
Abstract
Objectives:
To investigate the efficacy of laser acupuncture (LA) therapy in patients with dry eye disease (DED).
Design:
A two-center randomized controlled trial.
Settings/Location:
The Department of Ophthalmology, Chinese Medicine at the Kaohsiung Chang Gung Memorial Hospital, and the Sunming Eye Clinic in South Taiwan.
Subjects:
Fifty-nine participants ages 20 to 65 years were enrolled and randomly assigned to the experimental group (LA plus conventional treatment) or the sham control group (LA without laser output plus conventional treatment).
Interventions:
Subjects underwent LA treatment three times a week for 12 weeks. The subjects in the experimental group sequentially received 0.375 J of energy at each of the following acupoints: BL2, TE23, ST2, LI4, ST36, and GB37. Subjects in the control group received a sham LA treatment, without any laser output.
Outcome Measures:
The primary outcome measure was ocular surface disease index (OSDI). The secondary outcome measures included tear film breakup time (TFBUT), Schirmer-I test finding, and visual analog scale (VAS) score.
Results:
At 4 and 12 weeks after the first visit, the experimental group showed significant improvement of dry eye symptoms as measured by OSDI, TFBUT, Shirmer-I test, and VAS. Compared with the control group, the OSDI (7.23, p = 0.001) and TFBUT (−1.78, p = 0.001) significantly improved in the experimental group at 12 weeks of treatment.
Conclusions:
LA improved the symptoms and tear stability related to DED in conjunction with conventional treatment. The authors suggest that LA be considered a complementary therapy for DED when conventional treatment does not provide satisfactory effects.
Trial Registration:
Introduction
The prevalence of dry eye disease (DED) ranges from 5% to 50%, thus making it a worldwide health concern. DED is particularly common in people over the age of 50 years. In addition, it is one of the most common reasons for seeking ophthalmic care. 1 Women report a higher prevalence of DED than men. However, the differences become significant only with age. 2 Aqueous deficiency and increased evaporation are the two major causes of dry eye. 3 Dry eye is characterized by the loss of tear film homeostasis. This in turn results in varied ocular symptoms that include tear film instability, hyperosmolarity, ocular surface inflammation, and corneal damage. Neurosensory abnormalities, including abnormal neuromodulation, neuropathic and nociceptive pain, play etiological roles in this multifactorial disease of the ocular surface. Most of the symptoms, including the economic burden and impact of DED on vision, quality of life, work productivity, and the psychological and physical impact of pain, are considerable. In particular, the costs due to reduced work productivity, and the low rate of a satisfactory response to treatment, highlight the need to further investigate effective therapies. 4,5
Considering the highly variable clinical manifestations of DED, the diagnosis and subsequent treatment are often tailored to each patient by targeting the specific mechanisms underlying the disease. 6 Artificial tears, gels, ointments, and inserts are used to replenish the tear film. 7 Nonetheless, these treatments are often palliative and do not provide satisfactory relief from debilitating symptoms. 8 Thus, patients with DED may seek complementary and alternative medicine (CAM). Acupuncture is a traditional medicine technique, not only an alternative medicinal technique but also one of the most popular forms of CAM used to treat a variety of conditions. 9,10 While recent studies report on its efficacy for dry eye, 11 –13 there is lack of consensus on the most effective acupuncture method. This can be attributed to the study design, insufficient sample sizes, and few therapeutic sessions. 14,15
Laser acupuncture (LA) is a noninvasive technique that stimulates traditional acupoints with low-intensity, nonthermal laser irradiation, rather a metal acupuncture needle. LA has been used to treat several eye conditions, including amblyopia. 16,17 LA does not rely on somatosensation, compared with traditional acupuncture. In addition, it has the advantage of being noninvasive and aseptic. Furthermore, it requires less time than traditional acupuncture and does not generate heat during the procedure, thus being painless and safe. 18 –20 The authors aimed to conduct a 12-week-long, two-center randomized-controlled trial to assess the efficacy of LA in patients with DED.
Methods
This study was approved by the Human Ethics Committee of this hospital (Chang Gung Medical Foundation Institutional Review Board, IRB No. 201600333A3C503). The authors adhered to the tenets of the Declaration of Helsinki and its amendments and registered the protocol with
Study design
The authors conducted this two-center randomized-controlled trial at the Department of Ophthalmology, Chinese Medicine, at the Kaohsiung Chang Gung Memorial Hospital, and the Sunming Eye Clinic in South Taiwan from August 2016 to July 2019. Each center independently recruited the participants. They randomly allocated them to the experimental group (LA plus conventional treatment) and the sham control group (LA without laser output plus conventional treatment). All participants received 36 sessions of treatment over 12 weeks. Figure 1 depicts the study design.
