
Abstract
Suicide is a major public health problem in Australia, with more than 2500 deaths by suicide registered each year [1]. The overall suicide rate in Australia has remained relatively stable over the last century and is in the mid-range for developed countries [2]. Male deaths by suicide are consistently higher than female deaths across all age groups. However, there have been considerable changes in the rate of suicide among specific age groups. In particular, the rate for young men aged 15–24 has jumped threefold since 1960s, and more recently, the rate has also increased for males in the 25–39-year age group [3].
Rural communities experience higher rates of suicide than urban areas [3]. Suicide rates for males in rural communities have increased steadily over the past 20 years, with rates for young males consistently higher in small rural communities than in metropolitan and regional areas. More specifically, rural inland towns with populations of less than 4000 people have experienced the most significant increases in male youth suicide [4].
Several research groups have examined the possible relationship between suicide rates and geographic location. Dudley and colleagues [5] investigated rural–urban differences in youth (persons aged 10–19 years) suicide in New South Wales (NSW). They demonstrated a significant increase in the youth suicide rate in NSW rural cities, and an even greater rise in rural municipalities and shires over the 25 years from 1964 to 1988. The increase occurred largely among males aged 15–19 years. By contrast, the rate moderately increased in Sydney, and was stable in Newcastle and Woollongong. Consistent with these findings, Krupinski and colleagues [6] reported that the male suicide rate in Victoria was greater in rural compared with urban areas.
Cantor and Coory [7] however, found that the rural– urban difference (rural defined as any community with a population <20 000) in suicide rate in Queensland for the period 1986–1990 was not statistically significant. The rural rate for males was only marginally higher than the overall Queensland rate, while the rural rate for females was lower than the overall Queensland rate. In a later study, Cantor and Slater [8] highlighted the complexity of the relationship between suicide rates and geographical location by demonstrating that rural Queensland health regions displayed both the lowest (DarlingDowns and Mackay) and the highest (Peninsula) suicide rates.
In a further study, Dudley and colleagues [4] made a detailed examination of the rural–urban differences in suicide rate demonstrated in the ABS data. They reported that over a 30-year period (1964–1993) male suicide rates for the 15–24-year age group doubled in metropolitan areas, increased fourfold in towns with population <4000, and dramatically increased 12-fold in towns with <4000 population. Female suicide rates overall for the 15–24- year age group did not increase, but increased 4.5-fold in towns with population <4000.
Wilkinson and Gunnell [9] have also examined the relationship between overall population, male and female suicide rates and geographical location. They studied individuals of a broader age range (15–34-year-olds), living in Australian metropolitan and non-metropolitan (≤20 000 people) areas over the period 1988–1997. Their data demonstrated that for the decade 1988–1997, suicide rates for non-metropolitan males aged 15–24 years were 50% higher than metropolitan 15–24-year-old males, but for 25–34-year-old males, there were no significant differences according to area of residence. In 15–24- year-old females, there were no significant differences according to area of residence, while the rates for 25– 34-year-old females were higher in metropolitan than in non-metropolitan areas.
Most recently, Caldwell et al. [10] examined suicide data collected by the Australian Institute of Health and Welfare over the 4-year period 1997–2000. They compared age-specific suicide rates in metropolitan centres of population ≥100 000, rural centres of 10 000–99 999 population, and rural areas with population<10 000. Suicide rates for males were higher in rural centres and other rural areas across almost all age groups. The only exceptionwas those aged≥60 years living in rural centres. Men aged 20–29 years living in non-metropolitan centres had particularly high suicide rates (rate in other rural areas < rate in rural centres). Suicide rates for women were similar in metropolitan and rural areas with one exception: women in rural centres in the 30–44-year age group had higher rates than metropolitan women of the same age.
Overall, the available data on rural suicide rates in Australia reveal a complex picture. There is a need to go beyond a crude examination of urban–rural differences in suicide rates, to examine the nature of any differences, or issues that may be specific to or of particular importance in rural settings. One set of variables will most likely relate to place, and the very dramatic increase in male suicide rates in small rural towns suggests that there may be features in particular rural locations that have a significant ‘place’ impact on suicide rates.
How can the elevated rates of rural suicide be understood?
There is no single cause of suicide. Generally, psychosocial stressors impinge on a vulnerable person to promote suicidal thoughts and behaviour that may have varying degrees of lethality and intent. However, there is overwhelming evidence to suggest that mental health problems and mental illness (particularly mood disorders, substance abuse disorders and antisocial behaviours) play a major role in the aetiology of suicide. Studies have repeatedly shown that 90% of those who die by suicide have a treatable psychiatric illness at the time of death that may have contributed to the death [11]. Mood disorders are most frequently associated with suicide [12].
