
Abstract
Objectives:
Although Baduanjin (a traditional Chinese physical activity) has been reported to promote general health, the optimal exercise intensity and kinematic characteristics of this intervention remain poorly understood. This investigation aimed to quantify and compare the exercise intensities of traditional standing Baduanjin (TB) and sitting Baduanjin (SB) using cardiopulmonary exercise testing, to further clarify the sources of the previously observed benefits of this modality.
Study design:
Observational study.
Interventions:
Healthy individuals were recruited to perform TB, SB, and cycling (in order) until they reached their ventilatory threshold. Intensity-relevant parameters based on type of exercise and specific time points (exercise start and the end of the 2nd, 4th, 6th, and 8th set of motion) were compared between TB and SB with ventilatory threshold as control.
Results:
Forty individuals (18 male and 22 female) completed the trial. Significant differences in peak oxygen uptake, metabolic equivalent of task, and Borg scale existed among the three exercise types, indicating a decreasing overall exercise intensity in the order of ventilatory threshold, TB, and SB. All parameters except the respiratory exchange ratio fluctuated significantly across the time points.
Conclusions:
Both TB and SB resulted in a significantly lower exercise intensity when compared with the ventilatory threshold established through cycling exercise. The benefits of Baduanjin might be explained partly by its appropriate exercise intensity and intermittent intensity pattern. Baduanjin might be a potential alternative to existing schemes for exercise rehabilitation.
Introduction
Exercise rehabilitation is beneficial to restore functionality, exercise capacity, and cardiopulmonary function. 1 Exercise-based rehabilitation programs also prevent the occurrence of comorbidities, decrease total mortality, and generally improve patients' quality of life. 2,3 Unfortunately, exercise rehabilitation is generally underappreciated and underutilized by many clinicians as well as patients partially due to its diverse applications and exercise modalities. 4
Baduanjin is a traditional Chinese exercise that has been increasing in popularity; it is classified into traditional standing Baduanjin (TB) and sitting Baduanjin (SB). 5 This form of exercise comprises eight different sets of motions, each of which consists of certain repeated movements. Previous investigations have revealed extensive applications of Baduanjin in health promotion, especially in rehabilitation. 6 Relative to more common modes of exercise, Baduanjin exercise four times per week for 6 months has been shown to improve overall physical capacities and reduce fall and fracture rates. 7 A significant improvement in reported fatigue and quality of life after Baduanjin exercise has also been reported. 8 In addition, Baduanjin is useful when treating depressive symptoms that are commonly seen in elderly individuals. 9
However, how Baduanjin differs from other common physical activities or conventional exercise rehabilitation has not been well studied. 10,11 Despite these prospects, most of the existing literature typically reports on the characteristics and benefits of Baduanjin as a whole (e.g., including all eight motions), whereas each of its eight sets of motions is believed to act differently according to the theory of Traditional Chinese Medicine. 9 Therefore, specific comparisons at the motion level may help reveal the individual benefits of Baduanjin and aid in exploration of its application in rehabilitation.
Cardiopulmonary exercise testing is a noninvasive examination that provides diagnostic and prognostic evaluation of cardiopulmonary function, and quantitatively measures the benefits of a prescribed exercise rehabilitation intervention. 12 In cardiopulmonary exercise testing, ventilatory threshold is considered to reflect the approximate location of the lactate threshold, at which the supply of oxygen to muscles fails to meet the increased demand at a given intensity. Ventilatory threshold also enables accurate assessment of aerobic fitness and submaximal endurance performance 13,14 and, therefore, indicates a balance between safety and benefit that may help determine a protocol that maximizes patient benefit. 15,16
The purposes of this investigation were to (1) quantify and compare the exercise intensity of TB and SB when compared with the ventilatory threshold by using cardiopulmonary exercise testing measurements; and (2) explore the specific benefits of TB and SB by kinematic analysis. The authors assumed that relative to cycling exercise at the ventilatory threshold, both types of Baduanjin would result in lower peak oxygen uptake (VO2peak) as well as metabolic equivalent of task (MET) in exercise.
Design and Interventions
Ethical considerations and study design
All procedures were approved by the Ethics Committee of Guangdong Provincial Hospital of Chinese Medicine (approval number: BE2020-181-01) and conducted in accordance with the Helsinki Declaration.
