verum laser activations and deactivations greater than sham laser/rest. It was not our intention to compare again directly the verum acupoint to the control point. Future methodology for laser acupuncture experiments to include or not include a control point is dependent on what the aims of the experiment are, that is, to measure the full acupoint effect centrally (above sham or rest) or to compare the acupoint to control point.
We did not correct for multiple comparisons. At the first level, each condition was subtracted from rest to normalize the conditions. At the second level, each condition was subtracted from all the other conditions (which had also undergone first-level normalization). The analysis was then thresholded using a conservative cluster thresholding of 15 contiguous voxels. We were comfortable that this was a very conservative method. This threshold is greater than the usual 10 voxels used in previous experiments.
Acupoint Specificity
The choice of points on the skin surface that must be stimulated for physiological effects is based on the above-mentioned concepts of TCM, with no equivalence in our current understanding of human physiology. The acupoints chosen for this study therefore had only a tentative theoretical basis, and we cannot argue that these are indeed the best acupoints for a future intervention. Nonetheless, we did find differential activations with the selected acupoints. Stimulation of the acupoints LR 8, LR 14, and CV 14 altered activity in many brain regions relevant to mood, whereas HT 7 produced activation of middle frontal gyrus and deactivation of middle temporal gyrus only. HT 7 did not have any significant brain effects in our previous work on healthy subjects. The concept of acupoint specificity per condition has been tested previously.45–49
Classically, any acupuncture treatment has primary acupoints (essential for the condition) and secondary acupoints (helpful but not essential for the condition). Little biological evidence has been recorded in support of the above. In the present study, we have shown that some acupoints may well be of primary significance in depression. The KI 3 acupoint, which was included to treat anxiety present in the depressed subjects, did not have any significant brain effects. While these results hold true for this sample only, another depressed sample with more prominent anxiety features may well find KI 3 stimulation produces significant brain effects, thereby suggesting a secondary role to this acupoint. Further fMRI studies with larger samples are required to test these classical concepts.
Laterality of Stimulation and Sensorimotor Cortical Stimulation
Lateralization of limb acupoints appeared to be inconsistent and not predictable across the group. The trend for ipsilateral brain activation by acupoints on upper and lower limbs recorded in other laser studies on healthy subjects18,50,51 did not hold true for this depressed sample. It is possible that under the condition of depression, central modulation by low-intensity laser acupuncture resulted not only in more regions being stimulated but the activation was also bilateral. Needle studies describe consistently the involvement of the sensory cortex.13,40,41,52–54 As the low-intensity laser has non-nociceptive properties, activation of the primary somatosensory cortex was not recorded for all acupoints except LR 8, which was stimulatory of primary sensory and motor cortices. The significance of this is not known. A thorough investigation of the afferent fibers carrying the low-intensity laser signal of the acupoints utilized may shed light on this differentiation.
Modulation of the Default Mode Network
The resting brain has intrinsic brain activity now commonly referred to as the task-negative Default Mode Network (DMN). During this resting state, recall, thoughts about the future, and thoughts about alternatives to current situations may occur.27,55 Acupuncture has been recognized as being modulatory of the DMN.17,29,30,55–57 In this study, we have evidence of DMN modulation by low-intensity laser acupuncture, and there is emerging evidence regarding the role of the DMN in depression.30,55 It is possible that modulation of the DMN may be one mechanism by which acupuncture produces its antidepressant effect.
This study extends our previous work in healthy subjects and shows that laser acupuncture in depressed patients produces activation or deactivation of brain regions and modulation of the DMN that are potential mechanisms for an antidepressant effect, making laser acupuncture a plausible antidepressant treatment. The study provides a rationale for further empirical investigation of laser acupuncture as a treatment for depression in a randomized controlled trial. The ease of blinding with the laser makes it an ideal tool for such an investigation.
Conclusion
There is positive biological evidence to support the empirical evidence for laser acupuncture in the treatment of depression. Due to its minimal adverse effect profile and ease of application, laser acupuncture should be included in depression management strategies.
Footnotes
Acknowledgments
Thank you to all those at POWMRI (now known as NeuroScience Australia [NeuRA]) for their help and encouragement, Olivier Rochesson and Peter Jenkins for their technical expertise, Chao Suo for assistance with DMN analyses, and Angie Russell for her help with manuscript preparation.
Poster Presentation—Quah-Smith I, Wen W, Williams M, Sachdev P. Third International Congress of Complementary Medicine Research, 29–31 March, 2008, Sydney Convention Centre, Darling Harbour, Sydney, Australia. This poster presented an fMRI record of LA for HS vs. MDD showing TCM principles of “excess” and “deficiency” correlating well with the autonomic nervous system using fMRI. It won best scientific poster at the 2008 ICCMR conference.
Disclosure Statement
No competing financial interests exist.