
Abstract
Hospitalization is one of the costliest interventions in schizophrenia and the other psychoses [1], and increases the burden associated with psychotic illness, not only for those with the disorder but for family, friends and carers, and for the health-care system. Some of the risks associated with hospitalization are relatively static and therefore are not amenable to change. These include such attributes as sex, age, age at onset and diagnosis. However, it is also possible to identify modifiable risk factors for hospitalization; their elucidation could help ensure that the mental health dollar is targeted at interventions likely to produce the greatest benefit.
Many of the findings published on risk factors for hospitalization in psychotic illness are similar to those reported for psychiatric hospitalization in general. Previous or frequent hospitalization [2–4], comorbid substance abuse [5–7] (but not [3]), aberrant behaviours (threatening others, very bizarre behaviour, attempted suicide) [3, 8] have been found to be risk factors for hospitalization in psychotic illness. In addition, high levels of symptomatology are implicated in many readmissions (see the review by Sullivan et al. [6]). Neuroleptic treatment compliance is protective [5, 6], with the risk of hospitalization increasing as the level of compliance decreases [9]. Earlier age at onset has been reported as a risk factor by some [10] but not all [3] researchers, while findings for an association between hospitalization on the one hand and younger age, being male and being single/never married are, again, inconsistent [11, 12], and may be confounded by age at onset [10]. Harrison et al. [13] found the inclusion of two-year course type improved a prognostic model based on predictors taken from the World Health Organization 10Country Study on schizophrenia [14] including, among others, gender, age at onset, marital status, length of illness and type of onset.
However, the targeted assessment of the independent impact of modifiable risk factors is an objective that has been poorly pursued in this area of research, even though the identification of risk factors that have potential for change has important clinical and policy implications for the development of interventions in psychotic illness. In this regard, the work of Sullivan et al. has been exceptional. Sullivan et al. modelled systematically five groups of modifiable risk factors, namely, health beliefs and behaviours, utilization of health-care services, home environment, barriers to care and satisfaction with life [6]. When they conducted a separate analysis of the best predictors, they found medication non-compliance, criticism/rejection of the patient and alcohol abuse were significantly associated with rehospitalization [6]. A second, hypothesis-driven analysis reported on the risk of rehospitalization associated with aberrant behaviours compared with clinical symptoms: highly disruptive or dangerous behaviours (e.g. very bizarre behaviour, threatening others, attempted suicide) were found to be particularly strong predictors of rehospitalization, and more powerful than clinical risk factors such as medication non-compliance and alcohol abuse [8].
Method
The present study of factors associated with hospitalization among people with psychoses is an analysis of a unique set of data collected as part of the Australian National Study of Low Prevalence (Psychotic) Disorders [15, 16]. This study used a two-phase design. In Phase 1, a 30-day census of psychosis was undertaken in predominantly urban catchment areas across four Australian States (Australian Capital Territory, Queensland, Victoria and Western Australia) including inpatient and outpatient services, private psychiatric and general medical practices, and contact points (e.g. soup kitchens, refuges, welfare centres) for people living in marginalized settings. The total number screened in Phase 1 was 5710, of whom 3800 were screen-positive. In Phase 2, a sample of 980 individuals was randomly selected (stratified by treatment setting) for interview from those who were screen-positive in Phase 1. Non-participation if selected for interview in Phase 2 was around 50%; reasons for not participating included refusal, loss to follow up and key worker recommendation against interview. To assess whether non-participation introduced a systematic bias into the data, the psychosis screening data and demographic data for nonparticipators were compared with data for the interviewed sample for the Western Australian catchment area. The profile for both populations was very similar indicating no significant differences in terms of demographics and lifetime symptomatology.
Survey data were collected by face-to-face interview using the specially developed survey assessment instrument, the Diagnostic Interview for Psychosis (DIP), a semistructured interview for use by trained mental health professionals [17]. All variables included in the analysis, other than diagnosis, alcohol abuse with psychopathology and cannabis abuse with psychopathology, were self-reported retrospective measures based on the 12 months before interview. The ICD-10 diagnoses were generated using the algorithm for the Operational Criteria for Psychosis [18] which drives the diagnostic module of the DIP. Alcohol abuse with psychopathology and cannabis abuse with psychopathology are lifetime measures included in the DIP; these were rated by a clinical interviewer with mental health experience on the basis of responses to a series of items, including items from the well-validated CAGE screen [19].
