
Abstract
This paper sets out to critically evaluate reports from the Australian-wide National Survey of Mental Health and Wellbeing of very low rates of ICD-10 anxiety and depressive disorders in community resident older Australians. Data from the National Survey, which relied on the Composite International Diagnostic Interview (CIDI) were re-computed and re-analysed to address concerns about population sampling, interview response patterns and alternate measures of mental health. Rates of anxiety and depressive disorders fell to low levels after 65 years and continued to fall thereafter. This is at odds with findings from gerontological surveys that used assessment tools better suited to frail older people. Scores on mental health scales, together with diagnostic algorithms that obviated CIDI skip patterns, showed much less change in mental wellbeing across generations. It is argued that sampling and case ascertainment bias combined to reduce rates of anxiety and depression in very old people, especially when adjustments are made for the high morbidity levels encountered in aged residential facilities. Functional mental disorders almost certainly rise in frequency in advanced old age, often in conjunction with dementia.
A national mental health survey commissioned in 1997 by the Australian Commonwealth Government reported that older, community resident Australians were less prone than younger adults to substance abuse, anxiety disorders and depression [1, 2].
Figure 1 shows that alcohol use disorders peaked in young adulthood and fell steadily thereafter. Anxiety and depressive disorders both peaked in middle life and then declined to such an extent that only 4.5% of people aged 65+ years met ICD-10 criteria for an anxiety disorder and only 1.1% met criteria for major depression or dysthymia.
12-month prevalence of ICD-10 diagnoses by age. (——) alcohol, (——) anxiety, (–––) depression.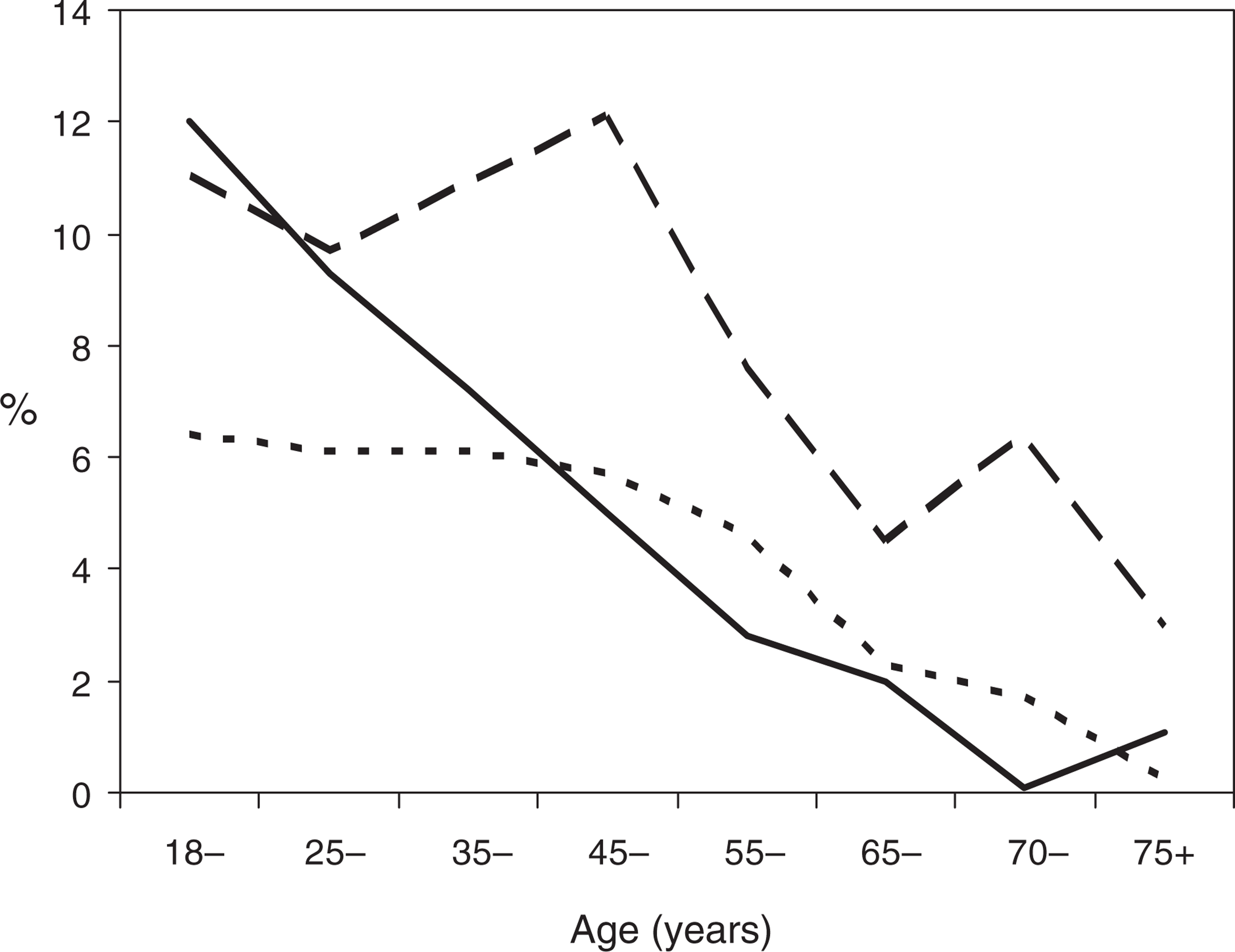
These findings have been disputed on the grounds that: (i) aged care facilities were excluded from the survey despite robust evidence of high rates of anxiety and depression in these settings; (ii) mentally disordered older people decline to participate in surveys or are shielded by carers; (iii) complex diagnostic interviews place an undue burden on cognitively frail respondents; (iv) older people falsely attribute anxiety and depression to medical illness; and (v) diagnostic glossaries like ICD-10 fail to capture important psychological morbidity [3, 4].
