
Abstract
Objective:
The aim of this systematic review with meta-analysis was to describe the status on the effects of physical scar treatments on pain, pigmentation, pliability, pruritus, scar thickening, and surface area.
Design:
Systematic review and meta-analysis.
Subjects:
Adults with any kind of scar tissue.
Interventions:
Physical scar management versus control or no scar management.
Outcome measures:
Pain, pigmentation, pliability, pruritus, surface area, scar thickness.
Results:
The overall results revealed that physical scar management is beneficial compared with the control treatment regarding the management of pain (
Conclusions:
Physical scar management demonstrates moderate-to-strong effects on improvement of scar issues as related to signs and symptoms. These results show the importance of specific physical management of scar tissue.
Introduction
Physical scar management represents an important field in science, as scars can negatively impact the quality of life of patients. 1,2 Disturbing perceptions such as pain, tenderness or itchiness on the one hand, and functional limitations in the form of contractures on the other, are consequences of problematic scars. In addition, scar esthetics can also have a negative influence on psychosocial factors. 3 –6 The restoration of injured skin requires a complex sequence of physiological interactions to form appropriate scar tissue and repair the dermal lesion. 7 Any dysfunction in the wound healing process may result in excessive scar tissue formation. 8 Hypertrophic scars or keloids are the results of such deviant wound healing. 9 Different therapy options, described in the literature include chemical, physical, and surgical methods. 10 The physiotherapist focuses on conservative modalities in the treatment of scar tissue. These physical scar management options can be grouped into mechanotherapy, occlusive and hydrogenatic therapies, and light therapy, whereby often combinations are used. 11 The purpose of physical scar management concentrates primarily on the prevention of an aberrant healing process of the skin. 12 To date, the effects of physical scar management are still controversially discussed in literature and previous reviews focus on the treatment of hypertrophic scars and keloids after burn injuries. 11,13,14 Consequently, the aim of this systematic review and meta-analysis was to evaluate the effectiveness of physical scar management on different symptoms in adults with any kind of scar tissue.
Methods
Research question
The research question was defined following the PICO model. 15 Population: Adults with scar tissue; Intervention: Physical scar management; Comparator: Control intervention or no treatment; Outcome: Pain ratings, pigmentation, pliability, pruritus, scar surface area, and scar thickness. The choice for the outcome variables was based upon the fact that physical interventions will have a direct influence on gaining functional, physical, and psychological improvements 12 and because these parameters show valuable signs that account for therapy progression. 16
Search strategy
An electronic search was conducted up to January 2020 on the databases PubMed (Medline), Cochrane Central Register of Controlled Trials (CENTRAL), and Physiotherapy Evidence Database (PEDro). Tissue-related keywords were combined with treatment-related keywords by using the Boolean operator “AND.” Tissue or treatment-related keywords themselves were combined with the function “OR.” The keywords used were proven for MeSH-terms (Table 1).
Overview of Keywords and Combinations
The
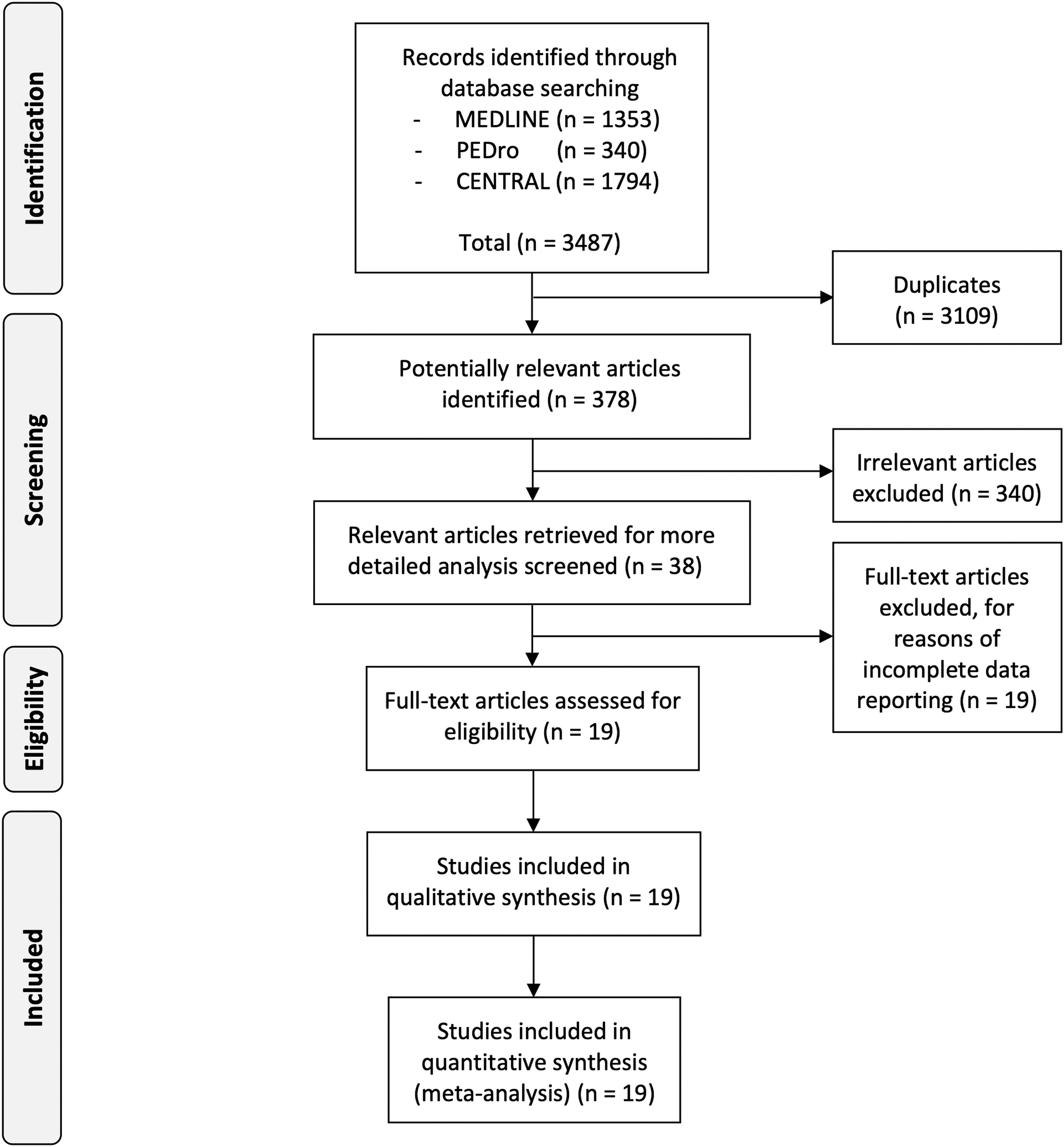
PRISMA flow chart describing the selection process.