Certain personality traits and coping styles; adverse social, interpersonal and family factors; alcohol and drug abuse and exposure to difficult or stressful life eventsmay all contribute to risk of suicide.
In terms of rural mental health, the 1997 Australian National Survey of Mental Health and Wellbeing found no urban–rural differences in prevalence for affective disorders, anxiety disorders or alcohol or drug dependence [13]. Furthermore, two studies have examined the prevalence of self-reported mental health problems in rural residents. One sampled in rural Victoria and NSW [14], the other in rural South Australia [15]. Both found no association between rurality and reported levels of psychological distress.
Both suicidal ideation and suicide attempts are known to be associated with completed suicide. Using the National Survey data, Pirkis and colleagues [16] found residential location (metropolitan/non-metropolitan) did not differentiate those who reported suicidal ideas from those reporting no suicidal ideas. Similarly, residential location did not differentiate those who made an attempt from those who reported no suicidal thoughts or associated behaviours.
The failure to demonstrate an association between rurality and psychological distress or mental disorder (or both) in these studies is not surprising. A variety of factors, which cannot be captured by broad descriptors such as ‘rural’ and ‘urban’, are likely to be important in the development of psychological distress or disorder (or both). There also may be a range of other methodological issues, such as under-reporting of symptoms, that may result in under-ascertainment of disorders. Furthermore, there may be important within-rural variation of symptoms or disorder that may influence suicide risk. For example, while the National Survey of Mental Health and Wellbeing found no urban–rural difference in prevalence of substance use disorders, the 2001 National Drug Strategy Household Survey [17] found that a higher proportion of people living in rural/remote areas drank at risky/high-risk levels. These different patterns of drinking may differentially affect suicide risk. In summary, a variety of factors must be considered when trying to explain urban–rural differences in suicide rates.
The role of place and context in suicide
While numerous studies have investigated the rural– urban differences in suicide rates [4–9], there has been less research examining the mechanisms that underpin these variations. One area of research that may provide some insight is the study of health and place. Over the past decade, there has been renewed interest in the role of place in shaping people's health experience, and studies have attempted to investigate whether differences between geographic areas in morbidity and mortality are due to the composition of the resident population or to features of place. Arecent reviewby Picket and Pearl [18] found a modest but consistent effect of place on health after controlling for compositional differences across a diverse range of studies.
Various research approaches have been applied in conceptualizing the effects of place on health. For example, Catalano and Pickett [19] describe three categories of mechanism through which spatial variations in health outcomes may occur: (i) environmental hazards; (ii) resources available to help individuals cope without exhibiting symptoms and (iii) tolerance of society for coping mechanisms. The latter includes factors which lead to assignment or adoption (or both) of the sick role and help-seeking behaviours.
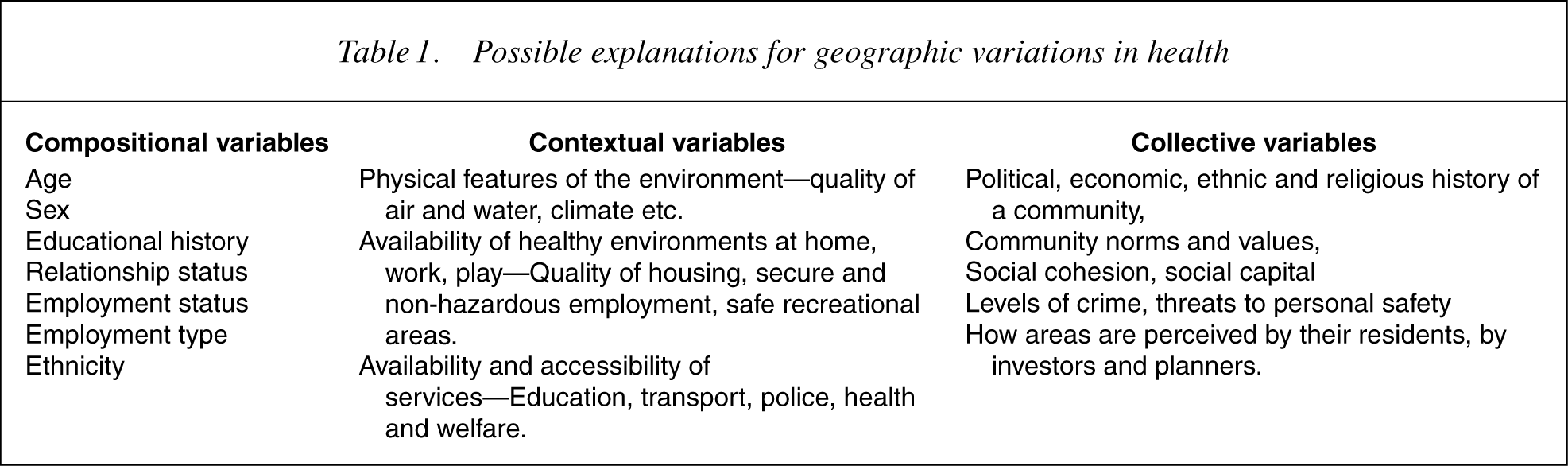
Another approach has been adopted by Macintyre and colleagues [20], who also have suggested three types of explanation for geographical variations in health: contextual, compositional and collective. Contextual explanations focus on the special characteristics of rural areas and examine opportunity structures in the local physical and social environment. Compositional explanations derive from the characteristics of individuals resident in particular places. Collective explanations are concerned with sociocultural and historical features of communities. Table 1 lists variables commonly considered in each of these categories [21]. To use marijuana abuse as an example, areas may exhibit high rates of poor mental health because marijuana is readily available (contextual). They may also contain many individuals whose personal characteristics predispose them to smoke marijuana (compositional). In addition, local norms and traditions may be tolerant of marihuana use (collective). Clearly, there is some overlap, particularly as the distinction between composition and context may not always be conceptually clear, nor are collective explanations always totally separate from contextual ones.
