
Abstract
Disorders of perception comprise some of the most important and complex phenomena encountered in psychiatric assessment. This complexity is due to the varied clinical contexts in which these disorders occur and the heterogeneity of their content. Perceptual disturbances, particularly hallucinations, are usually but not always characteristic of psychiatric disorders such as schizophrenia and delirium. Complex visual hallucinations (CVH) have been associated with organic brain disease, and are a common referral reason to psychiatrists in consultation-liaison, old age and neuropsychiatric settings. Accurate diagnostic assessment requires a detailed elucidation of the clinical features and associated investigation findings, an understanding of alternative phenomena such as visual illusions and distortions and an appreciation that terms such as Charles Bonnet syndrome (CBS), peduncular hallucinosis (PH) and organic hallucinosis have been poorly defined. By presenting three illustrative case reports, we aim to clarify the current understanding and nosology of visual hallucinations and discuss some of the putative biological mechanisms involved.
Case report A
Mrs VH was an 85-year-old widow with a long history of visual impairment who lived at home alone presented with a 2 day history of visual changes. These began with the experience of a ‘grey blind’ coming down over her left visual field over a number of minutes, without other neurological symptoms. Within hours her entire visual field was covered by a translucent sheet ‘… with yellow and pink flowers, like a nightdress’, and moving ‘like a sheet on a washing line’. Mrs VH was not distressed, until she subsequently saw frequent disembodied and grimacing male faces, mainly that of a James Bond actor. These faces then appeared on the bodies of ambulance officers and family members. Over the next 24 hours following hospital admission she continued to see these faces, which melted and distorted, as well as troops of children, one to two feet tall and in green-blue uniform, marching around her hospital bed. These hallucinations were prominent at night, and Mrs VH was observed stepping around perceived objects in an empty ward corridor. When interviewed, she described the phenomena as very real and was frightened they would recur. Thorough neuropsychiatric evaluation revealed no other neurological symptoms, perceptual disturbance, or other psychotic phenomena. Mrs VH also denied alterations in mood or recent changes in memory or other function.
Mrs VH's past medical history included 15 years of visual impairment (thought to be secondary to glaucoma), medicated hypertension, type-2 diabetes mellitus and hypercholesterolemia. There was no past or family psychiatric history. Medications included metformin, glipizide, amlodipine, irbesartan, simvastatin and timolol.
On physical examination, Mrs VH was normotensive and afebrile, with no carotid bruits or other cardiovascular findings. There were no focal neurological signs. Opthalmoscopy revealed bilateral severe macular degeneration and cataracts. On mental state examination she was awake and alert, and appeared anxious. Apart from her visual hallucinations, there were no other disorders of perception and she had partial insight. Cognitively, her attention, verbal and spatial memory and language were intact. There were no disorders of executive function or praxis, although constructional abilities were limited by poor vision. Her Mini-Mental State Examination [1] score was 25/25, with five points unable to be tested resulting from her visual impairment.
Routine blood investigations were within normal limits and electroencephalogram showed no evidence of encephalopathy or epileptiform activity. A single-photon emission computed tomography scan showed no areas of hypoperfusion, and occipital perfusion was normal. Magnetic resonance imaging (MRI) demonstrated multiple subcortical white matter intensities throughout deep white matter, and lesions bilaterally in the pons (Fig. 1A). On the basis of her abrupt-onset formed hallucinations (with patterned, Lilliputian and grotesque facial content), her lack of evidence of a delirious process or cognitive impairment, lack of other neurological signs and pontine lesions of likely vascular origin on MRI, a diagnosis of PH was made and she was commenced on olanzapine 2.5 mg at night. The hallucinations resolved after further 48 hours of olanzapine therapy.
Magnetic resonance imaging scans of cases A, B and C. (A) Axial fluid-attenuation inversion recovery (FLAIR) image of the brain demonstrating pontine white matter lesions (arrow). (B) T2-weighted scans show new right thalamic infarct (arrow), in addition to a moderate amount of periventricular white matter disease. (C) Preoperative T2-weighted scan showing left temporal/inferior parietal arteriovenous malformation (arrow), abutting the optic radiation.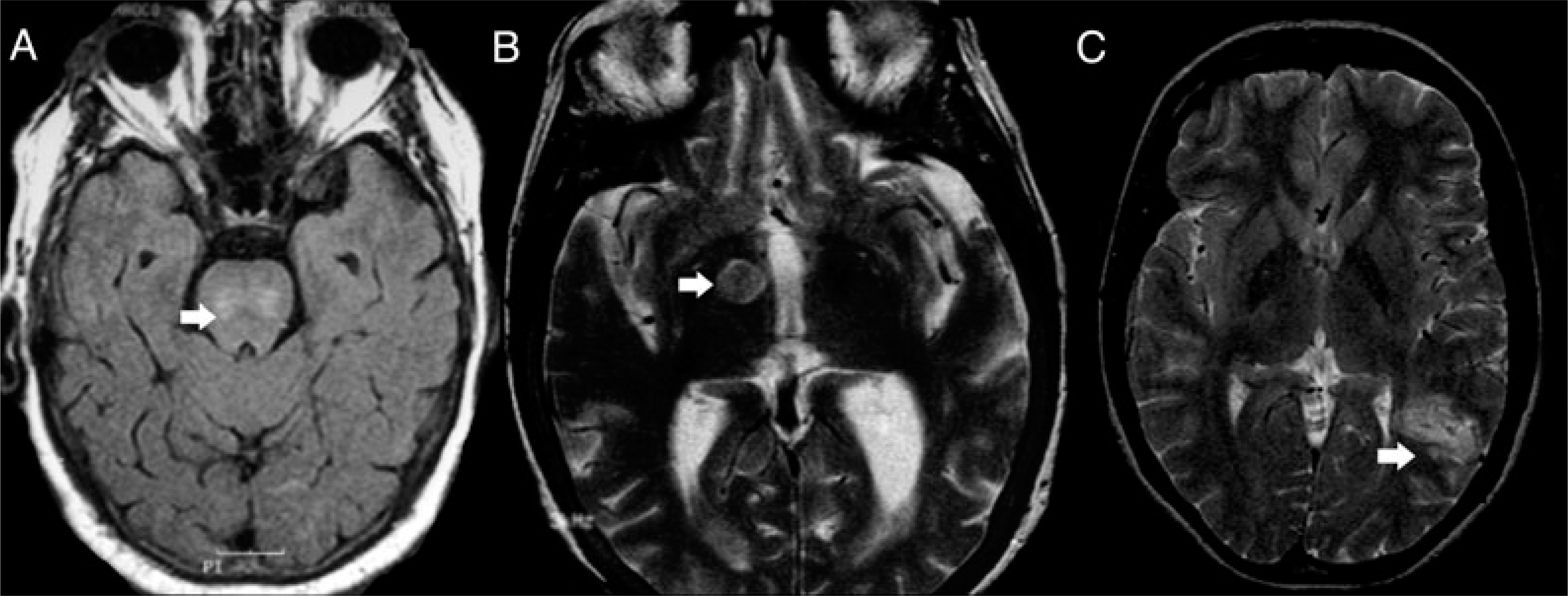
Case report B