Healthy individuals with unrestricted exercise abilities from local communities were recruited through poster announcements and billboard advertisements for scientific studies in Guangdong Provincial Hospital of Chinese Medicine.
The inclusion criteria included (1) age 18–40 years, (2) body mass index (BMI) 18.5–24 kg/m2, and (3) not participated in any clinical research within 30 days before enrollment. The exclusion criteria included (1) symptoms or behaviors (within 3 days before enrollment) that may affect exercise capacity, including but not limited to chest tightness, dyspnea, dizziness, fatigue, cough, nasal congestion and discharge, and fever; or intake of caffeine or alcohol; (2) diagnosed with diseases that may potentially affect performance in exercise, such as cardiovascular and pulmonary diseases; (3) disorders that impact limb mobility; (4) diagnosed with claustrophobia; (5) allergic to materials that might be used in the study; and (6) anyone unable to follow the research protocol. All participants were well informed of any potential benefits and risks of participating before providing written informed consent.
All enrolled individuals were instructed to perform TB, SB, and cycle exercise in this order, while connected to cardiopulmonary exercise testing equipment (Miraclink-100P/200P, Shenzhen, Guangdong, China). The time interval between two physical activities was at least 24 h. Demographic data and vital signs were collected at baseline for reference. After being connected to the metabolic equipment, the participant rested quietly for 3 min before exercise was initiated. Cycling exercise was performed in accordance with the modified Bruce scheme. 17 For TB and SB, all individuals watched a teaching video twice and followed along with the video the third time.
The experiment was terminated when the participants reached the ventilatory threshold or fulfilled any criteria for the discontinuation of cardiopulmonary exercise testing. As there was no consensus on the definition of ventilatory threshold, 14 the V-slope and ventilatory equivalents methods were combined and determined by two experienced physicians.
Study measurements
VO2peak, MET, Borg scale (range 6–20), 18 mean systolic blood pressure, and mean diastolic blood pressure were measured in all enrolled individuals and compared between TB, SB, and ventilatory threshold. To better explore the kinematic characteristics of TB and SB, heart rate, oxygen uptake (VO2), relative VO2, carbon dioxide output, respiratory exchange ratio, minute ventilation, MET, and ventilatory equivalent of oxygen, as well as ventilatory equivalent of carbon dioxide at five specific time points (exercise start and end of the 2nd, 4th, 6th and 8th set of motion) were measured and compared with the primary endpoints VO2 and MET.
Statistical analysis
IBM SPSS statistics software (version 25.0; SPSS, Inc., Chicago) was used for statistical analysis. Skewness and kurtosis were used to assess test appropriateness. Normally distributed data are expressed as mean ± standard deviation. Non-normally distributed data are expressed as median (first quartile–third quartile). Repeated-measures analysis of variance was used to compare the differences among each group. To compare among TB, SB, and ventilatory threshold, the authors used activity (TB, SB, and cycling exercise) as a within subject factor. Time points (exercise start and end of the 2nd, 4th, 6th and 8th set of motion) were used to compare data within participants. A Greenhouse–Geisser epsilon correction was used for data not passing the Mauchly's test of sphericity. p-Values <0.05 were considered statistically significant.
Estimated sample size was calculated using R software (version 4.0.2), in which package “pwr” (version 1.3-0) was used. Based on the clinical observations and other similar studies, a sample size of 37 per group was needed with a given effect size of 0.3. The calculation was performed using a significance level of 0.05 and power of 0.8 with a two-tailed test.
Results
A total of 40 healthy individuals (18 male and 22 female) aging 21–26 years (23.3 ± 1.4) were enrolled by local advertisements in this study and completed the trial at Guangdong Provincial Hospital of Chinese Medicine in Guangzhou, China (Fig. 1). Exercise parameters for TB, SB, and ventilatory threshold are presented in Table 1.
