
Abstract
In New Zealand, defendants found not guilty by reason of insanity may be disposed of by the court as special patients, whereupon they are treated, rehabilitated and monitored by Forensic Mental Health services. Special patients have a high degree of administrative structure overseeing their care, and may not be discharged or reclassified without ministerial assent. This reflects the high degree of public concern over the risk that these patients present to the community [1].
Forensic Mental Health services are dually tasked with both facilitating the patient's recovery and protecting the public [2]. Discharge from hospital is an important rehabilitative step, carrying the implication that any residual risk can be safely managed in the community.
Increasingly in mental health there is a need to adopt an outcome focus. Despite its limitations, reoffending is one primary outcome measure of interest for forensic treatment programs. However, little is known about outcomes in this population. This may contribute to the increasing public fears of violence perpetrated by the mentally ill, stigmatizing those suffering from mental illnesses, and may promote philosophies of institutional care in Forensic Mental Health services in an era where the advantages of deinstitutionalization have been widely embraced by the profession of psychiatry, and government policy.
Lengthy periods of inpatient care are common for insanity acquittees (e.g. [3]), a situation that is likely to continue until forensic treatment programs can demonstrate effective outcomes, including an understanding of reoffending rates in this population. In systems with political accountability, changing public attitudes will be a necessary consideration of any shift in treatment focus.
This study reports on outcomes, including duration of inpatient treatment, duration of special patient committal, and rates of reconviction and readmission following discharge from hospital for a national population of special patients following acquittal by reason of insanity over a period of two decades. We also explore the relationship between demographic, clinical and criminological variables and outcome measures.
Method
All 145 insanity acquittees disposed of as special patients after 1976, and recorded on the Ministry of Health Special Patient database, who had subsequently been discharged into the community were initially included in this study. Discharge was defined as either being reclassified (usually resulting in discharge from hospital), or being granted extended community leave, both of which require ministerial approval.
Data sources were secondary databases in a variety of government agencies:
The Ministry of Health Special Patient database, which records demographic and clinical details of all special patients (complete record from 1976);
The Justice Data Warehouse, maintained by the Ministry of Justice, which contains historical criminal and traffic conviction data (some missing data before 1980 for those who did not subsequently reoffend);
The New Zealand Health Information Service database, which records hospital admissions and discharges with basic demographic and clinical information (patchy records 1980–1988, complete from 1988).
Any patient not matching with the Justice Data Warehouse was excluded (n = 10) leaving a study population of 135. The 10 excluded patients are unlikely to have a subsequent criminal record because of the completeness of the database. Excluding them from further analysis is therefore likely to have overestimated the real reconviction rate.
The index offence, demographic, clinical diagnosis and criminal offending data were extracted from the Special Patient database. Readmission data were gained by cross-referencing with the New Zealand Health Information Service database, and criminal record was gained by matching with the Justice Data Warehouse.
All follow-up data until July 2004 were considered, giving a maximum follow-up period of 27.5 years. Where an individual's death was recorded, the follow-up period finished at the date of death. Some deaths following reclassification from special patient status but before the census date were probably missed, and some patients would have emigrated overseas, but for all others the Justice Data Warehouse is a reliable source of conviction data over the follow-up period.
Data were entered into SPSS version 13 (SPSS Inc., Chicago, IL, US) [4]. The inpatient duration and duration of special patient orders were compared between clinical, demographic and criminogenic groups using the Kruskal–Wallis non-parametric anova. The time to reconvictions were summarized using Kaplan–Meier survival curves and compared between groups using log-rank tests.
The National Ethics Committee granted ethical approval for this multicentre study. A contract between the Ministry of Justice and the Ministry of Health specified details of database information sharing.
Results
The study population of 135 were predominantly male (83%), averaged 32.5 years of age at the time of the index offence (range 16–66), and were proportionately overrepresented by Maori (36%), as compared with European (54%) in the general population (although Maori comprise approximately 50% of the prison and forensic mental health populations). The primary diagnosis in 59% was schizophrenia, while a further 17% suffered other psychotic disorders. Mood disorders accounted for 13%, organic disorders 3%, and personality disorders 8%, the majority of whom had brief psychotic episodes at the time of their index offence.
