
Abstract
Keywords
The issue of dual diagnosis is of major interest internationally and the prisons are an area where severe problems associated with multiple disorders are a very common form of presentation. Indeed the vast majority of those with disorders who are imprisoned have multiple disorders and services which aim to address such complex problems are more likely to have some positive impact. There are very limited data available to determine what proportion of those who have severe drug dependence problems and contact with a range of social and criminal justice services actually obtain help. Also there is limited information on whether there is appropriate matching between severity and actual level of service provision. There is a commonly held view that people with certain categories of disorders access more effective help than do others. This may be related to severity and complexity, but may also be related to current service structures and priorities, which could reflect systemic bias against disorders that carry high levels of stigmatization [1]. In our large prison survey [2], receipt of help for a mental or emotional disorder in the year before imprisonment, was most strongly associated with evidence of a psychosis and with presence of significant symptoms of common mental disorders such as anxiety and depression. In this paper we explore in some detail the relationship between drug dependence and receiving help, and explore the comparable likelihood of receiving help with different disorders and differing combinations of comorbidity. Of particular interest is the influence of various combinations of disorders in influencing both help seeking and actual receipt of help. This study was part of a large programme of national psychiatric morbidity in England and Wales [3].
Methods
In 1995, as part of a major national psychiatric morbidity survey, prisoners from all prisons that were operational at the time in England and Wales (n = 131) were surveyed by the Office for National Statistics (ONS). The Local Inmate Directory System (LIDS) was used as the sampling frame. The LIDS is a computerized database of all inmates that is entered in each local prison but also held centrally. Of the 3563 prisoners who were selected, 3142 (88.2%) completed private, face-toface interviews with trained ONS staff; 37 prisoners agreed to participate, but did not complete the interview, and 198 (5.6%) refused to take part. The main purpose of the survey was to determine the level of psychiatric morbidity within the prison population, as part of a national programme of psychiatric morbidity surveys, including general adult household, institutional, homeless and also a child and adolescent survey [3]. Further information about the study methodology and protocol has been presented elsewhere. Interviews covered a range of topics including sociodemographic data, daily living and social function, stressful life events, general health and service use in addition to psychiatric morbidity [2].
Measures
Demographic and background variables were established using a series of closed questions. The nine categories recommended by the Government Statistical Service were used to record ethnicity. Due to the small numbers of respondents reporting most ‘non-white’ ethnic groups, the categories were then collapsed into three groups (‘white’, ‘black’ and ‘other’) as used by Singleton [2]. Respondents were shown a list of traumatic events and serious problems (such as bullying at school, serious illness or injury and the experience of homelessness), and asked to indicate which ones (if any) they had ever experienced.
Psychiatric diagnoses
The Structured Clinical Interview for DSM-IV (SCID-II) [4] was used to diagnose personality disorders. Neurotic symptoms were examined using the revised version of the Clinical Interview Schedule [5]. This instrument is made up of 14 sections that each assesses the presence of a specific neurotic symptom during the past month (e.g. somatic symptoms, worry, depressive ideas, etc.). Each section is scored between 0 and 4. Symptoms are classified as ‘severe’ if a score of 2 or more is obtained. A series of binary variables were created to indicate whether or not each of the 14 symptom types was severe. A total score for all 14 sections in excess of 12 is used as the threshold to indicate the presence of some kind of neurotic disorder.
Drug use
Respondents were asked to indicate which of a list of drug types (cannabis, amphetamines, crack cocaine, cocaine powder, heroin, nonprescribed methadone, illicit tranquillisers, solvents and ‘other’) they had: (i) ever used (and their age at initiation); (ii) used while in prison; and (iii) used for the first time while in prison. Reports on injecting history and, where relevant, the age of initiation of this behaviour, were also sought.
Prison history
A number of questions were designed to assess respondents' prison history. Inmates were first asked whether they were on remand or sentenced and to indicate how long they had been in prison in relation to their current offence, from a list of eight options (ranging from less than 1 week to 2 years or more). They were then asked if they had any previous convictions and if this was their first time in prison. Where relevant, estimates for the total number of previous prison terms were sought.
Service use in the year before coming to prison
Questions about help received for mental, nervous or emotional problems in the year before coming to prison, were only addressed to those who had been in prison for less than 2 years.