Data extraction and quality assessment
Data were manually extracted from the included studies by three researchers (C.D., E.H., R.S.), independently from each other. In case of disagreement, a fourth researcher (R.C.) checked the variable and agreement was sought by consensus. The methodological quality of the studies was assessed with the Cochrane Risk of Bias Tool (Version 1). 17 Two researchers independently evaluated the 19 studies (E.H., R.S.). A third researcher (R.C.) rated in case of disagreement.
Data analysis
Comprehensive Meta-Analysis II software (CMA II; Biostat, Inc., Englewood, NJ) was used to conduct the meta-analysis calculations. A random-effects model was used to account for the fact that the included studies were not exact replicates of each other. Weighting factors were calculated based on the DerSimonian and Laird inversed-variance method.
18
As most of the eligible studies used small samples, the individual studies' effect sizes were standardized and expressed as Hedges' g. The corresponding 95% confidence intervals (95% CI) around the individual studies' effect sizes as well as around the overall weighted estimate were calculated. Cohen's benchmarking for effect size interpretation was followed: g < 0.20 (negligible effect), g between 0.20 and 0.49 (small effect), g between 0.50 and 0.79 (moderate effect), and g > 0.80 (large effect).
19
The null hypothesis of no heterogeneity (i.e., that all studies have a common effect size) was tested using the Cochran's Q-test. The Q-value, the corresponding degrees of freedom (df(Q)) as well as the corresponding exact
If a study showed an extreme effect size, a sensitivity analysis was conducted by excluding this study from the meta-analysis. An extreme effect size was defined, when the study's CI does not overlap with the CI of the pooled effect. The likelihood for publication bias was not tested because of less than 10 studies included in the different meta-analyses. 21
Results
Risk of bias analysis
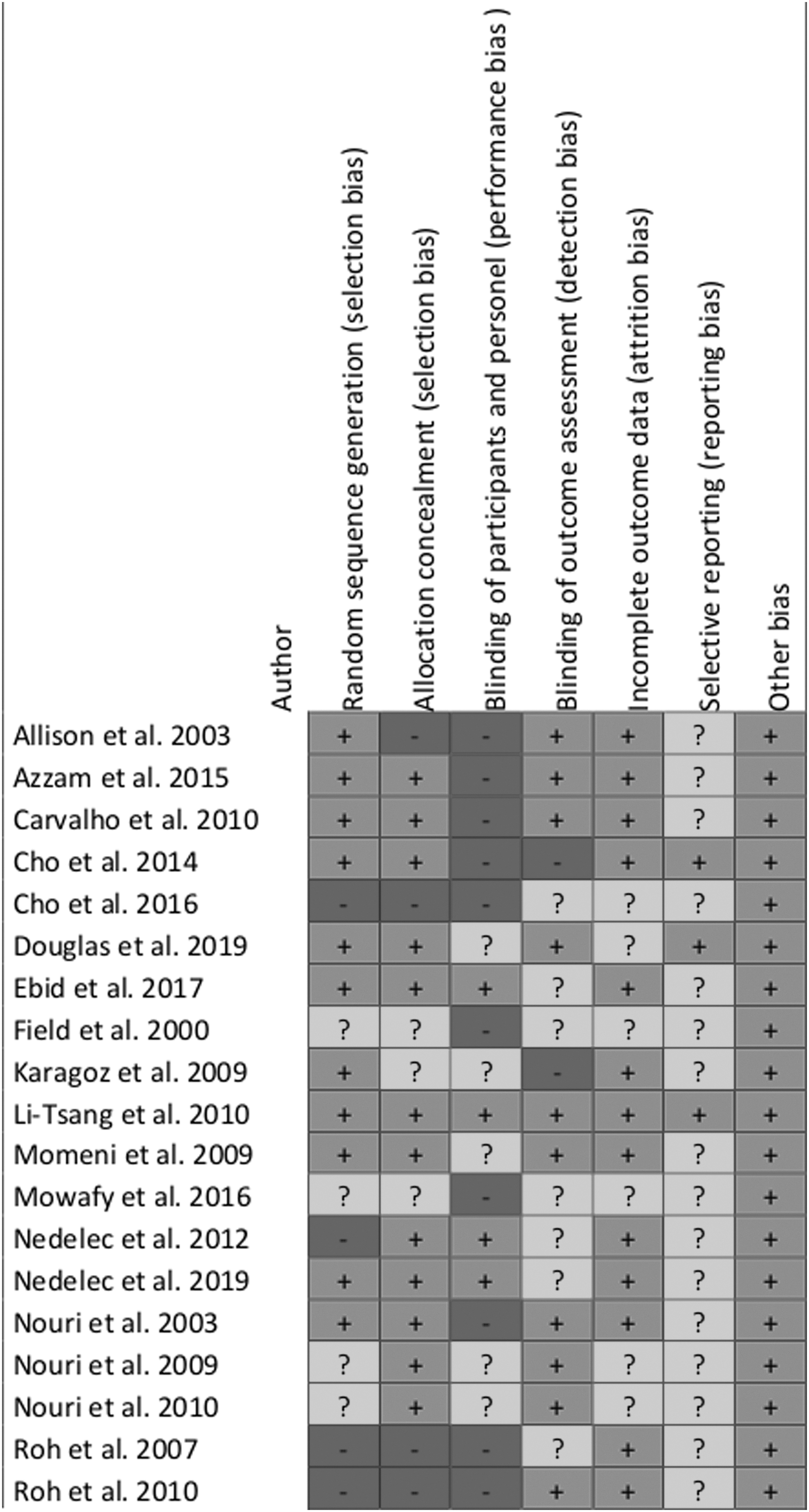
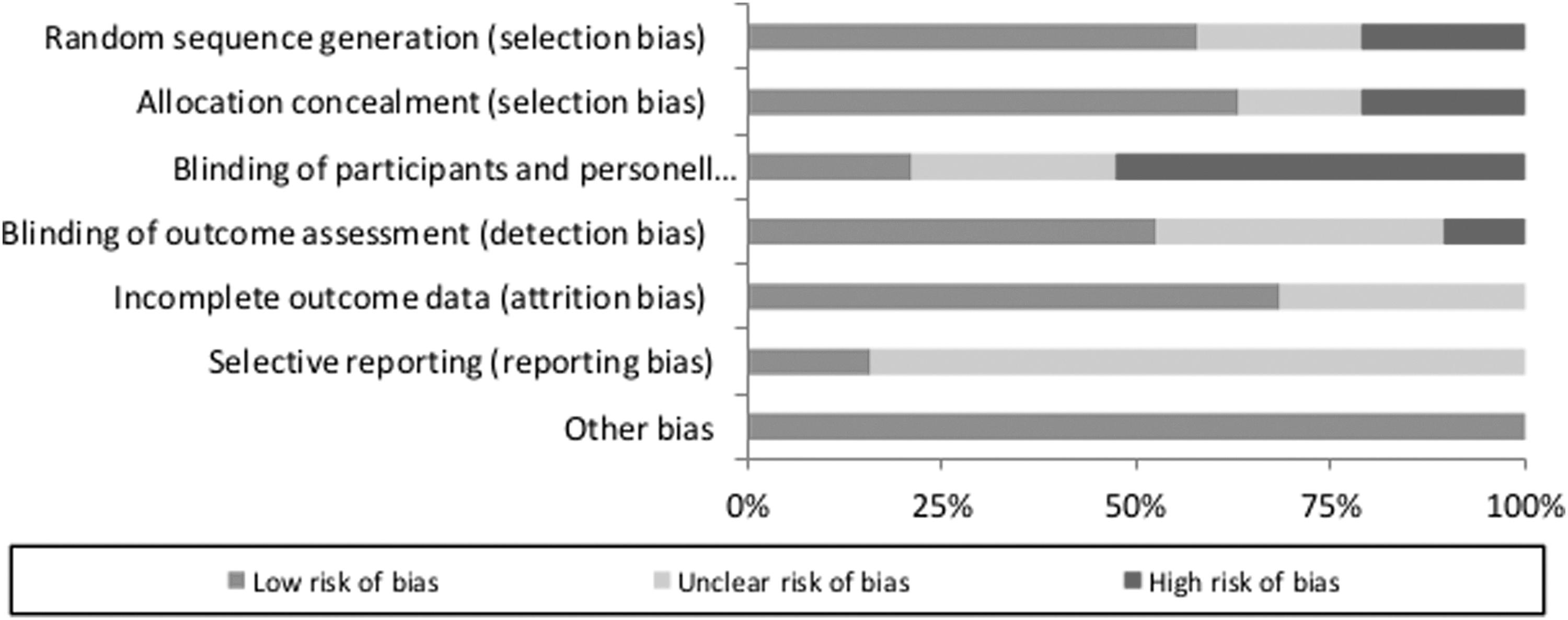
The risk of bias analysis demonstrated a high risk for performance bias with 47% (blinding of participants and personnel). The reporting bias stayed unclear in 84% of the observed studies due to unclear or insufficient information. A low risk of selection (63%), attrition (68%), and other bias (100%) could be observed throughout the studies (Figs. 2 and 3).
Risk of bias graph for each included study.
Risk of bias summary for all included studies.
