
Abstract
Oral treprostinil was recently labeled for treatment of pulmonary arterial hypertension. Similar to the period immediately after parenteral treprostinil was approved, there is a significant knowledge gap for practicing physicians who might prescribe oral treprostinil. Despite its oral route of delivery, use of the drug is challenging because of the requirement for careful titration and management of drug-related adverse effects. We aimed to create a consensus document combining available evidence with expert opinion to provide guidance for use of oral treprostinil. Following a methodology commonly used in business and social sciences (the ‘Delphi Process’), two investigators from the oral treprostinil (Freedom) studies created a series of statements based on available evidence and the package insert. The set of ‘best practice’ statements was circulated to nine other Freedom trial investigators. Their comments were incorporated into the document as new line items for further vote and comment. The subsequent document was put to vote line by line (scale of −5 to +5) and a final statement was drafted. Consensus recommendations include initial therapy with 0.125 mg for treatment na patients, three times daily dosing, aggressive use of antidiarrheal medication, and a strong preference for use of the drug in combination with other approved PAH therapies. This process was particularly valuable in providing guidance for the management of adverse events (where essentially no data is available). The Delphi process was useful to codify investigator experience and subsequently develop investigator consensus about practical issues for physicians who may wish to prescribe oral treprostinil.
Best practices in the use of a specific drug are often perfected over time. This is particularly true in rare diseases as such as pulmonary arterial hypertension (PAH) and even more so for drugs that require individual titration. Learning that accrues over time is, by definition, not reflected in the initial pivotal clinical trials for drug registration. Open label extension trials and early post-marketing experience often add substantially to our overall knowledge of the drug and thus lead to best practices that are not reflected in the official prescribing information. Subcutaneous treprostinil is an example of this limitation: the full prescribing information still reflects the dosing from the initial trial reported by Simonneau in 2002, 1 while practical suggestions published recently offer very different ideas for the use of the drug.2,3
In addition, adverse effects of trial medications are meticulously collected to assure safety for those exposed to an investigational drug. Researchers generally manage the side effects without direction from the clinical trial organizers. Their approach to adverse effect management is not systematically collected and therefore not reported and not available to less experienced clinicians that might consider using the drug.
Oral treprostinil (Orenitram™) was FDA approved in December 2013 for use as oral monotherapy. The initial trials commenced in 2006 and thus the accumulated investigator experience is much richer than disclosed in the package insert. The package insert includes little or no guidance on the management of common and important adverse effects, and even the most basic of prescribing information (twice or three times daily) is left to the prescriber with little direction. This leaves physicians who manage pulmonary hypertension (PH) but did not participate in the oral treprostinil (Freedom) studies with relatively little guidance in the practical use of the drug.
The Delphi methodology dates back to the 1950s and was developed to create consensus in social science topics.4–10 The methodology is particularly relevant when there is real knowledge available on a particular topic, but definitive experiments to prove the point are lacking. The Delphi approach involves digestion of the existing data and practices by subject matter experts, followed by successive refinement and consensus building among a larger group of experts. It seems particularly well-suited to a rare disease like PAH where significant advances in the use of a medication occur well after drug approval, often in trials not rigorous enough to influence changes to the labeled prescribing information. The ongoing, long-term Freedom-EV study will yield important information about three times daily dosing of oral treprostinil, effective doses, and appropriate titration strategies. However, until that data are available, we believe that the current approach has provided useful information which reflects the collective prescription and management pattern of experts with considerable experience using oral treprostinil in research studies.
Neither the manufacturer, nor any paid representatives of the manufacturer, participated directly or indirectly in the conception, design, implementation, analysis, or reporting of this project.
Methods
We used a modified Delphi methodology to reach a consensus statement. Delphi methodology has been previously reviewed.10–13 The basic method as described by Delbecq et al. is as follows:
14
Develop initial questionnaire and distribute it to the panel. Panelists independently generate their ideas in answer to the questionnaire and return it. The moderator summarizes the responses to the first questionnaire and develops a feedback report along with the second set of questionnaires for the panelists. Having received the feedback report, panelists independently evaluate earlier responses and independently vote on the second questionnaire. The moderator develops a final summary and feedback report to the group and decision-makers.
Following Delphi guidelines, the experts were encouraged to include comment and literature as they saw fit, for the benefit of the group. The literature and the aggregate responses were included anonymously. Comments were encouraged about the validity, specificity, and content of the items under consideration, and incorporated verbatim and anonymously in the tabulated statement. Anonymity is deemed essential in Delphi methodology to prevent bias by influential clinicians and to reduce the pressure towards conformity.
