
Abstract
Introduction:
Mind–body approaches are flourishing to answer the need for support in an increasingly demanding world. To provide scientific evidence of their effectiveness and contribute to the discussion on the role of the body in the effects of these approaches, we carried out a field survey on one such approach, somatic psychoeducation (SPE), with assessments focused on anxiety and self-esteem.
Materials and Methods:
An observational multicentric longitudinal study was conducted on SPE clients (N = 114) before and after a series of 10 SPE sessions freely implemented by practitioners (n = 25) in the field of their own practices. A one-off external group served as reference.
Results:
SPE had two major effects: one is immediate, as one session lowered anxiety state by 30%; the other is in the long term, as anxiety trait decreased by 6.2 points at the end of the intervention, and self-esteem improved by 3.5 points. The absence of a practitioner effect allows us to generalize the results to the practice as a whole.
Conclusion:
The beneficial responses obtained simultaneously on anxiety and self-esteem after a 10-session SPE follow-up are of interest and are discussed, as they suggest possible behavioral changes. We attribute these results to the combined action of bodily experiencing and the enrichment of self-perception. Thus, our results open up new perspectives for mind–body approaches in the context of well-being and preventive health care.
Introduction
Depression and anxiety are recognized scourges of our times. 1 When chronic, they can lead to a deterioration in well-being, and can be accompanied by altered affects even before mind and body impairment occur.
Following the increase in preventive health care approaches in the 1970s, 2 diverse personal development practices emerged and became widely used for excessive stress and anxiety regulation, particularly in nonclinical contexts. Studies on their actual impacts show beneficial effects on both positive and negative affect, particularly anxiety and self-esteem. 3 –12
Differential psychology considers both self-esteem and trait anxiety as personality traits that are stable for up to seven years. 13 These traits are closely linked: a good stable level of self-esteem has beneficial effects on the overall health and quality of social and personal life, as well as on anxiety and depression. 14 When an individual feels threatened, the resulting anxiety depends on the individual's level of self-esteem and not on the perceived threat. 15 Today, self-esteem is even believed to act as a secondary indicator of anxiety, that is, a consequence of the alteration of the main marker of anxiety. 16,17 Mu et al. 18 talk about surface characteristics as opposed to core characteristics, which include anxiety. Self-esteem, given its delayed response to changes in core characteristics, would then be ultimately a kind of by-product. 18 However, when a high level of self-esteem is combined with a high level of trait anxiety, it is generally described as unstable and authors suggest that this may be a narcissistic issue, 17 which can be accordingly treated when pathological.
Although defined as stable in time, these two traits have been shown to fluctuate and modulate over time, both naturally and in induced ways, suggesting potential for the development of intervention, assistance or support programs. 17 –24 There is still a need to better understand how these two traits change in relation to each other, considering the fact that they do not follow the same fluctuation patterns over time 19,20 or when facing life difficulties. 25
We believe that the body plays a major role in the link between self-esteem and anxiety. The body has been repeatedly demonstrated to be a relational organ, the locus of self-perception and of the relationship with the self, the substrate for experience and emotion. 26 –28 In the context of sport, the body is described as a place where external judgments and competitive anxiety are internalized, thus affecting performance and self-esteem. 29 –31 This process of internalization is further enhanced by the role of perceived physical worth in the process of building self-esteem. 26 In contrast, anxiety is known to build on an interaction between mental and physical disorders, which can lead, when overdeveloping, to the invasion of all physical, mental, and cognitive sectors of the person's life, a process called somatosensory amplification. * Under the surface of scientific research while it is being done, Quidu 32 observed how scientists related to their own body while conducting their research. Although reflexivity is acknowledged for the fruitful distance it gives to the events, he noted that as scientists internalized the judgmental feeling of external gazes, their reflexivity could generate anxiety, with associated inhibiting effects on self-esteem. However, with the process of verbalizing, articulating even to themselves, their bodily experience allowed self-esteem to detach itself from the external gaze and be linked to the recognition of one's own competence and reduce the anxious experience. In other words, “feeling one's body in the first person” 26 places the bodily experience as a relevant and beneficial driver, in the process of improving self-esteem and anxiety.
All this feeds into our sense of a cognitive and bodily pathway to act concomitantly on anxiety and self-esteem, as well as our understanding that their simultaneous change can reasonably involve a behavioral change. We investigated these hypotheses on one particular type of mind–body therapy called somatic psychoeducation (SPE).
What Is SPE?
SPE was developed by Professor Danis Bois in the 1980s and belongs in the field of personal development and support practices. It is a mind–body approach that focuses on tuning perception, feelings, thoughts, intentions, and actions within the person, through a bodily experiential learning process. The tuning pursued is defined as “the tool that the practitioner uses to re-establish the dialogue between the body and the mind. (…) The aim is for the patient to feel a strong sense of unity between all their parts. The parts of the body: top and bottom, front and back, right and left, the back and the face. But above all, the parts of being: intention and action, attention and intention, perception and movement, thought and experiencing.” 33 The proposed framework aims to enrich perception and self-awareness, particularly the immediate perception of lived bodily interiority, favoring the deployment of a presence mindful of the moment, of the self, of others and of the wider world, which facilitates the emergence of new understandings, meanings, or senses of the lived experience. 34,35 Therefore, SPE is chiefly intended for use on individuals who are in search of meaning or who are experiencing personal transition or life difficulties.