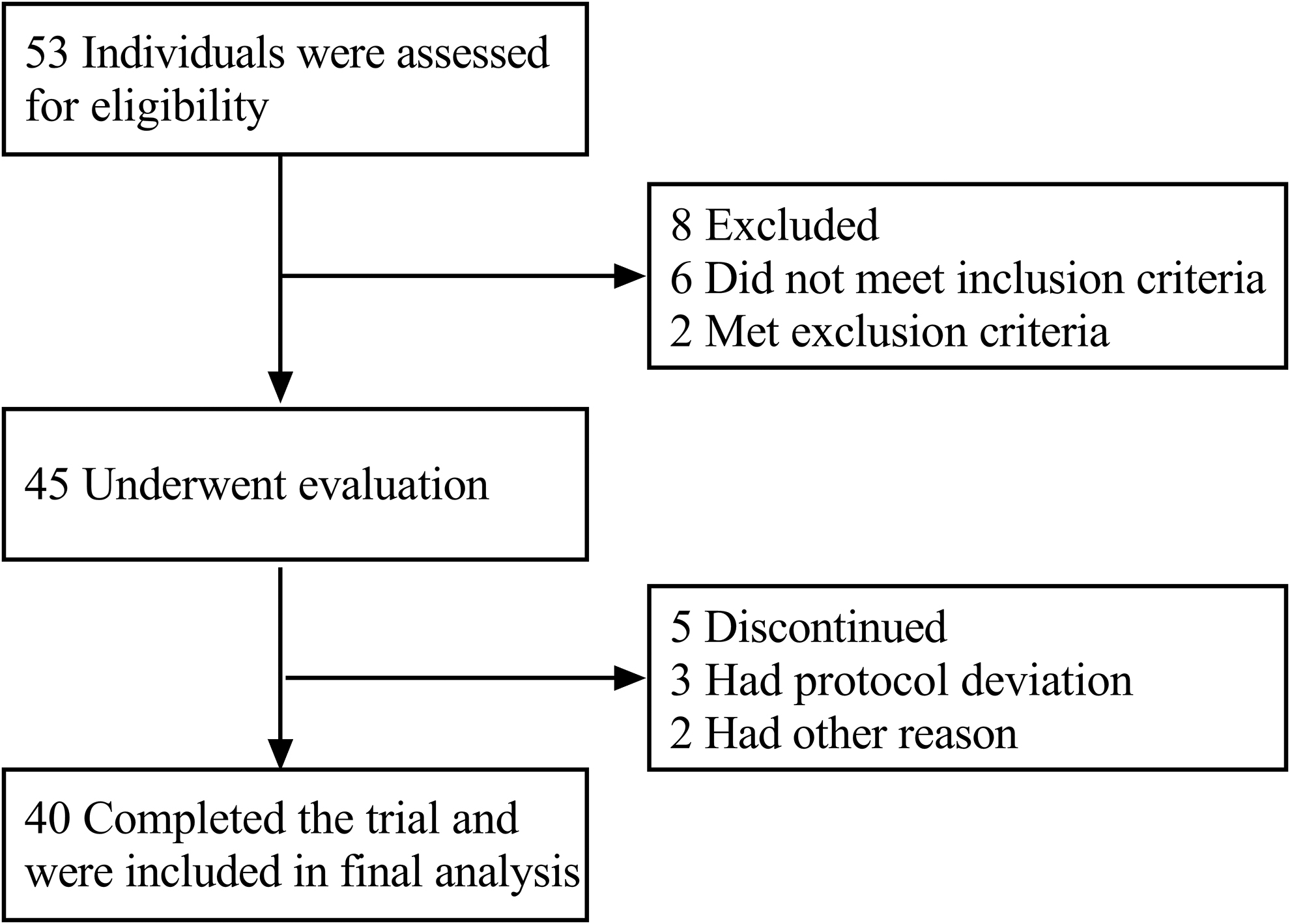
Flowchart of the study.
Exercise Parameters for Traditional Standing Baduanjin, Sitting Baduanjin, and Ventilatory Threshold
Greenhouse–Geisser epsilon correction was adapted for data not passing Mauchly's test of sphericity.
p < 0.05.
MDBP, mean diastolic blood pressure; MET, metabolic equivalent of task; MSBP, mean systolic blood pressure; SB, sitting Baduanjin; TB, traditional standing Baduanjin; VT, ventilatory threshold; VO2peak, peak oxygen uptake.