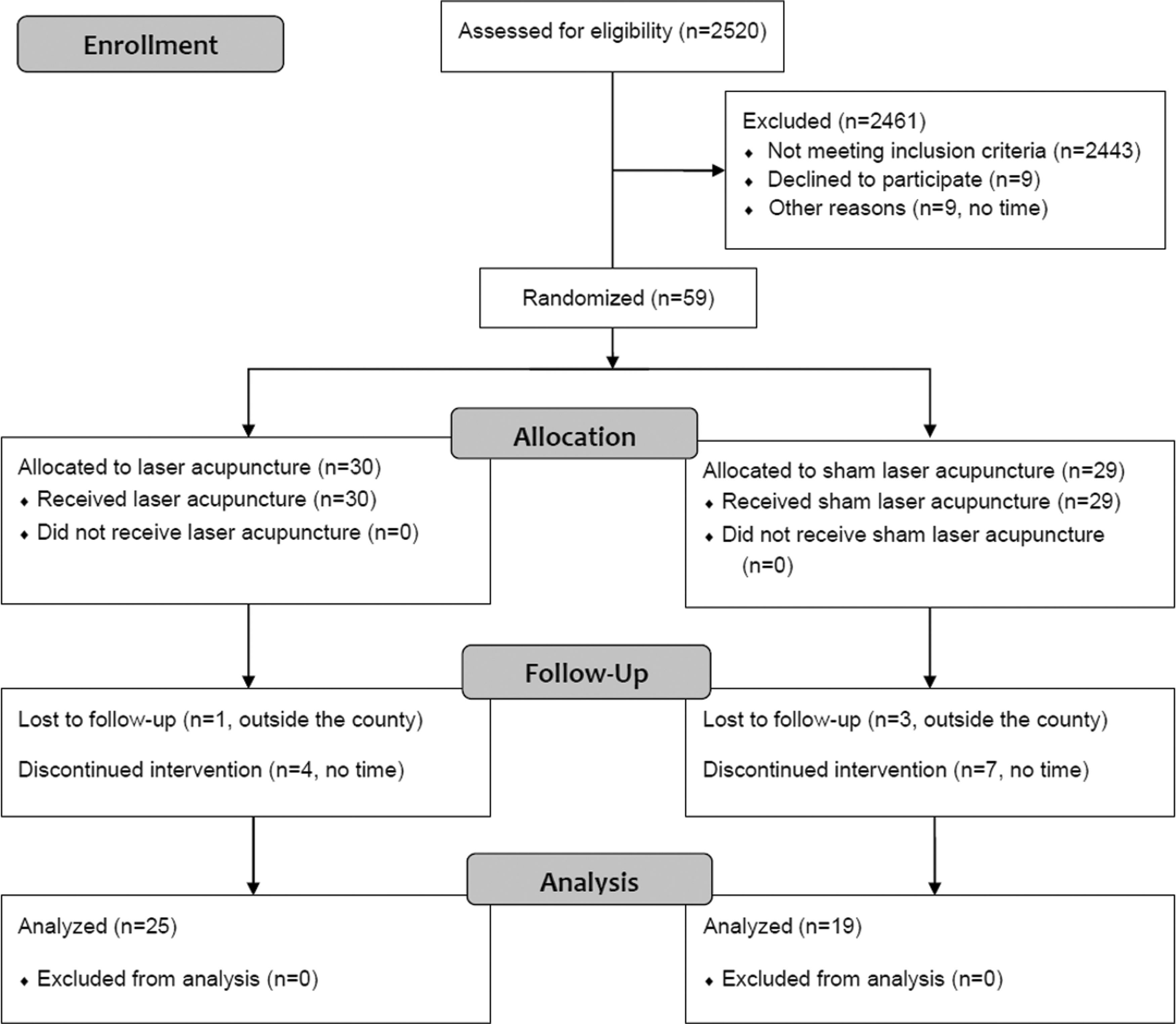
CONSORT diagram showing randomization and treatment of study patients.
Participants
Diagnosis of dry eye was based on the following criteria: (1) patient symptoms assessed using the Ocular Surface Disease Index (OSDI) questionnaire; (2) visual disturbance (blurred vision or poor vision) or visual dysfunction (problems reading, driving at night, working on a computer, or watching TV); (3) tear film breakup time (TFBUT); and (4) Schirmer-I test for assessing tear film stability.