If these concerns are valid, and rates of mental disorder have been seriously underestimated, older people and their carers will be deprived of their proper share of psychiatric services and social supports. It is important therefore to subject these questions to rigorous, systematic analysis.
This paper addresses each issue in turn with the aim of illuminating points of importance to older people. All data were taken from a Confidentialised Unit Record File supplied by the Australian Bureau of Statistics. Novel information presented here includes rates of mental disorder in very old age groups (70–74, 75+ years); comparisons with other adult and gerontological surveys; aged respondents' sociodemographic and cognitive status; their patterns of symptom endorsement and attribution, and their performance on mental health scales.
ICD-10 is preferred here to DSM-IV, in line with previous reports, except when drawing comparisons with North American studies. The two systems are not directly comparable. After age 75+ years, for example, ICD-10 detected more anxiety disorders than DSM-IV (3.0% vs 1.2%) but fewer cases of major depression and dysthymia (0.2% vs 1.1%). This is not a major issue, however, as 12-month prevalence rates fell steeply from middle age onwards in both glossaries.
The National Survey
The National Survey of Mental Health and Wellbeing mapped (i) the annual and current prevalence of mental disorder in Australia; (ii) the functional disability resulting from mental disorder; and (iii) the perceived need for medical, psychological and social services, thus setting a benchmark against which future activity can be compared and evaluated [2].
The Australian Bureau of Statistics was commissioned to survey a representative sample of residents of private dwellings throughout the country. Non-private dwellings (hospitals, aged residential facilities, hotels and prisons) were excluded. One person aged 18+ years from each of 13 600 eligible residences was invited to participate, of whom 78% agreed to be interviewed giving a total of 10 600 respondents. Weightings were applied later to ensure representation, at least with respect to age, gender and area of residence, of the total adult Australian population at that time.
The lay-administered assessment covered personal characteristics, physical health, mental disorder and its associated disability, health service use for a mental health problem, and the perceived need for health services. ICD-10 and DSM-IV diagnoses were derived by computer algorithm from the Composite International Diagnostic Interview (CIDI) which ascertains symptoms and their impact on day-to-day activities [5].
Respondents also completed three mental health scales: the General Health Questionnaire (GHQ-12) [6]; the neuroticism scale of the Eysenck Personality Questionnaire [7], and the Kessler Psychological Distress Scale (K-10) [8]. A cognitive scale, the Folstein Minimental State Examination (MMSE), was put to respondents aged 65+ years [9]. Those who scored 18 points or less out of 30 were not interviewed further.
Other studies
Whole population surveys
Table 1 lists the prevalence of anxiety disorders and major depression in the two other large mental health surveys of representative adult and aged populations based on single-stage structured interviews, computerized diagnostic algorithms and DSM criteria [10–12]. Study methods varied, as did rates of mental disorder. This is not surprising: ‘caseness’ is shaped largely by research methods and diagnostic rules [13, 14]. It is striking nonetheless that rates of both anxiety and major depression, however defined, fell to their lowest points after 65 years. Similar findings emerged in two earlier, less structured surveys by Swedish and Canadian psychiatrists [15, 16] and in a meta-analysis of 11 community surveys in which rates of depression dropped in both sexes from age 20 years onwards [17]. The prediction that mental disorder peaks in advanced old age as a result of physical illness, disability and dependency was not borne out.