A number of questions were designed to assess respondents' history of treatment before coming to prison. Prisoners were asked if they had sought or obtained help from a range of community agencies in the year and in the month prior to coming to prison. These agencies were categorized as
Help from general practitioner/family doctor Help from a psychiatric health professional Help from any other source Any source of help
These groups were chose because of the possible confusion between some titles and the desire to minimize confusion about identification of differing types of community agencies. The range and spread of professionals involved in the field make the simple categorization of help received difficult to clarify without using an exhaustive list.
The category psychiatric health professional was made up of the following professions: psychiatrist, psychotherapist, community psychiatric nurse, psychologist and psychiatric social worker.
Help from any other source was the category used for those reporting contact with a counsellor, drug worker, probation officer and ‘other’ categories of workers.
Statistical analyses
Logistic regressions were used to characterize the relationship that personal background and service utilization had with drug use and type of drug dependence. The direct association of drug use with service utilization status and psychiatric status (while controlling for personal background and social history effects) was also examined.
Logistic regression was carried out to look at the association with service use of each disorder independently of the other disorders and other possible confounding factors.
Results
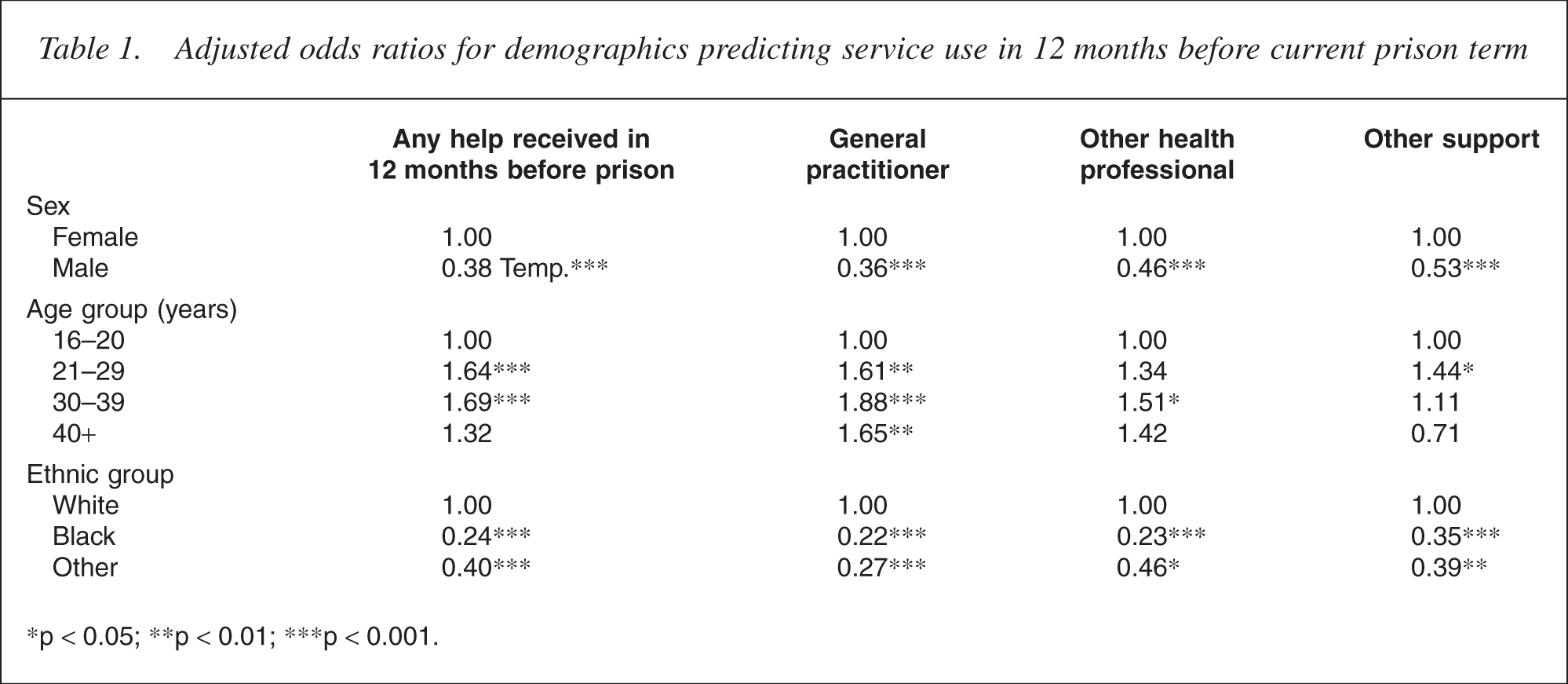
Receipt of any form of help was demographically most strongly associated with being older, white and female. Women were about twice as likely as men to report having received help for mental or emotional problems. The most common source of help was a general practitioner or family doctor, mentioned by about two thirds of those who had received help. Next most common source of help was a psychiatrist, followed by a drug worker and a range of other sources of help. Older age was also consistently associated with greater levels of reporting having received help, for both genders but only for use of general practitioners.
