
Abstract
Objective:
The purpose of this study was to determine the feasibility and preliminary effects of a vocal music therapy (VMT) program on chronic pain management.
Design:
A mixed methods intervention design was used in which qualitative data were embedded within a randomized controlled trial.
Setting:
An urban nurse-management health center on the East Coast of the United States.
Subjects:
Participants (N = 43) were predominantly Black (79%) and female (76.7%) with an average pain duration of 10 years.
Intervention:
Participants were randomly allocated to a 12-week VMT program or a waitlist control.
Outcome measures:
We tracked consent rate (percentage of participants enrolled out of total number screened), attrition rate, and treatment adherence. We used PROMIS® (Patient Reported Outcomes Measurement Information System) tools to measure pain interference, pain-related self-efficacy, pain intensity, depression, anxiety, positive effect, and well-being, ability to participate in social activities, and satisfaction with social roles at baseline and week 12. VMT participants also completed the Patient Global Impression of Change Scale. We conducted semistructured interviews to better understand participants' experience of the intervention.
Results:
The consent rate was 56%. The attrition rate was 23%. Large treatment effects (partial eta squared) were obtained for self-efficacy (0.20), depression (0.26), and ability to participate in social activities (0.24). Medium effects were found for pain intensity (0.10), anxiety (0.06), positive effect, and well-being (0.06), and small effects for pain interference (0.03) and satisfaction with social roles (0.03). On average, participants felt moderately better after completion of the VMT program (M = 4.93, standard deviation = 1.98). Qualitative findings suggest that VMT resulted in better self-management of pain, enhanced psychological well-being, and stronger social and spiritual connections.
Conclusions:
Recruitment into the 12-week program was challenging, but quantitative and qualitative findings suggest significant benefits of VMT for chronic pain management.
Introduction
Chronic pain is a significant public health problem amounting to an annual health care expense of approximately half a trillion dollars in the United States alone. 1 In 2016, the Centers for Disease Control and Prevention issued recommendations to move away from opioids and instead use nonpharmacological therapies for the treatment of chronic pain. 2 The use of music for the management of chronic pain is increasingly gaining interest, but more efficacy research is needed to encourage health care providers to recommend its use to patients. 3,4
To date, research on the use of music for pain has focused primarily on listening to prerecorded music for acute pain management with reported treatment benefits for reducing pain intensity and opioid requirements. 5,6 A recent review 3 on the impact of music on chronic pain reported a moderate effect size for pain (standardized mean difference = 0.60), but results were inconsistent across studies (I 2 = 60%). The majority of the studies (11/14) in this review employed listening to prerecorded music; one study used choir singing, and two studies used listening to live music.
The pain-reducing effects of music are often attributed to music's ability to distract and relax. However, chronic pain is a complex phenomenon that affects individuals physically, mentally, socially, and spiritually and its management, therefore, requires interventions that go beyond cognitive distraction. 7 Therefore, we developed a vocal music therapy (VMT) treatment program that addresses biopsychosocial components of chronic pain management. 8
Music therapy is the clinical use of music interventions to help clients optimize their health within a therapeutic relationship with a board-certified music therapist. 9,10 The VMT group sessions use toning (i.e., singing of elongated vowels) and humming, music-guided breathing, group singing, vocal improvisations, verbal processing of emotions and thoughts evoked by the music experiences, as well as psychoeducation about how music can address biopsychosocial factors that impact chronic pain management. We briefly summarize here the intervention's theoretical framework, but readers are referred to Bradt et al. 8 for a more in-depth discussion.
On a bioneurological level, music listening and music making activate brain areas involved with reward, emotion, and arousal such as the nucleus accumbens, amygdala, anterior insula, cingulate cortex, orbitofrontal cortex, and mediodorsal thalamus, through which affective and cognitive modulation of pain can be achieved. 11 –13 On a psychological level, toning and humming are used to help enhance body awareness, promote a positive connection with one's body, and facilitate relaxation. Since people with chronic pain often try to disconnect from their body to “escape” the pain, these are considered important mechanisms in chronic pain management. 14
Singing and active music making also help facilitate emotional expression; emotional expressivity has been shown to improve a sense of well-being and self-reliance in people with chronic pain. 15 Finally, group music making facilitates social inclusion and a sense of belonging. 16,17 Because people with chronic pain often feel isolated, this is an important aspect of the VMT group.