These patients were predominantly violent offenders, and were all deemed to be a safety risk to the public. Murder was the index offence in 28.1% (n = 38), sexual violence accounted for a further 6.5% (n = 9), while other violence accounted for 51.1% (n = 69). Property offences contributed 9.6% (n = 13), and other offences 4.4% (n = 6).
Granting extended community leave before reclassification was uncommon in the 1980s (less than 20%), but increased to more than 70% during the most recent decade. This change reflected an increasing acceptance of the value and effectiveness of compulsory community treatment, which was introduced into New Zealand's civil commitment regime in 1992 with the Mental Health (Compulsory Assessment and Treatment) Act.
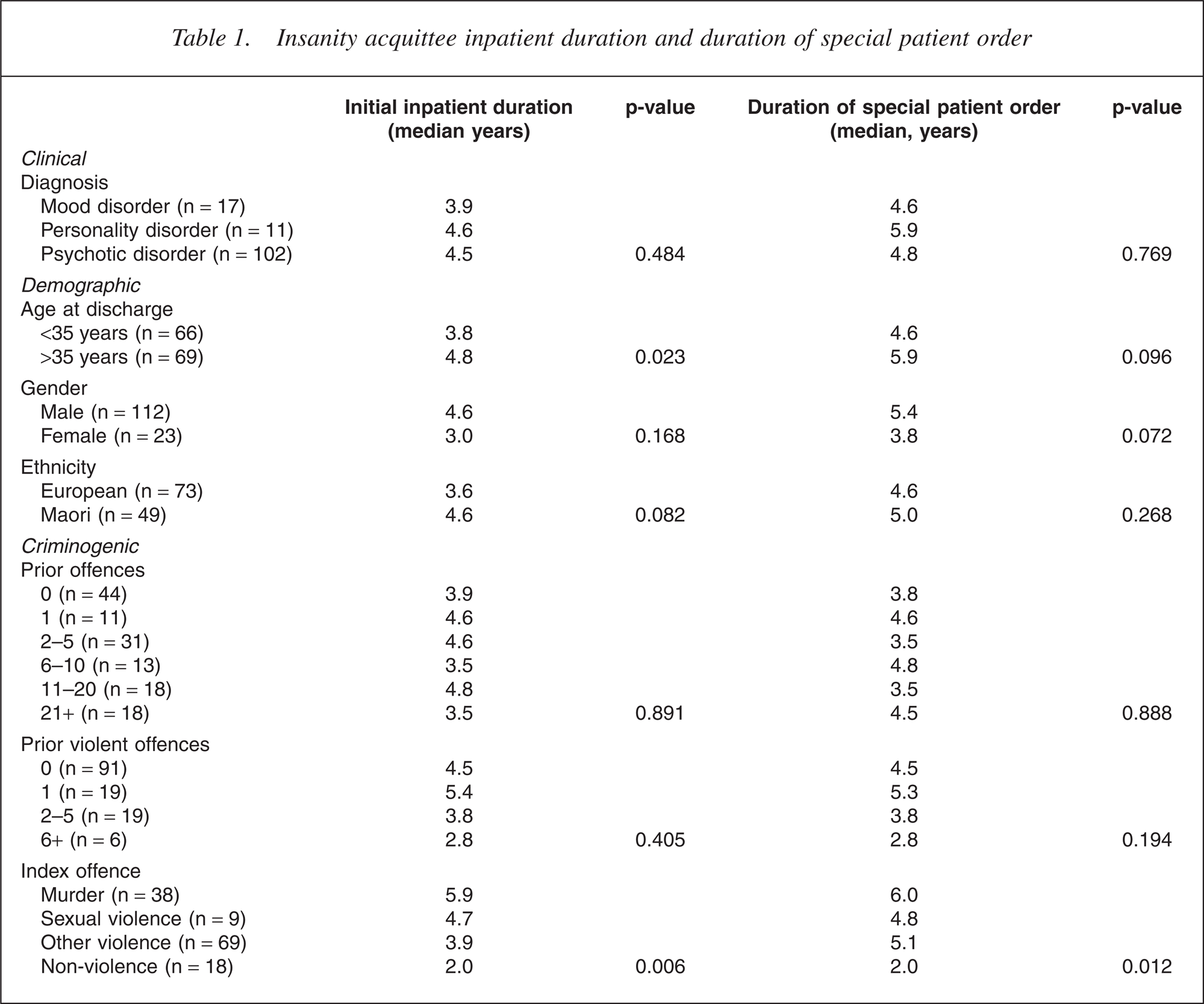
Overall, the initial period of inpatient admission averaged 5.0 years (range 0.3–15.9), while the duration of the special patient order averaged 5.5 years (range 0.3–17.0). The only variable predicting the duration of special patient order (p = 0.012) as well as the initial duration as an inpatient (p = 0.006) was the severity of index