The present analysis includes interviewed people identified at inpatient (n = 262) and outpatient/ambulatory services (n = 425). Interviews took place, on average, 2 to 3 months after screening, with a median interval of 70 days for those identified as inpatients and 81 days for outpatients.
The analysis proceeded in three stages. The first stage was to build a base model of factors associated with hospitalization at the time of census using correlates of hospitalization in psychotic illness that were (i) theory-driven on the basis of reported findings, (ii) relatively static or difficult to change and (iii) available in the current dataset. The second stage was to add to the base model, in separate steps, sets of more or less dynamic patient characteristics to assess their impact on hospitalization, adjusting for the static variables in the base model. Three sets of dynamic characteristics were used, namely, service utilization, symptomatology and risky behaviours. In the final stage, a single model was fitted including the static variables in the base model and the significant dynamic variables from the other fitted models. In order to assess the stability and the validity of the models, the analyses were rerun on two further samples from the Study of Low Prevalence (Psychotic) Disorder: (i) a subsample of the main sample analysed here but including only those people who had spent 13 weeks or less in inpatient care in the previous year; and (ii) a non-overlapping sample of people who had been identified outside of mainstream inpatient and outpatient services, having been recruited through contacts with general practices, private psychiatric practices or who were not in contact with services at all – and who reportedly had not been in contact with mainstream inpatient and outpatient services in the previous 12 months. Logistic regression modelling was done using SPSS 10.0 (SPSS Inc., Chicago, IL, US).
Results
The characteristics of the study sample are given in Table 1. The percentage of men was similar for both groups, but the distribution of ages differed, with inpatients more likely to be in the age group of under 25 years. Inpatients were more likely than outpatients to have an ICD-10 diagnosis of schizophrenia (59.5% compared with 49.5%) while the outpatient sample was more likely to have a bipolar affective disorder, or some other form of non-organic psychosis. Overall, the inpatient group experienced a more chronic and disabling form of disorder. The symptom profile for both groups was similar in pattern but, for each symptom, the percentage of inpatients reporting the symptom was substantially higher than the percentage of outpatients reporting the same symptom. The course of disorder also differed between the groups with over a third (34.7%) of inpatients reporting a chronic, deteriorating course of disorder compared with 16.7% of outpatients. On the other hand, the outpatient group was more likely to use a variety of services including rehabilitation services and the services of general practitioners, and to have a case manager. On average, the inpatient group had poorer social and occupational functioning and, for the most part, were more likely to report risky behaviours such as cannabis abuse, self-harm, offending and victimization; only for alcohol abuse with psychopathology was the percentage of outpatients reporting abuse higher than the percentage of inpatients.