The VMT program was initially tested as an 8-week program. 8 Study findings were promising with large and moderate effect sizes for pain-related self-efficacy and pain interference, respectively, but participants unanimously agreed that a longer program was desirable. Yet, concerns were raised by health care providers at the study site about the feasibility to recruit people with chronic pain to a lengthier program. Therefore, the purpose of this mixed methods feasibility study was to (1) determine the feasibility of a 12-week VMT protocol; (2) provide estimates of effect for core outcomes in chronic pain management; and (3) obtain qualitative data about participant experiences of the VMT program.
Materials and Methods
Study design
We employed a mixed methods intervention design, 18 in which qualitative data (i.e., semistructured interviews) were embedded within a randomized controlled trial. Participants were randomized to the VMT or waitlist control (WLC) treatment arm using a computer-generated list of random numbers. Allocation concealment was achieved through the use of sequentially numbered, opaque, sealed envelopes. Since self-report measures were used for all outcomes, outcome assessment could not be blinded as participants were aware of their treatment allocation. However, the statistician was blinded to group assignments (Fig. 1).
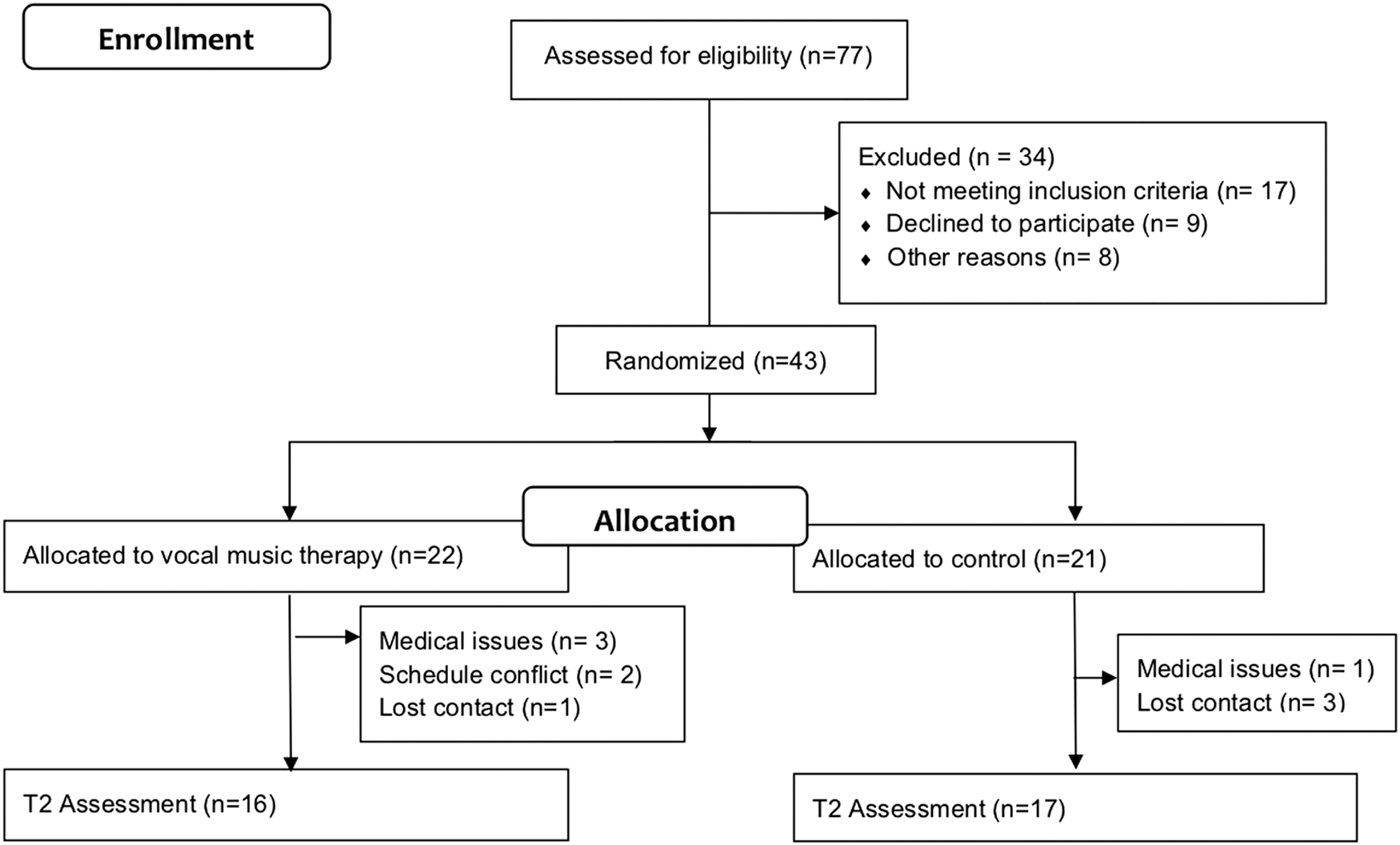
Participant flow chart.