Study characteristics
In the present work, 13 studies investigated burn scars. These included seven studies with burn scars, 22 –29 five with hypertrophic burn scars, 28,30 –33 and one with hypertrophic scars after burns, scalds, or other skin traumata. 34 Five studies focused on postsurgical scars, 35 –39 of which one concentrated specifically on hypertrophic and keloid scars. 39 Finally, one study included all kinds of hypertrophic and keloid scars. 40 Seven studies divided the scars into two or three halves to perform the intervention and control treatment on the same subject, 13,29,32,36 –38,40 whereas the other 12 studies analyzed scars of independent groups of subjects. 22,24 –28,30,31,33 –35,41 The intervention methods can be categorized into (1) mechanotherapy (massage, 26 –28,30,33 extracorporeal shockwave therapy (ESWT) 24,25 ), (2) occlusion and hydration therapy (silicone application, 31,32,34 moisturizing cream with protease enzymes 41 ), and (3) light therapy (noninvasive laser 22,29,35 –40 ). Table 2 gives a summary of the included studies.
Characteristics of the Included Studies
CG, control group, CO2, carbon dioxide, ESWT, extracorporeal shockwave therapy, f, females, FA, final analysis, HILT: high-intensity laser therapy, IG, intervention group, LLLT GA1As, low-level laser therapy, m, males,
Pain ratings
Pain ratings were evaluated in nine studies.
22,24,25,27,29,30,32,34,35
Of these, six studies measured pain with the visual analog scale (VAS),
22,25,27,30,34,35
two applied the Vancouver scar scale (VSS),
29,32
and one the numeric rating scale.
24
Two studies each treated the scars with massage therapy,
27,30
ESWT,
24,25
laser therapy,
22,35
and gel sheets,
32,34
and one study with a CO2 laser.
29
To test the hypothesis that physical therapy interventions had an enhancing effect to decrease pain as compared with control, an overall meta-analysis was conducted. Figure 4 shows that, in this set of sampled studies, physical scar management had a large and statistically significant effect on pain reduction compared with the control interventions (Hedges' g = −0.95 [95% CI: −1.69 to −0.20]). The observed heterogeneity was high and statistically significant (Q = 81.5; df(Q) = 8;
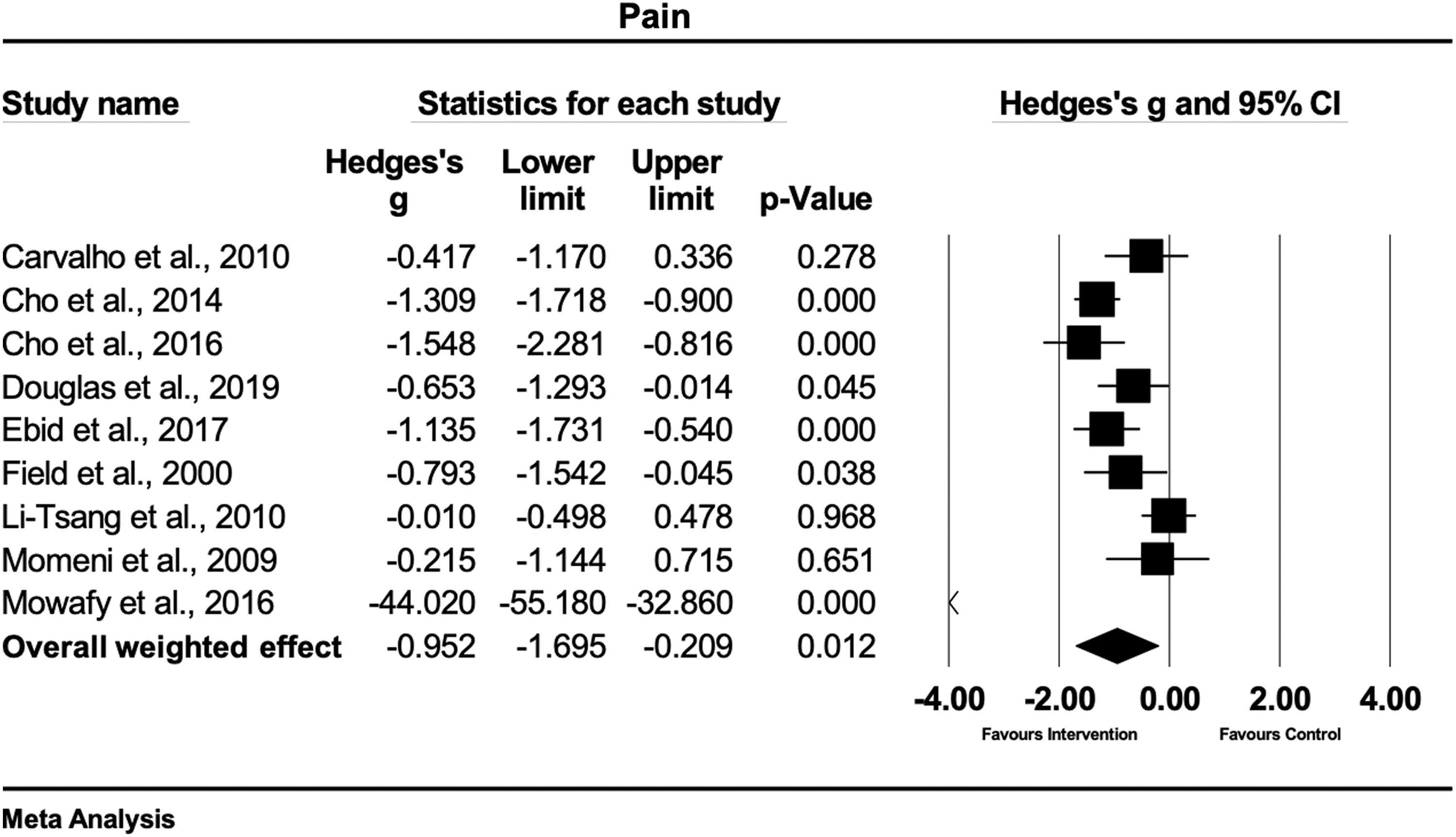
Forest plot of the meta-analysis illustrating the overall weighted effect size of physical therapy versus control on pain in patients with scar tissue. The
A sensitivity analysis was conducted since one study showed an extreme effect size.