offence. Diagnosis, ethnicity gender and prior offending were not associated with inpatient duration or duration of special patient order (Table 1). Older age (<35 years), however, was associated with a longer inpatient duration (p = 0.023). One-third of discharged patients were readmitted within 2 years of discharge, eventually increasing to nearly 80% readmitted within 15 years of discharge (Fig. 1).
Cumulative non-readmssion rate.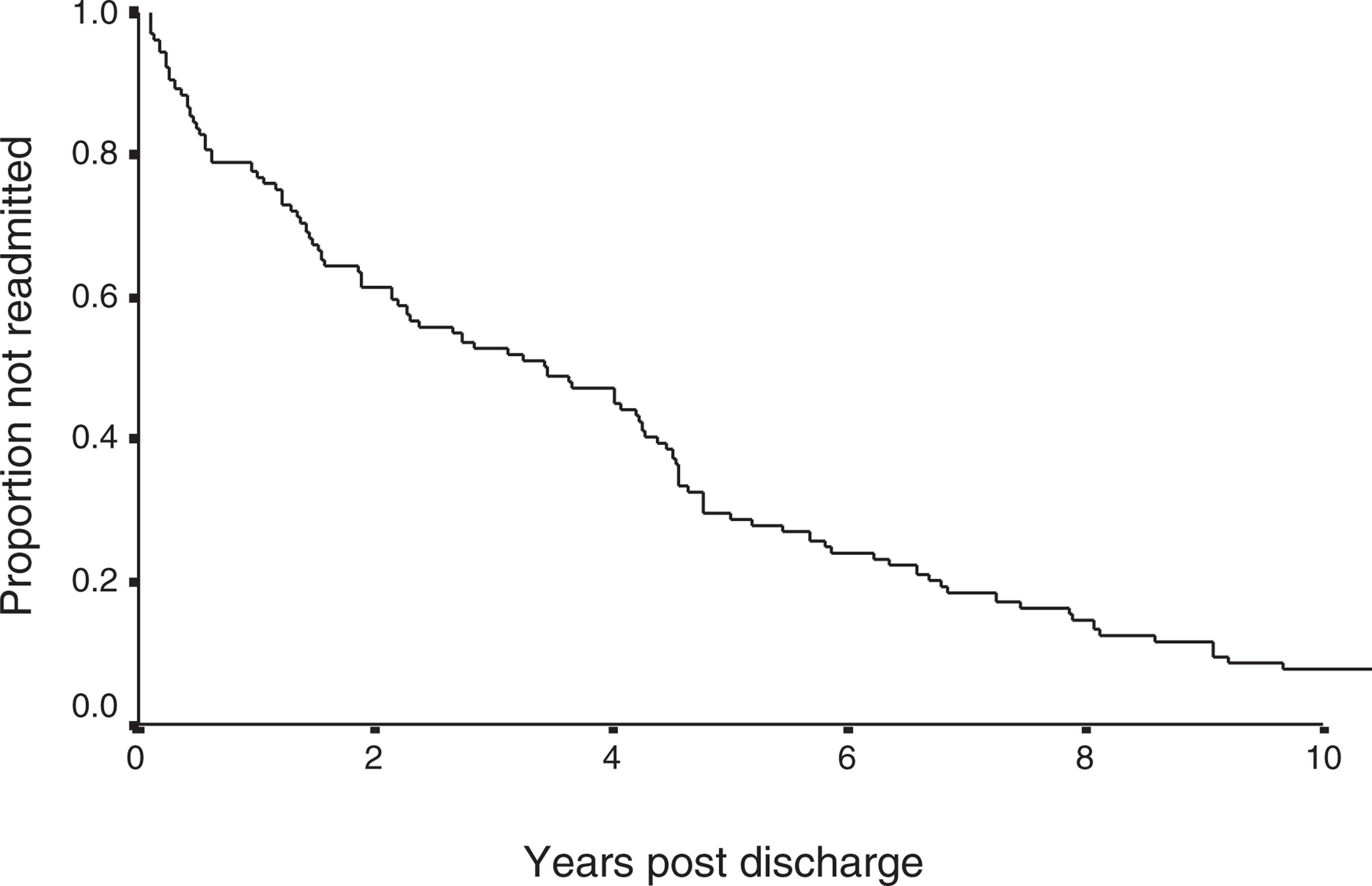
Insanity acquittee inpatient duration and duration of special patient order
The overall reconviction rate 2 years following discharge was 15% and this increased and plateaued to about 40% at 10 years following discharge. The violent reconviction rate over the same 2-year period was 5.8%. Neither the type of index offence, diagnosis or duration of initial admission predicted reconviction. However, ethnicity (p = 0.0126), age at discharge (p = 0.0166) and prior offending (p = 0.0035) were all significant predictors of violent reconviction. The same variables, as well as gender, were also associated with any reconviction (Table 2).
Insanity acquittee reconviction