Participants
Participants were recruited from an urban nurse-managed health center that predominantly serves inner-city, low-income African Americans. Eligibility criteria are included in Table 1. Participant demographic and clinical characteristics at baseline are presented in Table 2. The majority of the participants were female (76.7%), were black (79%), were on disability leave (60.5%), and had an average pain duration of 10 years. No significant between-group differences were present at baseline. The study was approved by an Institutional Review Board. Informed consent was obtained from all participants. We recruited participants in three waves. In each wave, participants were randomly assigned to VMT or WLC. WLC participants were invited to participate in the VMT intervention after completion of the outcome measures at the end of the waitlist period.
Study Eligibility Criteria
Impact score items derived from Deyo et al. 35
Sociodemographic and Clinical Characteristics of Study Participants at Baseline
Most commonly reported pain diagnoses.
Having played an instrument or sung in a choir.
SD, standard deviation.
Interventions
Vocal music therapy
Participants in the VMT treatment program received twelve 90-min weekly group therapy sessions (four to six participants). Sessions were led by a board-certified music therapist. The VMT sessions followed a similar structure, but were each focused on a different topic related to music-based pain management (Table 3).
Session Topics
After a brief music-guided deep breathing exercise and verbal check-in, the music therapist led the participants into toning (i.e., singing elongated vowels) and humming experiences. Using the voice in this manner can help facilitate greater body awareness and promote relaxation. The group then talked about somatic sensations experienced during the breathing and toning exercises.
The session then moved into vocal music improvisations. Percussion instruments were often added, resulting in energetic music making. These improvisations provided opportunities for emotional expression. Furthermore, group music making enabled participants to relate to others and share some of their struggles in novel ways. Verbal processing after the improvisation often evolved into additional improvisations focused on the main ideas of the group discussion.
Throughout the sessions, psychoeducation was provided about how music can address biological (e.g., music stimulates dopaminergic activity resulting in improved mood), psychological (e.g., song lyrics can help validate one's feelings), and social (e.g., group music making creates a sense of belonging) factors that play an important role in chronic pain management. Education about why and how music can address pain management can help with transferability of skills and knowledge outside of the session room and equips participants to explain to family and friends how music-based self-management techniques help them with their pain.
Each session ended with singing a song listed by one of the group members during intake. Participants were asked to underline a lyric that was particularly meaningful to them and could possibly be a source of emotional support during the week. The therapist then facilitated a discussion about the meaning of the selected lyrics. 8 The music therapist was trained by J.B. using a treatment manual. Each session was recorded and reviewed by J.B. to ensure treatment fidelity.
The original protocol tested in a previous study consisted of eight 60-min sessions. The 12-week protocol was very similar to the 8-week protocol, except that (1) the longer session length allowed for more time for each music experience and group processing and (2) the longer program length allowed for review sessions to revisit insights and music-based pain management skills gained. The VMT treatment manual will be published in the near future.
Waitlist control
Participants in the WLC group received care as usual at the health center. At the center, chronic pain management typically consists of pharmacological treatment and physical therapy services. Additional complementary services are available, including yoga and fitness classes.