SPE has both health care and educational potential and offers four major tools for the practitioner to choose from, depending on the level or nature of the educational progression envisioned: manual relational touch, gestural language, sensorial introspection (full-presence meditation), and verbal dialogue. Each tool allows the practitioner to gradually solicit the person's attention with respect to their perceptual abilities, based on the information that emerges from the bodily experience and on the reflexivity derived from it. 36
Relational touch is the easiest tool and most commonly used to open the person to the sensorial and perceptual dimensions of the bodily experience. It is based upon the mobilization of the physical and psychical tonus of the fascia, which are mostly the soft tissues of the body.
37
To access the subtlety of this multidimensional tone and the information available to their hands, the practitioners must develop specific perceptual abilities: “(The touch) calls upon manual perception skills that go beyond the epicritic sense of touch, which excels in discriminating shape, temperature, texture or weight. The objective (here) is to perceive a very slow motion animating the tissues of the whole human body. Such sensory dexterity is not spontaneous and requires a specific sensory learning for the practitioners unfamiliar with this type of touch. A whole range of new sensations (depth, movement, elasticity, internal tones, fluidity, etc.) gradually appear to the consciousness of the practitioner who discovers the moving, living, and touching interiority of the body. The closeness of this “sensitive” touch then becomes a means of silently weaving an intimate, deeply respectful, and caring dialogue between the two persons.”
38
The relational touch has therapeutic properties that are used in health care contexts. 39 SPE mobilizes it in a comprehensive way for the person's learning and transformative process—although corrective outcomes may occur, as in any nonmanipulative practice, the body remains its own master and the practitioner remains mindful of, and trained to recognize, any such outcome. 34 It may take several sessions for a new patient to access the subtleties and riches of their life within, as a process of perceptual training and perceptual enrichment builds up.
Gestural language has an educational objective of empowerment and self-reliance, and is aimed at “allowing the person to express the silent language” 33 of the inner world discovered through relational touch. It is made up of a series of gestural sequences performed in sitting and standing position, fully involving the person in what they are doing, how they are doing it, and where they are going. The purpose is for the person to learn to perform a set of tasks mobilizing cognition and reflexivity through the sensory perception of the body. Each specific sequence is a set of very simple symmetrical evolving codified gestures, which generate a state of rest, serenity, and balance, conducive to constructive inner reflection. 33 As a primary condition, the motion is slow, of a specific sensorial slowness allowing the person to mobilize their attention on the unfolding of the gesture and to adjust or change its course in real time. Not only does this slowness open the patient's perception up to information unavailable at normal speed, but also it allows the patient, while performing the gesture, both to perceive its sensory effects on their inner life and to access a sense of the globality of the body as coordination of the movement unfolds. It constantly challenges the person to pay attention to new ways of seizing and of accessing the details of each move. Progressively, the person discovers new perceptions of themselves with a renewed sense of self and of presence with the self.
Sensorial introspection is a meditative practice that uses perception as a means to access body and mind experience. Similar to other tools, it addresses bodily sensations of lived experience in a gradual and cumulative manner, to develop awareness and presence in the present moment. The term “sensorial” refers to “a form of inner-body intimacy” that is accessed by observing one's mental and internal states, whether physiological or psychological, through bodily perceptions in a sort of sense-felt observation, before it becomes mental. In other words, it is a seated practice that engages, while remaining still, all the sensory modalities, that is, proprioceptive senses, auditory and visual senses, interoceptive senses, and the “inner touch” of Maine de Biran. 40,41 When explaining this “inner touch” Maine de Biran refers to the inner sensation that gives any living being “the absolute sensation of existence.” He most often casts it as an inner tactile ability to “perceive oneself perceiving” (I feel that I feel), describing it as an “affective touch” or an “immediate touch” that relates “to the various affections of the body without the use of external senses.” 41 Such inner modality is central in the development of self-awareness, body awareness, and the felt sense of embodiment. 10 Sensorial introspection uses verbal guidance that deliberately avoids instructions that could activate mental control. The bases of the protocol are detailed in a study conducted by Lieutaud and Bois. 10
Body-centered verbal dialogue is crucial, and is aimed at learning to describe the experience in a phenomenological manner, that is, as facts of perceptions, of feelings and senses with as little speculation and interpretation as possible. It focuses on what is at play in the course of the session. It helps to keep the person attentive to and present in what is happening in their body in the real time of the experience, including passing feelings and emotions, tensions and memories, particularly when sensations lead to such thin or new perceptions that mental ability may drop and drift away. Overall, its aim is to discover and learn to describe, in the real time of the experience, lived bodily sensations to better appropriate them and gain understanding of the potential meaning they conceal.
SPE efficiency relies on the central place given to perception and to the learning process, that is, on the primacy of perception and bodily sensitivity as pivots of the experiential process. 38 Under the careful attention of the practitioner, the person progressively develops their perceptual abilities, up to a point where they access a peak sense of “penetrating the living interiority of the body,” 42 that is, both the nuances of the tones and feelings of their own body in the immediate moment of the experience, and the paroxysmal dimension of perception that then develops, which is often associated with a “sense of aliveness.” 42 SPE efficiency also relies on two pillars specific to this practice, the inner movement and the supporting point. The expression “inner movement” designates all the movements that are not accessible to an external observer, but can be experienced from an intimate first-person perspective. The inner movement can be understood as the expression of the multidimensional tone of the fascia, modulating altogether the psychological, physiological, and physical dimensions of the living matter. The “supporting point” is very specific to the overall practice at play, that is, a suspension moment where the hands of the practitioner, having stretched the tissues to their optimum tone of tension, both physical and psychological, place a stop in their motion while remaining in full presence in the tissues to allow and support the body to find its own way out. 37 Further information is detailed in Supplementary Data S1.