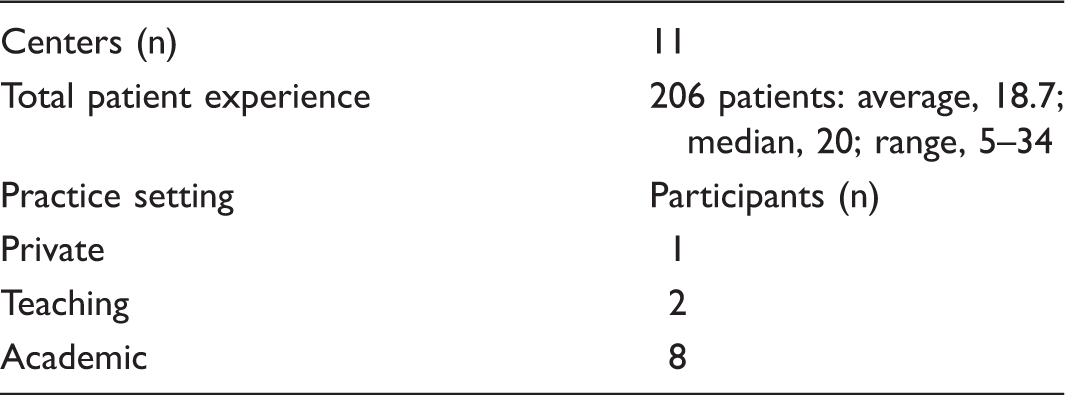
Characteristics of participants.
Dosing recommendations.

Statements based on available evidence.
SD, standard deviation.
Adverse event management.

SD, standard deviation.
Results
The final product of our modified Delphi process is presented as Table 2 for dosing recommendations and Table 3 for adverse events management. Those recommendations which are grounded in the package insert or available literature (present in the initial list) are identified with asterisks. The consensus statements (see the “Methods” section) are highlighted. There were other statements with favorable recommendations but some significant negative votes resulted in a large standard deviation which precluded a consensus recommendation.
The group strongly recommended three times a day (t.i.d.) dosing versus twice a day (b.i.d.) dosing (Table 2). As for the starting dose, both 0.125 and 0.25 mg were judged acceptable (but not 0.5 mg) with a suggestion to use 0.125 mg in smaller patients and in those with low blood pressure or low tolerance to side effects. Slow titration was preferred overall with 0.125 dose increments. Even though the 0.25 mg dose had a score of 2.54, there were a few strong votes against increasing the dose by 0.25 mg (standard deviation > 2.5). Investigators preferred that patients space the medication throughout the day with doses 6–8 h apart; they strongly agreed that doses be at least 5 h apart. Increasing just one of the doses (the evening dose) before increasing the other doses almost achieved “consensus.”
Investigators agreed that the doses achieved in the placebo-controlled trials were insufficient and demonstrated remarkable agreement on goal setting. The group set target doses of 4 mg t.i.d. at three months, 6 mg t.i.d. at 6 months, and 8 mg t.i.d. at one year. The group agreed that annual reassessments of dosing and efficacy were necessary at a minimum, and that the maximum dose would be dictated by side effects. Interruptions must be avoided, and if multiple doses ( > 2) are missed, investigators recommend resuming at a lower dose with rapid re-titration. In general, the group recommended that the drug be used in combination with other PAH-specific therapies. The group agreed that the drug should not be used as first-line therapy. The original combination studies were launched when only sildenafil and bosentan were available (2006); the package insert specifically states that dose adjustments for sildenafil and bosentan are not necessary, and the investigators agreed with that statement. Investigators strongly agree that headache is more common for patients when oral treprostinil is added to a background phosphodiesterase-5 inhibitor (PDE5-I).
The package insert indicates that oral treprostinil may be useful for patients who are already using parenteral or inhaled treprostinil and now includes data from the recently published parenteral to oral transition study delineating a methodology for transition. 24 Our Delphi process concluded that only carefully selected parenteral treprostinil patients with a durable response to therapy and excellent hemodynamics were reasonable candidates for transition to oral treprostinil. The group strongly recommended a 2–5-day transition in hospital and also were near unanimous that these participants should be using at least one additional oral PAH-specific therapy to insure disease stability during the transition. There was less consensus about the method for transitioning from inhaled treprostinil as there are currently fewer data.
Patients with end-stage renal disease on hemodialysis (and without PAH) have been formally studied and the package insert indicates that no dose adjustments are necessary. Our experts agreed with that but suggested that dialysis patients may require a slower up-titration with attention to hypotension at hemodialysis. The package insert identifies drug–drug interactions with HIV medications but only one of our experts commented on this as a problem in experience.
With regard to side effect management (Table 3), the investigators reached consensus about Loperamide (Imodium™) and Diphenoxylate/Atropine (Lomotil™) to ameliorate diarrhea. To alleviate nausea, investigators strongly recommended taking the drug with food as well as using Ondansetron (Zofran™). It is worth noting that specific food choices or calorie counts are not mandatory for t.i.d. dosing whereas specific calorie counts and fat content were protocol-required for b.i.d. dosing in the trials.
Promethazine was rated as a second-line nausea agent. Acetaminophen was preferred for headache, tramadol (Ultram™) for more significant pain, and opiates only in the most severe cases. Amitriptyline and non-steroidal anti-inflammatory agents (NSAIDs) were not recommended; however, there was a great deal of disagreement here and at least some investigators thought that these were helpful.