Prevalence of major depression and anxiety disorders in US, Canadian and Australian community surveys of adult and aged subjects
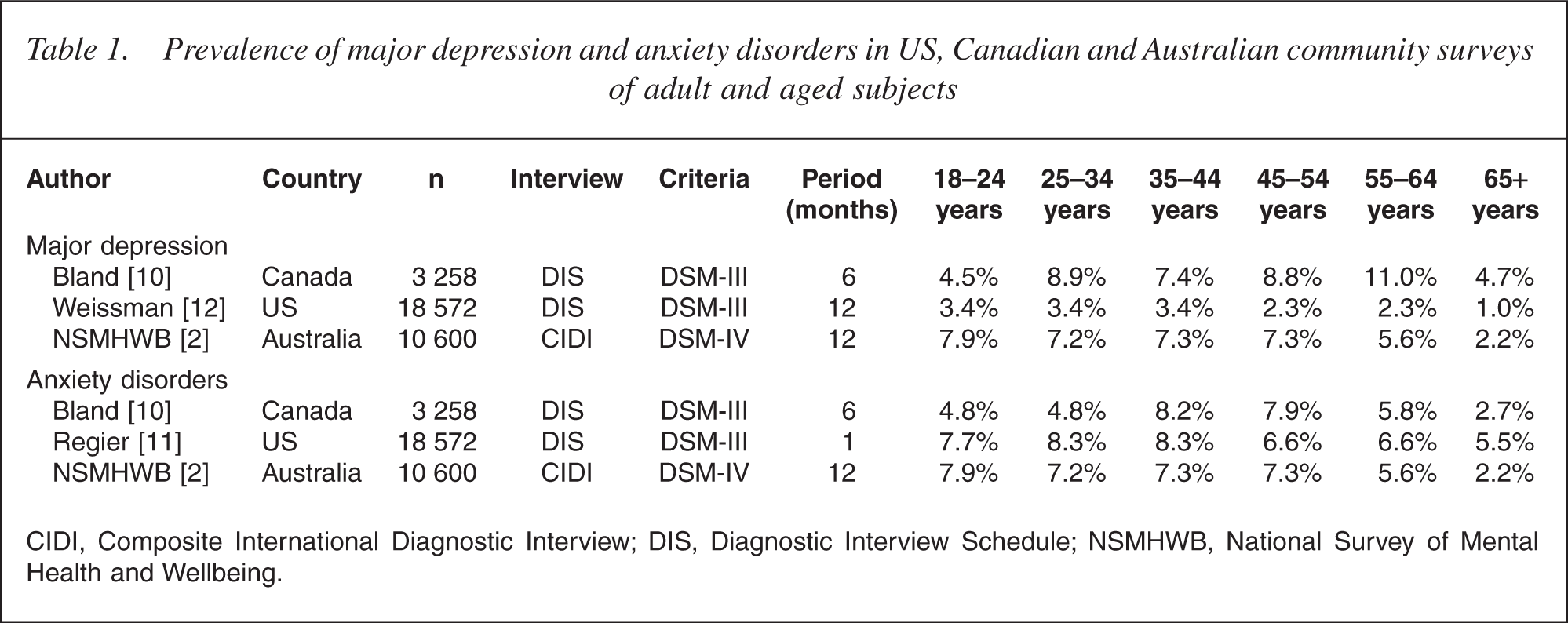
CIDI, Composite International Diagnostic Interview; DIS, Diagnostic Interview Schedule; NSMHWB, National Survey of Mental Health and Wellbeing.
Gerontological surveys
Surveys restricted to older age groups paint a different picture however. In four similarly structured gerontological studies, rates of DSM major depression rose from age 65 years onwards [13,18–20] (Table 2), in marked contrast to the Australian study in which alcohol and anxiety disorders rose fractionally just in very old men (Fig. 1). Nursing home residents were largely or completely excluded from all reports.
Prevalence of major depression in older age groups
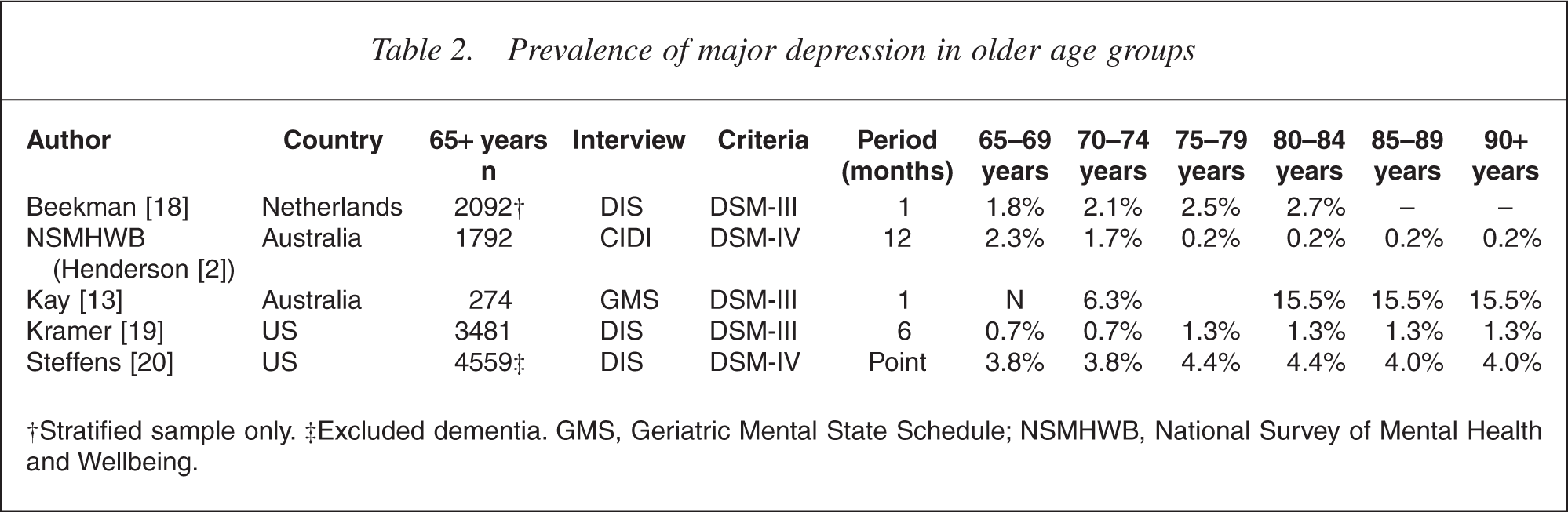
†Stratified sample only. ‡Excluded dementia. GMS, Geriatric Mental State Schedule; NSMHWB, National Survey of Mental Health and Wellbeing.