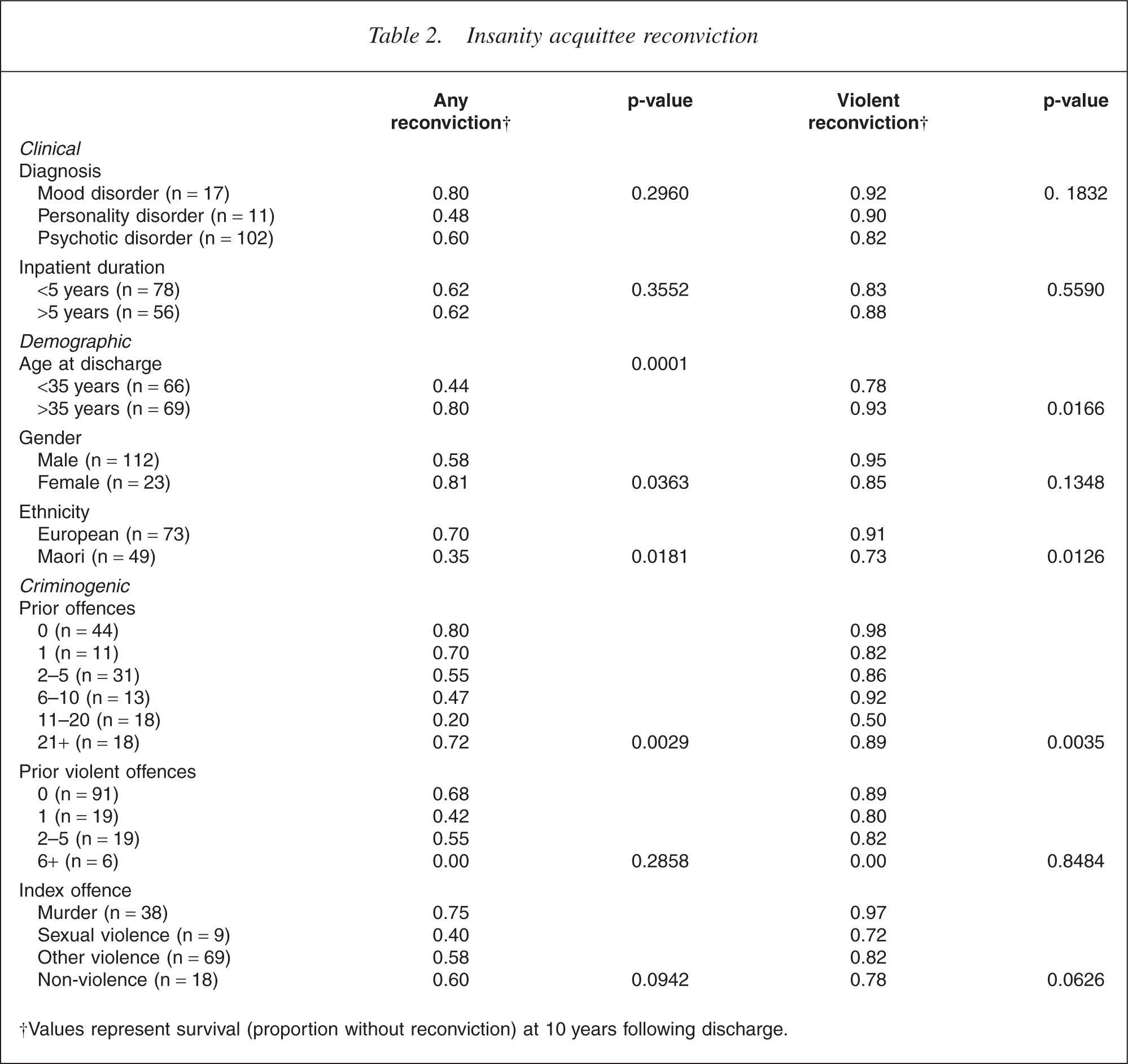
†Values represent survival (proportion without reconviction) at 10 years following discharge.
Discussion
Performance indicators for forensic services
Edwards et al. suggested that performance indicators for medium secure care would ‘describe the task of services as restoring mental health so that patients may be treated in conditions of lesser security, and preferably in the community within 18–24 months, without further incidents of violent or criminal behaviour’ [5].
Putting aside the important issue of measuring recovery in clinical terms, reoffending is also an important outcome in forensic populations. However, some caution must be exercised in interpreting reoffending outcome data in forensic populations for several reasons.
First, while it is apparent that reconviction significantly underestimates reoffending, the difference between reoffending and reconviction is less marked with more serious offending, and over the last decade 77% of all violent crimes reported to police were resolved, usually by way of prosecution (Statistics New Zealand). It is also known that the highest incidence of reoffending occurs in the immediate post-discharge period. Even employing the most sophisticated risk assessment and management strategies, some degree of reoffending is inevitable, which may be attributable to ‘unknowable’ factors, or factors unrelated to the patients' illness [6] and do not necessarily indicate program failure.
Second, although the same variables are repeatedly shown to correlate with reoffending in forensic populations, including age, gender, prior offending and ethnicity, these variables do not usually include clinical variables such as diagnosis, prior admissions, or duration of admission. It is unfortunate that assessments of risk aided by risk assessment instruments, such as the HCR20 [7], are seldom reported in the literature at the point of discharge, but they may provide a much more reliable clinical assessment of risk of reoffending.
A further issue to be aware of in comparing studies is whether the follow-up period includes periods of inpatient care, when reoffending and reconviction are less common. If we are concerned with public risk, the follow-up period should exclude inpatient time.