SPE Support of Affect
SPE has been the subject of scientific investigation since the early 2000s. 34 It seems to positively influence anxiety, as much among healthy adults 43,44 as among the sick. 45 Two studies using Spielberger's scale attest the positive effects of SPE on anxiety. 10,46 With regard to self-esteem, Bouchet 35 observed that after 12 SPE sessions, global self-esteem scores of participants increased by almost 7 points; meanwhile self-esteem was improved, the qualitative interviews revealed that a dialectic was taking place between the positive experience of the body and the affective dimension of self-esteem. A study conducted on young adults with eating disorders indicates that self-esteem reconstructs itself through a relationship to one's interiority based on internal reference points and no longer solely on external physical or psychological representations. 47
Considering SPE's influence on the organic dimension of self-perception, there is a strong probability that SPE acts concomitantly on both self-esteem and anxiety. The assumption of its effectiveness is based on the fact that the technique intervenes ahead of the individual's thoughts through the body's experiential and physical senses, by simultaneously mobilizing the psychological and physical pathways of the bodily experience through the relational touch aforementioned (detailed in Supplementary Data S1). It is also based on SPE's medium-term time frame, on the scale of a few months, making it possible to envisage a perceptual training process that can impact self-esteem and anxiety.
Hypotheses
This study aims at assessing the efficacy of SPE on anxiety and self-esteem using a real-life observational and noninterventional extensive survey. The idea is to verify the aforementioned exploratory results and observe how anxiety and self-esteem change in relation to each other over a medium-term follow-up.
Our major hypothesis is that SPE should improve clients' self-esteem and lower their trait anxiety, after the completion of a medium-term follow-up of 10 sessions further called the “program,” that is, lower trait anxiety and higher self-esteem scores should be found at completion than at the beginning.
We also expect that participants will have, on average, a high initial level of anxiety and a low self-esteem, motivating them to seek support, and that both levels should, at least, “return to normal” at the end of the program. This reference to a “normal” is endorsed by the setup of a reference group (RG) totally independent from the participants.
Materials and Methods
The study was approved by the scientific review boards of our laboratory and university, and was carried out in accordance with the 1964 Helsinki declaration and its later amendments. A dedicated scientific committee was set up to supervise the project. All participants, that is, practitioners, clients and RG members, signed an informed consent before their involvement in the survey. All data were fully anonymized before their digitization.
Participants
Participants (n = 114) were recruited over time by the practitioners among their clients on a voluntary basis, and practitioners were themselves recruited on a voluntary basis through the French federation of Full-Presence practitionersi (see Supplementary Data S2 for details regarding sample size). Inclusion criteria were to be of legal age, to speak French fluently, and to attend individual sessions at the practice's office (i.e., no group sessions and no home visits). From this set of volunteers, 76 completed the entire program, which was sufficient for strong results. They will be further referred to as the “program group” (PG). Because of the long-term unknown duration of our study, a wait-list control group could not be set up. We, therefore, built our reference using an external group whose one-off responses proved to form a reliable reference for the whole duration of the survey (see details in Supplementary Data S3, particularly Tables S3a and S3b). The sociodemographic data pertaining to the SPE clients (PG) and the RG indicate that apart from the physical activity, both groups are similar: mostly female; 50 years on average; equivalent (quite high) level of education (Supplementary Data S4).
Measures
To test our major hypothesis, we measured anxiety and self-esteem using worldwide validated self-reporting scales: the French version of the two-dimensional State and Trait Anxiety Inventory of Spielberger 48 (STAI-Y, excellent internal consistency with our data on both subscales α = 0.917 for state anxiety and α = 0.933 for trait anxiety); the French version of the 10-item Rosenberg Self-Esteem Scale 49 (RSE, very good internal consistency with our data α = 0.878). We also asked participants about their expectations, length of experience with this practice, and life events, using a sociodemographic initial questionnaire and a context questionnaire at each assessment time, thus collecting context information regarding the program (personal mind–body practices, changes in their expectations regarding SPE support, life events, etc.). All questionnaires and monitoring tables are displayed in Supplementary Data S6.
Procedure
A longitudinal (follow-up in time) and prospective (observing pre–post differences) study was designed to allow for temporal relationship analyses.
50
It was organized in a multicentric (each practitioner is a centrum) observational (no change in the practice due to the survey) field survey (questionnaires applied on site), to account for the between-practitioner variability and meet the real-life assessment objective of the study. The program consisted of a follow-up of 10 consecutive SPE sessions spread out over an unlimited period of time (see flowchart and details prevailing to data collection in Supplementary Data S5, and its figure S1), with two main data collection times (the engagement time when the consent form is signed is referred to as T0): T1, the first session of the program, includes two times for answering questionnaires: before the T1 session for context questions and trait and state questionnaires, and immediately after the session for state questionnaires. T10, the last session of the program, also includes two times for questionnaire responses: before the session for context questions and the state questionnaires, and immediately after the session for the state and trait questionnaires.
The average duration of an individual follow-up was 254 days ±108 months that is, 8.5 months ±3 months. Duration seems not to influence the psychometric responses (Analysis of Variance, F STAI-Y2 = 0.559, P = 0.42; F RSES = 1.939, P = 0.149; ρSTAI-Y2 = 0.091, P = 0.436; ρRSES = 0.135).