Incidence surveys
The prevalence of a mental disorder (the number of cases within a single period) is simpler to measure than incidence (the number of newly arising cases) but is harder to interpret. It is conceivable, for instance, that prevalence falls with age, despite a constant or elevated incidence, if older ‘cases’ remit faster or die sooner. Few incidence surveys have been conducted and their findings must be interpreted cautiously: the number of new cases is typically small and confidence intervals are wide. The incidence of depression fell steadily from mid-life onwards in the 15-year Lundby study [21] but rose from 70 to 80+ years in a gerontological study, also from Sweden [22]. In a North American study, the incidence of major depression and panic disorder fell with age (although rates varied between centres) while rates of phobic disorder rose a little in older men and obsessive compulsive disorder rose substantially in older women [23].
Specific issues
This section explores ways in which population sampling and case ascertainment techniques conceivably underestimated psychopathology in aged participants.
Aged residential facilities
The Australian survey excluded aged care facilities because of their non-random geographical distribution and the large numbers of residents with dementia. Diagnosing mental disorder in residential settings is difficult and the survey lacked the resources to employ skilled psychiatrists and psychologists with access to medical records and family informants.
In studies of nursing homes in Canberra, Hobart, Melbourne and Sydney, roughly 10% of assessable nursing home residents met ICD or DSM criteria for depressive psychosis or major depression [14,24–26] and 4% in Sydney had either generalized anxiety disorder or panic disorder [27]. Rates of major depression were even higher in six similar US and UK studies (range 6–30%, mean 21%) [28].
In 2001, 1.3% of Australians aged 65–74 years lived in ‘cared accommodation’. This proportion rose to 7.5%, 30.2% and 56.1% for persons aged 75–84, 85–94 and 95+ years respectively [29]. If 10% of all residents had major depression, in line with other studies, this by itself adds 3.0% to figures for age-group 85–94 years and 5.6% after 95+ years. Similarly, if 4% of residents had an anxiety disorder, this adds 1.2% and 2.2% respectively to rates for people aged 85–94 and 95+ years.
Non-responders
Across the whole of Australia, interviews were completed with 78% of selected individuals, an acceptable rate by current standards [2]. For privacy reasons, nothing is known of non-responders. It is not clear, therefore, if older people were more or less likely to participate than younger ones.
In a large US study, fit older people proved easier to contact than young, employed, urban-resident men [30] but the reverse applied in Canberra, Australia, where response rates fell from 70% in younger adults (18– 59 years) to 54% thereafter [31]. In gerontological surveys, non-response rose with advanced age and cognitive impairment [32–34]. This is expected. When faced with a lengthy, complex interview, some ill, deaf or confused old people will either decline to participate or be shielded by relatives.
In the Australian survey, participants looked at first glance to be highly representative of their cohort [35]. More lived alone and fewer than average came from non-English-speaking backgrounds but most drew government pensions and only 27% had completed high school (Table 3). As performance on cognitive tests like the MMSE is shaped by age, education and socioeconomic status, their scores should logically have been low [36, 37].
Social characteristics of survey respondents compared with Australian population (all aged 65+ years)
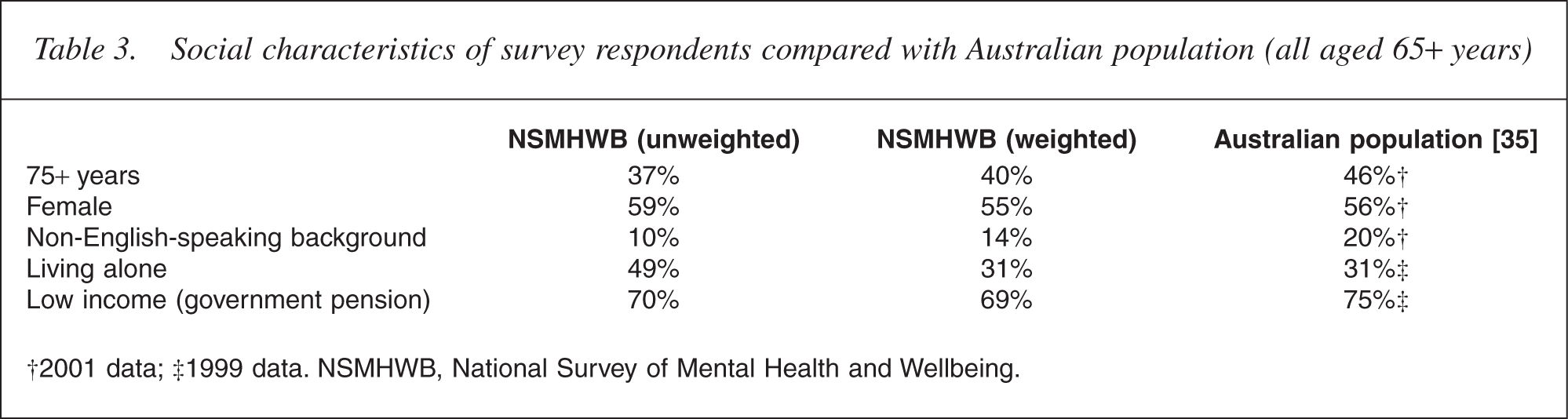
†2001 data; ‡1999 data. NSMHWB, National Survey of Mental Health and Wellbeing.
