
Abstract
Work is an important part of the lives of many people. Aside from generating income, it provides a time structure for the waking day, regular contact with people outside the immediate family, involvement in shared goals, enforced activity and a sense of identity [1]. Importantly, work is associated with positive mental health as it provides opportunities for skill development and social contacts and participation in the fabric of the community [2], all of which boost self-confidence and self-esteem. While work environments are challenging and sometimes stressful for people with severe mental illness, the bene-fits of participation, inclusion, empowerment and economic wellbeing outweigh any disadvantages [3].
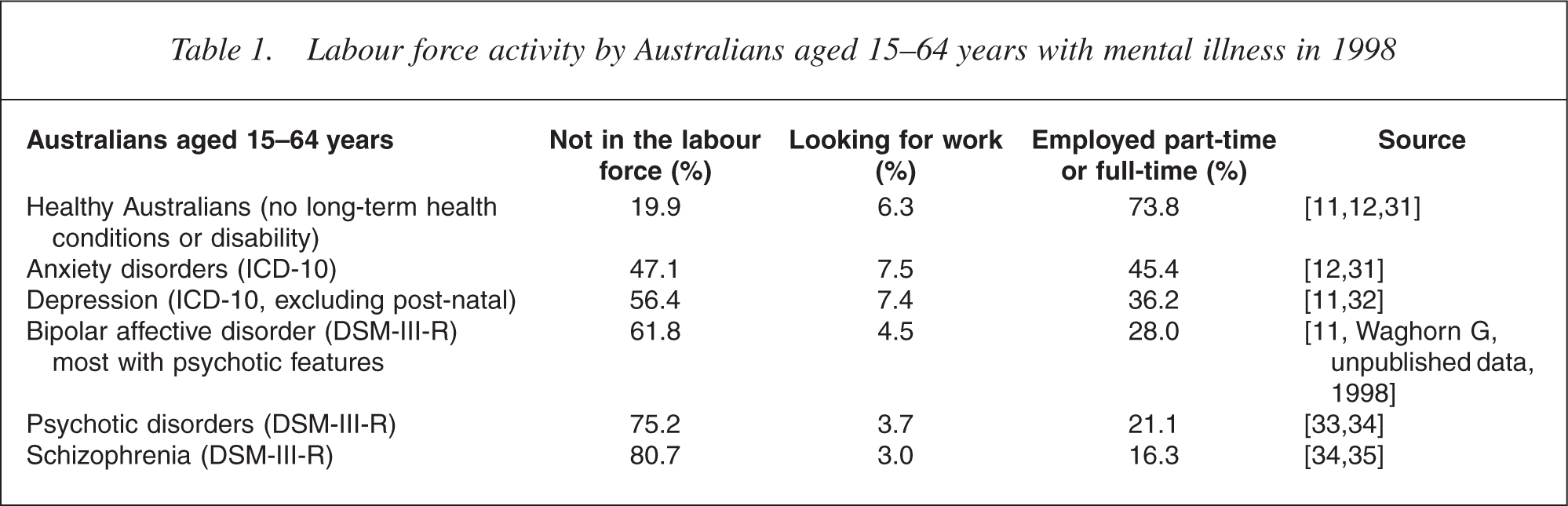
For people with severe mental illness, unemployment and non-participation in the labour force characterize the social exclusion that deinstitutionalization has failed to overcome [4, 5]. In Australia, the employed proportion of people with severe mental illness in 1998 ranged from 16.3% among people with schizophrenia to 21.1% among people with mixed psychotic disorders, in reciprocal contrast to healthy working-age Australians, 73.8% of whom were employed (Table 1). These populationlevel statistics reveal the difficult but not impossible challenges facing people with severe mental illness in terms of acquiring and maintaining employment [6]. At the community level, establishing people with severe mental illness in the workforce requires a commitment to providing suitably intense and continuous assistance [7] in order to help individuals overcome initial barriers to employment [8, 9] and to help individuals retain employment by acquiring new skills and maintaining productivity [10]. Employers may also need ongoing assistance to solve the problems which can arise, including finding ways to accommodate individual employment restrictions in particular work settings [11, 12].
Labour force activity by Australians aged 15–64 years with mental illness in 1998
The employment status of people with severe mental illness is recognized as an indicator of the quality of our society. Social quality refers to the concepts of social inclusion, socioeconomic security and empowerment [13]. Increasing opportunities for people with mental illness to rejoin their leisure, friendship and work communities are expected to substantially improve social quality. People with severe mental illness can contribute to the social and economic life of their communities, and any assistance provided can maintain an emphasis on maintaining individual wellbeing and realizing individual potentials.