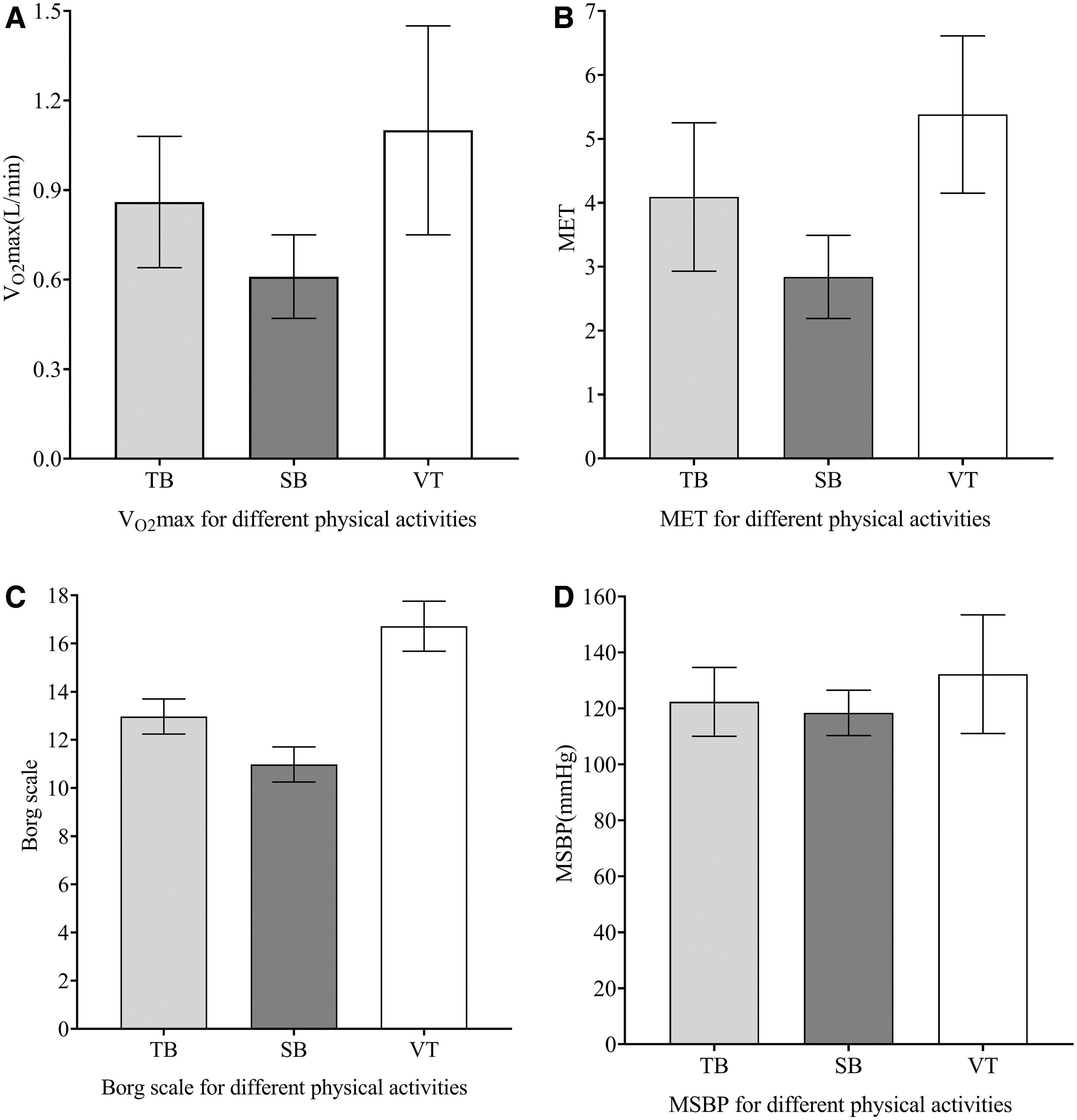
A significant decrease in overall exercise intensity in the order of ventilatory threshold, TB, and SB was detected in the study. MET (Greenhouse–Geisser corrected: F = 96.948, d.f. = 2.76, p < 0.001) for TB and SB were lower than for ventilatory threshold. The data also suggested differences in VO2peak (Greenhouse–Geisser corrected: F = 63.433, d.f. = 2.76, p < 0.001), Borg scale (Greenhouse–Geisser corrected: F = 616.576, d.f. = 2.76, p < 0.001), and mean systolic blood pressure (Greenhouse–Geisser corrected: F = 13.18, d.f. = 2.74, p < 0.001) among the three activities, whereas the value of mean diastolic blood pressure (Greenhouse–Geisser corrected: F = 2.015, d.f. = 2.74, p = 0.148) did not differ significantly (Fig. 2).