Cognitive status
The MMSE works adequately as a screen for dementia in clinical and research practice: a score of 23 or less out of 30 typically denotes dementia and a score of 17 or less denotes severe dementia [9, 37]. In the oldest Australian age band (75+ years), only 10.6% scored 23 points or less. The true rate was almost certainly much higher. As it happens, the author has access to the database of a large, genuinely representative sample of elderly UK general practice patients in which 29.6% of 75+ years, community-resident respondents scored in the same range [37]. Australian respondents were clearly atypical (Fig. 2).
The Folstein Mini-mental State Examination scores of community residents aged 75+ years in (——) Australian and (— —) UK surveys.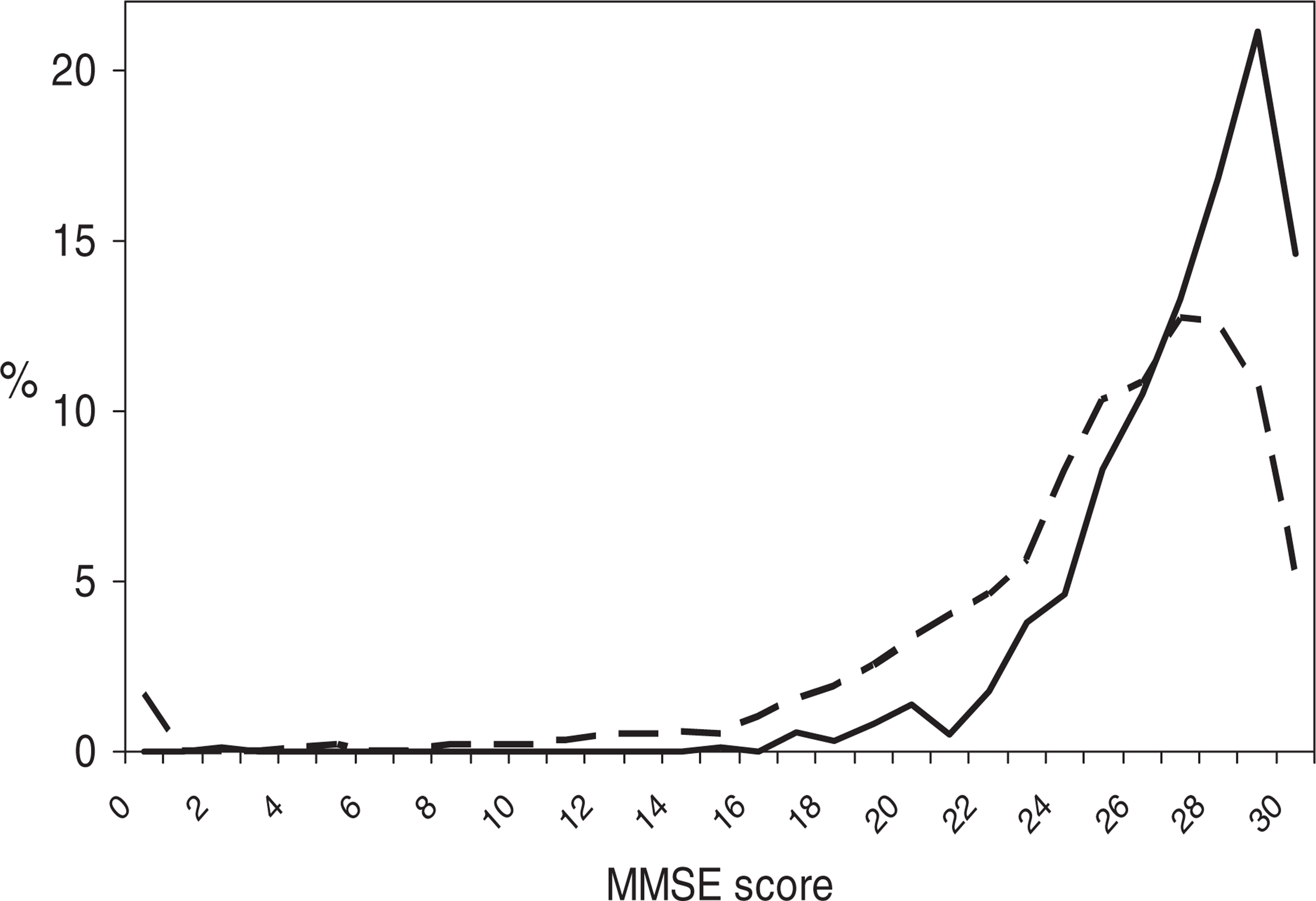
This made it important to check if persons with low MMSE scores were more vulnerable to mental disorder. There were too few Australians scoring between 18 and 23 points (n = 121) to draw valid conclusions. Instead, MMSE scores were bisected at the median for this group of 27/28 points. Low scorers (0–27 points) had higher rates of both ICD-10 anxiety disorders (3.2% vs 2.8%) and depressive disorders (0.5% vs 0%).
