
Abstract

The press announcement following the February Council of Australian Governments meeting included a determination to improve mental health services.
Issakidis and Andrews [1] analysed the 1997 National Survey of Mental Health and Well-being and showed that while eight out of 10 people with a mental disorder consult a general practitioner during the year, in less than a third was the mental disorder the focus of a consultation. A few patients sought help directly from specialist mental health services but, even so, only four out of 10 people with a mental disorder consulted a health professional for their mental disorder.
Andrews et al. [2] reported on a comparison of the cost-effectiveness of treatment of 10 mental disorders. Data for three affective disorders (depression, dysthymia and bipolar), four anxiety disorders (panic, social phobia, generalized anxiety disorder and posttraumatic stress disorder), alcohol harmful use and dependence, and for schizophrenia, were compared in terms of cost, burden averted, and efficiency of current and optimal treatment. They then calculated the burden unable to be averted with current knowledge. The unit of health gain was a reduction in years lived with disability (YLDs, calculated as the prevalence times the change in disability weight). Summing across all disorders, current treatment averted 13% of the burden at an average cost of AUD$30 000 per YLD gained. Optimal treatment at current coverage could avert 20% of the burden at an average cost of $18 000 per YLD gained. Even at 100% coverage, 60% of the burden of mental disorders was deemed not to be avertable in the light of present knowledge.
The situation in comparable physical disorders is different. Andrews et al. [3] and Simonella et al. [4] chose three physical disorders on the basis of similarities in burden, prevalence and natural history to be homologues of the anxiety disorders (asthma), depression (osteoarthritis) and schizophrenia (rheumatoid arthritis). The striking difference is in terms of the degree of coverage, with 92% of people with asthma or arthritis receiving treatment compare with only 42% of people with comparable mental disorder receiving treatment. In these three physical disorders current care averted 29% of the burden at a cost-effectiveness ratio of $14 000 per YLD. The comparable figures for mental disorders were 13% of the burden averted a $30 000 per YLD. Optimal care at current coverage was deemed capable of averting 54% of the burden of these physical disorders at $10 000/YLD gained. The figures for the comparable mental disorders were 20% of the burden at $18 000/YLD gained. Current and optimal care for mental disorders is half as effective and twice as costly as treatment for these physical disorders.
The key policy questions remain: what is the cost, and is it cost-effective to increase the coverage of people with mental disorders to that approaching those of people with physical disorder? The basic data have been presented before, in table 4 in Andrews et al. [2], but appear to have been lost among the other findings.
In the original study we modelled two optimal treatment scenarios for each disorder.
Optimal treatment at current coverage: first we assumed that coverage and severity levels remained constant and that clinicians only used evidencebased treatments. We calculated the YLDs averted, the total cost and cost per YLD averted of optimal treatment. Optimal treatment at optimal coverage: second, and of importance for the current purpose, we modelled the cost and cost-effectiveness of evidence-based medicine (EBM) at hypothetical optimal attainable coverage, total coverage for all disorders being impractical. Optimal treatment strategies were kept constant and optimal coverage was arbitrarily defined as 100% for schizophrenia, 70% for the anxiety and affective disorders and for alcohol abuse, and 30% for alcohol dependence. Severity levels were kept constant for those currently in treatment and were varied for the ‘extra cases’ in treatment under optimal coverage to reflect the severity one would expect if those not currently in contact with services were covered, that is, proportionally more mild cases and fewer severe cases were added. Lastly we calculated the change in cost per YLD of these additional strategies to reduce the burden of mental disorders.
In Table 1 we present data for optimal treatment in which coverage is increased to the practical levels defined above, and severity is assumed to reflect the shift in severity of the additional cases. The average coverage is now two-thirds, and in this situation it is estimated that 28% of the burden could be averted at an overall costeffectiveness ratio of $16 000 per YLD averted. The total cost rises by some 300 million dollars (in 1997 dollars) over the current level of expenditure on these disorders, but the marginal cost-effectiveness of treating the extra 26% cases was only $12 000/YLD gained because there is no increase in coverage for the expensive treatments for schizophrenia and because the major increase in coverage is for disorders with an advantageous costeffectiveness ratio.