25
The results of the sensitivity analysis show a moderate and statistically significant effect on pain reduction compared with the control interventions (Hedges' g = −0.77 [95% CI: −1.18 to −0.36]). The sensitivity analysis decreased the observed heterogeneity, but remained high and statistically significant (Q = 23.95; df(Q) = 7;
Pigmentation
Five studies investigated the effects of physiotherapy on pigmentation, using the VSS.
28,31,32,37,38
One study treated scars with massage therapy,
28
two with silicone applications,
31,32
while two studies used laser therapy.
37,38
Figure 5 shows that, based on this set of studies, there is evidence that physical scar management has a moderate and statistically significant effect compared with the control treatment on pigmentation (Hedges' g = −0.72 [95% CI: −1.27 to −0.17]). The heterogeneity was moderate and statistically significant (Q = 13.5; df(Q) = 4;
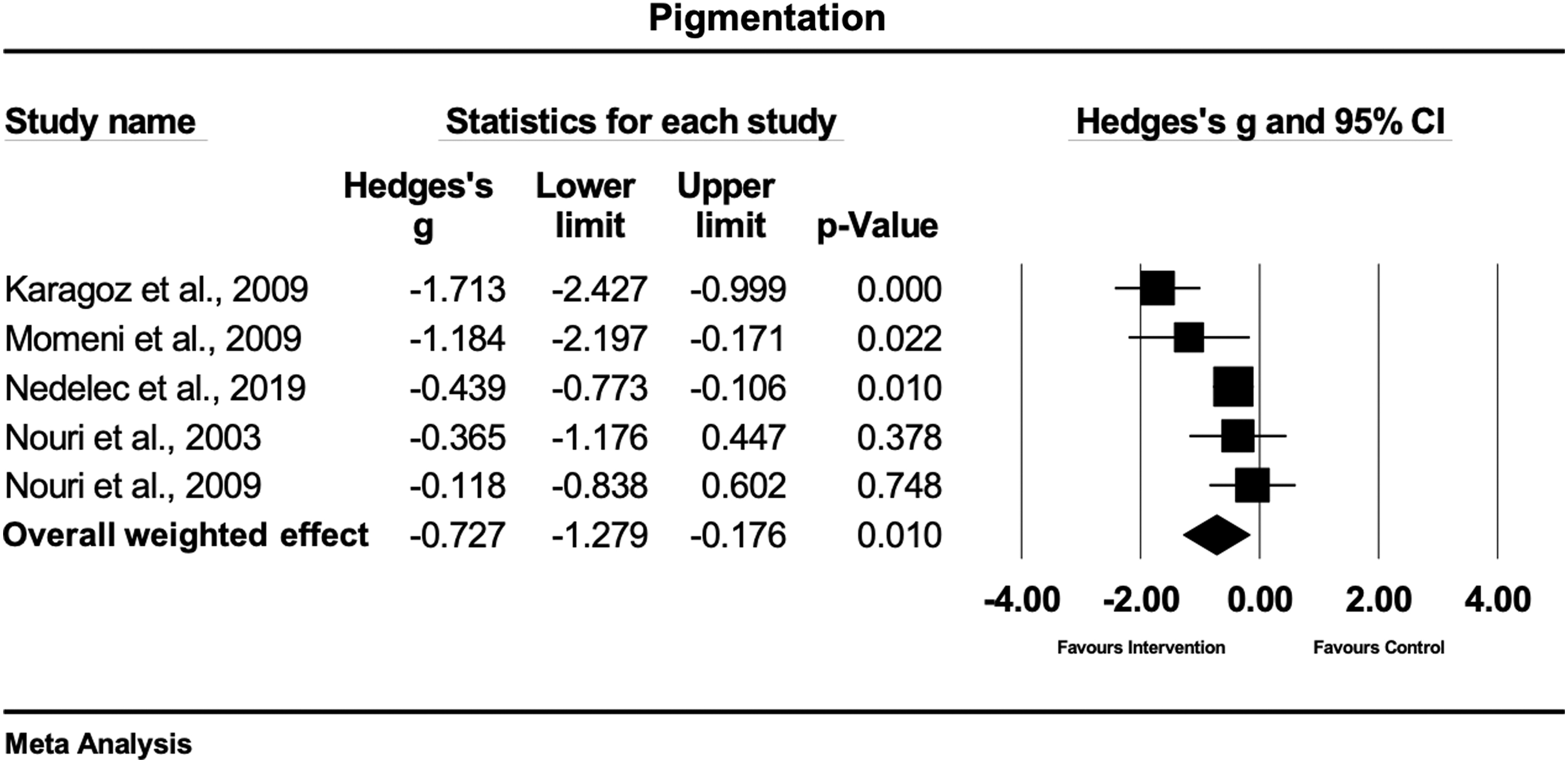
Forest plot of the meta-analysis illustrating the overall weighted effect size of physical therapy versus control on pigmentation in patients with scar tissue. The
Pliability
Pliability was evaluated in seven studies.
31
–34,36,37,39
Six studies used the VSS,
31
–34,36,37
while one study used a 5-point Likert scale,
39
for the quantification of pliability. Three studies treated the scars with laser therapy,
36,37,39
three studies with gel sheets,
31,32,34
and one study with massage therapy.