Three types of barrier to employment access for Australians with severe mental illness have been identified [8, 9]: (i) the impact of mental illness on the person; (ii) external barriers such as the nature of the labour market and the availability of suitable employment assistance; and (iii) other systemic barriers to employment, such as community stigma and low expectations of health professionals. These are not specific to Australia and present major challenges to vocational services for people with severe mental illness internationally.
However, in addition to these, there are structural barriers that are an effect of the Australian service environment. These distinctive barriers are: (i) the current system of service organization which provides no incentives for linking health care to vocational services; (ii) historical, legal and design constraints which limit the capacity of CRS Australia and the Job Network to provide suitably intensive and continuous services; (iii) limits on allocated case-based funding places in disability employment services irrespective of demand; and (iv) a right of client refusal extended to each service provider, with no access protections for people with more substantial assistance needs. These structural barriers indicate that the current organization of Australian services is inconsistent with those characteristics identified as critical to effective vocational services for people with severe mental illness [14, 15].
In this paper, we focus on the first of these structural barriers. We examine the Australian policy settings underpinning the separation of vocational and health services, we consider the implications of this separation for the implementation of evidence-based vocational services and we consider two approaches to overcoming this particular barrier.
The Australian policy framework for vocational rehabilitation
During the 1980s, the Commonwealth Rehabilitation Service (now known as ‘CRS Australia’) moved away from residential and outpatient institutional settings into community-based service delivery, involving a range of allied health practitioners working as case managers in multidisciplinary teams. The intention of this strategy, later reinforced through the Commonwealth State Disability Agreements and the Commonwealth Disability Services Act 1986, was to provide individualized vocational rehabilitation services in collaboration with the client's medical providers, local community and local employers [16]. The 1980s also saw the rise of consumerled demand for employment access for disabled people to work in competitive employment settings with access to ongoing support. The federal Disability Open Employment service network was enabled by the Commonwealth Disability Services Act 1986 to meet this need, and some services specialized in assisting people with severe mental illness [16].
The government agency responsible for funding vocational rehabilitation and disability employment services is currently the Australian Government Department of Employment and Workplace Relations. The Australian Government Department of Health and Ageing has responsibility for the National Mental Health Strategy, where state- and territory-operated health services provide public-funded clinical services to people with severe mental illness. The structural separation of public health from vocational services for people with disabilities is part of a larger pattern of service fragmentation involving public and private health services, state- and territoryprovided rehabilitation and disability support services, vocational training and higher education. This service fragmentation may be an unintentional consequence of a policy framework that encourages people with severe mental illness and more generally people with disabilities to access mainstream vocational and disability support services [17, 18].
Access to vocational rehabilitation and disability employment services is typically via Centrelink, although people can refer by oneself or be referred by others including health professionals. Increasingly, funding is case-based and service providers must obtain Centrelink endorsement that the person applying for assistance is eligible for a particular allocated place. There is considerable overlap between three arms of vocational assistance: vocational rehabilitation (via CRS Australia, intended to assist with reduction of disability and development of work capacity); open employment services (aimed at people who need more continuous assistance to retain employment); and assistance provided by Job Network services who provide the mainstream link between employers and job seekers as well as more intensive assistance for disadvantaged job seekers.
A recent reorganization of federal government departments collected all three programs together for the first time as the responsibilities of one federal agency, the Department of Employment and Workplace Relations. Funding for vocational rehabilitation and disability employment services expanded in 2005. Further, government reforms relating to assessment and referral mechanisms are under review and significant changes are expected over the next few years.
Supplementing the framework of vocational assistance, the employment of people with mental illness is also promoted in Australia by a range of state and federal anti-discrimination and unfair dismissal legislation [19], including the federal Disability Discrimination Act (1992). Although it is impossible to gauge whether legislation actually helps people with mental illness to obtain and retain employment, or simply increases employer disincentives, employees with a mental illness have the right to invoke legal protections against unfair discrimination in terms of recruitment, promotion, transfer, training and dismissal practices, as well as working conditions. However, employers have broader legal responsibilities, including the obligation to provide a safe workplace for all employees, customers and members of the public. A detailed discussion of the complex ethical and legal frameworks most relevant to the employment of people with mental illness is available elsewhere [19].