We suggest that in discharged forensic populations, serious or violent offending, rather than all criminal behaviours, is the outcome of most interest to clinicians, the general public and politicians, as it is questionable whether the risk of non-violent or minor offending should justify prolonged admissions, particularly with the well-known negative correlates of institutionalization. Further, applying some time limit to any outcome of this sort allows meaningful comparison with other populations. Notwithstanding political imperatives, although secure detention guarantees public safety, it becomes an increasingly unreasonable risk management strategy from a human rights perspective as the risk of reoffending diminishes. Decisions made at the point of discharge should focus on whether any risk can be safely managed in the community. Observing that the highest risk of reoffending occurs in the immediate postdischarge period, we have chosen somewhat arbitrarily to focus on the 2-year reconviction rate, beyond which time there will be a more sophisticated understanding of community adaptation, and rehospitalization can be effected if necessary. However, as can be seen from Fig. 2, the reconviction rate continues to increase, albeit at an ever diminishing rate, for at least two decades following discharge. Careful monitoring by wellresourced multidisciplinary community forensic teams should allow early intervention if there is any deterioration in mental state, or increase in risk. Readmission to hospital is one such risk management strategy, with approximately one-third of all patients in this study readmitted within 2 years of discharge. This rate of readmission may be higher than in general psychiatry because conditions of leave tied to known risk factors are intensively monitored, and there is a willingness on the part of forensic services to readmit in situations which may be managed in the community in general psychiatry. Having a low threshold for readmission provides political and public reassurance while also allowing patients the chance to demonstrate their ability to manage safe community living. It has been suggested that high rates of rehospitalization may in fact be necessary to achieve low rates of recidivism [6].
Cumulative non-reconviction rate. (—) Violent reconviction; (––––) Any reconviction.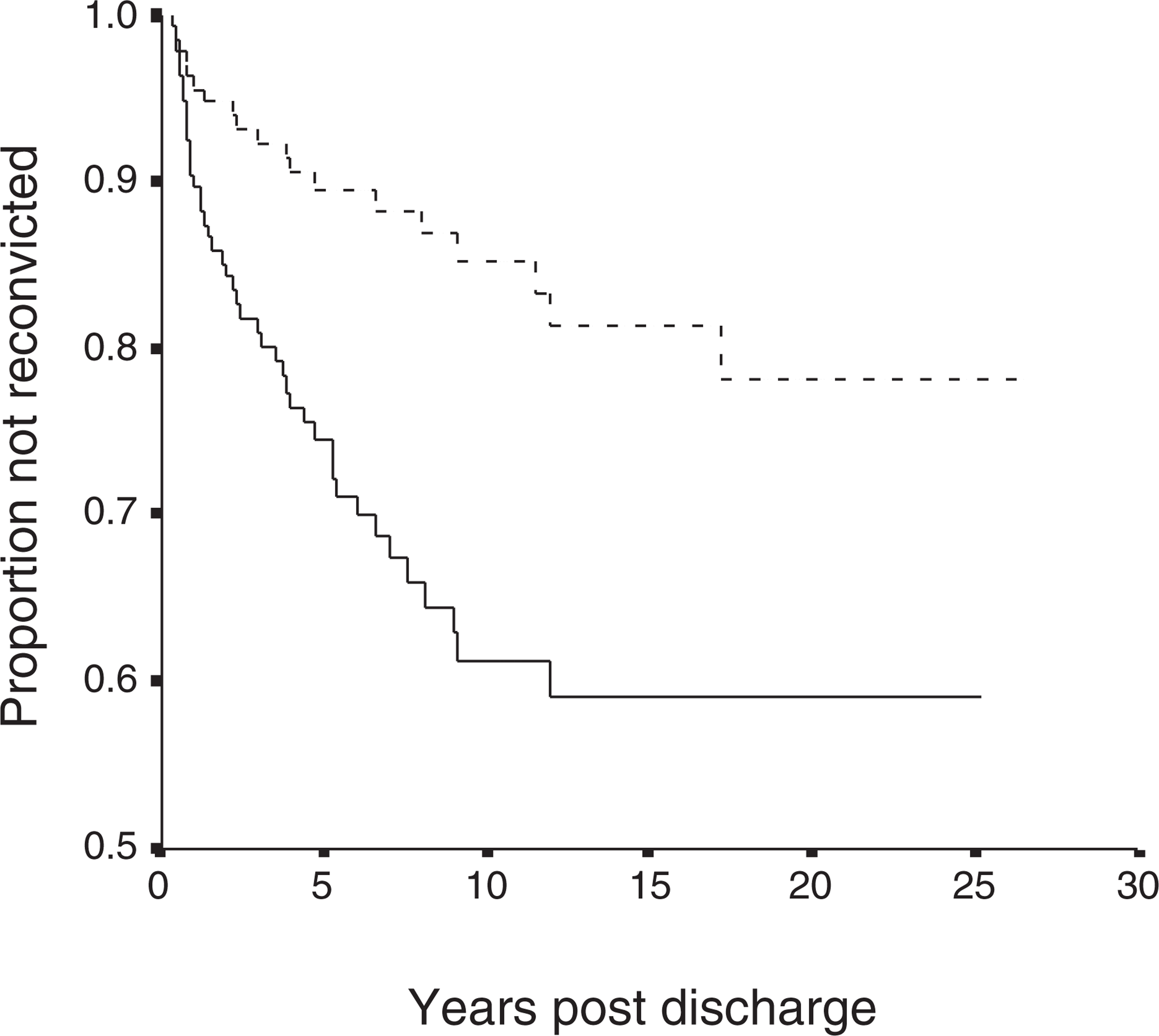
Only 6% of patients in this study were reconvicted of violent offences within 2 years of discharge (Fig. 2). Given the high resolution rate for violent crime reported to police in New Zealand, this reflects a very low rate of violent reoffending, suggesting that the current system operates conservatively, and that earlier release into the community under community forensic teams may be possible without exposing the public to unacceptable risk. Other studies with very similar rates of reconviction have concluded: ‘The rate of violent offending is so low that there is little scope for overall reduction and it would be better to concentrate on the identification of high risk patients’ [8].