Mrs CH was a 68-year-old woman who presented with a 3 week history of visual hallucinations. At the age of 38 years she had had a large left frontal haemorrhage, of presumed hypertensive aetiology, which she survived without significant cognitive or neurological sequelae. The hallucinations were of sudden onset, initially in the periphery of vision and without any other neurological symptoms. The patient described seeing small children in groups of three or four which appeared smaller than usual. They were dressed in colourful uniforms. Occasionally she felt they were calling her name. There were no other hallucinatory experiences. She was described as inattentive and disoriented with worsening confusion at night. There was no significant family or past psychiatric history. No medications were prescribed and there was no history of substance use.
On neuropsychiatric examination Mrs CH was afebrile and normotensive and there were no focal neurological findings. Fundoscopy was normal. There were no frontal release signs or features of parkinsonism. She was euthymic, had normal language function and there was no evidence of other disorders of perception or psychosis. By the time of examination the inattention had resolved, cognition was intact and Mrs CH had full insight into the hallucinatory experiences.
Routine investigations, including electrolytes, were within normal limits. An urgent computed tomography scan excluded any new haemorrhage, but demonstrated a developing lucency in the right thalamus consistent with a new infarct. An MRI scan 5 days after this confirmed a right thalamic lacunar infarct (Fig. 1B) as well as a frontal defect consistent with the old haemorrhage and periventricular white matter changes in keeping with the patients age.
A diagnosis of CVH due to a new thalamic vascular lesion was made and Mrs CH was commenced on risperdone 1 mg at night. The symptoms resolved completely after 1 week, and medication was successfully withdrawn.
Case report C
Ms VC was a 33-year-old single woman who had been diagnosed with a left temporoparietal arteriovenous malformation (AVM – Fig. 1C) on MRI after presenting with headache at the age of 25 years. The AVM had been angiographically embolized and surgically removed without significant complications. Ms VC successfully returned to her previous employment. One year later the lesion was found to have recurred medial to the surgical site, adjacent to the lateral ventricle, and although surgery was not recommended at that time, she was lost to follow up. She periodically had ‘flashes of light’ in the intervening 6 years, which were diagnosed as migraine. There were no significant features in the family or developmental history and no past history of psychiatric disorder.
At age 33 years Ms VC developed transient right visual field loss over a period of hours without any associated neurological features or headache. This was followed by a witnessed grand mal seizure resulting in admission to hospital. At that time all routine investigations were unremarkable and neuroimaging revealed no new findings.
Three days later, Ms VC reported a number of visual hallucinations with complete maintenance of insight. She saw red letters (W, R and K) on people's faces and on her own face in the mirror. She saw ‘hundreds of little spikes’ coming in and out of the floor and small ants moving on regularly patterned surfaces. These were experienced predominantly in the right visual field. During the following days she saw groups of disembodied faces and torsos floating 10 feet above the ground. These images were monochromatic, unfamiliar, of normal size and mobile. Although they moved their lips giving the appearance that they were talking to her, Ms VC experienced no auditory perceptual disturbances. There was no palinopsia and these experiences disappeared with eye closed and were worse in fading light.
Ms VC presented as anxious, but was otherwise euthymic and there were no features of delirium. No other psychotic features were noted, there were no focal neurological signs and fundoscopy was normal.
Routine blood investigations including electrolytes were normal. Electroencephalogram showed a midtemporal epileptiform focus, approximately at the site of the recurrent AVM. Ms VC was treated with phenytoin, which resulted in full resolution of her symptoms over the next 24 hours. The diagnosis was made of CVH resulting from an irritative, epileptogenic focus of the left temporal lesion.
Discussion
Each of the above cases describe examples of visual hallucinations occurring in the context of structural brain lesions and illustrate the difficulty categorizing such phenomena. In 1838 Esquirol provided the earliest and simplest definition of a hallucination as a percept without an object, perceived as real and in the external environment [2]. Slade refined this definition to refer to a percept-like experience in the absence of an external stimulus that is experienced as a true percept, is spontaneous, unwilled and cannot be readily controlled [3, 4]. Edition IV of the Diagnostic and Statistical Manual (DSM-IV) drew on this to define hallucinations as a ‘sensory perception that has the compelling sense of reality of a true perception but that occurs without stimulation of the relevant sensory organ’ [5]. Hallucinations may have a common origin in internal experiences in healthy individuals and in neuropsychiatric illness, where in illness states a failure in reality testing results in this internal experience being misattributed externally [4, 6].