Cost-effectiveness of treatment given optimal coverage and optimal treatment with evidence-based medicine (Amended from Andrews et al. [2])
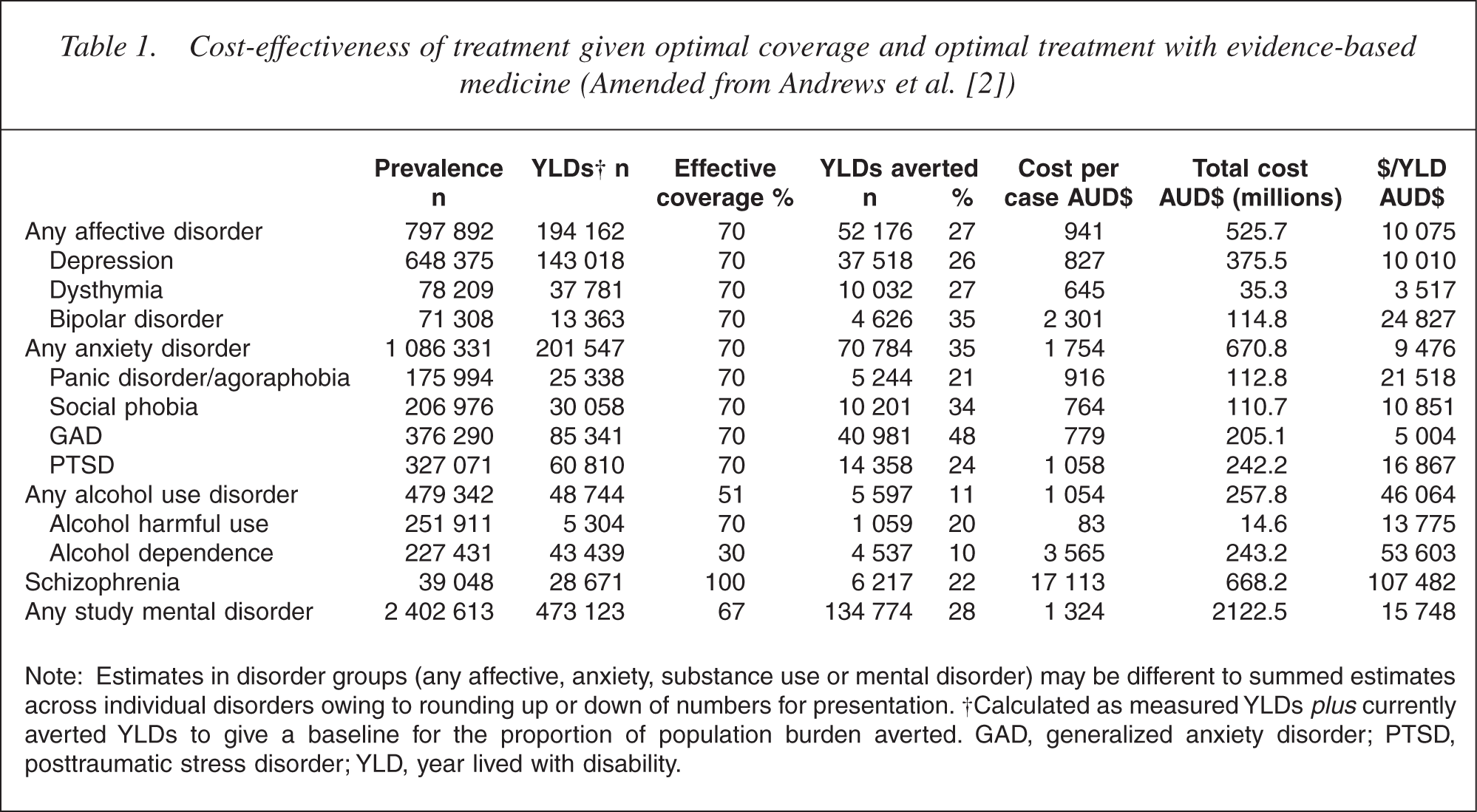
Note: Estimates in disorder groups (any affective, anxiety, substance use or mental disorder) may be different to summed estimates across individual disorders owing to rounding up or down of numbers for presentation. †Calculated as measured YLDs plus currently averted YLDs to give a baseline for the proportion of population burden averted. GAD, generalized anxiety disorder; PTSD, posttraumatic stress disorder; YLD, year lived with disability.