The results of repeated measure analysis of variance for comparison of VO2peak
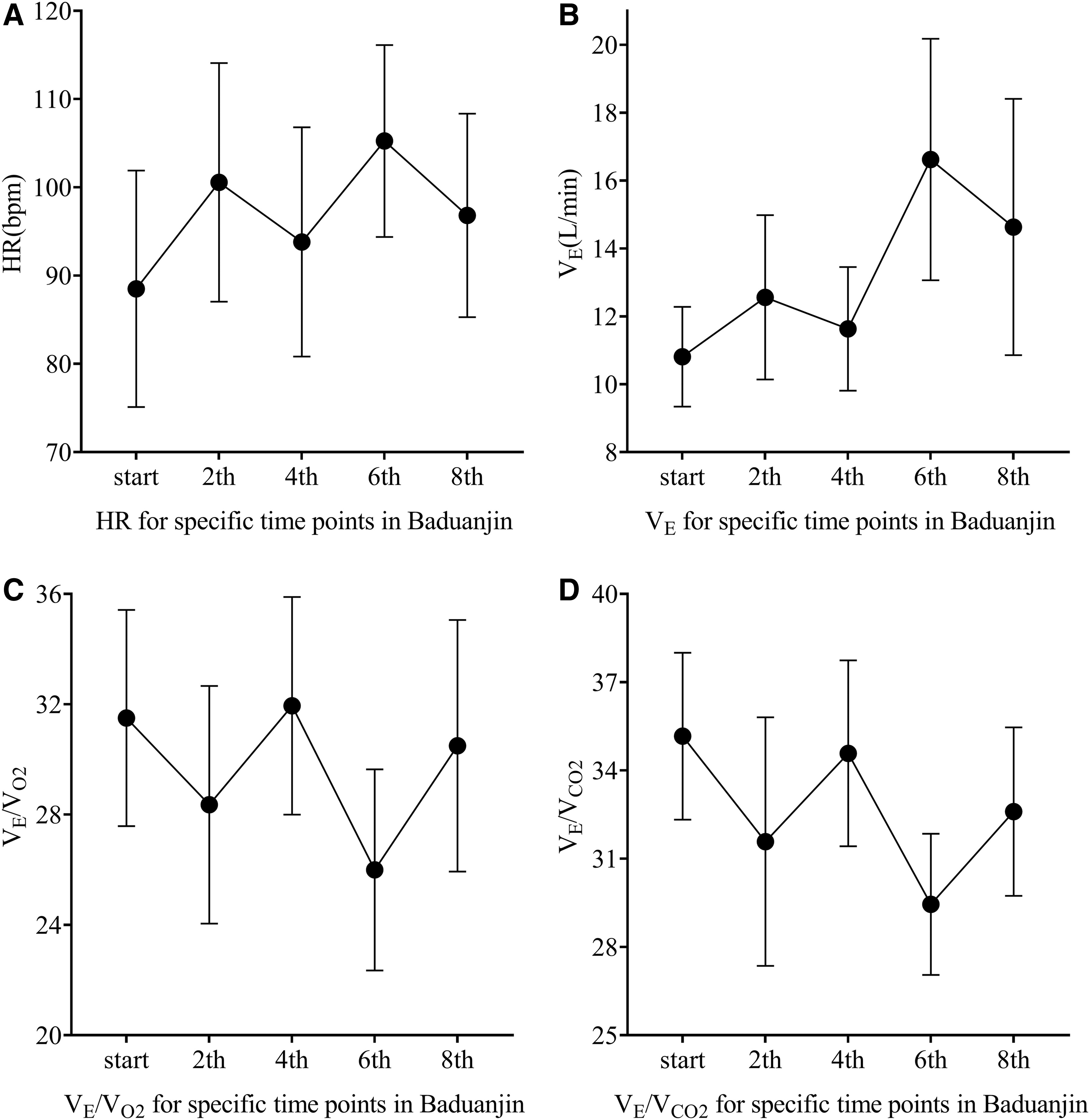
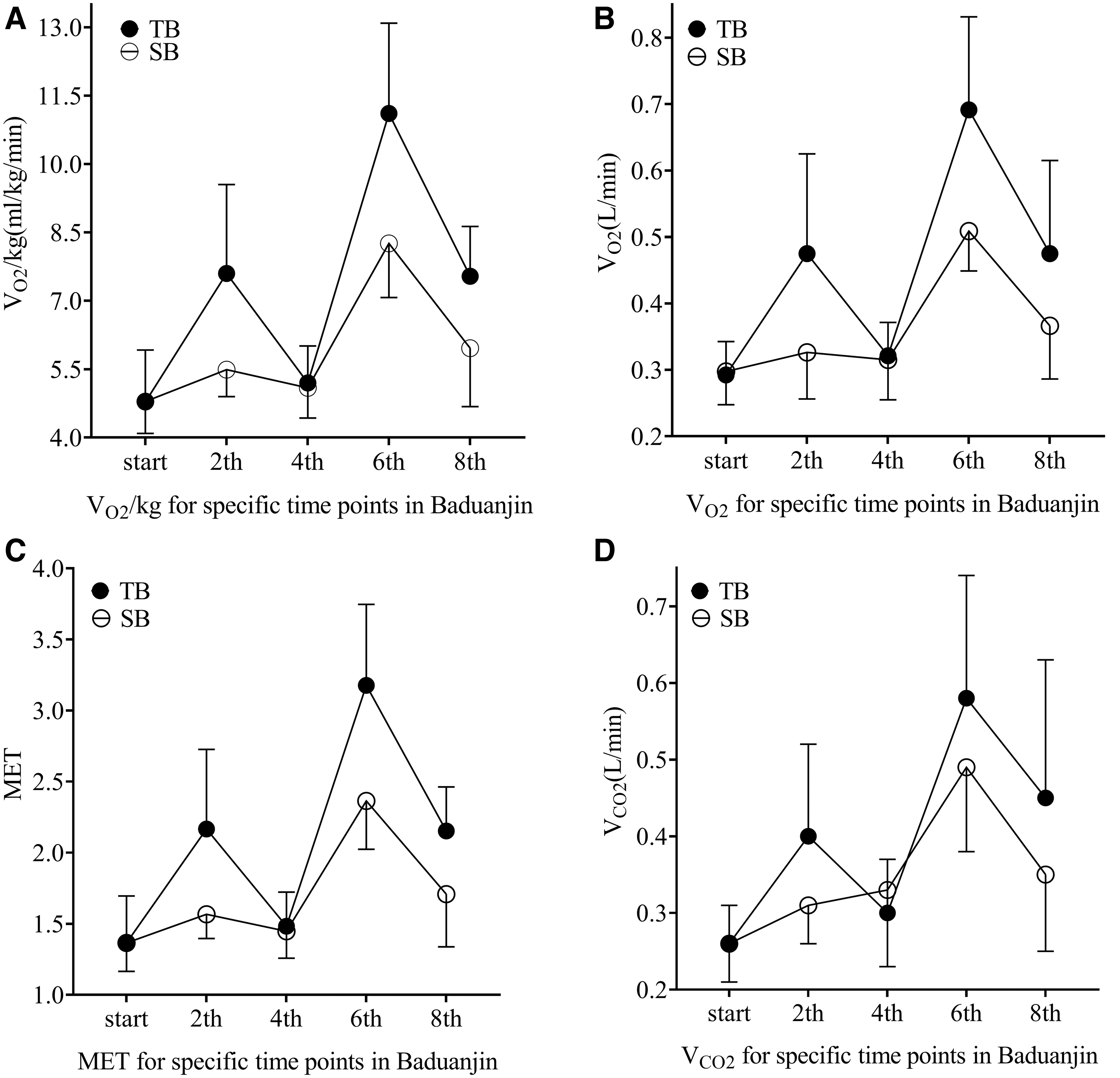
The parameters of TB and SB were also compared at exercise onset and the end of the 2nd, 4th, 6th, and 8th set of motion (Table 2), in which the measurements for TB were generally higher than for SB. Repeated-measures analysis of variance showed significant differences for time effect in heart rate (F = 25.227, d.f. = 4.56, p < 0.001), relative VO2 (F = 64.061, d.f. = 4.56, p < 0.001), VO2 (F = 54.124, d.f. = 4.56, p < 0.001), carbon dioxide output (F = 29.438, d.f. = 4.56, p < 0.001), minute ventilation (F = 20.256, d.f. = 4.56, p < 0.001), MET (F = 64.132, d.f. = 4.56, p < 0.001), ventilatory equivalent of oxygen (F = 7.569, d.f. = 4.56, p < 0.001), and ventilatory equivalent of carbon dioxide (F = 15.62, d.f. = 4.56, p < 0.001), whereas the respiratory exchange ratio (F = 1.834, d.f. = 4.56, p = 0.135) was not statistically different among different time points (Figs. 3 and 4).