Separate models (OR, 95% CI)
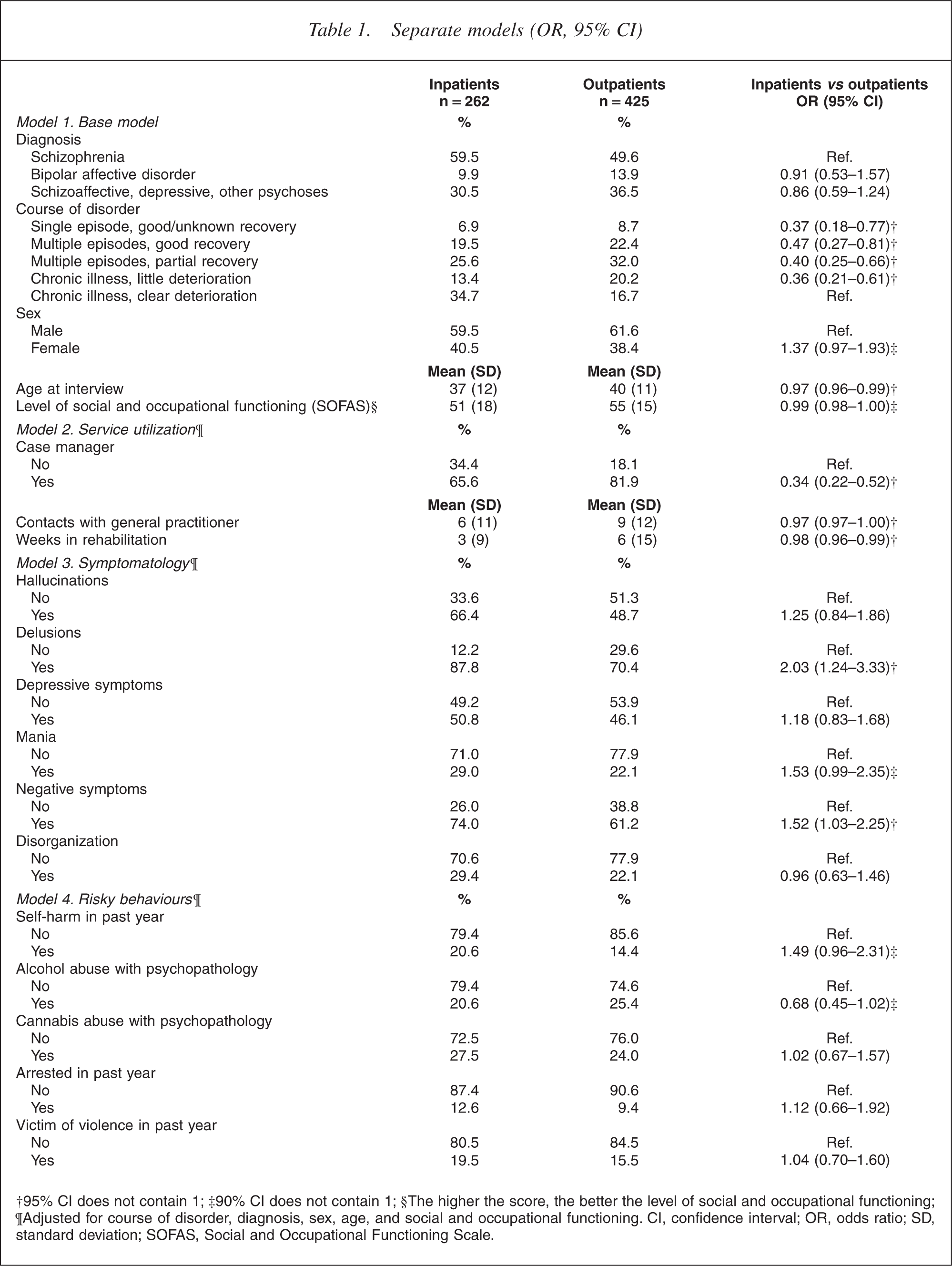
†95% CI does not contain 1; ‡90% CI does not contain 1; §The higher the score, the better the level of social and occupational functioning;¶Adjusted for course of disorder, diagnosis, sex, age, and social and occupational functioning. CI, con?dence interval; OR, odds ratio; SD, standard deviation; SOFAS, Social and Occupational Functioning Scale.
In stage one, a model (Model 1) was fitted regressing hospitalization status at the time of census (inpatient, outpatient) on the following variables:
ICD-10 diagnosis (schizophrenia; bipolar affective; schizoaffective, depressive and other psychoses); Course of disorder (single episode with good or unknown recovery; multiple episodes with good recovery; multiple episodes with partial recovery; chronic illness with little deterioration; chronic illness with clear deterioration); Sex; Age at interview; Level of social and occupational functioning as measured on the Social and Occupational Functioning Scale of the DSM-IV [20].
This model of static risks was determined after exploratory modelling of predictors identified in the literature. Course of disorder, used overtly as a measure of chronicity, also served as a proxy for previous hospitalization [12]. Age at interview was retained over either selfreported age at onset or duration of illness; age was a much stronger predictor, possibly because ageing is ameliorative [3]. Mode of disease onset was dropped as it did not contribute to the model, although others have found it to be predictive [13, 14].
When Model 1 was fitted, it was a significant improvement on the null model (change in scaled deviance 50.93, df = 9, p = 0.00) and a good fit overall (Hosmer and Lemeshow chi-squared statistic 4.34, df = 8, p = 0.83). The odds ratios and the 95% confidence intervals for each of the terms in the final model are displayed in Table 1. Course of disorder was significant at the 95% level with the odds of being hospitalized significantly reduced for each category of course compared with the reference category which was chronic illness with clear deterioration. Age at interview was also significant, with the odds of hospitalization dropping with increasing age. Sex and social and occupational functioning approached significance at the 95% level: the odds of a woman being hospitalized was 1.37 times the odds for a man, and the odds of being hospitalized dropped as social and occupational functioning rose. Diagnosis was not associated with hospitalization. Although adding diagnosis to the model did not significantly improve the fit of the model, it was retained on theoretical grounds. There was no interaction between sex and diagnosis and an interaction term was not included.