Being black was strongly associated with reduced likelihood of receiving help and this was maintained after adjusting for other sociodemographic variables. The category Other ethnic group had also significantly less service utilization in the previous year (Table 1).
Sociodemographic characteristics, family status and family burden of the parental generation of healthy non–offenders (n=103), non–schizophrenic offenders (n=103), schizophrenic non–offenders (n=103), and schizophrenic offenders (n=103) before age 18
∗p<0.05; ∗∗p<0.01; ∗∗∗p<0.001.
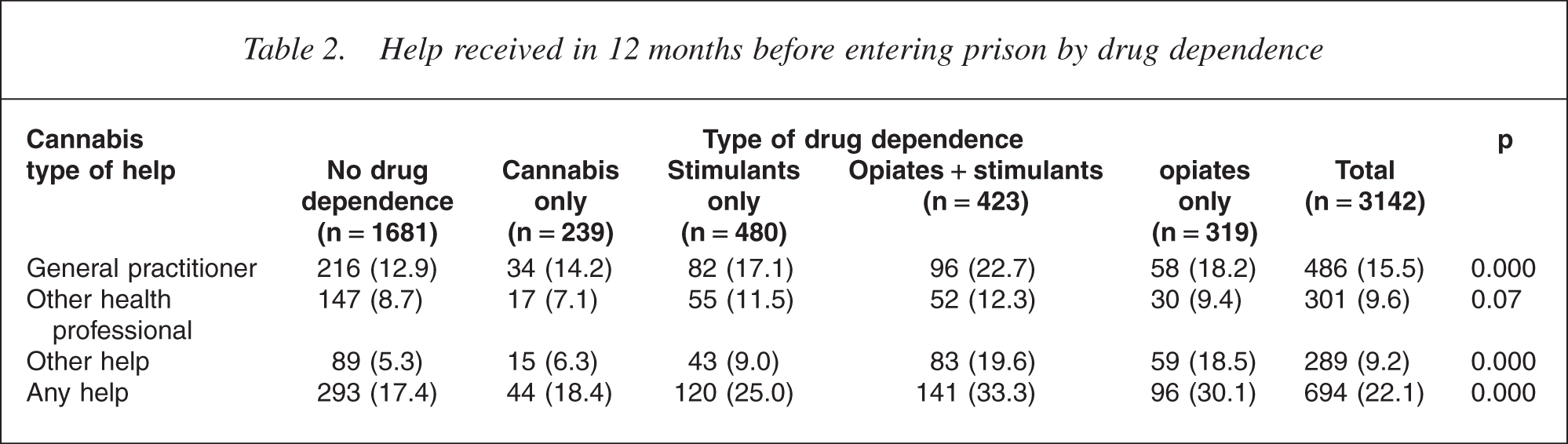
Overall the commonest source of help in the year before prison was the general practitioner, and this was true for all categories except possibly those dependent on opiates. However, overall only slightly over one in five of those who were rated as dependent on opiates had received help, and one in 10 of those rated as dependent on stimulants had received help. Nevertheless, those who were rated as dependent were significantly more likely to receive help than those with no drug dependence.