Results of repeated measure analysis of variance for comparison of HR
Results of repeated measure analysis of variance for comparison of VO2/kg
Parameters of Traditional Standing Baduanjin and Sitting Baduanjin at Exercise Start and End of the 2nd, 4th, 6th, and 8th Set of Motion
HR, heart rate; MET, metabolic equivalent of task; Relative VO2, oxygen uptake per kilogram body weight; RER, respiratory exchange ratio; SB, sitting Baduanjin; TB, traditional standing Baduanjin; VCO2, carbon dioxide output; VE, minute ventilation; VE/VCO2, ventilatory equivalent of carbon dioxide; VE/VO2, ventilatory equivalent of oxygen; VO2, oxygen uptake.
Discussion
In this observational study, the authors evaluated the exercise intensity of TB and SB and compared the results with each participant's ventilatory threshold to test the hypothesis that TB and SB result in lower VO2peak and MET in exercise. In addition, they examined exercise characteristics at specific time points during TB and SB to better document their source of benefits to rehabilitation. The results showed a lower overall intensity of TB and SB compared with ventilatory threshold, which supported the hypothesis. Exercise parameters, such as relative VO2, VO2, carbon dioxide output, and MET, were also significantly different at different time points for TB and SB.
Although many researchers have identified benefits of Baduanjin as a form of exercise, the kinetic characteristics have not been well characterized. To the best of the authors' knowledge, this is the first investigation to describe and compare the characteristics of TB and SB through cardiopulmonary exercise testing. The data indicated significant differences among TB, SB, and ventilatory threshold by MET (Table 1), for which TB and ventilatory threshold were classified as moderate-intensity activities, whereas SB was classified as light intensity. 19 As ventilatory threshold serves as a reference for setting target heart rate in exercise prescriptions of rehabilitation, and both TB and SB were lower than the ventilatory threshold in MET, these results may help identify a safe and efficacious intensity of Baduanjin for use as an exercise intervention.
Moreover, the Borg scale of SB in this study was 10.98 ± 0.73, with a variation in heart rate from 87.5 ± 13.74 to 102.38 ± 12.13. These parameters are in line with the recommended Borg scale (≤11) guidelines and heart rate (≈10–20 beat per minute increases in resting heart rate) for stroke survivors at the stage of hospitalization and early convalescence. 18 The kinetics characteristics of TB also fulfilled requirements for aerobic large-muscle activities in terms of the variation of VO2, heart rate, Borg scale (11–14) and duration as well as an integrated process with warm-up and cool-down activities. Therefore, the data suggest that TB and SB might be applied for rehabilitation based on the characteristics of the movement and the established recommendations for rehabilitation programs. 20
Despite numerous studies exploring the benefits of Baduanjin, 7 –9,21 it remains unclear how Baduanjin exercise improves health. 6 Crucially, the intensity of TB reaches the same MET level as fast walking and bicycling, whereas the intensity of SB in MET corresponds to slow walking and seated exercises. 19 As both TB and SB have been found to bring additional benefits to health in comparison with the aforementioned physical activities with similar MET level to Baduanjin, 7,8 the findings suggest that Baduanjin might contribute to health in a way independent of intensity itself.
In this study, parameters such as VO2 and MET for different time points in TB and SB fluctuated significantly. Conversely, heart rate, minute ventilation, ventilatory equivalent of oxygen, ventilatory equivalent of carbon dioxide, and carbon dioxide output (Figs. 3 and 4) increased gradually throughout the exercise (Table 2), representing the change in breathing efficiency during the practice of TB and SB. However, large variations in VO2, relative VO2, and MET for TB and SB at different time points were also observed (Fig. 4). Such findings suggest that an M-shaped curve of intensity for TB and SB may exist, in which the values corresponding to TB are higher than for SB. The largest differences between TB and SB appeared at the 2nd and 6th sets of motion, when more muscles and joints (mainly the upper body) were involved and mobilized.