Outcome measures
To determine feasibility, we tracked the following: (1) consent rate (percentage of participants enrolled out of total number screened); (2) attrition rate; and (3) treatment compliance (number of sessions attended). To measure the effects of the intervention, we used the Patient Reported Outcomes Measurement Information System (PROMIS®) 19 short forms (SF) to measure pain interference (SF-6b), pain-related self-efficacy (SF-6), pain intensity (SF-3a), depression (SF-4a), anxiety (SF-4a), positive effect, and well-being (SF), ability to participate in social activities (SF-4a), and satisfaction with social roles and activities (SF-4a). Finally, participants rated their perception of improvement using the Patient Global Impression of Change Scale (PGIC). 20
Measurements were administered at baseline and week 12. After completion of the week 12 measurements, participants (including WLC participants who opted to receive VMT after the WLC period) were invited to participate in a semistructured interview aimed at better understanding their experience of the intervention (Appendix 1). Measurements and interviews were administered by research assistants.
Data analysis
Quantitative data
For each of the outcome variables, we compared the average difference between the VMT and WLC conditions in improvements of the outcome from baseline to week 12. T-scores were used for all PROMIS tools. 21 Raw scores were used for the PGIC. Due to the small sample size, mean difference of improvement from baseline to week 12 between the two conditions and the 95% confidence interval (CI) was reported and used for inference. In addition, we compared the improvement in the outcomes between the two conditions controlling for baseline values. Partial eta squared from ANCOVA was used to quantify the effect size and was interpreted as small (0.01), moderate (0.06), and large (0.14). 22,23 Given the limited sample size, we based our inference on effect sizes. 24,25
Qualitative data
The transcripts of the interviews were imported into MAXQDA 11 26 and analyzed by two coders (M.Y.L. and C.L.) to ensure scientific rigor. We used theoretical thematic analysis procedures as outlined by Braun and Clarke. 27 Coding was based on a semantic approach in which codes are derived from “the explicit meaning of the data and the analyst is not looking for anything beyond what a participant has said” 27 (p. 84). After codes were agreed upon by both coders, they were organized into categories. These were presented to J.B. for input and were compared against the text excerpts associated with the codes for verification. The categories were then organized into broader themes. After final categories and themes were agreed upon, definitions for the categories and themes were developed.
Results
Feasibility
The consent rate was 56%. Of the 43 participants who completed the baseline, 33 completed the postintervention measures. This represents an attrition rate of 23% (Fig. 1). Of the VMT participants, nine participants attended nine or more sessions. Failure to attend a session was mainly due to childcare issues, family emergencies, bad weather, health issues, and traveling.
Preliminary efficacy
Table 3 details the mean change scores (baseline to week 12) and standard deviations (SDs) for each group as well as the effect sizes. There was a large treatment effect of VMT for pain-related self-efficacy, depression, and ability to participate in social activities. The 95% CIs associated with these large effect sizes suggest that these findings were statistically significant. Medium treatment effects were found for pain intensity, anxiety, and positive affect and well-being, and small effect sizes for pain interference and satisfaction with social roles. The 95% CIs of these medium and small effect sizes suggest that these were not statistically significant. On average, PGIC scores (M = 4.93, SD = 1.98) suggest that participants felt moderately better after completion of the VMT program (Table 4).
Change in T-Scores, Mean Difference and Effect Size
change from baseline to week 12.
Ninety-five percent CI intervals that do not include the value zero suggest that the findings are statistically significant.
ηp 2 , partial eta squared based on ANCOVA.
CI, confidence interval; MD, mean difference; SD, standard deviation; VMT, vocal music therapy; WLC, waitlist control.
Qualitative results
A total of 25 participants took part in the semistructured interviews. All participants reported that the VMT sessions were beneficial in helping them manage their pain inside and outside of sessions (Theme 1, Pain Management). One participant remarked, “Every time I play the instruments, it helped me with my pain […] That drum playing changed my pain in some kinda way. ‘Cuz I didn't have it [pain] once I stopped doing the drums.” Participants shared that they used VMT strategies to assist them with their daily activities and chores or for motivation in the morning: “I wasn't feeling too good this morning. I turned on some music and it took my mind off of that feeling. I was able to get dressed on time and I made it here on time.”