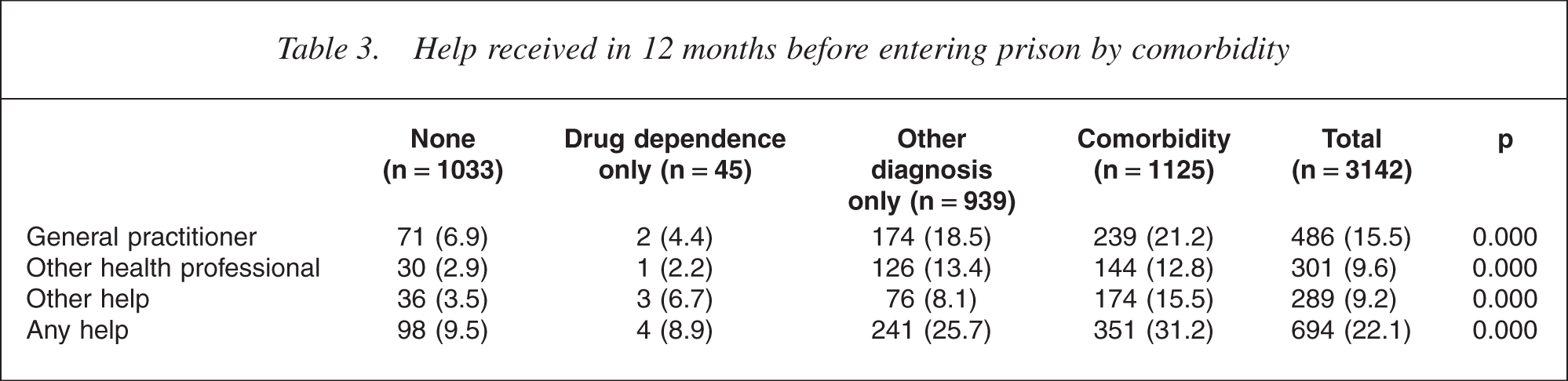
In order to explore this further, type of help was compared in those with drug dependence only and in those with comorbidity, which was rated where a common mental disorder, a psychosis or a personality disorder was assessed as being present according to the rating scales of the survey. Tables 2 and 3 demonstrate that when compared with individuals with no disorders, those with any type of drug dependence, or any type of drug dependence in combination with another psychiatric disorder, were significantly more likely to have received help of some kind.
Help received in 12 months before entering prison by drug dependence
Help received in 12 months before entering prison by comorbidity
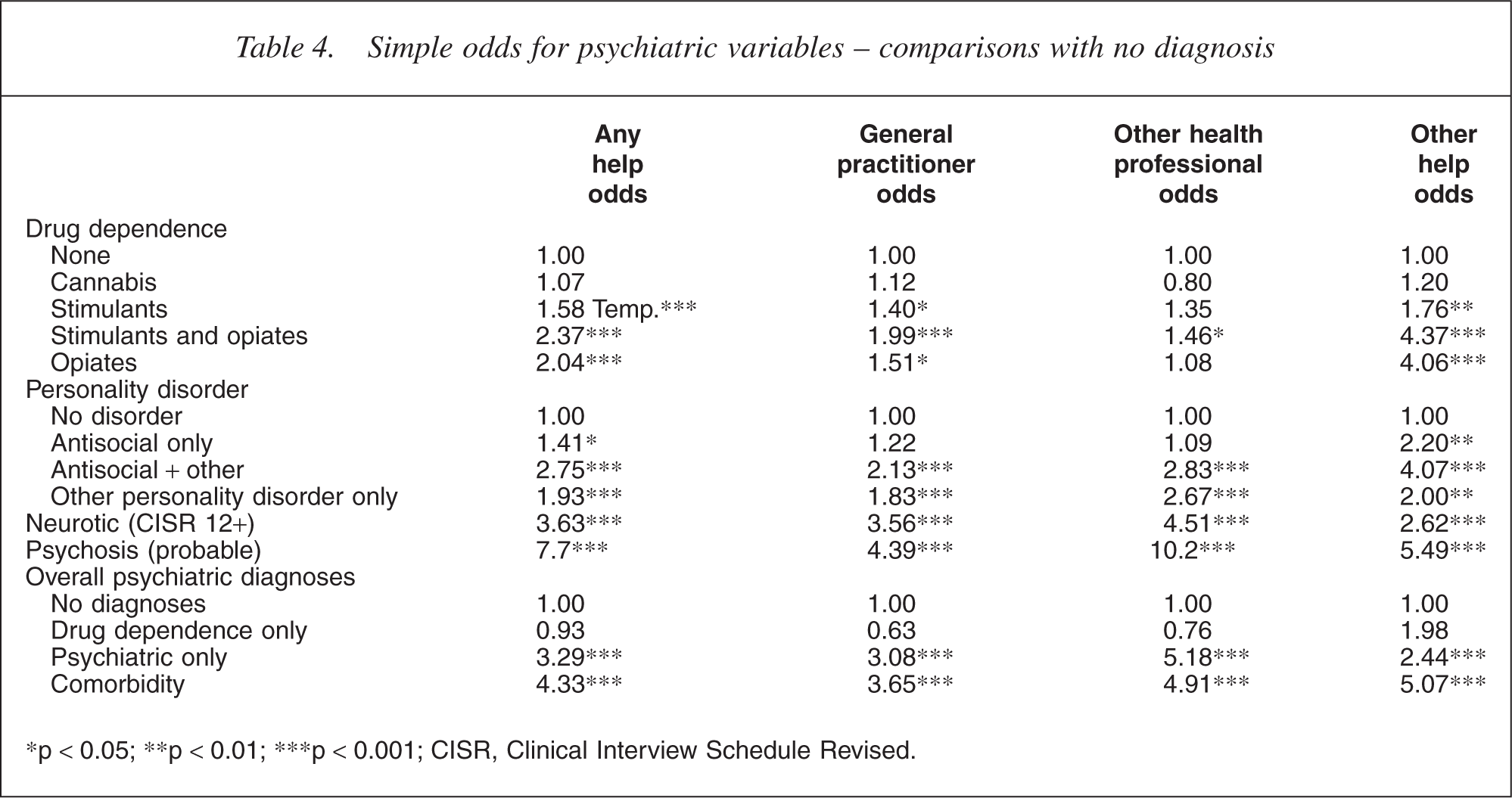
Multiple logistic regression was then carried out to look at the association with service use of each disorder independently of the other disorders. A comparison is made between those with no diagnosis and those with single or multiple diagnoses. A simple logistic regression Table 4 and an adjusted regression Table 5 to control for confounding variables was undertaken.
Simple odds for psychiatric variables - comparisons with no diagnosis
∗p <0.05; ∗∗p <0.01; ∗∗∗p < 0.001; CISR, Clinical Interview Schedule Revised.
Adjusted odds predicting service use in 12 months prior to entering prison
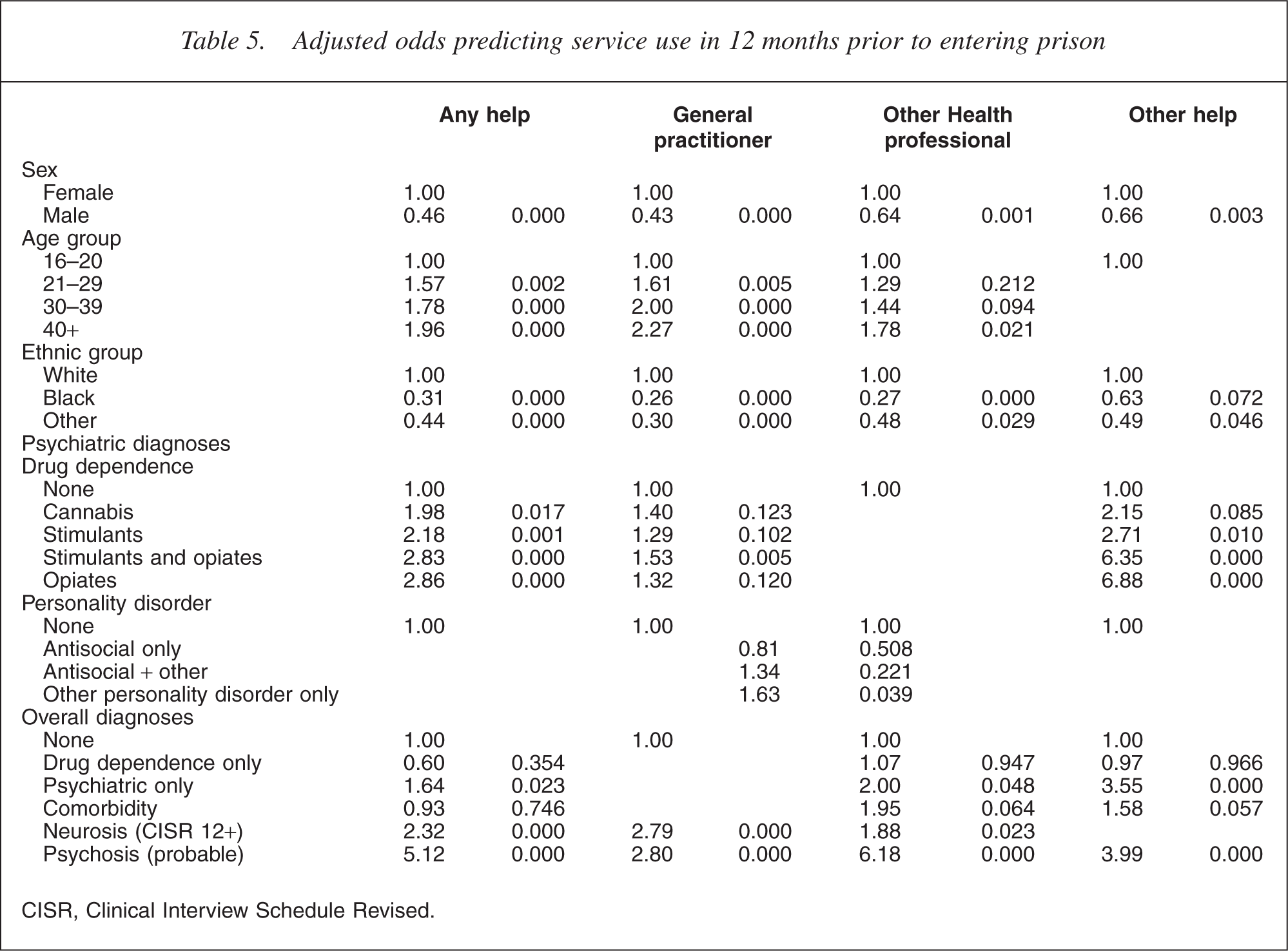
CISR, Clinical Interview Schedule Revised.
Because of the high prevalence of disorders and the complex combinations there is some substantial overlap in those categories where comorbidity is found. However, the results show that for drug dependence, treatment in the community is significantly predicted for those with opioid problems. The increased odds for cannabis and stimulants is much less than that for opioids. The presence of antisocial personality disorder with another disorder has similar odds of receiving treatment to opioid dependence.