33
The overall weighted effect size of physical (conservative) treatment as compared with control treatment in this set of scar studies, was large and statistically significant (Hedges' g = −1.29 [95% CI: −1.88 to −0.70]), favoring the physical scar management (Fig. 6). The observed heterogeneity was moderate but statistically significant (Q = 23.7; df(Q) = 6;
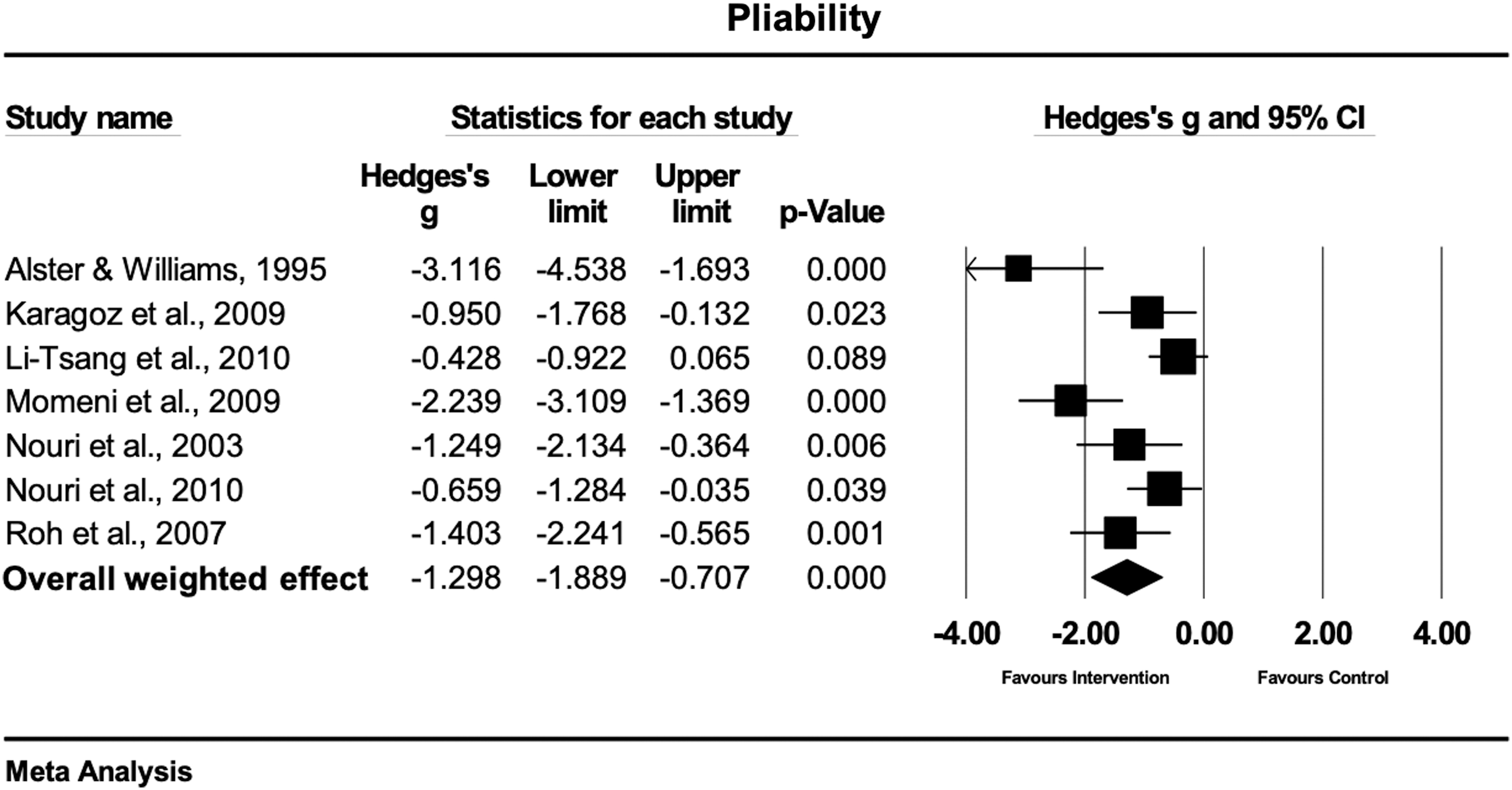
Forest plot of the meta-analysis illustrating the overall weighted effect size of physical therapy versus control on pliability in patients with scar tissue. The
Pruritus
Five studies compared the effects between physical scar management and a control condition on pruritus.
29,30,32,34,41
Two studies evaluated pruritus with the VSS,
29,32
while the other studies used a VAS
34,41
or an itching scale.
30
Two studies treated the scars with gel sheets,
32,34
one study each with massage therapy,
30
CO2 laser therapy,
29
and moisturizing cream with protease.
41
In this sampled set of studies, the overall weighted effect revealed that conservative therapy had a large and statistically significant effect on pruritus compared with the control condition (Hedges' g = −0.99 [95% CI: −1.54 to −0.44]) (Fig. 7). The heterogeneity of the included studies was high and significant (Q = 17.0; df(Q) = 4;
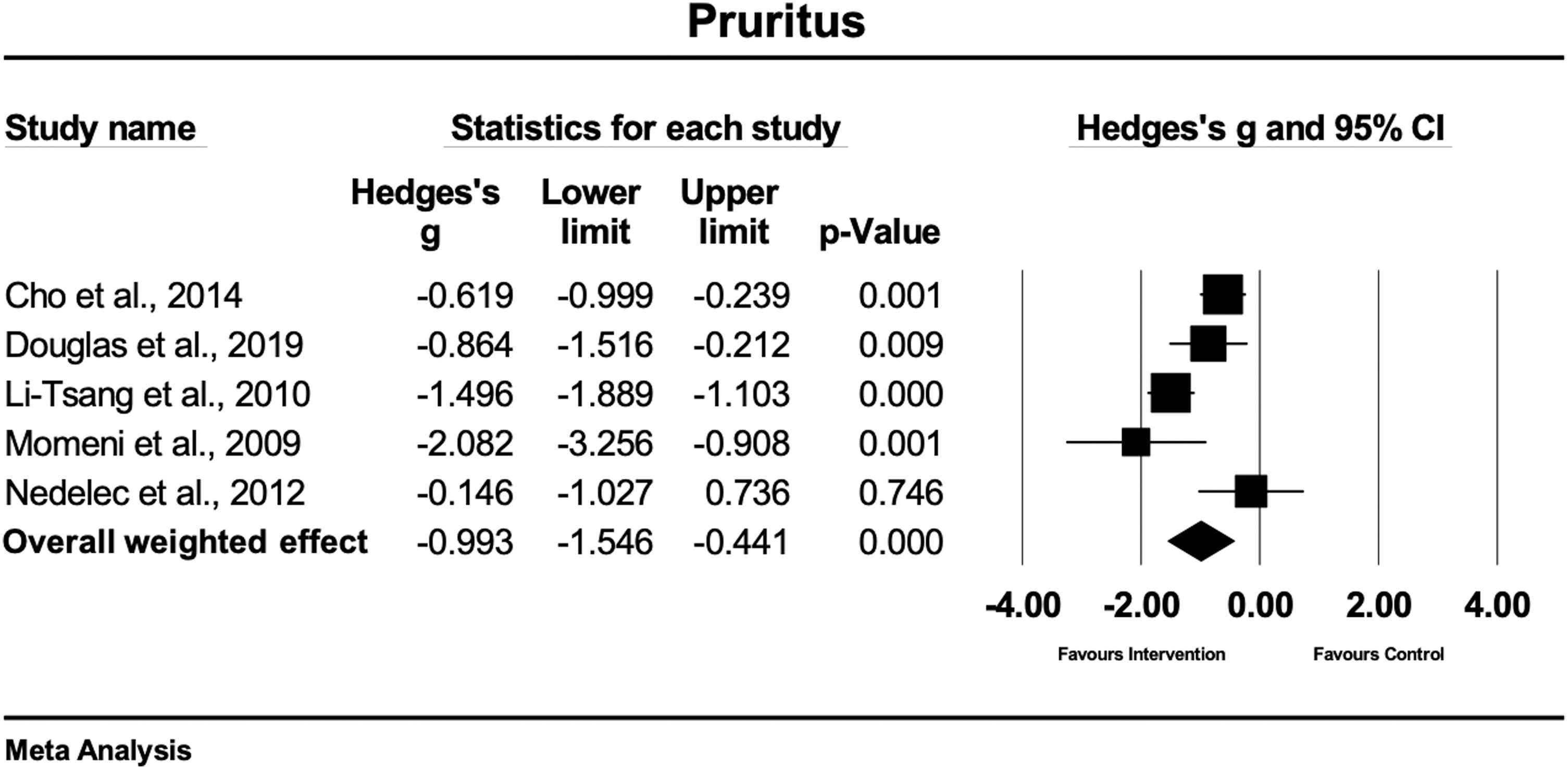