There is evidence of a modest link between depressive symptoms on the one hand and low scores on cognitive tests on the other in aged community populations [14,38]–[40]. The evidence is less clear, however, with respect to clinical diagnoses. In a survey of Swedish people aged 85 years, rates of major depression, dysthymia and anxiety disorders peaked in those with mild dementia [41]. In another Swedish study, people known to have dementia were at increased risk of major depression [42]. By contrast, no association between major depression and dementia emerged in Australian and US surveys [13, 36].
Symptom endorsement
To save time, CIDI checks for ‘core’ symptoms of substance abuse, anxiety and depression and probes further only if these symptoms are endorsed. The two core depression questions are: ‘In the past 12 months, have you had two weeks or longer when nearly every day you felt sad, empty or depressed for most of the day?, and: Have you had two weeks or longer when you lost interest in most things like work, hobbies and other things you usually enjoyed?’. A negative response to both items prompts a skip to the next section.
Some writers argue that older people are prone to ‘nondysphoric depression’, a condition that presents with vegetative and cognitive complaints rather than dysphoria [43]. If this is true, core questions relating to sadness and anhedonia will miss genuine melancholia presenting just with anorexia, insomnia, somatization, forgetfulness and the like.
Only a minority of Australian respondents endorsed the two core depressive symptoms, sadness (13%) and lost interest (14.1%) and were questioned further. Most were not. Nothing is known therefore of other active CIDI symptoms but, fortunately, most non-core symptoms were addressed in either the K-10 or GHQ-12 scales that all respondents completed. This made it possible to improvise ICD-10-type diagnoses of major depressive episode that help shed light on missing elements.
The K-10 scale checks if mental symptoms have been present in the last 4 weeks ‘for all, most, some, a little or none of the time’. The GHQ-12, by contrast, asks if symptoms have been present in recent weeks ‘much more, rather more or no more than usual’ or ‘not at all’. For the purposes of this exercise, relevant K-10 items (mood, energy, self-esteem, confidence and motor activity) were dichotomized arbitrarily to ‘all/most’ versus ‘some/little/none’ responses. The GHQ-12 items (enjoyment, concentration, sleep) were dichotomized to ‘much more’ versus ‘rather more/same/less’. When diagnoses were manufactured using ICD-10 rules (two core plus any two non-core symptoms), a distinct picture emerged. In contrast to CIDI's ICD-10 diagnoses which fell steeply with age from mid-life onwards (Fig. 1), improvised diagnoses were much more evenly distributed with a slight fall in late middle age and a later peak and trough in the eighth decade (Fig. 3).
(— —) The Composite International Diagnostic Interview and (——) improvised ICD-10 diagnoses of major depression by age.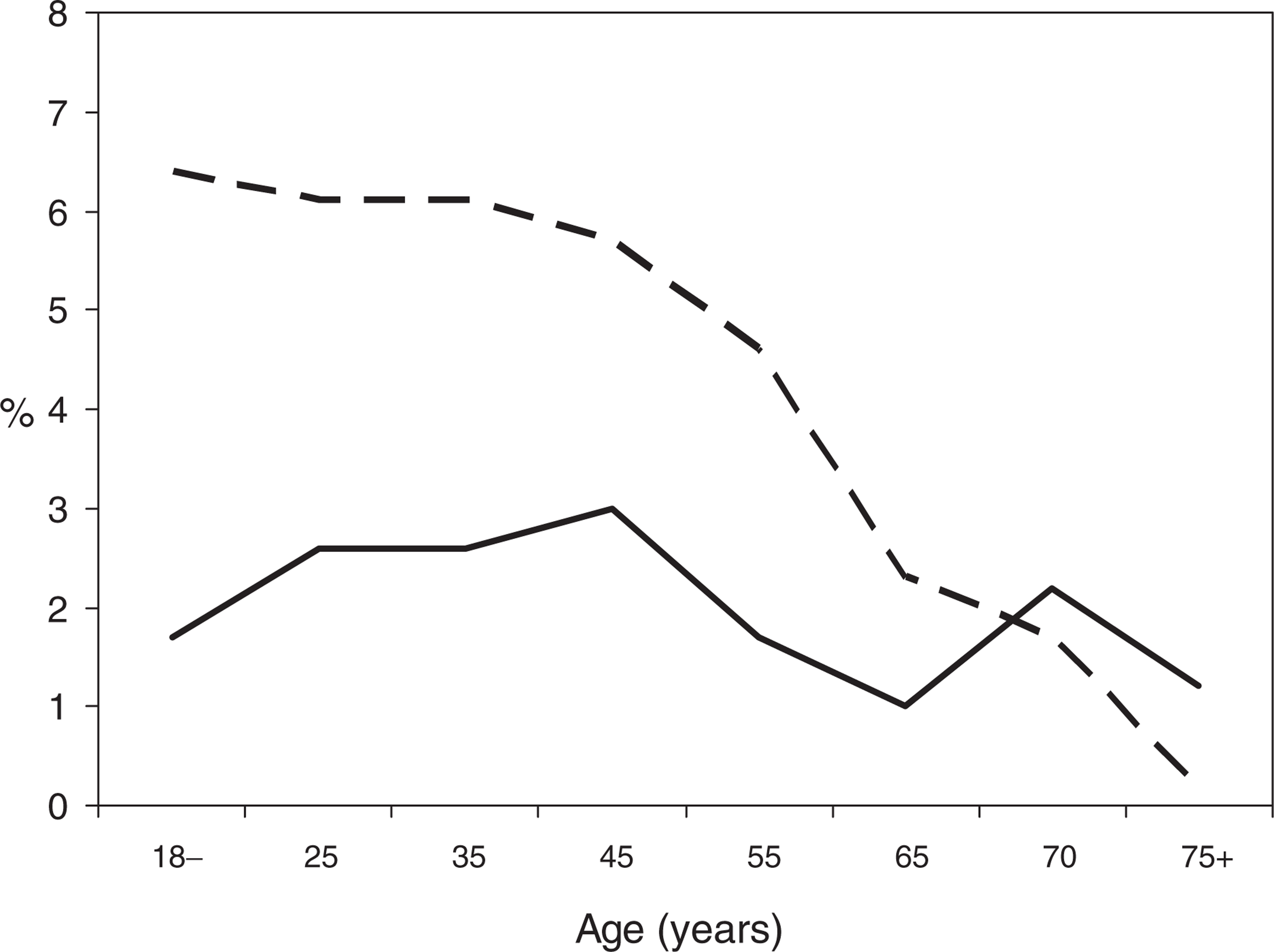
Symptom attribution
Hasin and Link found that North American older people more commonly attributed depressive symptoms to physical illness [44]. This makes sense. The link between depression, physical illness and disability is complex [45]. Illness can precipitate depression; depression in turn can trigger new or heightened somatic complaints [46], and symptoms like fatigue may stem from normal physical changes [47].