In stage two, three sets of dynamic and therefore potentially modifiable patient characteristics were fitted, in separate blocks, to the base model. This permitted assessment of each set of patient characteristics, adjusting for the static variables in the base model. The three blocks were:
Model 2. Base model + service utilization in the past year: having a case manager; number of contacts with a general practitioner; number of weeks in a rehabilitation program;
Model 3. Base model + symptomatology in the past year: hallucinations; delusions; depressive symptoms; mania; negative symptoms; and signs of disorganization;
Model 4. Base model + risky behaviours in the past year: selfharming behaviour; alcohol abuse with psychopathology; cannabis abuse with psychopathology; police arrest; victim of violence.
In Model 2, all three service utilization variables were significant at the 95% level. People who had a case manager had markedly reduced odds of being hospitalized in the census month compared with those without a case manager. The odds of being in inpatient care were also reduced significantly, but not as substantially, as the number of contacts with a general practitioner rose and as the number of weeks in rehabilitation programs increased.
In order to test whether State/Territory of residence affected the type of service utilization, the model was rerun including State. Having a case manager and number of weeks in a rehabilitation program, but not the number of visits to a general practitioner, remained significant. Course of disorder was no longer significant.
Model 3 added patient symptoms to the base model. The symptoms experienced in the past year that were most strongly associated with an increased odds of being hospitalized in the census month were delusions (OR = 2.03, CI = 1.24–3.33) and negative symptoms (OR = 1.52, CI = 1.03–2.25). There was a trend to an increased odds of hospitalization in people with hallucinations, depressive symptoms and mania; none of these symptoms were significant at the 95% level, and only mania was significant at the 90% level. In a variation to Model 3, hospitalization was regressed on the number of types of symptoms present; there was a cumulative effect with the odds of hospitalization increasing as the number of different symptom clusters present in the past year rose.
When risky behaviours were fitted to the base model, cannabis abuse with psychopathology, police arrest and being a victim of violence were not associated with hospitalization: their odds ratios were close to unity with confidence intervals extending well beyond both sides of unity. Self-harming behaviour and alcohol abuse with psychopathology were significant at the 90% level only. Those who had self-harmed had a 50% increased odds of hospitalization compared with those who had not, while there was a surprising, marked decrease in the odds of hospitalization for those abusing alcohol with psychopathology.
At stage three, a final model was fitted including all the static variables in the base model and those dynamic variables that were significant at either the 90% or the 95% level when fitted in the separated models. These variables were: having a case manager; number of contacts with a general practitioner; number of weeks in a rehabilitation program; delusions; mania; negative symptoms; self-harming behaviour; and alcohol abuse with psychopathology. The model was a significant improvement on the null model (change in scaled deviance 127.37, df = 20, p = 0.00) and a good fit overall (Hosmer and Lemeshow chi-squared statistic 2.66, df = 8, p = 0.95). The results for the dynamic variables were similar to those already reported in Table 1 for the separate models except that, in the full model, all these variables were significant at the more rigorous 95% level.
The data were re-analysed using a less chronic subsample of people who had spent 13 weeks or less in inpatient care in the previous year. In the service utilization model, having a case manager and attending rehabilitation, but not visits to a general practice, were negatively associated with hospitalization. In the risky behaviours model, none of the variables were significantly associated with hospitalization. In the symptomatology model, the variables significantly associated with hospitalization were the same as those reported for the full sample, namely, delusions and negative symptoms.
The model was then rerun using a non-overlapping sample of people who had been identified outside of mainstream inpatient and outpatient services (through general and private psychiatric practices or in marginalized circumstances, and reportedly had not had contact with inpatient and outpatient services in the previous 12 months). The outcome variable was any inpatient contact; this contact was presumed to have occurred after the census date. The variables associated with an inpatient admission were, for the service utilization model: case management; for the risky behaviours model: self-harm; and for the symptomatology model: the presence of mania and depressive symptoms in the past year. There was no significant effect for any other variable.
