
Abstract
Background:
Complementary and alternative medicine (CAM) is subject to heated debates and prejudices. Studies show that CAM is widely used by psychiatric patients, usually without the guidance of a therapist and without the use of a solid working method, leading to potential health risks.
Aim:
The purpose of this study is to facilitate the judicious use of CAM alongside conventional psychiatry in an outpatient psychiatric clinic.
Methods:
A search was made through scientific and legal articles and discussion in focus groups.
Results:
In the Centre for Integrative Psychiatry (CIP) of Lentis in the Netherlands, some carefully selected CAM are offered under strict conditions, alongside conventional treatments. Because of the controversy and the potential health risks, Lentis designed a protocol that is presented.
Conclusions:
The CIP hopes, by using this protocol, to better serve and respect the individual needs and preferences of the diversity of psychiatric patients in our Dutch multicultural society, and better protect them from harm.
Introduction
Supporters of CAM claim that conventional treatments have too many side-effects, lack effectiveness and room for patients' wishes and needs. On the other hand, opponents state that CAM is quackery and that the effects are based on placebo and “ridiculous principles.” 1 This reaction reminds us of earlier resistance to change in medicine; for instance, in 1911 Herrick was almost laughed out of medicine for stating that atherosclerosis causes myocardial infarction. 2
Previous and current bias against new developments is undesirable because both patients and doctors are uncertain about safety and effectiveness of CAM. This is all the more important because about half of the population in a variety of Western countries 3 and almost half of Dutch psychiatric outpatients use CAM annually. 4
A majority of patients get information on CAM via the Internet, friends, or family. The quality of this information varies greatly, leading to potentially harmful and dangerous situations. 5
In the Netherlands, many doctors do not inform their patients about CAM and they certainly avoid prescribing or referring to CAM. Recently the Dutch Minister of Health has announced more severe punishment for practitioners who harm their patients either by applying unsafe therapies or by delaying the start of conventional treatment. 6 Therefore, in the Netherlands patients and doctors are informed about what cannot be done concerning CAM, while it remains unclear what could or should be done. Despite calls from the World Health Organization (WHO) 7 and the European parliament, 8 until now the Dutch government did not formulate a policy on this matter.
In an effort to fill this gap and inspired by the North American consortium of 44 academic health centers for integrative medicine (CAHCIM) 9 , Lentis (a community mental health facility in the North of the Netherlands) founded a Centre for Integrative Psychiatry (CIP) in 2006. It consists of an outpatient clinic, a research department, an educational department, and organizes an annual conference (with approximately 1000 attendees). 10 Its main purpose is to provide safe and effective integrative mental health care.
What Is Integrative Psychiatry?
Integrative psychiatry is based on the principles of “integrative medicine”: reaffirming the importance of the relationship between practitioner and patient; focusing on the whole person; using all therapeutic approaches (conventional and CAM) based on the principles of evidence-based medicine (EBM); and achieving optimal health and healing.
The debate in the Netherlands focuses mainly on the principle of EBM (i.e., the use of CAM within conventional treatment centers, and the correct definition of EBM). In this regard, it is noteworthy that Sackett et al. 11 defined EBM as (1) the best available evidence for effective and safe treatment options, (2) the preferences and needs of the patient, and (3) the clinical expertise of the professional. These three together should be decisive in making treatment choices. This definition is in contrast with the present-day more reductionist explanation of EBM in which the first and third principles are emphasized without paying much attention to the patient's preference. 12 The original definition therefore accommodates therapies that still lack (sufficient) evidence-based proof. It is also important to realize that according to some researchers, only about one third of culturally and professionally accepted interventions in Western medicine are proven effective by randomized controlled trials. 13,14
Prejudices
Some reasons why opponents feel doctors should not use CAM seem to be based on prejudices. Table 1 compares the most common prejudices against CAM with information from scientific studies.
Van de Creek L, Rogers E, Lester J. Use of alternative therapies among breast cancer outpatients compared with the general population. Altern Ther Health Med 1999;5:71–76.
Astin JA. Why patients use alternative medicine. JAMA 1998;279:1548–1553.
Eisenberg DM, Davis RB, Ettner SL. Trends in alternative medicine use in the United States, 1990–1997. JAMA 1998;280:1569–1575.
Furnham A. Why do people choose and use complementary therapies? In: Ernst E, ed. Complementary Medicine: An Objective Appraisal. Oxford: Butterworth Heinemann, 1996.
Ernst E, ed. The Desktop Guide to Complementary and Alternative Medicine: An Evidence Based Approach. Edinburgh: Mosby, Hartcourt Publishers Limited, 2006.
Lake JH, Spiegel D, ed. Complementary and Alternative Treatments in Mental Health Care. Washington, DC, London: American Psychiatric Publishing, 2006.