The authors recruited patients aged 20 to 65 years with aggravating acute or chronic dry eye symptoms in one or both eyes. Physicians and ophthalmologists assessed their eligibility for participation. The inclusion criteria were based on the following ophthalmic test results: a TFBUT below 10 sec and a Schirmer-I test (with anesthesia) value below 5 mm/5 min. The ophthalmologists were blinded to the treatment allocation. The exclusion criteria were as follows: (1) participants with eye lesions, diabetes mellitus, vitamin A deficiency, sequelae of Bell's palsy, a critical illness, such as the Stevens–Johnson syndrome, cancer, infectious disease of the skin, a history of seizure or epilepsy; (2) those who had undergone an eye operation in the past 3 months or hemodialysis; (3) those using a combination of other ophthalmic medications, contact lens, a pacemaker, or immunosuppressants; (4) those who had taken or needed active treatment (including Chinese Medicine); (5) those who did not meet the physician's assessment for recruitment or were unwilling to provide informed consent; and (6) pregnant women.
Sample size and randomization
The necessary sample size was calculated from the results of a previous study on the effects of acupuncture. The mean difference (standard deviation) in the OSDI after acupuncture treatment and after sham acupuncture was −17.61 (15.61) and −17.20 (18.81), respectively. 14 Anticipating a 15% dropout rate, a total of 200 participants were expected to be recruited and evenly assigned to each center (100 participants in each center). A research randomizer that generates the random sequence was applied to select random permuted blocks with a block size of four and an equal allocation ratio. Allocation concealment was implemented through the use of numbered containers. The allocation sequence was concealed from the researcher enrolling and assessing participants in sequentially numbered, opaque, sealed, and stapled envelopes. The authors equally randomized patients who were refractory to conventional treatment and those who were stable and responded to conventional treatment. The trial participants, outcome assessors, and data analysts will be blinded after assignment to interventions using label A and B for the two groups.
Interventions
There are different treatments for dry eye, including topical medication and surgical intervention. The authors enrolled patients who received artificial tears, four times a day, with 0.02% fluorometholone, a weak steroid, twice daily before or at the start of treatment. They did not change the medication until the completion of this study.
Each group underwent three sessions a week for a total of 36 sessions. The LA treatment involved a gallium aluminum arsenide LaserPen (maximal power, 150 mW; wavelength, 810 nm; area of probe, 0.03 cm2; power density, 5 W/cm2; pulsed-wave; and Bahr frequencies [B1: 599.5 Hz, B2: 1199 Hz, B3: 2398 Hz, B4: 4776 Hz, B5: 9552 Hz, B6: 19,104 Hz, and B7: 38,208 Hz]; RJ-Laser, Reimers & Janssen GmbH, Waldkirch, Germany). The authors selected and located all acupoints according to the WHO Standardized Acupuncture Point Location guidelines. 