Discussion and conclusion
The current analysis indicates how the risk of hospitalization in a census period among people with psychotic disorders who are using mainstream services may be modelled initially using relatively static variables, namely, course of illness, age, social and occupational functioning, sex and diagnosis. Within this base model, diagnosis was not significant, contrary to some expectations and, although women were more likely than men to have been hospitalized at the time of census, this was only significant at the 90% level, as was social and occupational functioning.
However, a number of dynamic variables may modify a person's risk of hospitalization. All three service utilization variables entered into the model were significant: as the use of services rose, and the risk of hospitalization in the census month fell. The small but significantly reduced odds of hospitalization associated with increased participation in rehabilitation and increased contact with general practitioners point to the important roles played by these services in reducing hospitalization. However, being assigned a case manager was particularly critical. For those with a case manager, the odds of hospitalization was 0.34 (CI = 0.22–0.52); put differently, the odds of hospitalization almost tripled (OR = 2.95, CI = 1.94– 4.47) for those without a case manager. Correcting for a common outcome, the estimated true relative risk is 1.86 (CI = 1.51–2.18) [21]. If the lack of case management is causal, then 46% of hospitalizations of people in mainstream services in a census month may be attributable to not having a case manager, with a population attributable fraction of 17% [22].
The impact of State/Territory of residence on the service utilization model may reflect real differences in pathways to care, or differences in the catchment areas selected for inclusion in the study at the point of census. The finding that course of disorder was no longer significant when State was included in the model suggests that the illness profile of people within the catchment areas is the main source of the differences found. However, it is notable that, even with State in the model, having a case manager and attending a rehabilitation program remained significant negative predictors of hospitalization.
Three symptom clusters in particular were associated with an increased odds of hospitalization, making symptom reduction an important consideration in risk modification. The odds of hospitalization doubled for people experiencing delusions, and increased by 50% each for people with negative symptoms and with symptoms of mania. There was also a trend towards an increased risk for people experiencing hallucinations and depressive symptoms.
While the service utilization and symptomatology models were both significant improvements on the base model (change in deviance 38.20, df = 3, p = 0.000; change in deviance 28.64, df = 6, p = 0.000, respectively), the risky behaviours model did not improve the fit of the base model and was difficult to interpret. Attempted self-harm [3] and antisocial behaviours [8] have been found to be predictive in other studies. In our study, attempted self-harm was not a strong predictor, and criminal offending was not at all associated with hospitalization. In contrast to other studies, we also found that the odds of hospitalization was reduced in the presence of alcohol abuse with psychopathology. Furthermore, for those who had spent any time in an inpatient facility in the 12 months before interview, the mean length of stay was higher for those who were not abusing alcohol; this held true for both inpatients and outpatients when examined separately. This result is difficult to interpret in the absence of longitudinal data to explore the temporal sequence of related events. It conflicts with findings by Gerding et al. [7] that people with schizophrenia who are actively abusing alcohol are at higher risk for hospital readmission and have a longer length of stay if admitted, although Gerding et al.'s study was limited to a small sample of neuroleptic-compliant patients with schizophrenia. One interpretation may be that hospitalization itself results in reduced alcohol abuse rather than that alcohol abuse is protective. More generally, the ambiguous results emerging from this model may be due to the heterogeneous nature of risky behaviours and complex interactions that are not reflected in the current model; this is supported by the poor fit of the model.
The Low Prevalence Disorders Survey provided a strong epidemiological framework within which to examine factors associated with hospitalization in psychotic illness, including the capacity to sample across the range of treatment services within a census month. Nonetheless, the present analysis faced several limitations. First, the survey data are essentially cross-sectional. Consequently, we have been able to determine correlates of hospitalization, but longitudinal data are needed to establish the temporal and causal relationships between the factors fitted and hospitalization. Nonetheless, both the short average time span between screening and interview, as well as the specific coverage by the survey instrument of the 12 months before interview, lend some confidence to the models presented here. A second limitation is that modelling was restricted to variables collected as part of the Study of Low Prevalence Disorders, and did not include pertinent modifiable risk factors such as neuroleptic treatment compliance when collecting data on medication use and side-effects [23]. A third limitation is the potential for various forms of bias to affect the findings. For example, the use of self-reported data may introduce some element of recall bias, although the use of clinical interviewers to administer the survey, and the inclusion of mechanisms in the design of the survey protocols to minimize invalid statements [16] served to reduce the impact of recall bias. Study non-response is another form of bias that may affect results; here, the similarity between the profiles for respondents and non-respondents suggests that study non-response is not a factor.