A hallucination is phenomenologically distinct from either a sensory distortion or a false perception. A distortion refers to perceived changes in the nature of a real object, such as changes in intensity (louder or brighter), or geometric properties (larger/smaller or distorted). Other false perceptions include illusions in which an object is transformed into another form and pseudohallucinations. Pseudohallucinations are experienced as percepts that arise from the patient's inner world rather than the external environment and are usually recognized as ‘not real’ and/or as vivid internal visual imagery [7, 8]. These perceptual disturbances are generally considered to occur along a continuum from reality-based percepts through to frank hallucinations [9], in common with a range of other psychotic symptoms such as delusions, passivity experiences and thought alienation [10]. Visual hallucinations are more strongly associated with ‘organic’ illness such as visual pathology, neurodegenerative disorders or central nervous system (CNS) lesions [11–13] rather than ‘functional’ psychiatric disorders such as schizophrenia where auditory hallucinations are more common.
Visual hallucinations of an organic aetiology are frequently characterized by variability in insight. Although the patient in case A described being frightened by the hideous faces she saw, she clearly identified them as not real once they abated. The patients in cases B and C always identified their experiences as not real. Hence, these experiences do not always strictly meet phenomenological criteria for hallucinations. Classificatory systems such as the International Classification of Disease (ICD-10) acknowledge this by the use of terms such as ‘organic hallucinosis’ [14]. The use of the term ‘organic’ is problematic when used to describe psychiatric symptoms or syndromes [15] as it implies that there are ‘nonorganic’ hallucinations that lack a biological substrate.
Although the form of visual hallucinations described in these cases is protean, there are common features: their vivid and colourful nature(cases A, B, C), the inclusion of small people or children (Lilliputian hallucinations [LHs], cases A and C) and the involvement of regular patterns (cases A and C) or disembodied faces or limbs (cases A and C). These complex visual phenomena are differentiated from more simple, unformed hallucinations such as crudely formed flashes of light and colour, or indistinct forms. Complex visual hallucinations may also include branching or tessellated patterns, vivid and colourful formed animals (real or bizarre), soldiers or others in uniform, landscapes and complex scenes. Complex visual hallucinations are frequently associated with a variety of visual distortions, such as palinopsia, in which repeated images of a perceived image is seen, or distortion of a face or head (prosometamorphopsia) [16].
Complex visual hallucinations – the role of lesion location
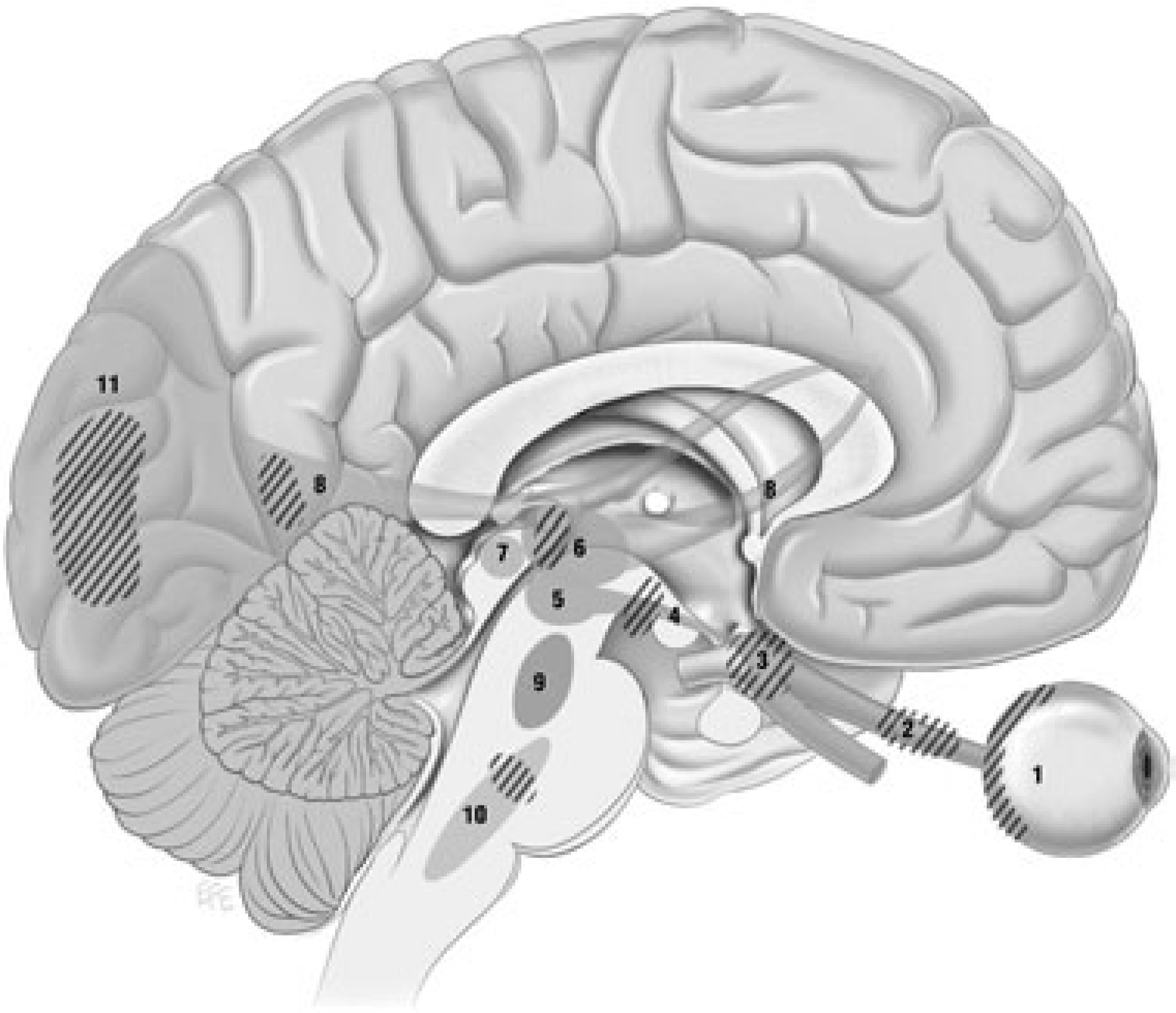
The anatomy of the retinogeniculocalcarine tract is well understood, including how lesions of the tract at different levels produce classically described visual field defects (Fig. 2). Although these not completely characterized in mammals, basal projections onto this tract arise from excitatory cholinergic centres (parabrachial and parabigeminal nuclei) with inhibitory serotonergic input coming from the dorsal raphe nuclei [16] (shown in Fig. 3). At the centre of this tract lie the dorsal lateral geniculate nucleus (LGN) of the thalamus and the lateral pulvinar. The primate pulvinar has an important role in simple visual processing, but also visual salience (generating signals related to the salience of visual objects) and linking eye movement to this function [17].