Opponents of using criminal recidivism as an outcome measure for forensic populations [9, 10] have argued that follow-up studies repeatedly show an association between preadmission and post-discharge offending, and that psychiatric institutions are therefore ineffective in changing patterns of offending behaviour. While this study also found a strong association between prior offences and risk of reconviction, some other studies comparing the outcomes of matched prisoners and forensic patients show significant differences (e.g. [11]) in reconviction outcomes for these populations. It is only by matching for risk factors with different populations that comparisons can be made. In a follow-up to this study, we intend to do a similar match of this population with released prisoners to determine whether forensic services achieve better reconviction outcomes than prisons with similar populations.
Ethnicity
The proportion of Maori in this population (36%, 95% CI 28–44%) is lower than would be expected based on the prison and forensic health populations which comprise 50% Maori. This may reflect a cultural paradigm that sees Maori as less accepting of conventional psychiatric diagnosis or expert opinion. It has been demonstrated that incarcerated Maori present to mental health services in lower numbers and at a much later stage of illness than do their Pakeha counterparts reflecting this culturally based difference in perception of mental health ‘systems’ [12]. Other possible explanatory factors may include poor legal representation and advice to Maori involved in this process, or jury bias against Maori, although such possibilities could not be explored in this research.
Maori ethnicity was associated with violent reconviction in this population (see Table 2). This finding is also observed in released prisoners even when controlling for gender, age when released, type of offence, sentence type/length imposed, number of prior convicted cases and number of prior prison sentences [13]. It is notable that culturally based services were only in place over the latter part of this study period, and may have conferred benefits not seen over the entire period. Certainly, the impact of the development of culturally based services towards addressing this high rate of reconviction is a significant shift, the outcomes of which are worthy of further investigation.
Comparison with other programs
Comparison with three types of forensic or correctional programs merits consideration: insanity acquittee programs, forensic mental health treatment programs, and released prisoners. It must be noted that international comparison is complicated by the fact that forensic populations are usually defined legally, and with no two jurisdictions identical, generalization of findings is problematic.