Some participants reported using music-based skills as alternatives to their pain medication as the music helped to soothe the pain and refocus their attention. Other participants stated that the music made their pain “go away”: “That day I was having a lot of pain. We started singing and […] it just went away.” One person commented how purposefully music listening helped them with daily activities: “There are certain songs I like, I can get into the rhythm of them. I just focus on the music part, and it gave me a rhythm. As long as I was listening to the music when I was working, I was able to keep going.”
Many participants reported enhanced psychological well-being in response to the VMT experiences and the psychoeducation about how music can address different factors that influence their pain (Theme 2, Improved Psychological Well-being). Participants shared that the VMT program led to (1) better understanding of the contribution of stress and other emotions to their pain, (2) greater awareness of the presence of stress and uncomfortable emotions, and (3) learning new music-based skills to help deal with mental states that exacerbated their pain. One participant shared the following: “I have step-children that I take care of. It can become overwhelming. [Music] helps me just take that moment to woosh (sic) and […] release that negativity so they don't see that and feel that.”
Some participants told us that they are now more intentional with their use of music and that they create playlists for specific purposes. Participants also emphasized that learning to be kinder to oneself, achieving mindfulness, and understanding who they are were important skills gained from the program. One person shared that “keeps you away from that self-blame—because that [self-blame] adds to the pain.” A large number of comments referred to feeling empowered to prioritize one's mental health and physical needs over demands by others and seeking out things in life that bring joy. Participants also appreciated that attending the program was a form of self-care as expressed by one participant: “It made me feel like I'm doing something for myself.”
The third and final theme (Developing Meaningful Connections) relates to music aiding in facilitating deeper connections with one's spirituality and stronger bonds with others. One participant commented, “The spiritual aspect of music and the emotional feelings that I got from just beating on the drum, or playing the tambourine, or that ocean drum!”
Many participants reminisced fondly about the bonds among the group members that were created through the VMT program. One participant said, “It was wonderful because the group started out with everybody was in their little shell. […] And on the recording [excerpts from sessions] that we heard after the group, we just heard our story, and like how amazing how everybody developed. And we became united. We became a family.” Another participant appreciated the accepting and nonjudgmental environment the group provided, “With friends or family or romantic partners or even doctors, sometimes struggling so much to explain intermittent, invisible chronic pain to the point of disability […] Hearing and being understood and sharing just felt really comfortable and in a way that I had not experienced.” Participants shared that these bonds continued outside of the sessions (Table 5).
Qualitative Findings
PTSD, posttraumatic stress disorder.
Integration of quantitative and qualitative findings
Participants' reports of using music-based pain management strategies at home aligned with the large treatment effect for self-efficacy as the self-efficacy questionnaire measured participants' beliefs that they are able to control their pain and use methods other than medication for pain relief. Given this finding, the small improvement in pain interference was surprising, especially since the 8-week VMT program resulted in a moderate effect size for this outcome. 8 As for psychosocial outcomes, participants shared that they had learned to use music to address emotions that worsen their pain and that the VMT program had helped to develop stronger connections with others. This was supported by the large treatment effects for depression and participation in social activities (i.e., ability to do things with others).
The lack of improvement in satisfaction with social roles and activities (i.e., being able to do things for family and friends) is explained by the qualitative findings: participants stated that the VMT program had empowered them to set boundaries with friends and family and prioritize self-care, thus suggesting that “being able to do things for others” may not have been a desirable outcome for study participants. This makes sense given that this study included many low-income residents with complex family situations and high caregiver burden. Participants shared in the interviews that self-care involves being selective with their effort in taking care of other people.
Discussion
The purpose of this study was to determine the feasibility and preliminary effects of a 12-week VMT program on chronic pain management. Despite suggestions from participants in a prior study of an 8-week version of the VMT protocol to increase program length to 12 weeks, 8 the consent rate for this study (56%) was much lower than that obtained in the 8-week VMT study (77%). The fact that the attrition rate in this study (23%) was lower compared with the 8-week study (27%) suggests that the length of program negatively impacted enrollment rates, but not participants' ability to complete the program.