Possible explanations for geographic variations in health
Macintyre and colleagues [20] have focused on the contextual and collective aspects in their attempts to identify features of local areas that might be health promoting or health damaging. This approach can readily be applied to the exploration of possible explanations for geographical variation in suicide rates.
Contextual explanations
Contextual or area effects are defined as communitylevel variables that are associated with individual health but are independent of association at the individual level (composition). While contextual effects have been demonstrated for a range of physical health outcomes, their association with mental health outcomes has been more rarely studied [18]. The elevated rates of suicide in small rural inland towns (population < 4000) provide an interesting example of how changes in context correlate with changes in the suicide rate. As already described, these towns have very high rates of suicide, which have been steadily increasing over the last 20 years. Concurrently, these areas have experienced significant social and economic change, including significant population decline, which commenced three decades ago. These changes have included a dramatic fall in land values [22] and widespread drought [23], the need for farms to become larger, resulting in fewer farms [24], reduced employment of paid labour [25] and increasing centralization of public and private sector services (health, education, financial) [26]. This process of decline in rural areas has led to out-migration (particularly of the young and educated) and in some cases the ‘entrapment’ of older people or those without the resources to relocate, who are unable to sell their properties at a price that would allow movement to more prosperous areas [23].
In some instances, the loss of infrastructure and public amenities such as schools, hospitals and banks has had a social and collective psychological impact on a town's remaining residents [26, 27], reducing the sense of cohesion and community participation of inhabitants [28]. Those who have left these areas are more likely to be better educated and have greater job prospects [29]. Persons who have moved in to towns replacing residents who have left tend to be from low-income groups [30], and are attracted by depressed rural property prices and lower costs of living [31].
At this point in the discussion, it is important to note that ‘rural’ is a heterogeneous concept. While as described above, some rural areas may have been negatively affected over the last three decades, others, such as coastal and picturesque rural settings in close proximity to major urban centres, have prospered. More careful examination of the spatial variation of suicide could reveal differences between declining and prospering small rural towns.
It may be postulated that these important contextual and collective factors could be significant in explaining the elevated rates of suicide in certain rural areas. For example, Fraser et al. [32] examined how population growth and decline as an indicator of changes to social, economic and physical characteristics of a town was related to self-reported mental health in rural settings. The study demonstrated that living in a declining area was associated with greater psychological distress and less satisfaction with life.
In a similar vein, a recent study demonstrated that area deprivation was associated with an increased 12-month prevalence rate of mood disorders after adjusting for individual socioeconomic status [33]. An additional study found that income inequality, another population characteristic, was associated with common mental disorders [34]. This was particularly so for those participants with the highest incomes within their region of residence.
Other studies [35–37] have demonstrated higher suicide rates in areas of socioeconomic disadvantage as measured by the proportion of persons of low income, low education and high unemployment living in an area. Cantor and colleagues [37] found that the relationship between area socioeconomic disadvantage and suicide rate was greater in males than females, and that area socioeconomic disadvantage was associated with the greatest variance in suicide rate among those aged 30–54 years. This group's finding of lower suicide rates in some rural areas such as Darling Downs and Mackay [8] appears consistent with, but perhaps not fully explained by, this association with area socioeconomic disadvantage.