21 They used similar acupoints in both the groups. While the participants in the control group received sham LA treatment, without any laser output (no stimulation), those in the experimental group sequentially received 0.375 J of energy at each of the following acupoints 22 : BL2 (Cuanzhu, B3), TE23 (Sizhukong, B3), ST2 (Sibai, B3), LI4 (Hegu, B3), ST36 (Zusanli, B2), and GB37 (Guangming, B2) (Figs. 2 and 3). The combination of these acupoits was based on the clinical practice for DED. The laser treatment was applied to each point for 5 sec and a total dose of 4.5 J/cm2 was delivered. The laser application was performed by the same trained and experienced physician for all participants. The latter is a licensed Chinese Medicine practitioner in Taiwan who has the experience of >10 years in traditional acupuncture practice and 5 years in LA practice. The operator and the patient used a protective goggle and laser shield, respectively, to inhibit visual perception during LA.
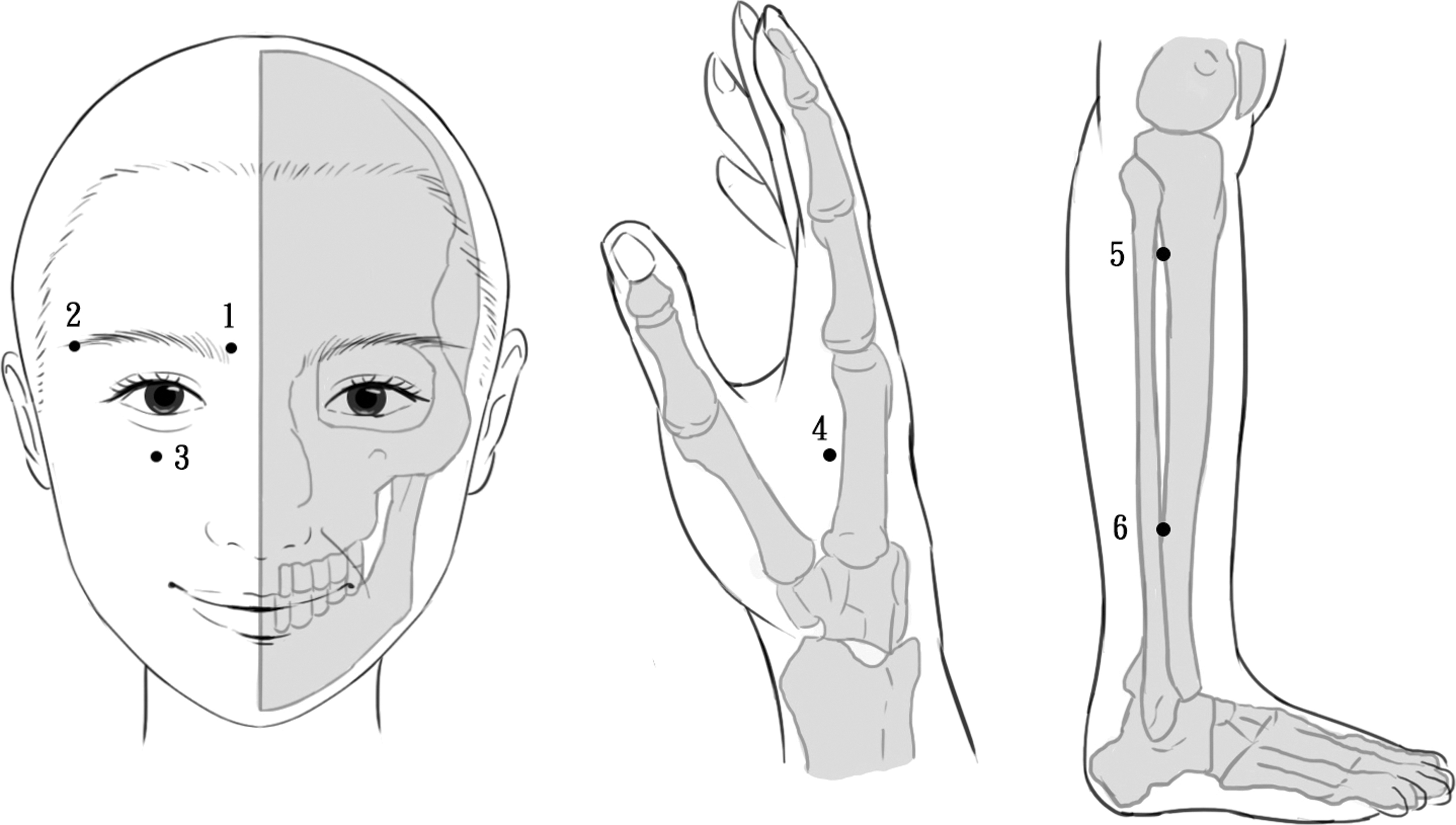
Schematic representations of the acupoints used for dry eye are as follows: (1) BL2, (2) TE23, (3) ST2, (4) LI4, (5) ST36, and (6) GB37.

Demonstration of laser acupuncture performed using the LaserPen device at the GB37 acupoint.
Outcome measurements
The authors assessed the outcomes in both eyes at 4 and 12 weeks after the first visit. Outcome measurements included two aspects, namely objective ophthalmic tests and subjective questionnaires for ocular symptoms related to DED. The difference in the OSDI changes between the two groups was the primary outcome at week 12. In contrast, the secondary outcomes included differences in TFBUT, Schirmer-I test (with anesthesia) score, and 10-cm visual analog scale (VAS) score of eye discomfort.
The OSDI is a 12-item scale for the assessment of DED-related symptoms and their effects on vision. 23 The score ranges from 0 to 100, with higher scores representing severe dry eye symptoms. TFBUT measures the time required for tears to evaporate and diffuse after natural blinking. 24 It was performed using fluorescein strips (Fluoro Touch; Madhu Instruments Pvt. Ltd.) and both centers used this as a control. A Schirmer-I test (with anesthesia) assessed the speed of production of tears. 25 In addition, a 10-cm VAS (0–10 points, least to greatest discomfort) was used to measure eye discomfort. Separate assessors who did not perform the LA treatment evaluated the OSDI and VAS scores. Furthermore, ophthalmologists evaluated the outcomes of the TFBUT and Schirmer-I test.
The authors recorded the patients who dropped out of the study for the following reasons: adverse events/intercurrent illnesses, suboptimal response to therapy, failure to return for follow-up visits, failure to meet selection criteria at entry, other protocol violations, and refusal to receive treatment. Despite the delivery of 0.375 J to an acupoint, they recorded the adverse events.
Statistical analysis
All data are presented as mean ± standard deviation. A paired t-test was used for intragroup comparison at each checkpoint. A hierarchical linear model was used to evaluate the changes in the OSDI, TFBUT, Schirmer-I test result, and VAS scores between the experimental and sham groups. Differences were significant at a p-value <0.05. All analyses were performed with SPSS for Windows, version 22 (Statistics 22, SPSS; IBM Corp., Chicago, IL).
Data monitoring
A data monitoring committee was not needed. This can be attributed to LA being a general and noninvasive intervention.