It is important to determine if older respondents in the National Survey attributed core affective symptoms to physical illness or injury as, had they done so, the CIDI algorithm would have discounted their complaints in the absence of pointers to the contrary (e.g. a diagnosis of depression by a doctor). There is some evidence that this occurred. Only 6.2% of reports of recent sadness by respondents aged 18–64 years were attributed to physical illness or injury. This figure rose to 11.4% for people aged 65+ years. Equivalent figures for complaints of lost interest were 10.8% and 23.5% respectively.
Some of these attributions were almost certainly incorrect. However, even if all complaints were actually due to depression, it would make little difference to final figures as twice as many younger respondents reported recent sadness and lost interest than older ones and virtually all such reports were accepted by CIDI as ‘possible psychiatric symptoms’ regardless of age. Thus, CIDI accepted 93% and 87% reports of sadness and lost interest, respectively, in the 18- to 64-year age band compared with 89% and 71%, respectively, after 65 years. Similar findings emerged from a re-analysis of North American data [48]. The reason is that many diagnoses had been confirmed by doctors' diagnoses or treatments in all age groups.
Mental health scales
Psychiatric glossaries divide respondents into ‘cases’ of mental disorder and ‘non-cases’. The results are clinically useful but somewhat arbitrary as ‘caseness’ can hinge on responses to a single question. Continuous measures of mental health, by contrast, shed light on the whole community including ‘subthreshold cases’, that is, respondents who fail to meet criteria for diagnosis but might still be disabled and worthy of attention [49].
The K-10 and GHQ-12 both tap general mental wellbeing with items concerning mood, energy, self-esteem, etc. but they are different enough to warrant inclusion here. The K-10 scale, for example, focuses on symptom persistence while GHQ-12 focuses on symptom severity (see above). Note that high K-10 scores denote good mental health in contrast to GHQ-12 which follows the standard pattern.
Both scales show a reduction in distress with age but differences across the lifespan are actually trivial. Mean GHQ-12 scores fell from a peak of 1.05 (age 45– 54 years) to a low of 0.56 (age 65–69 years) out of maximum of 12 points. Similarly, mean K-10 scores ranged only from 45.1 (age 18–24 years) to 46.9 (age 65– 69 years) where 50 represents ideal health.
Previous surveys of adult and aged community groups using a mental health scale reported similar reductions in scores with age [31, 50, 51]. By contrast, gerontological surveys showed either no change with age [39] or a modest increase [38, 40,52–54].
Discussion
The National Survey has met its objective of generating interest in the prevalence and consequences of mental disorder in Australia. Its findings are shaping public policy and it is important to subject them to critical analysis as errors of fact or interpretation could have onerous consequences.