Wilson K, Mills EJ. Introducing evidence-based complementary and alternative medicine: Answering the challenge. J Complement Altern Med 2002;8:103–105.
EBM, evidence-based medicine; CAHCIM, academic health centers for integrative medicine; WHO, World Health Organization; EP, European Parliament.
Similarly, those in favor of CAM also seem to have prejudices. Those are mentioned in Table 2. We therefore argue that CAM needs serious attention, both within conventional treatment centers and in the alternative field (Table 2).
Ernst E. Serious psychiatric and neurological adverse effects of herbal medicines: A systematic review. Acta Psychiatr Scand 2003;108:83–91.
Walach H, Falkenberg T, Fonnobo F, et al. Circular instead of hierarchical: Methodological principles for the evaluation of complex interventions. BMC Med Res Methodol 2006;6:29.
The CAM Protocol
One of the primary tasks of our center was to formulate a scientific model based on the requirements that it would (1) answer patients' needs and wishes; (2) respect their freedom of choice; (3) would offer Western medicine and CAM that are safe and effective; (4) would protect against quackery and abuse; (5) should be based on Dutch law, the jurisprudence of the Medical Disciplinary Tribunal, and the rules of the Dutch Association of Medical Practitioners; and (6) be based on scientific evidence.
The authors reviewed documents, the scientific literature, and collected information with the help of focus groups. 15 This resulted in the CAM protocol. 16 In this protocol, we distinguish (between) complementary and alternative medicine. The first is defined as “approaches based on mainstream biomedical theory and supported by research evidence but not part of mainstream practice because of social, political or ideological reasons.” Examples are St. John's wort and massage. Alternative medicine is defined as “approaches that are based on concepts that are outside mainstream Western medicine.” Examples include homeopathy and healing. 17 Based on an analysis of the results, we produced the algorithm shown in Figure 1.
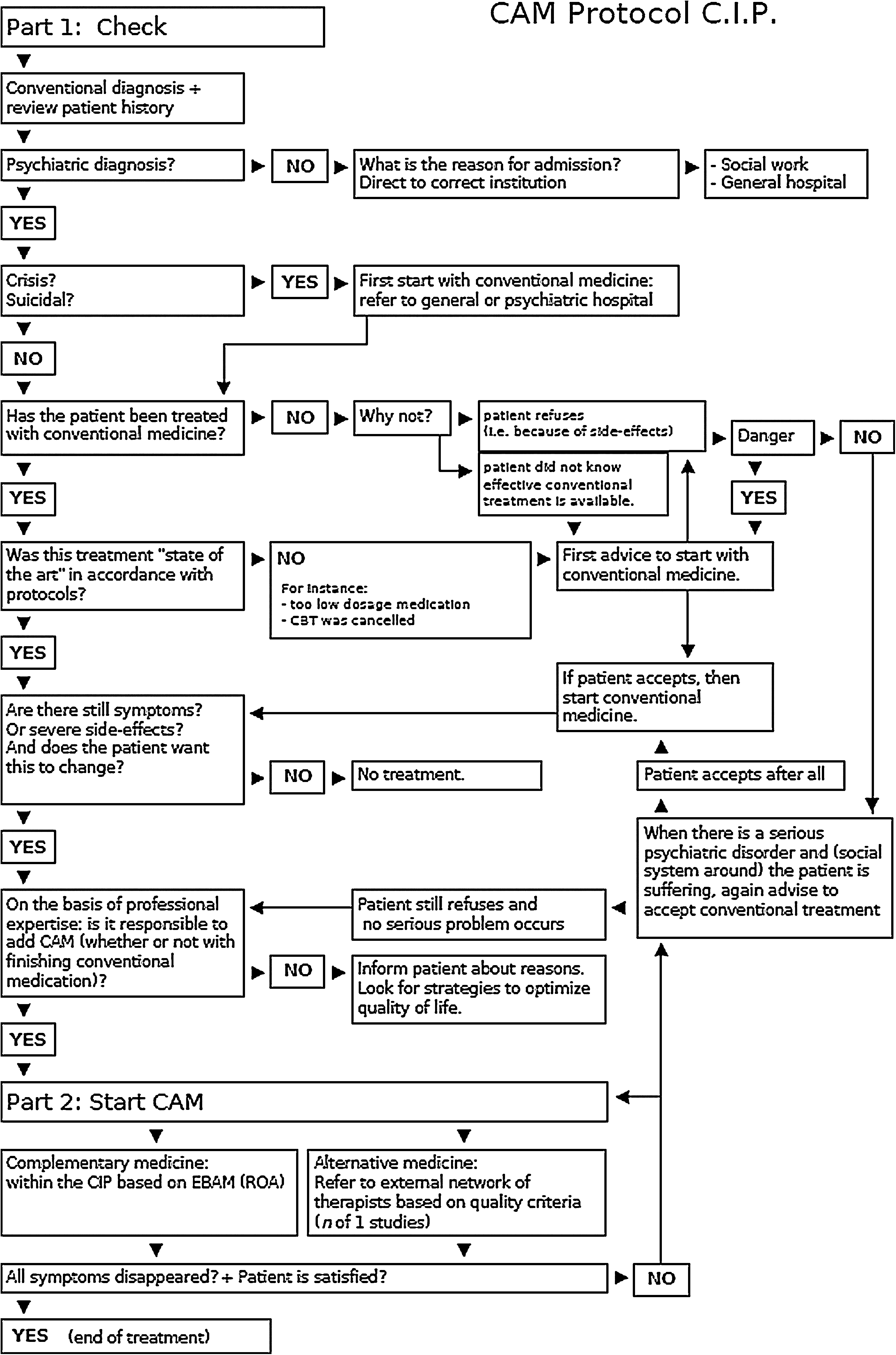
Complementary and alternative medicine (CAM) protocol for the Center for Integrative Psychiatry (CIP). CBT, cognitive behavioral therapy; EBAM, evidence-based alternative medicine; ROA, routine outcome assessment.