Retinogeniculocalcarine tract. Optical information from retina (1) passes along optic nerve (2) through the optic chiasm (3) and optic tract (4) into the lateral geniculate nucleus of the thalamus (5) where it receives input from the superior colliculus (7) via the pulvinar (6) and then traverses the optic radiation (8 and 9) through temporal lobe (13) into visual cortex (10–12). Intersection of ascending pathways. Optical information in the retinogeniculocalcarine tract (1–8, 11 as in Fig. 2) is modulated by ascending input from pedunculo-pontine and parabrachial nuclei (9) and raphe nuclei (10) via the superior colliculus (7). Hashed areas show regions where interruptions are known to produce visual hallucinations.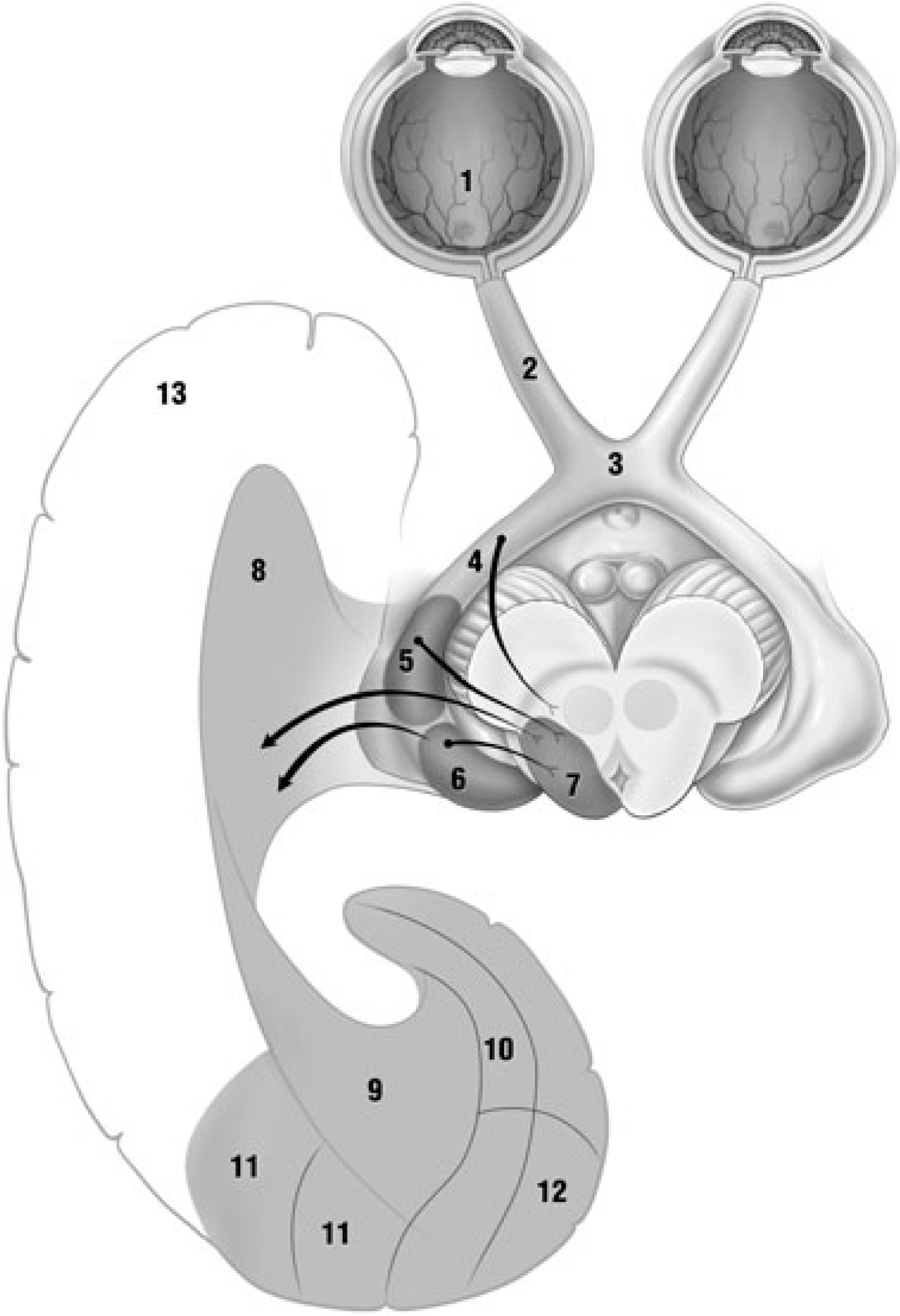
Retinal or other proximal lesions remove or disturb direct inputs of the external environment to the visual system. Complex visual hallucinations may then arise from spontaneous discharges in distal portions of this system [18] (Fig. 4a). Brainstem lesions may disrupt these serotonergic inhibitory raphe nucleus inputs resulting in excitation of the dorsal LGN and dysregulation of retinal inputs resulting in CVH (Fig. 4b). The dorsal raphe nuclei have also been implicated in both the sleepwake cycle [19] and regulation of rapid eye movement (REM) and non-REM sleep [20] in mammals. Sleepassociated CVH may be seen in normal sleep (hypnopompic and hypnogogic hallucinations), sleep disorders (narcolepsy–cataplexy syndromes), delirium and Lewy Body Dementia. Complex visual hallucinations in CBS are often accentuated in states of reduced consciousness or fading light. These clinical findings further suggest an important role of the dorsal raphe system in the generation of CVH. Thalamic lesions may directly affect critical structures such as the pulvinar or the associated brainstem inputs described above, and disrupt visual processing and salience (Fig. 4c). Damage to retinal inputs in this area may also operate in the same fashion as a more proximal de-afferentating lesion.