The rerun of the models using different survey samples supports the reliability of the findings and their stability across populations. To explore the possibility that chronically hospitalized people were less likely to have access to case management rather than that case management averted hospitalization, analyses were rerun on a less chronic subsample of the main sample, as well as on a non-overlapping sample of people who were not in contact with either inpatient or outpatient services at the time of census. These reanalyses produced similar conclusions to the main analysis. Symptoms were predictive for all samples, although the specific symptoms varied by sample. The risky behaviours model remained difficult to interpret, with no significant associations other than selfharm in the non-overlapping sample. The trend for a negative association between alcohol abuse with psychopathology and hospitalization was apparent in the less chronic subsample, but was not found in the nonoverlapping sample not using mainstream services. It appears that the model developed on the basis of available data has not captured the complexity of risky behaviours as predictors of hospitalization. Finally, in all samples, case management remained a strong negative predictor of hospitalization. The results from the model with the non-overlapping sample not using mainstream services at the time of census in particular suggest that nature of the significant relationship between case management and hospitalization may be causal, rather than merely associative. However, these must remain tentative assertions in the absence of prospective, longitudinal data.
In sum, our findings point to a base model of static risks in which course of disorder and age, but not type of psychosis, are significantly associated with hospitalization. When dynamic risk variables are included in the model then, among symptoms, delusions, negative symptoms and mania significantly increase the odds of hospitalization; service utilization reduces the odds; and risky behaviours are difficult to interpret. Despite the limitations of the current model, it highlights the impact of dynamic factors over and above static factors in the risk for hospitalization in psychotic illness. As such, it points to important areas for resourcing in the management of psychotic disorders.
In particular, case management emerges as a strong negative correlate of inpatient status in psychotic illness. Within the Australian Study of Low Prevalence Disorders, a case manager was described as a mental health worker, usually a nurse, who sees the patient on a regular basis and who coordinates the care provided on a community basis [16]. However, that study was not able to collect detailed information on the style of case management. Indications are that, to be effective, case management must move beyond the perfunctory provision of an administrative interface between the various sectors and key workers involved in the care of a patient and the patient, in favour of an assertive and responsive model.
Finally, there are occasions where hospitalization is an appropriate response to a psychotic episode and at least one study has demonstrated the potential for community care programs directed at vulnerable psychiatric patients to increase readmission rates [24]. The survey data do not distinguish between appropriate and inappropriate hospitalization. The findings suggest, however, that creating strong and individualized community-based supports for people with psychoses is vital to the provision of consistent care and the maintenance of equilibrium. Hospitalization remains a proper intervention at the times of individual crisis, but should not be a result of a potentially avertable deterioration precipitated by a crisis in community support.
Footnotes
Acknowledgements
The present paper is based on data collected in the framework of the Collaborative Study on Low-Prevalence (Psychotic) Disorders, an epidemiological and clinical investigation which is part of the National Survey of Mental Health and Wellbeing, Australia 1997– 1998. The study was funded by the Commonwealth Department of Health and Aged Care, the Australian Capital Territory Department of Health and Community Care and the Psychiatric Epidemiology Research Centre, Australian National University.
The authors note, with sadness, the recent death of their co-author, Ailsa Korten, and wish to acknowledge the important contribution she has made to Australian and international psychiatric research over many years. Ailsa was an outstanding psychiatric epidemiologist and statistician, with over 120 publications, and was represented in the top 1% of researchers in the Category of Psychiatry/Psychology on the ISI Web of Science. She was a committed supporter of the Australasian Society for Psychiatric Research (and ACT representative for many years), a humanist, an active sportwoman (a great skier), a wonderful colleague, and a good and kind friend. Ailsa died peacefully at her property Half Moon near Braidwood, ACT on 15 December 2005 after battling motor neurone disease. She will be missed by many.