The SPE Sessions
Each practitioner filled out, for each participant, a monitoring table of each session of the program. We could reconstruct a typical SPE session, which turned out to be remarkably similar among the 25 practitioners who participated in the study: an average session was 62 minutes ±12.5 minutes, the main tool used was relational touch (100% of the practitioners for over 77% of the session duration on average), and all the practitioners routinely used verbal support either during the session or at the beginning/end of the session (8%–20% of the duration of the session on average).
Results
The survey took place between July 2015 and February 2017. Analyses were conducted using descriptive statistics and usual difference-of-the-means and variance tests (see details in Supplementary Data S7). The scores collected are summarized in Table 1. Whenever further mentioned, the levels called “medium,” “high” or “low” refer to Bruchon-Schweitzer's interpretation grids 48 for state and trait anxiety and to Vallières's 49 for self-esteem.
Average Scores (STAI-Y1 and Y2, RSES) with Standard Deviations of the Program Group and the Reference Group (RG), and Between-Group Comparison of the Means at T1 and T0 Using the Hypothesis of RG Scores’ Invariance Overtime
d and 1-β values for significant tests only.
One-off at the end of the survey.
M, mean; PG, program group; RG, reference group; RSES, Rosenberg Self-Esteem Scale; SD, standard deviation; STAI, State and Trait Anxiety Inventory of Spielberger.
Variability Among the Practitioners
Variability among the practitioners was tested using the 41 persons who attended the entire program, and came from practitioners with at least 4 participants each (8 practitioners). There was no significant difference on STAI-Y and RSE values or their before–after differences, either on the scale of a session for state anxiety [post–pre STAI-Y1, F (7,33) = 1.183, P = 0.339] or on the scale of the program (T10-T1), for both trait anxiety [STAI-Y2, F (7,33) = 0.815, P = 0.582] and self-esteem [RSES, F (7,33) = 1.292, P = 0.287]. And there was no difference between the 41-person subgroup and the remaining 35 participants regarding those variables neither at T1 [F preSTAI-Y1(1,74) = 2.48, P = 0.12, F STAI-Y2(1,74) = 0.006, P = 0.937, F RSES(1,74) = 0.032, P = 0.858] nor at T10 [F preSTAI-Y1(1,74) = 1.167, P = 0.28, F postSTAI-Y1(1,74) = 0.337, P = 0.563, F STAI-Y2(1,74) = 0.008, P = 0.929, F RSES(1,74) = 1.486, P = 0.227]. We conclude that there was no detectable difference between practitioners and that the 76 participants who completed the program can be taken as one single homogeneous sample, that is, the PG.
Effects on Anxiety and Self-Esteem
First, there is a within-group (PG) response, that is, an effect from the participant's perspective (Table 2):
Comparison of the Means to Null Value (Bilateral Student's t-Test) of Program Group Scores Before and After Program (T10-T1) or Session (Post–Pre), on the Three Psychometric Variables