Comparison with other surveys
The finding that anxiety, depressive and alcoholrelated diagnoses decline with age is not unexpected. Similar observations have emerged in Canada, the US and Sweden and arguments have been marshaled by way of explanation: (i) older people were reared in tough times and cope better with adversity; (ii) their coping mechanisms have been honed over decades; (iii) they have greater emotional stability; and (iv) they experience fewer daily hassles [55].
While these points have merit, some questions remain. Why is it, for example, that anxiety and depressive diagnoses fell from age 65 years onwards to a degree not seen in similarly crafted gerontological surveys? At 75+ years, only 3% of respondents met ICD-10 criteria for any sort of anxiety disorder and only 0.4% met criteria for major depression. DSM-IV rates were not much different at 1.2% and 1.1% respectively.
This steep decline in morbidity is at odds too with the relatively stable profile of specially improvised ICD-10 diagnoses and K-10 and GHQ-12 scores, suggesting that CIDI, which places great reliance on small numbers of probe questions, exaggerates differences between the generations. Tools that draw on a larger body of data show a more attenuated picture.
Population sampling
The Composite International Diagnostic Interview is too complex an instrument to apply in nursing homes where 80% of residents are cognitively impaired [26]. While the decision to exclude aged residential facilities was reasonable, the implications have not been properly grasped. As admission to residential care rises steeply with age, the effect of excluding such facilities is small for the young-old but much greater for the old-old [56]. If 10% of nursing home residents aged 75+ years have major depression, this alone adds another 1–2% to the 0.4% reported previously for this age band.
These figures are almost certainly conservative as even nursing home researchers exclude residents too confused to complete their scales or questionnaires. In a recent Australian study that collected information on new nursing home residents regardless of cognitive capacity, 25% met strict DSM-IV criteria for major depression (Martyn K: personal communication, 2006). Most depressed residents were also confused and would have been missed using standard approaches. It is likely therefore that anxiety and depressive disorders are actually much commoner in advanced old age than the National Survey suggests.
Case ascertainment
While survey respondents were otherwise remarkably representative of the Australian population, their MMSE scores were implausibly high. Cognitively impaired older people were almost certainly sidelined (quite apart from those with very low scores whose interviews were terminated) but it is impossible to deduce how this happened: we know nothing of the characteristics of people who preferred not to participate or were shielded by families or even by interviewers.
The National Survey asked about the nature, duration and overlap of multiple psychological symptoms in the previous 1 year interspersed with many dozens of questions about personal and social circumstances, physical health and service use. Older respondents presented a special challenge: they tire faster, cope less well with lengthy interviews and have a limited working memory [57–59]. Some are also deaf, visually impaired and physically frail. By contrast, gerontological surveys, which actively recruit frail, confused old people, tend to focus on current symptoms using scales or specially crafted schedules like the Geriatric Mental State Examination [60]. Perhaps not surprisingly, these ‘user-friendly’ studies generate rates of anxiety and depression that either remain steady or trend upwards in advanced old age.
The K-10 and GHQ-12 scales, and the ICD-10 ‘diagnoses’ derived from them, showed only trivial changes in subjective mental health with age. Both scales have been validated extensively in clinical and community populations: the more abnormal the score, the likelier it is that a clinician will diagnose a mental disorder but the fit is imperfect. But neither is it perfect for CIDI or its North American equivalent, the Diagnostic Interview Schedule. The agreement between the Diagnostic Interview Schedule and clinical diagnoses of major depression ranged from a kappa value of 0.25 in one study [61] to 0.70 in another [62] where 1.0 represents perfect concordance. Scales, structured interviews and even diagnostic glossaries represent approximations of what an experienced clinician deduces following an exhaustive assessment. Scales are useful nonetheless and were especially informative here because they were completed by all National Survey respondents.
Summary
The National Survey's rates of ICD-10 and DSM-IV mental disorder in very old community residents were so much lower than those in gerontological studies using identical or similar criteria that their validity must be questioned. Mental health might certainly improve with age and there are good reasons for it to do so [55]. Mental health scales, and the improvised ICD-10 diagnoses created for this paper, confirm a tendency to lesser anxiety and depression with age – but the trend is subtle, not extreme.
When allowance is made for the very high levels of morbidity seen in aged residential facilities, this trend might reverse in direction, at least in very old age groups. One recently mooted idea is that depression has two peaks of onset, one in the very young and another in the oldest old [63]. The former peak is well described: the latter warrants further exploration by means of prospective studies of anxiety and depression in the frailest, most dependent aged, many of whom also have dementia.
The CIDI assessment taxes the capacity of frail older community residents who look to have been sidelined from the National Survey. This is an important issue as the oldest old (80+ years) are growing faster numerically than other age bands [29] and assessment protocols should be as age-inclusive as possible. Mental health scales which take a few minutes to complete and focus on recent weeks could play an important role here.
The Federal Government has devoted huge resources to dementia care, both in the community and residential facilities. If it is true that the National Survey has underestimated rates of anxiety and depression in very old age groups, these conditions will warrant more attention too.
Footnotes
Acknowledgements
I thank Professor Gavin Andrews, Dr Ruth Parslow, Associate Professor Jane Pirkis, Dr Tim Slade and Associate Professor John Snowdon for helpful comments on an earlier draft of this paper.