Forest plot of the meta-analysis illustrating the overall weighted effect size of physical therapy versus control on pruritus in patients with scar tissue. The
Surface area
Two studies met the inclusion criteria of evaluating the effects of conservative therapy versus a control condition on the surface area of the scar.
39,40
All of them used different assessment methods comprising Magiscan digital image processing system
39
and scar tissue biopsy.
40
Each study applied laser therapy as physical scar management. The overall weighted effect size in this sample of studies was large and statistically significant (Hedges' g = −1.72 [95% CI: −2.12 to −1.33]) (Fig. 8). The observed heterogeneity was low and statistically not significant (Q = 0.70; df(Q) = 1;
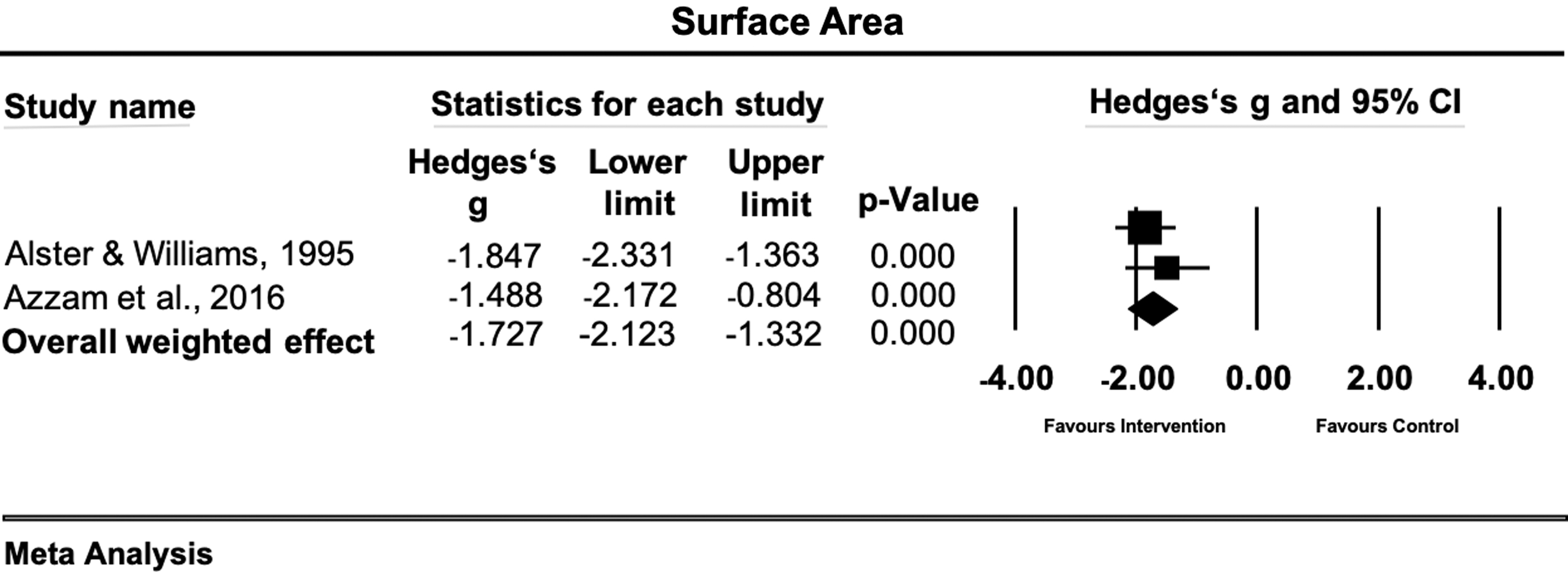
Forest plot of the meta-analysis illustrating the overall weighted effect size of physical therapy versus control on surface area in patients with scar tissue. The
Scar thickness
A total of 10 studies evaluated the effects of physical scar management versus the control condition of scar thickness.
26,28,30,32,33,34,36
–39
The evaluation techniques were ultrasonography,
26,28,30
tissue ultrasound palpation system,
34
VSS subscale height,
31,33,36
–38
and caliper measurements.
13,39
Four studies treated the scars with laser therapy,
36
–39
four studies with massage therapy,
26,28,30,33
and two studies with gel sheets.