T10-T1 on state anxiety (STAI-Y1) was computed using the presession scores.
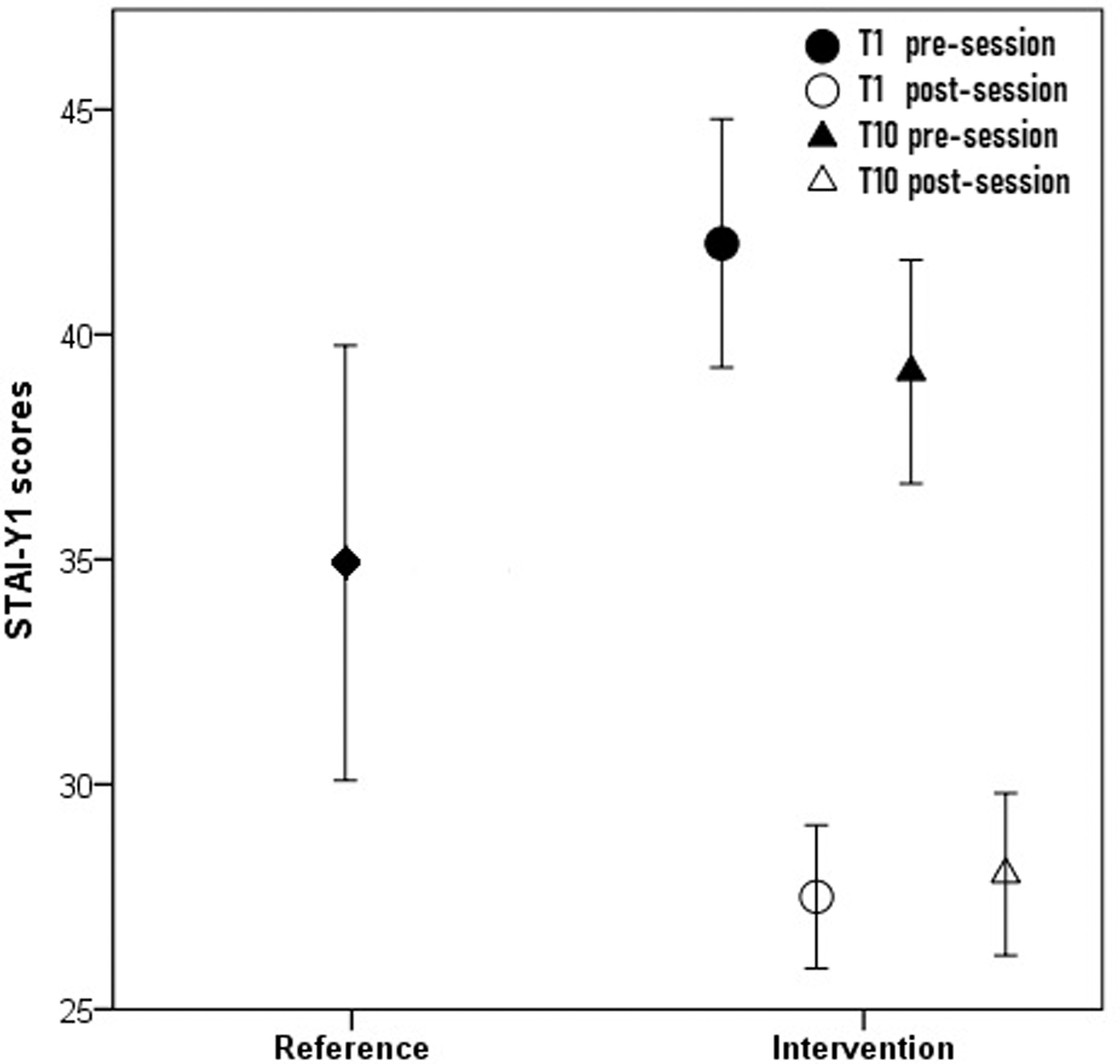
State anxiety (STAI-Y1) dropped after both T1 and T10 sessions by 14.53 and 11.17 points, respectively, from a “low” level before the session (M T1preSTAI-Y1 = 42, M T10preSTAI-Y1 = 39.2), to a “very low” level after the session (M T1postSTAI-Y1 = 27.5, M T10postSTAI-Y1 = 28). This drop corresponds to an average decrease of 30% each time (Fig. 1). The session decrease is both times highly negatively correlated to the initial level of state anxiety, that is, the “state anxiety baseline” (ρT1 = −0.817 and ρT10 = −0.696), which means that the drop increases with the increase of the state anxiety baseline and that there is a uniformization trend in the postsession state anxiety levels near to the lowest levels of state anxiety (or a bottom effect of the scale). Another remarkable point is the significant decrease over the 10 sessions of the “state anxiety baseline” (T10-T1 pre STAI-Y1, t = −2.098, P = 0.039; Table 2).
Trait anxiety (STAI-Y2) decreased by 6.2 points (−13%) after 10 sessions, from a “medium” level at T1 (M T1STAI-Y2 = 49) to a “low” level at T10 (M T10STAI-Y2 = 43).
Self-esteem increased by 3.8 points at the end of the program (+13%), with a score rising from “low to medium” level at T1 (M T1RSE = 29.11) to a “medium” level at T10 (M T10RSE = 33.07).
To validate the effects of the program needs referring our data to an external group, we compared the PG score discrepancies to the RG scores, on the trait variables (Table 1):
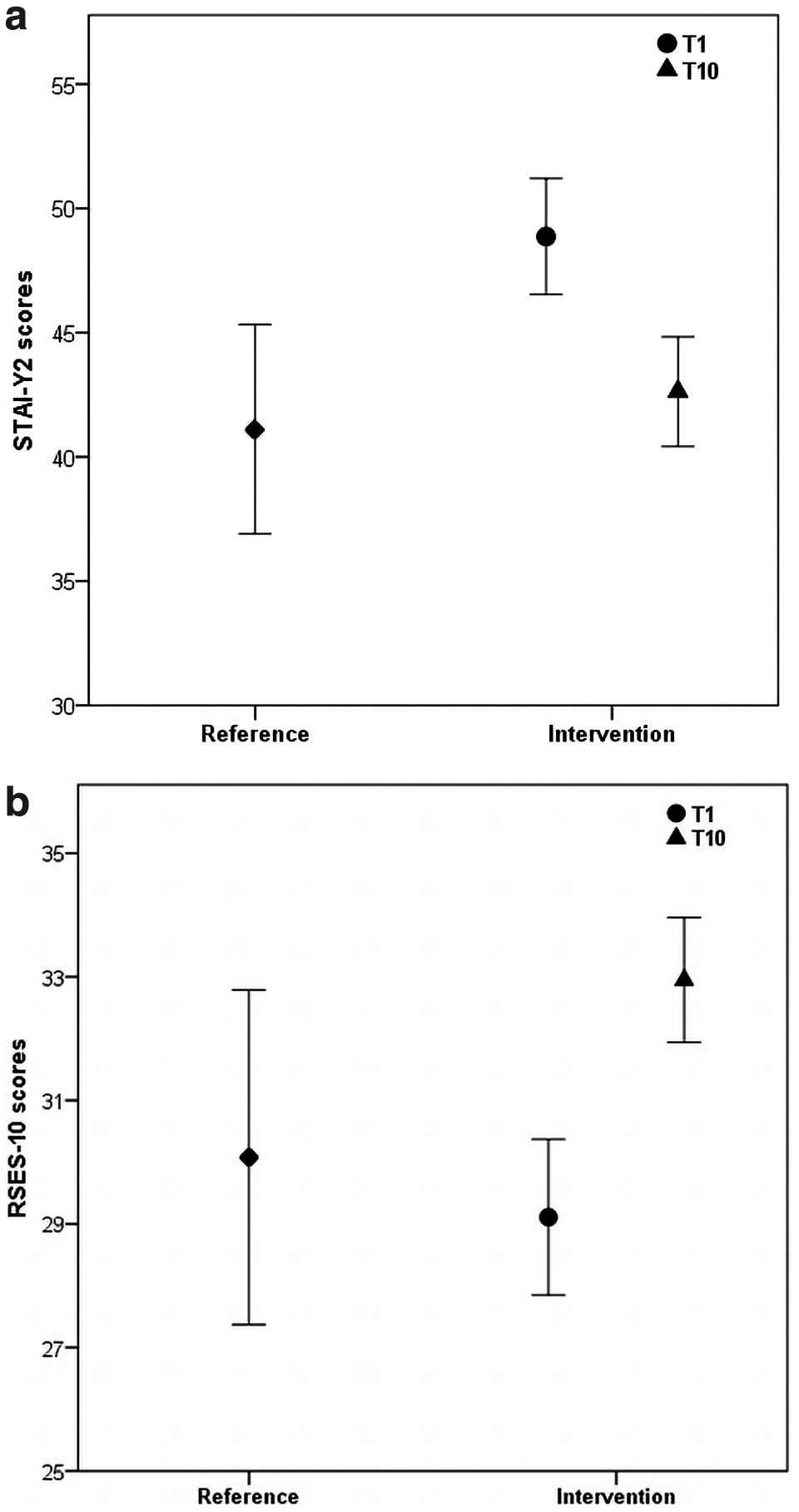
Regarding trait anxiety STAI-Y2, PG strongly differs from RG at T1 (t T1 = −3.333, P = 0.001), with higher scores in the PG (M PG = 48.9) than the RG (M RG = 41.1), which confirms our initial hypothesis of a highly stressed population of participants. And at T10 this difference is no longer significant (t T10 = −0.666, P = 0.507), which confirms our second hypothesis that the participants' anxiety would return to “normal” at the end of the 10 sessions, assuming the RG was our “normal” reference. This is displayed in Fig. 2a. The effect of the program is strong (d = 0.75) and very reliable (1-β = 0.91).
The effect of the program on self-esteem follows a reverse pattern to that of trait anxiety (Fig. 2b). At T1 both groups have the same low to medium level of self-esteem (M PG = 29.11 and M RG = 30.08; Table 1), which means our participants have “normal” levels of self-esteem. However, at T10, their self-esteem score is significantly higher, with moderate effect size and reliability (M PG = 33.01, P = 0.041, d = 0.53, 1-β = 0.63) in a first approach. After decorrelation from trait anxiety, the effect size of the program on self-esteem was revealed to be high and strong [Analysis of Covariance (ANCOVA) F (1.99) = 87.35, P < 0.01, η 2 = 0.47]. The rise of our participants' self-esteem at the end of the 10 sessions can then be computed. Given the equal trait anxiety of the two groups (STAI-Y2 = 42.22, which was roughly the case), its “marginal mean” is 3.5 points greater than that of the RG [M PG(T10) = 33.2 ± 0.43 vs. M RG = 29.69 ± 0.73]. The program, therefore, has, when controlling for anxiety, a significant and strong effect of increasing self-esteem, even without initial self-esteem issues.