Results
A total of 2520 participants were assessed for their eligibility across two research centers. Fifty-nine DED patients met the inclusion criteria and were randomly allocated into the LA and sham LA groups. Five participants from the LA group and 10 from the sham LA group dropped out during the study (Fig. 1). In the LA group, the authors lost one participant to follow-up due to living outside the county. In addition, four of them discontinued treatment due to time constraints. They lost three and seven participants to follow-up due to living outside the county and time constraints, respectively, in the sham LA group. The baseline characteristics of the groups are shown in Table 1.
Baseline Characteristics of Participants
LA, laser acupuncture; OSDI, ocular surface disease index; TFBUT, tear film breakup time; VAS, visual analog scale.
Ocular surface disease index
The authors analyzed 53 and 40 eyes in the LA and sham LA groups, respectively, following 4 weeks of treatment. The hierarchical linear model revealed significant differences in the changes from baseline OSDI between the two groups, with the LA group and sham group changing −11.41 and −2.35, respectively. After 12 weeks of treatment, 46 and 34 eyes were analyzed in the LA and sham LA groups, respectively. The change in OSDI was −18.06 and −3.12 for the LA and sham LA groups, respectively. Significant improvement in OSDI in the LA group was reported after both 4 and 12 weeks of treatment (both p < 0.001), while no significant change was found in the sham LA group (Table 2). Differences in OSDI between the two groups from baseline to 4 weeks were 4.82 (p = 0.051), and differences in OSDI between the two groups from baseline to 12 weeks were 7.23 (p = 0.001, Table 3) (Fig. 4).
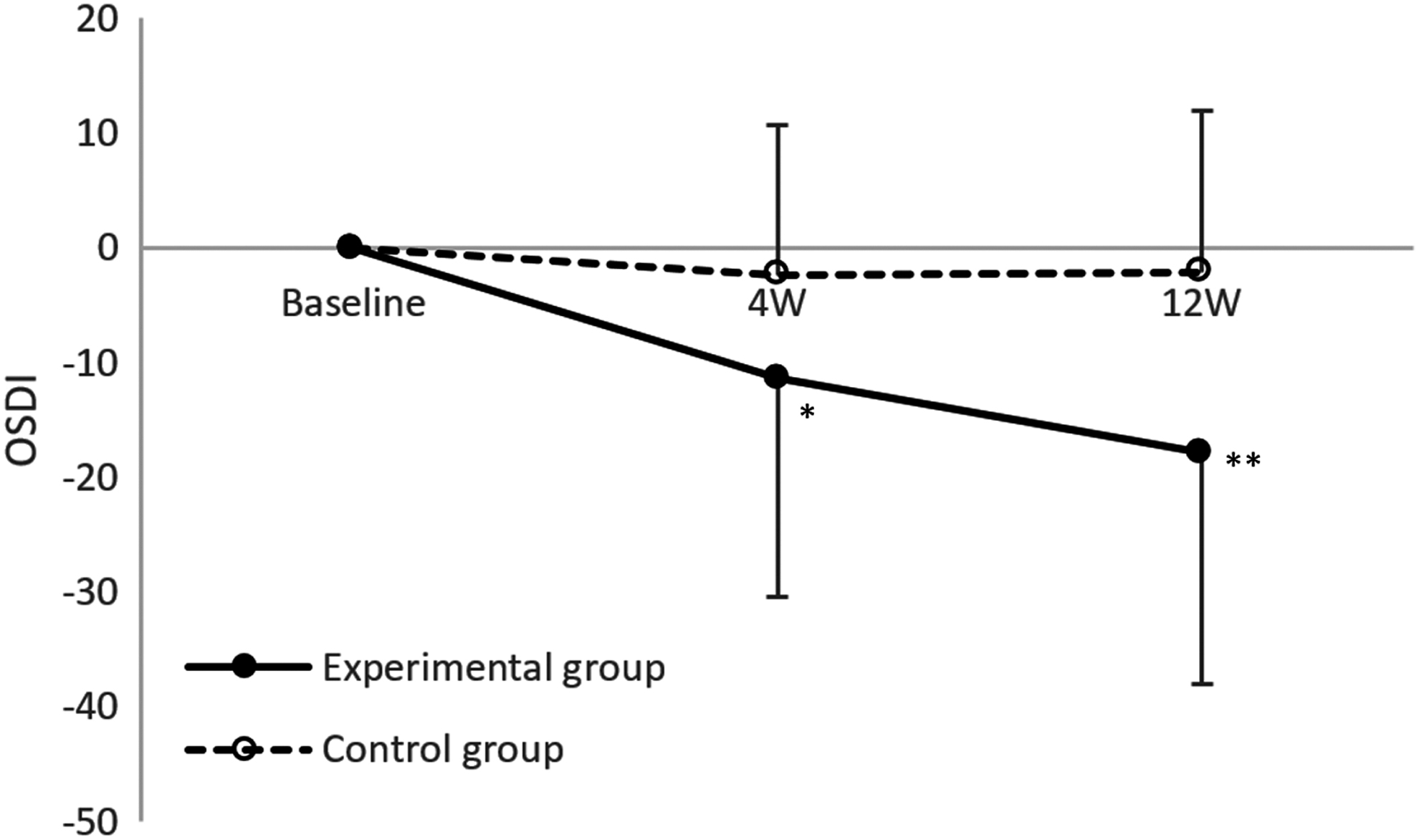
OSDI, *p = 0.051, **p = 0.001. Hierarchical linear model was used for the statistical analysis of changes from baseline in each outcome between the two groups. OSDI, ocular surface disease index.