Insanity acquittee programs
Harris summarized the peer reviewed literature from 1975 to 1999 relating to insanity acquittees and criminal recidivism, using re-arrest as the primary outcome measure [14]. We have already argued that the focus on all types of reoffending obfuscates the real issue of serious or violent reoffending. However, this meta-analysis suggested a ‘very strong direct linear relationship between length of follow-up and re-arrest rate’. The rate of rearrest for any offence at 2 years was approximately 10%, compared with a reconviction rate of 15% in our study. The somewhat lower rates of reoffending achieved internationally may be partly explained by the linear model applied, which ignores the widespread observation that the highest rate of reoffending occurs in the immediate post-release period. The higher rate of reconviction in the immediate post-release period was also evident in the findings of this study, highlighting the need for close supervision and monitoring during the period of initial transition into the community.
Forensic treatment programs
Similar rates of reconviction are described in various released maximum and medium secure unit populations in the UK (e.g. [5, 8,15–19]), but these populations are not clinically or legally equivalent with our study population, and the follow-up periods are not always started at the time of discharge into the community further complicating direct comparison.
Released prisoners
There were 22 340 prisoners released from New Zealand prisons between 1995 and 1998, of whom 6520 were violent offenders and therefore more closely resembled our population. Of the violent offenders, 65.3% were reconvicted of any offence within 2 years, and 28.3% of a violent offence within the same 2-year period [13]. Although this is nearly five times higher than the 5.8% violent reconviction rate within 2 years in our population, it must be remembered that the groups are not equivalent in terms of known risk factors, such as prior convictions (e.g. the released prisoners averaged 30 prior convictions, while the insanity acquittees averaged 9 prior convictions).
Policy implications
This study, along with other insanity acquittee followup studies, suggests that patients who committed more serious offences are detained in hospital longer than patients with trivial offences [3]. Previous New Zealand research has indicated that in Auckland, forensic patients (including insanity acquittees) are now released in accordance with clinical recovery rather than after a period of detention proportional to the severity of any offending [20].
However, while clinical factors may drive treatment setting for some forensic patients, the lengthy timeframes involved in the inpatient phase of rehabilitating of insanity acquittees are not justified by the relatively low rates of criminal recidivism following release, and are unlikely to be clinically justified given the average length of inpatient admissions in general mental health services which now occur in the context of well-developed community treatment services.
We suggest that policy-makers need to be clear about the expectations of any aftercare system for insanity acquittees. The public, and in particular any victims, have a right to demand a high level of accountability from the system charged with the task of rehabilitating the offender, but do not have the right to demand punishment. We suggest that the higher degree of accountability should be in place for a period of time proportional to the severity of the offending, but that it should not mandate inpatient care. Treatment should be in the least restrictive environment that is appropriate in the circumstances. In this study, severity of index offence was the strongest predictor of inpatient duration, and special patient duration. While the latter fits with proportional accountability, it is not clear that the former does. The seriousness of the index offence is one of many relevant considerations in determining the duration of hospitalization. Inpatient stays of many years for the most serious offenders are probably not needed to protect the public from risk of violence in most cases, and may be counterproductive in this regard. Public demands for safety and accountability can probably be met by shorter inpatient periods and a longer community period of intensive monitoring and support, with unobstructed access to hospital readmission.
If the current system is reformed, one key issue will be whether political accountability should be replaced by a quasi-judicial tribunal, as has occurred in some Australian jurisdictions (e.g. Queensland). There are certainly theoretical advantages with such reform in maintaining a consistent judicial framework throughout the special care period. Laudable attributes of any aftercare system include accountability, transparency of process, meaningful inclusion of patient, family, public and victims' interests, and the presence of appeal mechanisms. Although some of these features are lacking in New Zealand's current system, there is no barrier to forensic community care being provided at an earlier stage in the recovery of insanity acquittees.