There is indeed a strong correlation between trait anxiety and self-esteem in the PG, which is preserved at T1 and T10 (r IRG1 = −0.727, P < 0.001, r IRG10 = −0.644, P < 0.001), and which can also be found in the RG (r RG = −0.671, P < 0.001). This correlation is also preserved in the T10-T1 differences of the two PG variables (r PG = −0.608, P < 0.001). It, therefore, seems that the program has no effect on the relationship between trait anxiety and self-esteem, which would, therefore, be an independent human characteristic. This observation is confirmed by an ANCOVA [F (1.99) = 0.013, P = 0.911] conducted on the predicted values of self-esteem and trait anxiety. †
Characteristics of the Population Requesting SPE Support
Characterization of the parent population of our participants is conducted by comparing between-group data at the beginning of the program (PG vs. RG), which are displayed in Table 1:
PG's initial state anxiety (pre-STAI-Y1) is far higher than RG's state anxiety (M PG = 42.03, M RG = 34.92, t T1 = −2.593 P = 0.011, d = 0.59, 1-β = 0.73).
PG's initial trait anxiety (STAI-Y2 at T1) is far higher than that of the RG (M PG = 48.87, M RG = 41.12, t T1 = −3.333 P = 0.001, d = 0.75, 1-β = 0.91).
PG's initial self-esteem is no different than RG's (M PG = 29.11, M RG = 30.08, P = 0.465).
This means that the PG presents a significantly more anxious profile than the RG, but a similar low-to-medium level of self-esteem to that of the RG. It is consistent with our study premise: given their normal level of self-esteem, our participants can be considered psychically balanced. 17 This confirms our initial hypothesis that our participants come from a “nonpathological” population with a higher level of anxiety than normal.
Because of differences in the literature regarding discrepancies between genders, 20,48,49,51 we also verified the behavior of our participants' scores using a two-factor Multivariate Analysis of Covariance (program and gender). There was no difference detected between the genders whatever the group, after controlling for age [multivariate test F (8, 87) = 1.665, P = 0.118, Roy's Largest Root = 0.153, partial η 2 = 0.133, power = 0.694]. However, a detailed analysis by variable on the PG revealed that women's state anxiety scores after one session were lower than men's (post STAI-Y1, FT1 = 14.048, P < 0.001, FT10 = 7.833, P = 0.006), indicating that women would respond more strongly than men to sessions on the state anxiety variable, without this having any repercussions on the evolution of trait anxiety.