Evidence-based vocational services for people with severe mental illness
The evidence base for interventions designed to achieve vocational outcomes for people with severe mental illness can be considered from both the component perspective and the program perspective. The component perspective focuses on identifying a set of characteristics that distinguish effective services. The program perspective focuses on differentiating more successful programs from less successful programs. The benefit of the component perspective is that it potentially allows for a wide range of programs, suited to specific environments, to be generated from a set of evidence-based components. However, because the evidence base has been primarily generated through testing of programs, it is possible that components are effective only when combined in specific ways to achieve a program with high fidelity.
Waghorn [9] identified 11 vocational service components with potential importance in evidence-based employment services for people with severe mental illness. These include seven components specified by Bond [14], four of which have been endorsed as having strong empirical support [15]:
The goal is competitive employment in the open labour market Consumer choice as the only entry criterion Rapid commencement of job search activity within 4 weeks of commencement Integration of mental health care with vocational services Assistance components are determined by consumer preferences Support is not time-limited Benefits counselling to minimize disincentives through the impact on health benefits, income support payments and fringe benefits.
In addition, Waghorn [9] identified four components with potential to enhance vocational outcomes: (i) a capacity to provide intensive on the job support; (ii) a multidisciplinary team approach; (iii) an emphasis on the rehabilitation alliance; and (iv) the use of systematic stigma countering and disclosure strategies [19].
At a program level, supported employment (SE, often termed ‘open employment’ in Australia) is an approach that incorporates many of these components and has an established evidence base for effectiveness [14, 15,20–23]. Among SE programs, Individual Placement and Support (IPS) has consistently outperformed other employment services for people with severe mental illness in randomized controlled studies and day rehabilitation conversion studies [14, 15]. Individual Placement and Support is usually provided in a fully integrated mental health service environment, typically with employment specialists providing vocational services within a community mental health team, often using an assertive community treatment approach [23].
Although co-location and complete integration of mental health care and vocational services has become the accepted means to achieve integration, there is one report of successful delivery of the IPS approach without complete integration, via the Massachusetts Supported Employment and Education service [24]. Here, the employment service operated as a separate team and met IPS fidelity through weekly meetings with the clinical team. Although not a controlled trial, outcomes were benchmarked against previously reported IPS outcomes. The results suggest that effective communication protocols can substitute for full integration of vocational and mental health services.
Individual Placement and Support is not the only approach to have outperformed usual services in achieving employment outcomes for people with severe mental illness. The multi-site Employment Intervention Demonstration Program recently reported that a range of mental health programs with employment-focused enhancement outperformed usual care [25]. Of particular importance was the finding that the common feature of more effective programs was integration between employment services and mental health services.
In summary, there is evidence to support both specific components of effective employment services for people with severe mental illness and programs that combine components. The evidence base is insufficiently developed to specify a minimum or necessary component combination, but there is growing evidence that effective integration of employment and mental health services is critical in differentiating more effective services from less effective services. Integration is a key differentiating feature of IPS, which is the most empirically SE program, and has been found to be the single variable that best differentiates more and less effective programs across a range of services. Integration is usually achieved through co-locating employment specialists within the mental health team [23].
Discussion
While evidence-based ingredients have emerged from overseas studies, it is difficult to determine the extent that Australian vocational rehabilitation and open employment services make use of such practices. Disability Service Standards [26] require practices that include encouraging clients to identify jobs consistent with their career goals and focus on competitive employment rather than use lengthy periods of pre-vocational training. Clients who commence employment are typically offered reasonably flexible, intensive and continuing support of an employment specialist. In addition, some services report offering counselling with respect to the impact of employment on government income support payments and fringe benefits.
However, the framework for service provision in Australia presents structural barriers in relation to two components. First, the role of Centrelink in determining eligibility for support, and the right of refusal allowed to all employment service providers, means that consumer choice is not the only entry criterion. Second, for policy reasons discussed above, integration of employment services and mental health services (through shared teams, co-location of services and shared meeting and recordkeeping processes) is difficult. Furthermore, it is likely that separate services have limited interest in outcomes beyond those that are specific to either employment or health. Given the emerging importance, in multiple welldesigned empirical studies, of service integration as a critical component of employment outcomes for people with severe mental illness, this is probably the more important challenge to the implementation of evidencebased services.