This is the working method of the CIP. The first step of the algorithm clarifies that CAM can only be used after an extensive and precise stepwise process. CAM can only be started if conventional treatments have been applied before or at least advised as suggested by guidelines and protocols. In addition, CAM is considered if there is no danger when a patient refused treatment (for instance: a patient with mania or psychosis with severe symptoms will be strongly advised first to accept conventional medication even when asking for CAM).
After deciding to start CAM, the second step is based on the principles of EBM (i.e., alternative treatments with a lower level of evidence can be provided on a patient's request when there is no contraindication). However, these treatments will not be offered within the CIP. Patients will be referred to an external network that provides these treatments in conjunction with proven treatments provided by CIP and not instead of them. In addition, there are the following required conditions: • The therapists are members of a (para)professional organization with a formal procedure for complaints and malpractice. • The therapists base their treatments and way of working on the professional guidelines of the organization. • The therapists conform themselves to legal demands concerning patient files. • The clinic or office where patients are being treated meet privacy and hygiene demands, as common in conventional medicine. • The therapists have malpractice insurance. • There has to be at least monthly contact between the CIP and the alternative practitioner. • After finishing the alternative treatment, there will be at least one contact with the CIP to evaluate. • The alternative therapists agree to be included in scientific evaluation by routine outcome measurement (ROM) of the effect of the treatments and agrees with publication, regardless the results.
Center for Integrative Psychiatry
In the CIP of Lentis, only conventional and complementary medicines that have been proven effective and safe are being practiced. That means that they have to be based on (reviews of ) several well-designed scientific studies. Examples are St. John's wort for depression,
18
valerian for insomnia,
19
relaxation for anxiety,
20
mindfulness-based stress reduction
21,22
and mindfulness-based cognitive therapy for depression,
23
massage for stress, anxiety, and depression,
24
exercise for depression, anxiety, and sleep disorders,
25
heart rate variability training for anxiety and stress-related and depressive symptoms,
26,27
single vitamins as a supplement to medication for depression (such as folic acid),
28
food supplements like such as S-adenosyl-
These treatments, integrated with conventional psychiatry, have been offered for 3 years to psychiatric outpatients in the CIP.
Alternative medicine such as homeopathy, Reiki, or healing are not being offered. However, patients can be referred to these treatments under strict conditions, which are explained above. All treatments are evaluated by ROM. In addition, we study the outcome of innovative treatments with individual outcome measurements (IOM) such as “N of 1 design,” “single-subject experimental design,” and “time serial analysis.” ROM consists of six questionnaires: psychopathology, quality of life, resiliency, costs, satisfaction, and one self-report personalized outcome indicator, chosen by the patient. Patients fill out these forms before treatment starts, every half year, at the end of treatment, and half a year after their discharge. Patients with IOM fill out diaries concerning items that are most relevant to their treatment and symptoms to assess subjective improvement on core symptoms and complaints.
Conclusions
Because of the increasing demand of patients for alternative medicine and integrative treatments and because of social, political, scientific, and ethical reasons, and inspired by the CAHCIM, Lentis has founded a CIP. Here it offers selected complementary treatments alongside conventional ones under strict conditions. By doing so, the CIP responds to a call from the WHO and European Parliament, even though the Dutch government still has not made a policy on this subject. Because of the controversy surrounding CAM, because of the lack of clear information, and because we need not only an open attitude but also a critical one, the CIP has formulated the CAM protocol. It believes that in this way CAM can be offered in a safe and effective way within conventional treatment centers. The CIP hopes in this way to better serve and respect the individual needs and preferences of the diversity of patients who need mental health care in our Dutch multicultural society. It believes the protocol also protects against quackery, abuse, and false hope.