Discussion
The results of this longitudinal and prospective field survey indicate that a 10-session follow-up in SPE lowers trait and state anxiety and improves the self-esteem of a population of people spontaneously seeking individual support.
No Practitioner Effects
We have seen that the practitioners who treated at least four clients throughout the entire program (eight practitioners holding on average five clients each) did not show any difference in results regarding the effects of their practice on anxiety and self-esteem. This result invites us to consider the absence of a practitioner effect on the results obtained by the practice of SPE on anxiety and self-esteem. This generalization makes it possible to consider the effectiveness of SPE on its own as a practice to support nonclinical issues of anxiety and self-esteem, regardless of the personal touch of each practitioner. Such a result runs counter to the discourse of convenience arguing that alternative approaches in health and wellness care are practitioner dependent. It calls for more dissemination of such results particularly to the health care community, which could find relevant complementation and support in such mind–body practices.
Specificity of the Population Seeking SPE Practices
The results highlight the existence of some specificities of the people requesting individual support in SPE, who present real but nonclinical anxiety issues. The differences in state and trait anxiety compared with the Francophone “normal” exemplified by our RG are to be compared with the initial expectations of our sample (physical pain, mental and emotional suffering, difficulty coping, discomfort, loss of sense, see Supplementary Data S2), 83% of which are linked to negative affect. And negative affect is known to be a trigger for potential anxiety issues. 52,53 In other words, although anxiety and self-esteem were not mentioned as an issue in the initial expectations, the quest for individual support seems to be driven by an overall problem of negative affect. Further SPE field studies can build either on matched control groups with consideration of initial trait anxiety and bodily practice, or on large random sampling with trait anxiety as a selection criterion.
Contribution of SPE Sessions
A one-time SPE session offers an immediate benefit for state anxiety by lowering it by more than 30% of its initial value with a very large effect size (d > 0.7). A temporal follow-up of 10 sessions in SPE has three major effects: (1) it strongly reduces trait anxiety (by −13% or −6.2 points, η 2 > 0.14), (2) it strongly increases self-esteem (by +13% or +3.5 points when controlling for trait anxiety, η 2 > 0.14), and (3) it decreases the state anxiety baseline. The increase in self-esteem is remarkable in the sense that it leads to a higher level of self-esteem than “normal,” highlighting the rather low and, however, rarely discussed level of the “norms.” In a previous study on an SPE follow-up, 35 self-esteem increase was associated with the development of a perception of self that the people described as totally new to them, similar to a sense of feeling “alive from the inside,” which led to a renewed and improved vision of themselves and of their self-esteem, thus reducing their vulnerability to stress. Such improvement of the self-esteem baseline along with the disappearance of trait-anxiety issues is indicative of a behavioral trend change, in favor of improved coping and adaptation abilities when relating to a difficult or confronting environment. The decrease in the state anxiety baseline enforces this hypothesis, as the “state” measure is indicative of the sensitivity to the immediate context of life events. It probably takes time for the sensitivity to external events to subside as the anxious trait subsides, which explains why the decrease in state anxiety baseline is not as strong as that of the trait anxiety. Indeed, sensitivity could be a behavioral expression of the anxiety profile, which takes longer to stabilize.
These different effects are detected despite the average program durations of 4–13 months and despite the pivotal age of our sample (on average 50 years) with regard to the “ages of self-esteem.” 19,54 We thus confirm some of the founding hypotheses of this study: (1) that the trait parameters can vary over time when the program proposes an action on the behaviors causing discomfort, in particular the relationship with the self; and (2) that the intrinsic instability of anxiety and self-esteem parameters in mature and even elderly adults seems able to benefit greatly from this type of support. We also note that the scales initially designed to describe differences between groups can validly account for such developments.
The Bodily Experience
As previously mentioned, hypotheses in the literature consider bodily experience to have a positive effect on anxiety and self-esteem and on the relationship between anxiety and self-esteem. Our results confirm the positive effect of a bodily practice on self-esteem and anxiety. Indeed, with the practice of SPE being dominated by the use of a particular relational touch, our results suggest that it is such bodywork practice that is at the origin of the positive impact of SPE on anxiety and self-esteem. The perceptual and relational nature of the touch that is applied calls for the person's conscious attention to the ongoing experience within their body, qualifying it in what Quidu 32 and Andrieu 26 described as bodily experience in the first person or as the body sensed in the first person. Under the effect of what one could call a “bodily rootedness” of the experience, this stimulation generates a learning effect capable of improving the perceptual performance of the person, over the sessions and over time. According to this model, the greater the number of sessions, the longer the integration time will also be, and the more marked and reliable the evolution of self-esteem and anxiety will be. It can, therefore, be expected that the effect of lowering the state anxiety baseline will be more marked.
Interestingly, our sample has a lower frequency of bodily practice than our RG, which can explain, in part, the high initial anxious profile of our participants. None of the SPE support was oriented toward the development of a bodily practice, thus no change on this aspect of the participants' personal practice was detected. Nonetheless, the initial issue of malaise has faded away. This is in line with the work of Copstead, 55 which demonstrates a direct relationship between relational touch and self-esteem in a support situation. We expand the hypothesis to propose that the perceived and experienced body, and more specifically the enhancement of bodily perception, plays an important role in the process of improving self-esteem, 35 adding that this bodily pathway acts simultaneously on the lowering of anxiety. Our results should help to sustain reflections such as those of Bonitz, 56 who notes the benefits on self-esteem of the introduction of an adapted and benevolent manual touch in psychotherapy sessions.