Changes from Baseline in Primary and Secondary Outcomes at Each Visit
Hierarchical linear model was used for the statistical analysis of changes from baseline in each outcome with missing data being multiply imputed. Negative values of difference in OSDI and VAS (positive difference in TFBUT and Schirmer) are in favor of LA group.
LA, laser acupuncture; OSDI, ocular surface disease index; TFBUT, tear film breakup time; VAS, visual analog scale.
Changes from Baseline in Primary and Secondary Outcomes Between Two Groups
Hierarchical linear model was used for the statistical analysis of changes from baseline in each outcome with missing data being multiply imputed.
LA, laser acupuncture; OSDI, ocular surface disease index; TFBUT, tear film breakup time; VAS, visual analog scale.
Tear film breakup time
The change from the baseline of TFBUT was 1.99 and 0.79 in the LA group (p < 0.001) and the sham LA group (p = 0.139), respectively. At 12 weeks of treatment, TFBUT showed a significant increase in the LA group (LA: 3.66, p < 0.001; sham LA: −0.21, p = 0.711). Differences in TFBUT between the two groups from baseline to 4 weeks were −0.56 (p = 0.145) and differences in TFBUT from baseline to 12 weeks were −1.78 (p = 0.001, Table 3) (Fig. 5).
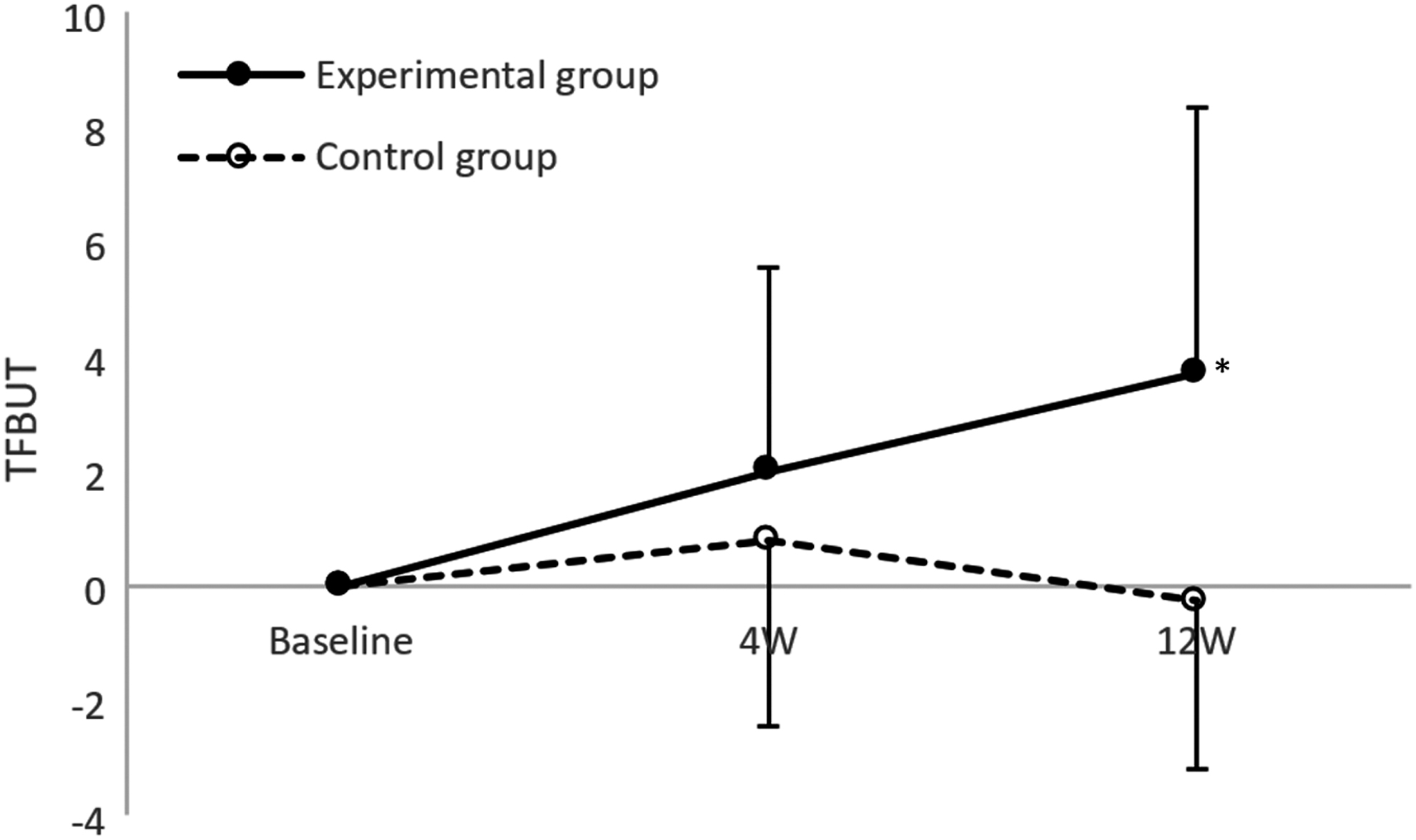
TFBUT, *p = 0.001. Hierarchical linear model was used for the statistical analysis of changes from baseline in each outcome between the two groups. TFBUT, tear film breakup time.
Schirmer-I test scores
The authors observed statistically significant differences in the Schirmer-I test score in both groups after 12 weeks of treatment (LA group: 1.52, p = 0.001; sham LA group: 1.30, p = 0.008) (Table 2). Differences between the two groups from baseline to 4 and 12 weeks were −0.12 (p = 0.644) and −0.133 (p = 0.800), respectively (Table 3).
Visual analog scale
VAS showed statistically significant improvements in the LA group at 4 weeks (−0.59, p = 0.005) and 12 weeks (−1.07, p < 0.001) of treatment (Table 2). Differences between the two groups from baseline to 4 and 12 weeks were 0.16 (p = 0.430) and −0.02 (p = 0.915) (Table 3).
Adverse events
There were no reports on adverse events related to intervention during the study period.
Discussion