There is an opportunity to improve employment outcomes for Australians with severe mental illness through enhancing integration of mental health care and vocational assistance. The overseas evidence suggests two approaches to this challenge. Full integration involves structural links, usually achieved through co-location with subsequent shared opportunities for formal and informal communication. There is an established evidence-base to suggest that this kind of integration differentiates more successful from less successful employment services for people with severe mental illness [25]. The other approach might be termed ‘enhanced intersectoral links’ and involves the establishment of formal communication structures to enable collaboration and sustained communication between vocational and clinical services, supported by formal protocols and regular cross-training. The empirical basis for concluding that this approach can yield the benefits of integration is relatively weak, but this reflects limited investigation rather than implementation attempts that have failed.
The major advantage of attempting to achieve integration through enhanced intersectoral links is its consistency with current policy settings that favour mainstream disability support services. It is possible, although far from certain, that there are also cost advantages. Relative program cost is an important issue and it is also possible to identify cost advantages associated with full structural integration. A summary of some possible advantages and disadvantages of each approach in Australia is set out in Table 2.
Possible advantages and disadvantages of full integration and enhanced intersectoral links as approaches linking continuing care to vocational services for people with severe mental illness
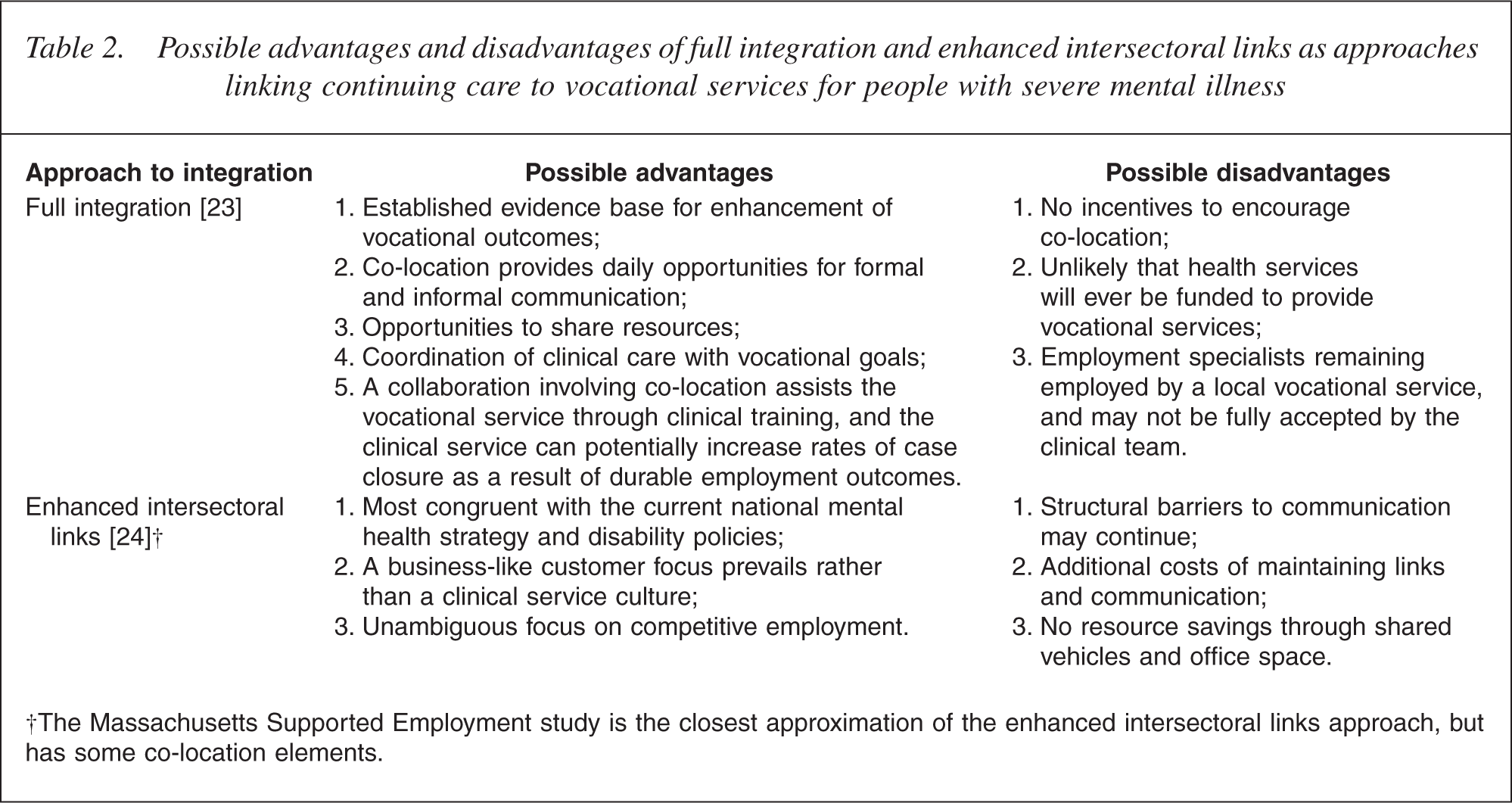
†The Massachusetts Supported Employment study is the closest approximation of the enhanced intersectoral links approach, but has some co-location elements.