Subsequent studies could usefully explore the value of developing a personal daily bodily practice for the persistence of the beneficial effects of SPE support, as a means of gaining autonomy in self-care.
Relationship Between Self-Esteem and Anxiety
In our results we observe that the relationship between anxiety and self-esteem is strong at all stages of the program, both in our sample and in the RG. We showed that this relationship is a co-relation, not a redundancy. The decrease over time in the state-anxiety baseline of our participants suggests a decrease in the sensitivity to anxiety factors, and the strong decrease in trait anxiety signals a change in the anxious profile of the persons within which the dependence on external events and the issue of control weakened. 57 Simultaneously, the effective increase in self-esteem, that is, strongly significant when controlling for trait anxiety, also signals a reduction in the sensitivity to anxiety factors and confronting events, and a better capacity to respond to positive elements in the environment, 35 giving the person greater autonomy in their management of events with less recourse to internal or external defense, enhancement, or justification strategies. 58,59 Such simultaneous beneficial action on anxiety and self-esteem is reported in the literature and most often reported from a psychological perspective. 18 Yet the perceptual capabilities of the body seem to play a decisive role: the beneficial effect on trait anxiety can be explained by the way SPE touch simultaneously focuses the attention on the bodily perceptions and the reflection on the immediate experience 10,38,42 ; the beneficial effects on self-esteem are explained by the development of a genuinely new relationship to the self, embedded in a bodily lived sense of calm, gentleness, positivity, and of feeling “alive inside,” which, by renewing the vision of oneself, contributes to the reduction of one's vulnerability to stress. The support at play in SPE helps the person to build up, within the immediate experience, new perceptual capabilities of their body and a renewed bodily sense of self. It seems that the efficiency of SPE on anxiety and self-esteem is at the heart of this combined action, by developing a self-perception that encompasses in a single embrace bodily awareness and a sense of being concerned, touched, involved in one's living body. 60 Such changes affect the behaviors of the person, leading them toward more autonomy and emotional stability in the face of events, and more freedom from their own internal anxiety mechanisms. Although we could not find any changes in this relationship after the SPE follow-up, further conclusion requires complementary work, particularly with regard to the duration of the follow-up.
The Questionnaire and the Program (Learning) Effects
Finally, some practitioners report feelings of an accelerated calming process in their patients, unprecedented awareness and sudden connections that had never existed before in long-term clients. This suggests the possibility of the influence of participating in the survey on the effects of support. In other words, the fact of answering the questionnaires several times seems to induce in the participants, even without any interaction with the practitioner, a new form of reflexivity, in which the sessions have beneficial, or even amplifying, effects. This is consistent with the analysis made by Mruk, 61 who developed a support program integrating various types of work and interactions based on progressive solicitation, personalized guidance, and regular stages of self-assessment, which, he explains, are the core of the effectiveness of his interventions. SPE aims to stimulate the learning processes drawn from bodily experience by arousing the active and conscious perceptual participation of the person, placing them in a dynamic of awakening and availability conducive to learning and reflection. 34,62 We believe that in this context of perceptual and cognitive mobilization, the administration of self-evaluative questionnaires has been able to stimulate and strengthen the synergy between bodily experience and reflexive dynamics, promoting awareness beneficial to the person's initial quest, and hence to their anxiety state (and trait) and their self-esteem, even when anxiety and self-esteem were not the conscious drivers of the demand for support.
Conclusions
This field survey aimed at highlighting the effects of SPE on anxiety and self-esteem. It enabled the characterization of the population requesting individual support in this practice and showed a strong immediate effect of a single session on state anxiety, a strong attenuating effect on trait anxiety along with a decrease in the state anxiety baseline, and an improvement in self-esteem over the course of 10 sessions. This combination of changes, associated with the decrease in state anxiety baseline, is indicative of an ongoing beneficial transformation in the relationship to the self and to life events, suggesting a change in behavior and in coping abilities.
Such efficiency finds its source in the place given to the body and to the development of bodily perceptual capabilities in the practice of SPE. It confirms the positioning of SPE at the crossroads of care and training as it induces a long-lasting learning effect, and also at the crossroads of mind and body approaches due to the place of perception in the development of the relation to self. Similar to some meditative practices, it stimulates the relationship with interiority, “interoceptive” sensory awakening, and awareness of the self and of the body. 8,10,63
Through its simultaneous action on self-esteem and anxiety, SPE could be beneficial in the accompaniment of certain specific difficulties involving hypersensitivity of the relation to the world and to self, for example, in adults with high potential 64 or in situations of burnout and exhaustion. We hope to have contributed to showing the relevance of research on the role of bodily perception in the improvement of anxiety and self-esteem issues, and on their interaction.
Footnotes
Acknowledgments
The authors thank the practitioners who volunteered to participate in this study and all of the anonymous participants who donated their time to make this research possible. The authors note special thanks as well to the translators for their help.
Author Disclosure Statement
The authors report no conflict of interest and declare that they have not received any form of influence that could have impacted their study or their results.
Funding Information
This study was supported by the FePAPP (Fédération des Professionnels de l'Accompagnement en Pleine Présence), grant reference 2016-08-001.▪
Supplementary Material
Supplementary Data S1
Supplementary Data S2
Supplementary Data S3
Supplementary Data S4
Supplementary Data S5
Supplementary Data S6
Supplementary Data S7
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.