During exercise, the efficiency of pulmonary gas exchange (detected by the efficiency of oxygen utilization) was higher in TB than in SB, whereas the ventilatory efficiency did not differ. This result could be attributed partly to the increased intensity in exercise. More importantly, the authors' observation verified unique kinetic characteristics for both TB and SB with regular fluctuation, which might help explain the desirable values of the Borg scale for TB (12.97 ± 0.73) and SB (10.98 ± 0.73) in the study, and why Baduanjin was better tolerated in previous investigations. 8,18
Considering that each Baduanjin motion consists of repeated movements with short rest intervals, and that a regular fluctuation of intensity was observed in this study, this type of exercise could be considered as a special form of moderate-intensity intermittent training, 22 indicating lower-intensity training—instead of high-intensity intermittent training—induces similar or more benefits to health promotion when compared with traditional continuous aerobic training. 23
Generally, the superiority of moderate- and high-intensity intermittent training comes from the mode and intensity of exercise, of which the latter has been reported to correlate positively with overall benefits. 24 Recent evidence suggests that intermittent training, rather than continuous activity, may have positive impacts on maximal VO2 and blood lipids that are independent of exercise intensity, 25 which were also observed in this study. In addition, lower intensity exercise has also been shown to be effective at eliciting positive health benefits while reducing the risks of injury. 26 More importantly, increased adherence and accumulated benefits from regular movement were observed for activities with moderate intensity such as walking and sitting exercise in comparison with those with high intensity. 27,28 Hence, Baduanjin has shown the potential to serve as alternative mode of exercise for exercise-based rehabilitation programs.
Furthermore, Baduanjin exercise is characterized by regular use of important muscles and joints such as the shoulder and the hip, which has been associated with lower all-cause and cardiovascular disease mortality risk. 29 In addition, the stress on unity of motion and spirit in Baduanjin helps to co-ordinate mind and body and, therefore, fully enhance health, 30 suggesting its potential as a transition of exercise intensity from low to high. Collectively, the benefits of Baduanjin may be explained at least partly by its appropriate exercise intensity and intermittent intensity pattern with regular fluctuations, which likely improves long-term adherence to exercise and rehabilitation.
Limitations
There are several limitations of this study. As described previously, there are eight sets of movements in Baduanjin, which mean that at least nine specific time points (at the start and end of each set of motion) should be observed independently. However, only five of them were measured and compared herein. As each set of motion differs during the exercise of Baduanjin, different conclusions may be reached when the whole process is monitored and compared throughout the duration of the entire program. The statistical power of this investigation is also limited by its relatively small sample size and the use of multiple comparisons.
In addition, the authors only enrolled healthy young adult individuals with a normal BMI, which does not represent older individuals or those with chronic disease. Besides, although TB, SB, and ventilatory threshold testing were performed by the same individual and were analyzed with repeated-measures analysis of variance in the study, bias from potential confounding factors such as exercise habit was not eliminated. Finally, previous experiences with Baduanjin or cycling should be taken into consideration. In this study, each participant was required to watch the teaching video twice before engaging in formal exercise. However, 28 of 40 individuals had learned Baduanjin before enrollment. Therefore, further studies with a larger sample size, including individuals with a broader age range and varied health status, are required to verify the authors' observations.
Conclusions
This investigation was the first to show a lower overall exercise intensity when compared with the ventilatory threshold in TB and SB. The benefits of Baduanjin may be partially explained by its intermittent intensity pattern, which likely confers good adherence. Baduanjin may be an especially effective means of improving adherence to exercise-based rehabilitation programs.
Footnotes
Authorship Confirmation Statement
D.X. designed the study protocol and provided supervision. J.L., B.W., L.L., Y.D., B.Z., Z.H., and M.L. jointly contributed to recruitment, data collection, and data management of the study. J.L. performed statistical analysis and drafted the article. All authors have reviewed and approved of the article before submission.
Acknowledgments
The authors appreciate Qian Li and Leshi Huang for their assistance with this study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The study received grant support from the Research Centre of Health Services and Industry Development of Traditional Chinese Medicine of Guangdong Province, Guangzhou University of Chinese Medicine (grant number 2020YJZX018). The funding agency played no role in study design, data collection, analysis, interpretation, report writing, or decision to submit for publication.