The results in the original paper were displayed according to the burden presently averted, burden averted by improvements in intervention and coverage, and burden unavertable in the light of existing knowledge. We would like to review these results commenting on each of the disorders in turn.
Affective disorders: current coverage is 60% with about half of those with affective disorders report receiving medication or cognitive behaviour therapy. Fifteen per cent of the burden is averted at an average cost of $20 000/YLD. When all receive treatment according to the clinical practice guidelines the burden averted climbs to 27% at an average of $10 000/YLD. Optimal treatment for the affective disorders is cost-effective, that for dysthymia (at $4000/YLD) especially so.
Anxiety disorders: Current coverage is low, too low for what are the most treatable disorders. For example, only 7% of people with social phobia received a notionally effective treatment. We do not know why coverage is so low. These patients identified anxiety as their principal complaint and treatment with antidepressants (selective serotonin re-uptake inhibitors) is not difficult. Increasing coverage to 70% with all getting EBM changes the picture. A third of the burden is averted (half the burden in generalized anxiety disorder) at an average cost of $9000 per disability adjusted life year. Nevertheless, even with perfect coverage and treatment, half the burden of anxiety disorders would not be avertable.
Alcohol use disorders: Coverage, at 11% is extremely low. Only 2% of the burden is averted and at $97 000/ YLD efficiency is low, not because the cost per case is especially high, but because the calculated health gain is low. Increasing coverage of interventions for harmful use to 70% and for dependence to 30% would result in one ninth of the burden being averted but the average cost per YLD remains high. Nevertheless, a campaign to encourage recognition and brief intervention in primary care for cases of harmful use may well be a sensible investment of funds, given the potential efficiency of $14 000 per YLD gained for such a treatment. EBM for alcohol dependence on the other hand is costly, even though we only included inpatient detoxification for people with hallucinations or seizures.
Schizophrenia: Coverage of schizophrenia was deemed to be complete because the data were obtained from catchment area studies in which every effort was made to identify all cases in contact with any of a wide range of services. We have argued elsewhere that there are probably an additional 10–20% of undiagnosed cases in the community [5] but for the purposes of this exercise we have accepted the coverage at a notional 100%. Current treatment with effective agents relieves 13% of the burden at a cost close to $200 000/YLD gained, owing in part to the high cost per case. Adoption of clinical practice guidelines could increase the proportion of YLDs averted to 22% but the cost per YLD, would still remain somewhere between $60 000 and $205 000.
To conclude: increasing coverage to an attainable 66% would cost, in 1997 dollars, an extra $300 million at an overall cost-effectiveness of $16 000/YLD and a marginal cost-effectiveness of $12 000/YLD, both costs being well under the automatic affordability threshold of the Gross National Income per Capita which, in 1997, was $27 000. The extra $300 million is probably in part already occurring owing to the impetus for general practitioners to identify and treat people with common mental disorders, paid for by the Better Outcomes in Mental Health Initiative and the accompanying leverage of Medicare funds. Given the new initiatives announced following the Council of Australian Governments meeting in February 2006 it is important that health planners realize where the health gains are to be made. Money and efficiency do not appear to be rate limiting steps.