It is also possible that CVH arise from lesions in other cortical areas, such as the frontal and temporal lobes which project to the visual system via the dorsal LGN and medial pulvinar [17]. These regions are essential for object recognition and linking ideas and concepts with the perceptual experience of the external environment [21]. Complex visual hallucinations can also occur in lesions of the occipital cortex usually within the dysfunctional hemianopic field [22, 23]. This may relate to disruption of corticothalamic projections and generation of percepts within adjoining intact visual or visual association cortex [24]. However, this is also suggestive of ‘back-projection’ of images stored in other intact cortical systems, but in this case into a disturbed visual field. This may represent a normal process by which the percept generated by the visual system is linked to visual, verbal and affective memory (generating an ‘internal’ percept) in order for it to be identified [21, 25]. Epileptiform discharges may generate hallucinations in a similar fashion. However, there is some evidence visual cortex can be activated by discharges originating in visual association areas in temporal and parietal regions, indicating a mechanism for CVH in some cases of temporal lobe epilepsy [16].
While differing pathologies may lead to complex visual hallucinations, the form these hallucinations take may relate to particular cortical locations. Using factor analysis of clinical information collected from patients with CBS linked with predominately primate functional MRI and neurophysiological information, Santhouse and Howard have postulated that CVH in CBS can be linked to hierarchical visual pathway streams [26]. These workers suggest hallucinations of extended scenes and people and objects (including LHs) are associated with the ventral occipitotemporal cortex, hallucinations of faces and facial distortions (prosopometamorhopsia) with the superior temporal sulcus, and visual perseveration and delayed palinopsia (reappearance of a percept with shift in gaze after time delay) with visual parietal regions [26]. These compelling findings await further study and clarification.
Complex visual hallucinations have been reported in a wide variety of clinical and non-clinical circumstances. They may occur as hypnopompic or hypnagogic phenomena in healthy individuals or in sensory deprivation states [27]. Complex visual hallucinations have been described in narcolepsy–cataplexy syndrome, delirium tremens, Parkinson's disease, Lewy Body Dementia, intoxication with psychoactive substances and temporal lobe epilepsy. The best described conditions characterized by CVH are PH and the CBS, both clinical syndromes encompassing CVH and historically associated with particular clinical contexts.
Peduncular hallucinosis
‘Peduncular hallucinosis’ is used to describe vivid and complex hallucinations in the presence of lesions of the midbrain and/or thalamus [28]. PH was first described by the French neurologist and neuropsychiatrist Jean Lhermitte in a 72-year-old woman with hallucinations of strangely, colourfully attired people and groups of children which occurred at dusk [29]. These were associated with no alteration of conscious state and neurological signs consistent with an infarct of the pons and midbrain. Lhermitte's colleague Von Bogaert coined the term ‘peduncular hallucinosis’ in his description of a patient with a similar presentation, together with post-mortem neuropathological evidence of midbrain infarction [30]. The term ‘peduncular’ was not intended as a reference solely to the cerebral peduncles but to the whole midbrain and its surrounds. De Morsier extended the syndrome to include thalamic lesions, and re-established the lesion model for PH [31] whereas his predecessors had suggested sleep-wake cycle disturbances and ego dissolution as the likely origins [29, 30].
PH has subsequently been associated with a range of differing CNS pathologies, including vascular and infectious midbrain [32], pontine [33] and thalamic lesions [34], local subarachnoid haemorrhage [35], compression by local [36, 37] and distal [38] tumours, basilar migraine [39], basilar vascular hypoplasia [40] and following regional surgical [41] or angiographic [42] interventions. Most of these pathologies have been basilar in location, and resolution of hallucinations has been noted to result from treatment of reversible pathologies such as compression [43]. Common hallucinations include animals, people or children, grotesque and deforming faces or heads, landscapes and tessellated patterns, and groups of people walking in file are commonly reported [31, 34, 44].