A major advantage of full integration is that clinicians and employment specialists coordinate their work with clients. Clinicians take into account vocational goals and current vocational activities when implementing changes to treatment or continuing care plans. Employment specialists attend to mental health status while monitoring client work performance, because this is likely to provide early warning of deteriorating mental health status or the intrusion of other life problems. As a result, the fully integrated team can achieve flexible and assertive engagement in treatment and mental health selfmanagement, levered by another goal of the patient, to obtain and sustain satisfying employment.
The major disadvantage of the fully integrated approach in the Australian context is that policy settings currently provide no incentives for state-operated community health services to formally collaborate or colocate with federally funded vocational services. It may be possible to achieve co-location, but there are no existing precedents that would support this. Furthermore, the separation of clinical and disability support services is underpinned by a philosophical commitment, especially in the health sector, to mainstream and the use of intersectoral links rather than integration to facilitate access [18].
Co-location may imply increased costs if it is delivered in an environment of low clinical caseloads and extended hours of service [27, 28] characteristic of some implementations of the IPS model of mental health service delivery. Caseloads in Australian mental health services are typically around 30 per full-time clinician [29], whereas more flexible, assertive extended hours clinical services require caseloads of less than 20, implying a possible increase in total service costs. However, IPS has been successfully delivered within the framework of standard multidisciplinary clinical teams, which means that lower clinical caseloads are not a necessary feature of co-location. There are potential cost–benefits deriving from employment (decreased need for income support or contribution to taxation), but these would not be routinely factored into service budgets, which means that it would be difficult to establish a favourable funding environment unless there was a substantial reduction in need for expensive clinical services, such as inpatient admissions [27]. However, there is potential for integrated employment services to result in decreased demand for clinical services [30], which is a direct cost offset.
The alternative approach of enhancing intersectoral links between vocational rehabilitation workers and mental health clinicians to achieve integration has the advantage of being consistent with current policy settings. In this approach, the vocational rehabilitation service remains administratively separate from the clinical services and integration is achieved through the allocation of case-based funding places to the health service's outpatients, supported by cross-training and service protocols that emphasize frequent and effective communication.
The major challenge for this approach is the time and energy required for maintenance of sufficient communication and continuing agreement on service priorities, so that health-care plans do not conflict with vocational plans and so that clinicians and employment specialists have access to pertinent information obtained by one or other. Such communication cannot be assumed in the absence of geographical proximity and subsequent natural opportunities for both formal and informal communication. Thus, while in principle, adjustment to existing mental health caseloads is not required, in practice, clinicians would probably require somewhat lower caseloads to free up the time for higher levels of communication with employment services. It is also likely that there would be costs associated with the installation of a quality assurance mechanism adequate to maintain high-quality linkages. These costs are not offset by the resource sharing that is potentially available through co-location and separate service provision necessitates some duplication of services compared with co-location.
Because the concept of integration of health and vocational services is new to Australia, it remains to be seen how the barriers to linking mental health care with vocational services are best overcome. Well-designed studies that investigate the impact of service integration on both employment outcomes and costs are urgently needed. We think that the first step is to demonstrate the feasibility of both linkage and co-location models in the Australian service environment. Once feasibility is established, we recommend randomized controlled trials that evaluate both kinds of integrated services against current services. There may not be a uniform solution. It is plausible that each regional, rural and remote area may need its own local solution, which may be different to the form of integration suited to a populous and service-rich urban area.
Conclusion
People with severe mental illness are highly disadvantaged with respect to participation in the labour force, and the provision of more effective employment services for this population is of international importance. Components of effective employment services for people with severe mental illness have been identified and the importance of service integration is well established. However, integration between employment and clinical services is difficult to achieve in the current Australian policy environment. Co-location of clinical and employment services and enhancement of intersectoral linkages between separately located clinical and employment services are two strategies for achieving better integration. Each has identifiable advantages and disadvantages. Given the importance of employment outcomes for people with severe mental illness, systematic investigation of the different means by which clinical care can be integrated with evidence-based employment services is a research priority.