The prevalence of DED in Taiwan is approximately one-fourth of the total population. It is particularly related to age, gender, and environmental factors. 26 The authors assessed the effectiveness of a 4- and 12-week LA treatment on the subjective and objective outcomes of DED. All improvements were observed in the experimental group; there were statistically significant differences that favored the LA treatment in OSDI and TFBUT at the 12-week follow-up. The main strength of this study is the improvement of OSDI and TFBUT in DED by LA.
One study reported that LA had similar efficacy as traditional acupuncture in relieving symptoms and improving tear secretion in DED. 27 However, herbal and natural products, along with acupuncture, require more Level 1 studies to be widely accepted as potential treatment options for DED. 4 Previous research on DED reported on the effectiveness of needle acupuncture, compared with artificial tears in treating DED. However, the former showed high heterogeneity that was not influenced by differences in the intervention. 11 Needle acupuncture plus conventional treatment improved the clinical symptoms of DED. Nonetheless, there was no significant improvement in the TFBUT or Schirmer-I test, compared with conventional treatment. 28 Despite needle acupuncture not being more effective than artificial tears in improving ocular symptoms during the 4-week treatment, it may have benefits on the midterm outcomes of DED. 12
When combined with artificial tear treatment, needle acupuncture had a weaker effect on TFBUT. However, it had a stronger effect on Schirmer's test and a better overall effect than artificial tear alone. 9 This outcome could be explained by the differences between the two tests. While Schirmer's test evaluates tear production, TFBUT evaluates tear film stability. Thus, the combined treatment created a synergetic effect on tear production, and not in tear stabilization. Despite the impact of manual acupuncture on the protein composition in tears, 29,30 it did not have synergetic effects when combined with artificial tears. Thus, clinicians should consider this while creating tailored treatment plans. This study revealed that LA improved all outcome measurements in the intragroup comparison, except in the Schirmer-I test at 4 weeks of treatment. Moreover, TFBUT improved in the intergroup comparison.