PH frequently presents with LHs, defined by Leroy as a visual phenomenon in which a patient views detailed miniature people in lines or groups, often undertaking unusual postures or actions, usually accompanied by wonder rather than terror [45, 46]. LHs can occur in a range of neuropsychiatric syndromes including schizophrenia [47], dementia [48], encephalomyelitis [49], traumatic brain injury [50], AIDS-related dementia [50], multiple sclerosis [51], side-effects of dopaminergic and anticholinergic anti-Parkinsonian medication [52] and abuse of over-the-counter substances such as cough syrup [53]. Generally, LHs have been felt to have no localizing significance [54], although they have been reported in basilar conditions such as basilar migraine [39] and are a common presentation in PH [22].
Risser and Powell have reviewed the commonly reported features of PH [44], seen in Table 1 alongside those reported to characterize CBS. These are predominantly formed and colourful visual hallucinations, occurring during clear sensorium and often during night-time. Interestingly, they also noted that peripheral (ocular) rather than central visual (CNS) dysfunction may be present.
Comparative features of peduncular hallucinosis and Charles Bonnet syndrome
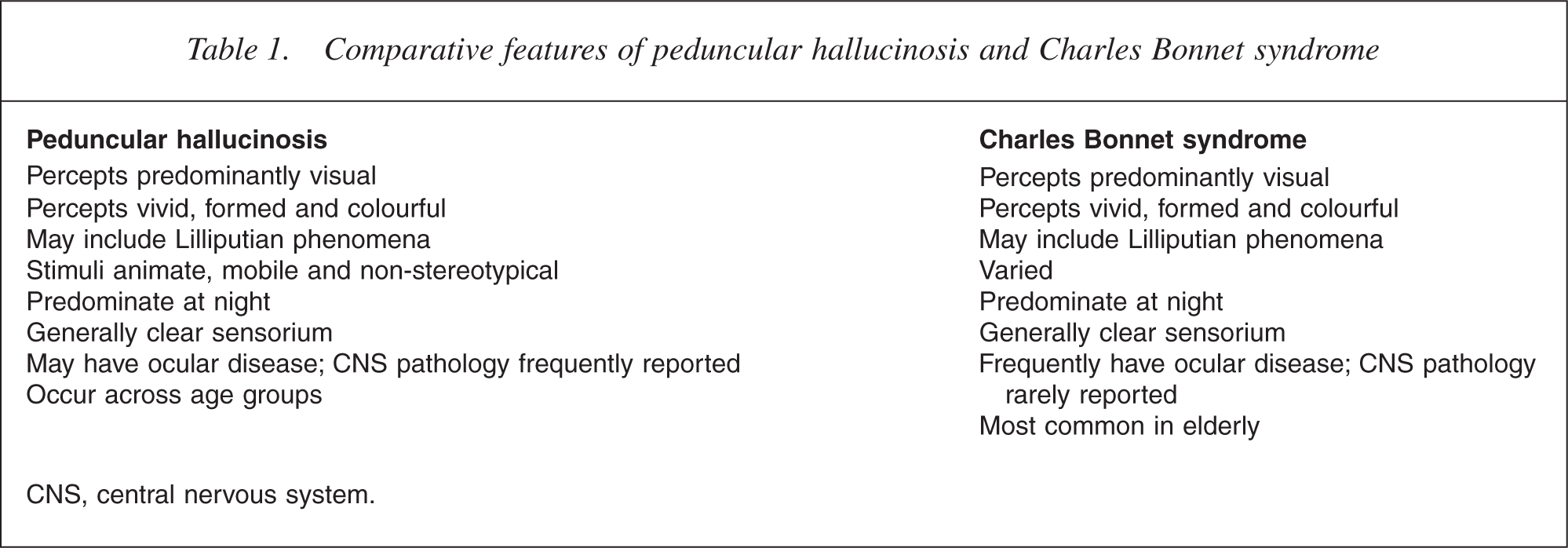
CNS, central nervous system
The lesions responsible for PH appear to impinge on the brainstem reticular formation or its thalamic targets [16] (Fig. 4b,c). Whereas lesions in visual pathways appear to produce hallucinations via release phenomena in the visual cortex through loss of corticocortical or thalamocortical inputs (Fig. 4a), mesencephalic lesions may produce hallucinations via interruption to serotonergic inhibitory afferents into the dorsal LGN of the thalamus, resulting in a dysregulated LGN which then projects to visual cortical regions [16]. Of note is that an allied auditory form of PH has been reported and associated with pontine lesions of varying pathologies [55, 56], and the underlying neurobiology again is reported to be loss of serotonergic raphe nuclei ascending inhibition.