31,34
The meta-analysis of the effect sizes extracted from this set of studies showed that physical scar management had a moderate and statistically significant effect on scar thickness reduction compared with the control group (Hedges' g = −0.68 [95% CI: −1.27 to −0.09)] (Fig. 9). The observed heterogeneity was high and statistically significant [Q = 81.0; df(Q) = 9;
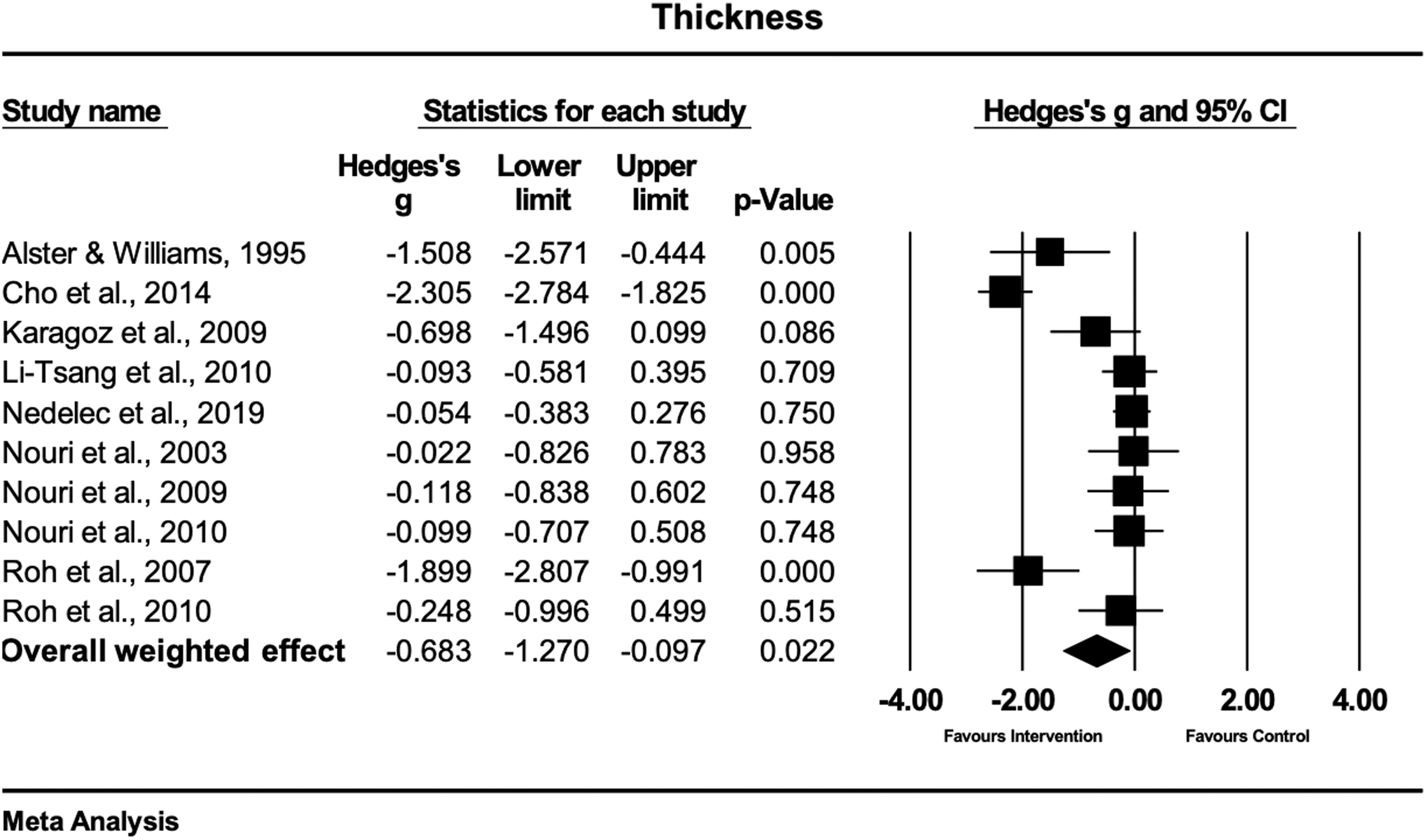
Forest plot of the meta-analysis illustrating the overall weighted effect size of physical therapy versus control on scar thickness in patients with scar tissue. The
Discussion
The aim of this review and meta-analysis was to evaluate the effectiveness of physical scar management on scar tissue. The main results of this analysis show significant overall effects in favor of the physical scar management compared with a control treatment for pain, pigmentation, pliability, pruritus, scar area, and thickness in adults suffering from any type of scar tissue.
However, this study has potential limitations. Although the performed literature search was conducted in three scientific databases, the authors are aware that publication bias might have occurred because no gray literature was screened. Insufficient data reporting might have led to potential over- or underestimation of the true effect as some authors did not show exact values (e.g., mean ± SD) but present the results as graphs only. Most of the included studies used small sample sizes, which limits the translation of these results into practice.
Pain
The main results of this meta-analysis reveal that physical scar management as compared with a control treatment has a significant positive influence on pain ratings (Hedges' g = −0.95 [95% CI: −1.69 to −0.20]). The strongest effects were seen in two studies, 24,25 both using a combination of ESWT and medical or standard treatment. Both ESWT treatments were conducted according to the guidelines of the international society of medical shockwave therapy, with ESWT of 100 impulses per cm2 on the affected location. These strong effects (Hedges' g range = −1.54 to −44.02) were seen in patients suffering from burn scars. The combination of ESWT and medical treatment 25 demonstrated stronger effects compared with the combination of ESWT and standard therapy. 24 The study from Mowafy et al. 25 consisted of medication, physical therapy, and burn rehabilitation massage therapy while the content of the medical treatment of the other study from Cho et al. 24 was not further described. A study showed an extreme effect size for ESWT. 25 Therefore, we performed a sensitivity analysis where the study was excluded. The statistical significance of the overall effect of physical therapy management on pain reduction was maintained but changed from large to moderate (Hedges' g = −0.78 [95% CI: −1.19 to −0.37]).
A moderate-to-strong effect on pain reduction was observed in two studies, where scar tissue was treated with massage therapy for the duration of 30 min. 27,30 Both studies used massage therapy in combination with standard therapy in hypertrophic burn scars 30 or burn scars, 27 respectively. A possible explanation for the stronger effect of massage therapy in the study of Cho et al. 30 (Hedges' g = −1.30) could be the higher treatment frequency of three times versus two times a week, as used in the study of Field et al. 27 (Hedges' g = −0.79). Another possibility is that a mechanotherapy, such as massage, might lead to better results in hypertrophic compared with nonhypertrophic burn scars.
The results of our study indicate that mechanical therapies, such as ESWT and massage therapy, seem to have a positive effect on pain reductions in burn scar. The non-nociceptive mechanical stimuli can reduce pain through the stimulation of nociceptive fibers, which are known to transmit sharp, acute, diffuse, and burning pain sensations. 42 –44 However, these interpretations should be handled with care as both studies using ESWT demonstrated a high risk of bias. 24,25
Different types of light therapy also demonstrated to be effective interventions for pain reductions in the treatment of burn scars. 22,29 Using a CO2 laser led to a significant and moderate pain reducing effect (Hedges' g = −0.65), 29 whereas pulsed high-intensity laser therapy (HILT) showed a significant and large pain reducing effect (Hedges' g = −1.13). 22 Published studies already reported that the higher intensity and the greater depth reached by HILT might be one reason for its effectiveness to relieve pain compared with low-level laser treatments. 45 –47 The reduction of pain levels by HILT is probably based on the inhibition of Aδ- and C-fiber transmission 48 and by enhancing the production and release of endorphins. 22 The results of this analysis might reveal that the general effects of HILT might be strong in the management of burn scars for pain reduction. However, future studies should evaluate this issue for making a valid statement.