The tear film comprises three main layers, namely the outer lipid, the middle aqueous, and the inner mucous layers. 31 Each layer has a different composition and function. Both extrinsic and intrinsic factors can initiate or amplify the inflammatory cycle in dry eye. These factors cause tear instability and changes in tear composition, including hyperosmolarity. This activates the stress signaling pathways in ocular surface cells, thus triggering the production of innate inflammatory mediators. These mediators eventually lead to the recruitment and activation of CD4+ T cells. The production of cytokines contributes to corneal, conjunctival, and lacrimal gland epithelial disease. 32 The anti-inflammatory effect of needle acupuncture has been found to decrease proinflammatory cytokines. This has implications for chronic inflammatory conditions, such as inflammatory bowel disease, dry eye, rheumatoid arthritis, and depression. 33 –35 The analgesic effect of needle acupuncture also decreases ocular irritation, one of the most distressing symptoms of DED. 36
Needle acupuncture helps in the management of DED that occurs through dilating the blood vessels and increasing the supply of neuropeptides (e.g., calcitonin gene-related peptide). 13 Manual acupuncture can modulate the autonomic nervous system and immune system. This in turn eventually increases lacrimal secretion by stimulating the lacrimal gland. 37 –39 The mechanisms underlying needle acupuncture on DED are associated with enhancing the secretion of tear protein, regulating hormone levels and lacrimal metabolism, increasing the content of acetylcholine in the lacrimal gland, and regulating the vasoactive intestinal peptide. 40
A literature review reported on the commonly used acupoints for acupuncture therapy on DED. These included acupoints near the eyes, such as Jingming (BL1), BL2, Tongziliao (GB1), Taiyang (EX-HN5), and TE23. 41 Another study reported on the differences in acupoints in the treatment of DED. Treatment regimen, including BL2 or ST1, showed significantly weaker effects than regimens without the aforementioned acupoints. In addition, the values for other acupoints were not significantly different (BL1, TE23, ST2, Ex-HN5). 9
LA integrates the positive effects of both acupuncture and low-level laser therapy. 42 The authors used the local and distal acupoints based on the principle of “places where meridian passed; treatments thereby can be reached,” 43 including BL2. The latter is the most commonly used acupoint for DED treatment. 44 Moreover, they observed almost all improvements in the experimental group. BL2 is located at the medial end of the eyebrow, near the supraorbital nerve, which innervates the conjunctiva, thus increasing its sensitivity and tear production. Zhenjiu Daquan shed light on the treatment of all eye diseases with LI4 and GB37. 45 In addition, the study also reported on the impact of stimulation at ST36 on reducing the chronic inflammation of the ocular surface or accessory organs through vagal modulation of inflammatory responses in the internal organs. 46 Vanzini and Gallamini not only demonstrated the effectiveness of LA in vasodilation but also in the perfusion control. The latter seems to restore functionality in the central artery of the retina in patients with open-angle glaucoma. 47 The majority of the selected acupoints belong to the Yang Ming meridians, comprising qi and blood. 48 Therefore, stimulation at these acupoints can restore the circulation of qi and blood in the body organs and meridians.
One of the greatest challenges in acupuncture research is the selection of an appropriate sham acupuncture control. While several sham regimens exist, researchers have raised serious concerns about their efficacy. 49 It is challenging to design a perfect placebo control that does not have therapeutic effects, while maintaining effective masking from patients. The authors treated the participants in the sham control group with LA without laser output, which served as an appropriate placebo control.
This study had several limitations. First, the data on intervention safety were incomplete because only adverse events related to the intervention were assessed. Second, the sample size was smaller than the expectation. Although there were 2520 eligible subjects, 2461 of them were excluded for failure to meet the inclusion criteria, declining to participate, and lack of time (Fig. 1). However, the sample size of eyes per treatment group provided sufficient power (90%) to detect the difference in OSDI or TFBUT at α values of 0.05 between the experimental and control groups in this study. Third, the course of LA was 12 weeks. A longer course might have produced more obvious effects in the Schirmer-I test. Future studies should include follow-up evaluations to strengthen this conclusion.
In conclusion, under the conditions of this study, a 12-week treatment of LA in conjunction with conventional treatment was more effective in improving the OSDI and TFBUT than conventional treatment alone. Thus, LA can be utilized as an adjuvant therapy for DED, when conventional treatment does not provide satisfactory results.
Footnotes
Acknowledgments
The authors thank the Biostatistics Center, Kaohsiung Chang Gung Memorial Hospital, for statistics work.
Authors' Contributions
W.-L.H., H.-J.Y., and L.-Y.P. developed the study concept and design. W.-L.H., H.-J.Y., L.-Y.P., P.-C.W., C.-C.P., C.-E.K., and Y.-J.T. were involved in data collection. W.-L.H. drafted the article. All authors W.-L.H., H.-J.Y., L.-Y.P., P.-C.W., C.-C.P., C.-E.K., Y.-J.T., and Y.-C.H. participated in data interpretation, reviewed, revised, and approved the article.
Ethics Approval
Chang Gung Medical Foundation Institutional Review Board, IRB No. 201600333A3C503.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the Chang Gung Medical Research Fund (CMRPG8F0551, CMRPG8F0552; 2016/04/19 version 2). The funding source had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the article; and decision to submit the article for publication.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.