Reassurance was suggested for jaw pain and flushing. In response to dizziness or overt hypotension, the investigators strongly recommended that physicians reduce or eliminate other medications for systemic hypertension. They also suggested close monitoring of blood pressure and oral treprostinil dose reduction. Investigators strongly recommended gabapentin for pain in the extremities and also suggested screening for iron deficiency to address restless legs as a possible contributor.
Discussion
The purpose of this paper was to give practical guidance about using oral treprostinil with specific regard to dosing and management of adverse effects. We used a well-established method, the Delphi process, to build consensus among a group of US investigators who had substantial oral treprostinil experience. The consensus statements in Tables 2 and 3 with the final scores were generated with an initial draft and two iterations (voting at second iteration). We highlighted as “consensus” any statement that achieved an average score above 2.5 as long as the standard deviation was less than 2.5.
The strongest consensus was built around three times daily dosing with a strong emphasis on dividing the doses evenly over waking hours. In the experience of this group, the drug is best tolerated when dosed every 7–8 h. B.i.d. dosing causes wide swings in blood treprostinil levels with a large peak:trough ratio and a prolonged time at the end of the dosing period when blood levels are quite low. 17 Data presented in abstract form confirm that trough blood levels were higher in a group of 13 participants who switched from b.i.d. to t.i.d. dosing; adverse events in this group were less intense during the t.i.d data collection phase suggesting that the hypothesis of peak:trough levels driving adverse events is reasonable. 25 Similarly, in the recent report of participants transitioning from parenteral to oral treprestonil, participants using the t.i.d. drug had a lower peak:trough ratio and achieved higher daily doses of oral treprostinil with apparently better drug tolerance as compared to those using the b.i.d. drug. 24
The group generally favored a starting dose of 0.125 mg and titration by 0.125 mg. Some investigators have found that it is helpful to increase the evening dose first (to allow overnight acclimation). Others have found that spacing the titration out even further is advantageous: a “stair step” process in which the evening dose is increased on one day and then the afternoon dose the next titration day and finally the morning dose (possibly a Monday–Wednesday–Friday strategy for simplicity). Slower strategies may be especially helpful for smaller patients or those who get “stuck” at a dose because of headache, nausea, or diarrhea with dose increases. No consensus was reached as to the number days or frequency of up-titration. The variety of opinions are reflected in the statements that did not reach consensus in Table 2, including the package insert suggestion of not up-titrating more than twice a week. More research is necessary to clarify optimal titration strategies, as reflected in the lack of consensus around dosing strategies.
There is little literature available as to the place of oral treprostinil in the pantheon of medications now available to use for PAH. Aside from the preference to not use the drug as a first-line agent, the process did not result in statements attempting to define the kind of patient that would benefit from oral treprostinil. There is now recently published evidence supporting the group consensus around combination/second-line therapy. 26
A key goal of our effort was to outline expert opinions on the management of adverse effects because the primary publications and package insert do not generally make statements about management approaches. Table 3 makes very specific suggestions and shows the degree to which the group agreed on any given strategy. The group strongly recommended aggressive treatment of nausea with Ondansetron, diarrhea with Loperamide, and headache with analgesics. The list generated by the Delphi process is a distillation of what the experts are practically using to address adverse events. The specific adverse events may have many other remedies explored in other disease states. We have included in the references reviews of current general management of diarrhea,27–29 nausea,30–32 and headache33–36 for readers' benefit.
There are important limitations to this methodology. A clear advantage was the electronic nature of data collection and dissemination, which minimizes financial constraints and need for support. The anonymous nature promotes the free sharing of opinions and ideas, preventing a dominant leader from dismissing less popular concepts. In contrast, a face-to-face process allows individuals to explain and defend ideas, which might improve the quality of some recommendations. Similarly, the process gives equal voice and weight to the most and least experienced; this has the advantage that a variety of opinions are expressed and the disadvantage that very knowledgeable opinions might be “out-voted” in the process. For example, the need for dose adjustment among those taking certain HIV medicines is near certain (and is described in the label), but the panel did not recognize this fact.
An additional limitation has to do with the selection of experts. We explicitly limited our work team to those in the United States with substantial experience in the Freedom studies. The number of investigators was also limited to make a manageable process. Table 1 demonstrates that this group had a substantial composite research subject experience, but investigators outside the US are not represented here.
In conclusion, we used the Delphi methodology to assist practicing physicians in the use of a newly approved drug. The information in Tables 2 and 3 are intended as a practical supplement to the data reported in the primary trials and the information in the package insert.
Footnotes
Acknowledgments
FFR would like to thank the Hamilton Family Fund for support of scholarly activities at the Cleveland Clinic Florida.
Conflict of interest
VT, FFR, ZS, RPA, and JF serve or served in the past on the speaker s bureau of United Therapeutics (makers of Oral Treprostinil). VT, FFR, ZS, RPA, MMC, JME, and JF served as United Therapeutics consultants. RJW serves as a consultant to UT but all compensation goes to the University of Rochester.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.