Having a common mental disorder is associated with increased odds for getting help, but the strongest predictor of receiving treatment is the presence of a probable psychosis.
The adjusted odds (Table 5) indicate that there are many overlapping influences and when these are controlled for, it is opioid dependence alone or opioid dependence with stimulant dependence, psychiatric disorder alone and probable psychosis that are most predictive of service use in the 12 months prior to imprisonment.
The type of service used is hard to interpret, but it is most striking that all types of services are involved in responding, and it's mainly with opioid dependence that other sources of health care are most used, and with psychosis that other health professionals are used.
Discussion
Currently, there is a paucity of knowledge and understanding of patterns of service utilization. It is generally assumed that the majority of people with substance use disorders make limited use of services and only a minority are in contact with services at any given time. The heterogeneous nature of these disorders may be such that many who rate for having a disorder do not meet severity criteria that would necessitate formalized treatment, and this may explain to some extent the low levels of service access. However, this study uses data on a more complex and severe population, who are rated as having high levels of substance dependence and very high levels of other psychiatric disorders; it explores factors predictive of prior service utilization. The overall impression of this population is one of severe needs with high levels of psychosis, high levels of personality disorder and high levels of tobacco, alcohol and drug dependence.
The challenge of providing community-based interventions prior to, during and after imprisonment is at the core of the debate on the nature of services for dual diagnosis. It is this population with multiple diagnoses and substantial additional social disadvantage that fall between most of the community-based services.
This analysis indicates that those with the most severe problems appear to be the ones most likely to receive help. This analysis also indicates that use of psychostimulants, and demographic factors such as ethnicity, are associated with reduced likelihood of receiving help. The disparity across the different ethnic groups in terms of health access is striking, it is not clear whether this is unique to England and Wales but it is reasonable to speculate that ethnic minorities in most settings will have similar experience of low access to health care and higher risk of imprisonment.
Farrell et al. [6] reported that psychostimulant use and heavy cannabis use in the prison population was associated with increased risk of psychotic disorders. The rising use of psychostimulants worldwide and the risk of increased psychiatric morbidity associated with psychostimulant use requires improved formal access to services at the community level.
This study explores factors predictive of service use prior to imprisonment. It is cross-sectional in nature and very much will reflect the nature of service provision of the era. Despite this limitation it provides a useful snapshot of patterns of needs of this population and indicates that in the year prior to imprisonment, the majority of mental health needs of these individuals were not being met by community-based services.