Small effects and nonsignificant treatment differences for pain reduction (
Pigmentation
The main results of this analysis reveal that the physical scar management compared with control has a significant positive effect on pigmentation (Hedges' g = −0.72 [95% CI: −1.27 to −0.17]). With respect to the other study results, the strongest effects were seen when applying a silicone gel twice a day on hypertrophic burn scars (Hedges'g = −1.71).
31
A possible explanation might be that silicone applications are believed to positively influence the scar tissue through wound hydration,
49
which is probably one reason that explains the great acceptance of this therapy since the early 1980s.
9
Similarly to silicone gel applications, silicone gel sheets demonstrated to have a large and positive effect (Hedges'g = −1.18) on pigmentation of hypertrophic burn scars.
32
Hydration and occlusion are known positive effects of silicone applications, while occlusion regulates epidermal cytokine and growth factor production in scar tissue.
11,50
A 5-min massage treatment in burn patients showed a small and significant positive effect (Hedges'g = −0.43;
Pliability
The main results of this analysis show a significant positive effect on scar pliability with physical scar management compared with the control treatment (Hedges' g = −1.29 [95% CI: −1.88 to −0.70]). The largest effects were observed in studies, where pulsed dye laser (PDL) therapy was used to treat postsurgical scars. 36,37,39 All studies used a laser wavelength of 585 nm with a pulse duration of 450 μs. However, the study of Alster and Williams 39 used higher fluences per pulse (mean 7.0 J/cm2) compared with 4.0 and 3.5 J/cm2, respectively. 36,37 Interestingly, PDL led to stronger effects on hypertrophic and keloid postsurgical scars, 39 compared with early postsurgical scar treatment. 36,37 The use of an adhesive tape in combination with the PDL treatment demonstrated an additional positive effect of the tissue pliability in postsurgical scar treatment. 37
Silicone gel and silicone gel sheets demonstrated to be effective in the treatment of pliability in hypertrophic burn scars (
Only one study investigated the effects of skin rehabilitation massage therapy on the pliability of burn scars, showing a large and significant effect (Hedges'g = −1.40,
Pruritus
In general, the present analysis shows a significant positive effect of physical scar management compared with control treatments in the management of pruritus (Hedges' g = −0.99 [95% CI: −1.54 to −0.44]). The strongest effect in the reduction of pruritus or itching was seen for hypertrophic burn scars, treated with silicone gel sheets (Hedges'g = −1.49 and −2.08, respectively). 32,34 Furthermore, the moisturizing effect of the silicone gel sheets on the stratum corneum layer also demonstrated to be effective to reduce pruritus in other traumatic skin lesions. 34 A key factor seems to be the regulation of epidermal cytokines and growth factor production, which are evoked from occlusive therapy. 50 Another effective method showing large and significant effects (Hedges'g = 0.86) in the treatment of pruritus was achieved with CO2 laser. 29 Manstein et al. 55 reported that the relief of itching can be explained by the undamaged columns of the skin between the microthermal treatment zones in CO2 laser treatment, resulting in rapid epithelialization. 55
Further treatment that positively influenced pruritus in hypertrophic scar tissue was rehabilitation massage therapy, containing effleurage, friction, and petrissage techniques (
Surface area
Physical scar management showed a large and significant positive effect on the scar surface area (Hedges' g = −1.72 [95% CI: −2.12 to −1.33]). Only two studies investigated the effects of laser therapy on scar surface area in patients suffering from hypertrophic and keloid scars. 39,40 A stronger effect was found for the PDL treatment (Hedges'g = 1.84), 39 in comparison to fractional CO2 laser (Hedges'g = 1.48) 40 in the management of hypertrophic and keloid scars. The study using PDL investigated postsurgical hypertrophic and keloid scars, while the fractional CO2 laser study included hypertrophic and keloid scars from different origins. The different laser therapy specifications and treated scar types make a general recommendation for a specific treatment setting difficult. However, these results demonstrate that laser light therapy is a promising treatment option for reducing scar surface area, probably due to increased tissue repair processes 58 and enhanced anti-inflammatory actions. 59
Scar thickness
Physical scar management has a significantly positive effect on scar thickness management compared with control interventions (Hedges' g = −0.68 [95% CI: −1.27 to −0.09]).
Scar thickening was significantly (
Two studies demonstrated that massage therapy was effective in reducing scar thickening in hypertrophic and burn scars.
30,33
However, also controversial results were found in our analysis. Two included studies, using skin rehabilitation massage in the treatment of hypertrophic and burn scars, showed no effects to reduce scar thickening.
26,28
Besides the interindividual treatment intensities of massage therapy, the treatment frequency of the intervention might have also contributed to the different effects of massage therapy. While the two studies
30,33
showing a positive effect of massage therapy on scar thickening used a treatment frequency of one to three times per week with a treatment duration of 30 min, the noneffective studies showed only treatment durations of 5 min
28
or did not report
26
the exact frequencies and durations. It seems that the combination of massage therapy with standard therapy (including joint mobilizations, silicone gel applications,
Conclusion
In general, this meta-analysis shows that physical scar management has a significant positive effect to influence pain, pigmentation, pliability, pruritus, surface area, and scar thickness compared with control or no treatment.
Treatment modalities, such as ESWT, massage, as well as high-intensity light therapy, seem to be most effective agents in reducing pain in burn scars. Regarding the treatment of pliability and scar thickness, positive effects were seen for the use of PDL in postsurgical scars, while silicone gel and silicone gel sheets demonstrated to be effective in the management of pliability in hypertrophic scars. Our study further revealed strong effects in the reduction of pruritus, using silicone gel sheets in hypertrophic burn scars. Scar thickness was positively affected when hypertrophic and burn scars were treated with massage therapy, while scar surface area was positively influenced by laser therapy modalities (PDL and CO2 laser).
To investigate the most effective physical therapy strategy, further studies are needed, evaluating head-to-head comparisons of different physical scar therapy modalities.
Footnotes
Author Contributions
C.D., E.H., R.S., and R.C. were responsible for acquisition, interpretation, and drafting the article. J.T. and R.C. substantially contributed to the data analysis and critically revised the work for important intellectual content. U.v.D. was included in the article drafting and also critically revised the work. All authors provided final approval of the version to be published and agree to be accountable for all aspects of the work.
Statement of Ethics
As this study was a review of published literature, no ethics approval by a Research Ethics Board was required to conduct our research.
Acknowledgment
The authors like to thank the “Thim van der Laan foundation” for the support.
Author Disclosure Statement
The authors have no conflicts of interest to declare.
Funding Information
No sources of external funding were utilized for this project.