Even though a higher percentage of people remained in the study in the 12-week program, treatment adherence (i.e., number of sessions attended) was better in the 8-week program (86% of the participants attended seven to eight sessions). Yet, the interview data suggest that the VMT program was meaningful, beneficial, and highly enjoyable for participants in this study. Taken together, these findings suggest that people may be more hesitant to commit to a study or treatment program of longer duration and that regular, weekly attendance in a 3-month program may be more challenging due to accumulation of life- or health-related events in a longer period of time. Indeed, childcare issues, family emergencies, and health issues were frequently given as reasons for missing a session.
VMT had a large treatment effect on self-efficacy. Self-efficacy is considered a core outcome in chronic pain management as greater levels of self-efficacy have been associated with greater physical functioning, participation in physical activities, and performance satisfaction; enhanced health and work status; and decreased pain intensity in people with chronic pain. 28 Large treatment effects were also found for depression and ability to participate in social activities. This was supported by the interview data that indicate participants derived a lot of joy and support from group music-making with their peers. The experience of having chronic pain may negatively impact relationships, thereby limiting social resources for pain management. Therefore, being connected to a community or support system has been identified as an important need of people with chronic pain. 29,30
The treatment effects between the 8- and 12-week program were very similar, except for pain interference (Table 6). It is unclear at this time if the difference in pain interference is a function of treatment length or selection of outcome measure, as a different outcome measure was used in the 12-week study.
Comparison of Treatment Effects Between 8- and 12-Week Vocal Music Therapy Program
ηp 2 , partial eta squared based on ANCOVA.
VMT, vocal music therapy.
The qualitative findings, namely enhanced pain management, improved psychological well-being, and development of meaningful connections, align with the biopsychosocial framework that underlies the treatment protocol. Importantly, participants reported how active engagement in VMT experiences facilitated these benefits inside and outside of the session. Furthermore, creative engagement in music-making helps people tap into their inner playfulness and creative selves. These are important resources that, when strengthened, may facilitate resilience in the face of life's challenges. 31
Creative participation also empowers people to actively take part in their pain management, rather than feeling victimized by pain and relying on passive pain management strategies such as taking medicine. 8 Research increasingly finds that active engagement in pain management enhances self-efficacy, which can lead to improved health outcomes. 32,33 Participants reported that learning about how their stress and emotions are intricately linked to their physical pain, and being able to use music-based strategies outside of the sessions to holistically address these mind-body connections was an important treatment benefit. Self-management strategies that can be easily learned and used anywhere can lessen dependency on health care systems and reduce health care cost. 34
This study has several limitations. The study was limited to one urban setting that serves mostly low-income African Americans. Furthermore, this study did not use an active control condition. Finally, all outcome measures were self-report and subject to bias. Based on the promising preliminary treatment effects obtained in this as well as the prior study, future research on the VMT protocol should expand to statistically powered multisite trials that use active control conditions. Given the qualitative findings, future studies should consider including measures of spirituality, self-care, and empowerment. In addition, accurate measurement of pain interference may need to be explored further, given that participants spontaneously reported in the interviews improved ability to do chores and increased physical activity, yet, quantitatively, only a small effect size was found.
Conclusions
Both quantitative and qualitative data suggest important benefits of VMT for chronic pain management, particularly in the areas of self-efficacy, depression, and ability to participate in social activities. However, feasibility data indicate that recruitment into a 12-week VMT program for chronic pain may be challenging. Based on the feasibility comparison of the 8-week versus 12-week VMT protocol studies and the fact that both programs resulted in similar treatment estimates for core outcomes in chronic pain management, future research efforts should focus on efficacy and effectiveness testing of the 8-week version of the VMT program.
Footnotes
Acknowledgments
We like to express heartfelt thanks to all the people who participated in this study. We also would like to thank the staff and providers at Stephen and Sandra Sheller 11th Street Family Health Services for their enthusiasm for this study and their help with referrals. Special gratitude is extended to Lindsay Edwards, Director of Creative Arts Therapies, for her unwavering support for this research.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported through a cooperative agreement with the National Endowment for the Arts Research Labs program.