Lesions and their effect on the visual circuit. (a) Lesions in the proximal visual system may result in deafferentation producing in ‘release’ activity in the cortex, with CVH arising from spontaneous discharges in visual and associated cortical areas. (b) Brainstem lesions involving the dorsal raphe system result in loss of ascending inhibition to the dorsal LGN may result in a hyper-excited geniculate and generation of CVH at the cortical level. (c) Lesions involving thalamic nuclei may disrupt the important processing function of these structures possibly resulting in impaired retinal signals and CVH. 1, retina; 2, lateral geniculate nucleus; 3, pulvinar; 4, superior colliculos; 5, occipital cortex; 6, doral raphe nuclei; 7, parabrachial and pedunculopontine nuclei; 8, reticular nucleus of thalamus.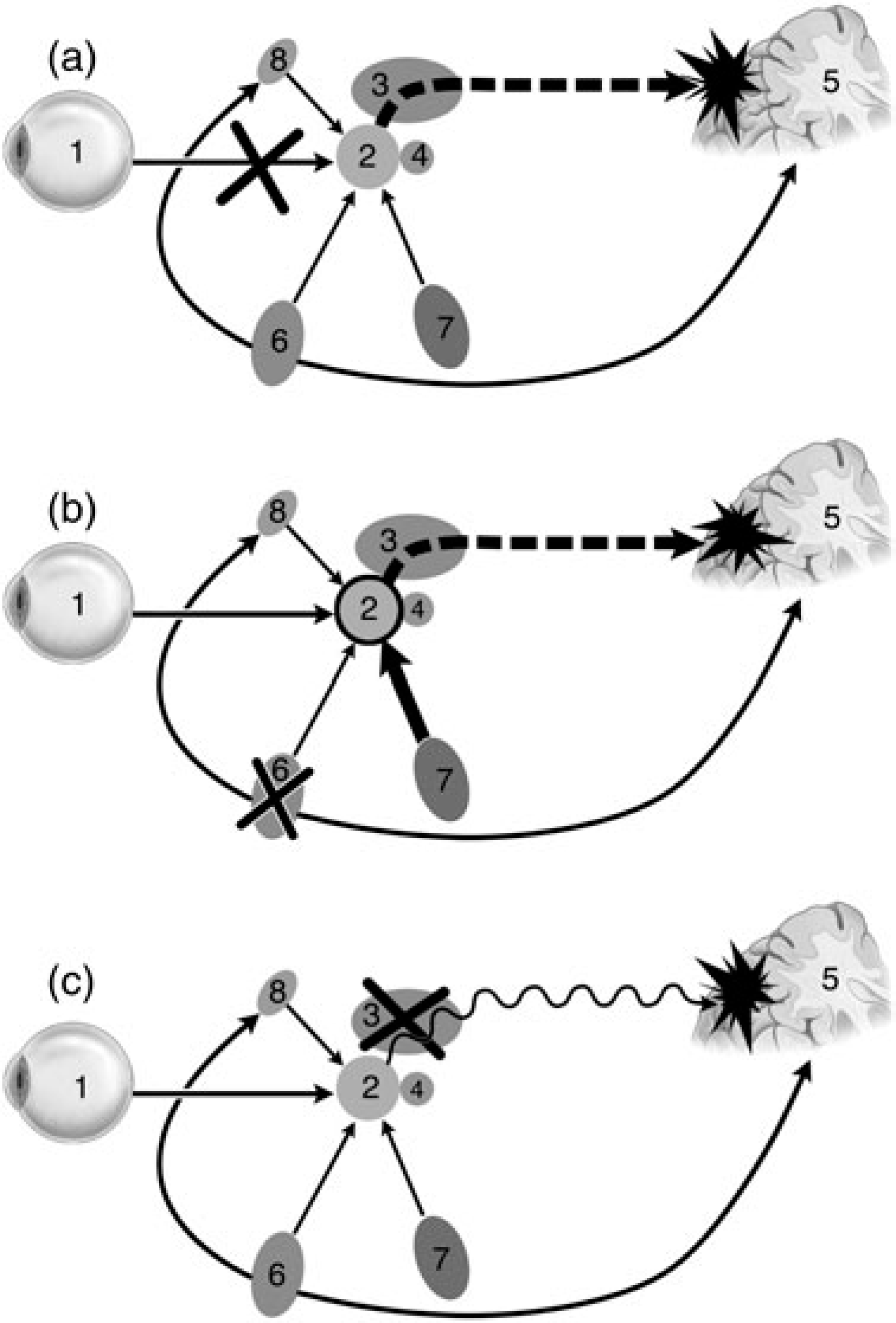
Charles bonnet syndrome
Charles Bonnet syndrome describes a group of patients with visual hallucinations in the setting of visual loss, and shows significant clinical overlap with PH. In 1769 Charles Bonnet described his 89-year-old grandfather who was healthy but blind as a result of severe cataract disease. He experienced colourful visions of men, women, fantastical birds and buildings, which changed in size, shape and location but were never accepted as real [57]. Later, Bonnet described similar experiences when he himself developed visual impairment [58]. There has been an extensive case-report based literature over the past 200 years describing groupings of similar phenomenology, generally including the appearance of complex visual hallucinations without other psychopathology and in the presence of a clear sensorium. However, little agreement exists as to whether eye or brain pathology is central to constitute this syndrome, unlike PH where aetiology is implicit. De Morsier, who eponymized the syndrome, de-emphasized eye pathology, and some recent authors have employed the very broad definition: ‘any state of visual hallucinations in the elderly irrespective of accompanying symptomatology’ [59].
More recently, visual impairment has been regarded as central to the syndrome [60]. In a large systematic review, 12% of visually impaired people met criteria for CBS defined as complex visual hallucinations associated with insight and in the absence of other disorders of perception or delusions [12]. Sufferers had a mean age of 74.5 years, showed a female preponderance and suffered from common causes of visual loss in this age group (macular degeneration 56%, diabetic retinopathy 17.5% and glaucoma 6.5%). Hallucinations generally included clear, colourful and often Lilliputian images of people, animals and inanimate objects which often varied over time. They tended to occur in the evening, poor light, or personal isolation. These patients were not screened clinically or radiologically for CNS disease, meaning that CNS lesions such as those found in PH cannot be excluded.
Many attempts have been made to understand the neurobiological basis of CBS. In general, most authors have agreed on the important role of reduced or absent visual system stimulation or input. This altered input may originate not only from the retina (such as in macular degeneration or cataract disease) but from lesions at any point in the visual system (including lesions of intracerebral visual pathways or visual cortical areas – Fig. 4a).
Berrios and Brook understood hallucinations in CBS as de-afferentation phenomena which resulted from ‘intracerebral perceptions’ not unlike the ‘phantom limb’ syndrome [59]. De-afferentation in the CNS has been shown to result in cortical hyperexcitability, secondary to presynaptic neurotransmitter vesicle changes, postsynaptic receptor up-regulation and changes in GABA (γ-aminobutyric acid) and NMDA (n-methyl-d-aspartate) sensitivity in surrounding CNS regions [18]. Hence, minor stimuli may be elaborated into complex hallucinations when received by a system disordered in this fashion. An effective de-afferentation may also occur following ocular lesions. Downstream cortical changes may result in ‘minor’ stimuli being amplified, distorted and elaborated into complex hallucinations when received by a hyper-excitable cortical network. Spontaneous activity in the absence of sensory input can also result from de-afferentation, resulting in bursts of paroxysmal synchronous electro-physiological discharges resembling seizure activity and potentially resulting in de novo image formation [18, 61]. This has been supported by attenuation of hallucinations in CBS when anticonvulsants are used [62]. We would favour a more restricted definition of CBS as a syndrome where lesions to primary visual pathway structures result in reduced visual throughput of the retinogeniculocalcarine tract and produce a functional de-affererntation syndrome.
Complex visual hallucinations – a common pathophysiology
Without an understanding of the preceding sections the three presented cases could be simply diagnosed as a case of CBS in a blind, elderly patient (case A), a diagnosis of PH in a patient with a new thalamic infarct (case B) and CVH secondary to epilepsy originating from mid temporal scarring (case C). Further scrutiny of each of these cases, however, allows for a more sophisticated understanding.
The early symptoms described in case A are suggestive of a vascular event such as infarction. Although the descending ‘grey blind’ approximates the classic features of amaurosis fugax (transient monocular blindness resulting from embolization of retinal arteries), involvement of the left visual field is more suggestive of a lesion distal to the optic chiasm. Rather than solely arising in a de-afferented visual system the CVH in case A are more likely to have resulted from an ischaemic vascular event affecting ascending structures superimposed on a visual system made vulnerable by both de-afferentation (blindness) and previous vascular disease (represented by extensive white matter disease in cortex and brainstem seen on MRI).
In case B, although the thalamic infarct, probably resulting from hypertensive small vessel disease would account for the onset of delirium and CVH, pre-existing pathology could also contribute to a vulnerable substrate. The scarred area resulting from the frontal haemorrhage some 30 years previous may have involved the temporal portion (Meyer's loop) of the optic radiation. Lesions of the tract in this region may result in an upper and peripheral visual field defect, and the hallucinations originated in the periphery of vision. White matter changes noted on neuroimaging may have also contributed to this vulnerability.
Epileptic activity most likely arising from a mid-tem-poral region surgical scar resulted in CVH in case C, representing one of the other CNS conditions (temporal lobe epilepsy) which are known to produce these symptoms. However, the symptoms of ‘flashing lights’ may also herald the recurrence of the AVM or development of scar tissue. The AVM is in a region closely related to the temporal portion of the optic radiation – again suggestive of a vulnerable substrate if this structure was impinged upon by the AVM or damaged by embolization or surgery when it was removed.
These three cases illustrate that anatomically disparate lesions can result in similar forms of CVH (Fig. 4) and that knowledge of the pathophysiology of CBS and PH aid in understanding how such different lesions may generate similar types visual symptoms.
Treatment of complex visual hallucinations
In general, management of CVH must be broad in its approach. An understanding of the possible pathologies that produce CVH allow for the correct attribution of neurobiological aetiology – for example, in a patient with impaired vision, not overlooking the possibility of a thalamic or brainstem infarct as an underlying pathology and thus ensuring that brain imaging is undertaken. The reassurance provided by the explanation of the organic basis of the symptoms is often helpful, and that symptoms often resolve spontaneously. Withdrawal of potential pro-hallucinogenic medications, if feasible, often forms the first step. In cases A and B patients' improvement may not be attributable to the use of atypical antipsychotics alone as the symptoms may have resolved spontaneously. As a result it may be appropriate in some cases showing spontaneous improvement of symptoms to not initiate pharmacotherapy. Evidence for pharmacological management is limited, although treatment response has been reported with atypical antipsychotics [63, 64] and anticonvulsant medication [65, 66], although the potential seizure threshold-lowering effect of antipsychotics may worsen symptoms in some cases of CVH. Only a brief period of antipsychotic treatment may be required, particularly when the causative process is thought to have resolved (such as in cases of transient ischemia or delirium). Correction of predisposing factors via interventions such as cataract surgery [61], laser photocoagulation of the retina [67] and the use of optical correcting devices [68] can be important additional considerations. Additionally, there is increasing evidence that controlling risk factors for cerebrovascular disease in elderly populations is important in preventing stroke and maintaining functional level [69, 70]. Visual hallucinations may therefore herald underlying cerebrovascular disease, and investigation and addressing risk factors such as hyperlipidaemia, hypertension and diabetes control may be equally important therapeutic aims. This does, however, need to be balanced against the potential risk of cerebrovascular events with atypical agents such as olanzapine and risperidone in the elders with significant cardiovascular risk factors [71].
Conclusions
Use of historical eponymous syndromes characterizes medicine, and ensures the work of medical pioneers lives on in current medical practice. However, in certain circumstances, the use of eponymous terms such as PH and CBS – particularly when definitions are fluid – may impair an accurate pathophysiological understanding of illness and result in barriers to appropriate disease taxonomy, investigation and treatment. An understanding of the underlying neuroanatomy and functional neurobiology of the structures where lesions are associated with CVH can aid both clinician and patient in understanding the underlying pathological processes responsible for this often highly distressing neuropsychiatric syndrome. The investigation of the processes involved in the generation of CVH can provide a structure on which the study of other neuropsychiatric symptoms such as auditory hallucinations may be modelled.
Footnotes
Acknowledgements
We thank Dr Levent Efe for his illustrations, funded by a grant from Organon Pharmaceuticals.