One possible explanation for these findings may be that for some rural residents the sudden and unexpected changes in social and economic positionmay leave the individual unable to cope—‘anomic suicide’ [38]. In addition, those who are left in declining areas may experience a feeling of ‘entrapment’. Limited education and employment opportunities, and other social pressures may lead to a sense of powerlessness, loss of hope and few or no options for the future [39].
Service utilization, which may reflect service availability and accessibility, is another important contextual factor to consider. Parslow and Jorm [40], using information collected through the National Survey of Mental Health and Wellbeing [13], examined factors associated with utilization of mental health services. Important regional variation in service utilization for mental health problems was shown. While living in a rural or remote location was not significantly associated with utilization rates of general practitioner services, those in remote locations (population <10 000) had lower levels of utilization of specialist mental health services compared with more populous regions.
Pirkis and colleagues [41] shed further light on this issue. Again using the National Survey data, they examined the extent to which suicidal ideation and suicide attempts are correlated with service use. In a multivariate analysis, after controlling for a range of potential confounders, suicidal ideation, not surprisingly, was significantly associated with use of mental health services. Of importance, people with suicidal ideation living in nonmetropolitan areas (population ≤100 000) were less likely to make use of services. This finding may reflect the lesser availability of these services in such areas, thus potentially placing inhabitants with mental health problems or those in crisis at risk.
Caldwell et al. [10] again using the National Survey data looked at prevalence of mental health disorders in metropolitan and rural areas and compared the use of professional help by residents of those areas. They found that in non-metropolitan areas (population ≤100 000), of those who met criteria for a mental disorder, a smaller proportion accessed professional help than in metropolitan areas. The differencewasmostmarked for males aged 18–29 years (25.2% vs. 11.4%, p < 0.05).
Taken together, these studies raise important questions. Less service utilization may reflect less availability and accessibility of services, an important contextual issue that may contribute to variation in suicide rates. It may also be due to other factors such as poor mental health literacy, or greater concern about stigma and discrimination and so less willingness to seek help. Whatever the mechanism, the findings that elevated rates of suicide in rural areas particularly affect young males, and that nonmetropolitan males in the age group of 18–29 years are those who are less likely to seek help, cannot be ignored. Further evidence of differing patterns of service utilization between urban and rural residents in Australia comes from studying general practitioner service use for mental disorders. Using data from three sources, namely the Bettering the Evaluation and Care of Health (BEACH) program data, Medicare data and the Pharmaceutical Benefits Scheme data, Caldwell and colleagues [42] found the rate of psychological problems managed by GPs per 1000 population was far less for residents of large rural (population 25 000–90 000), small rural (population 10 000–24 999), other rural (population<10 000) and remote areas than capital cities. In addition, mental health medications were less frequently prescribed for residents of small rural, other rural and remote areas than capital cities. GPs managed less depression problems per 1000 population among residents of other rural and remote areas (i.e. rural areas of population <10 000), and less anxiety problems among all rural and remote compared with metropolitan residents.
These findings raise important questions. The lower rate of management of psychological problems by general practitioners in rural areas may reflect a lower rate of recognition or treatment of psychological problems. Alternatively, rural general practitioners may adopt different approaches to management, or may be able to provide fewer follow-up consultations. The lower number of encounters per 1000 population where depression is managed in smaller rural centres and where mental health medications are prescribed for residents of these areas suggests higher levels of unmet need in these areas. While the reasons for lower service utilization among rural residents are not evident, the effects of this, particularly with respect to a possible contribution to the elevated rural suicide rate, are of concern.
Compositional explanations
As has been shown above, there appear to be contextual differences between urban and rural areas and within rural areas that may impact on suicide rates. Compositional differences between geographical areas may also contribute to differences in the rate of suicide. At an individual level, the demographic and socioeconomic correlates of mental disorders and suicide have been well described. In summary, the prevalence of mental disorders is generally greater in individuals who are unemployed, of lower social class or have limited educational attainment [34, 43]. Australian studies have shown that suicide [44] and suicide attempts [16] are also more common among the unemployed, and suicide ismore frequent in those with socioeconomic disadvantage [37]
Using the National Survey of Mental Health and Wellbeing data [13], an association has been demonstrated between socioeconomic status and reported mental disorders [13, 45] and suicide attempts [45, 46]. Taylor et al. [36] found a significant relationship between socioeconomic status relationship and suicide attempts after adjusting for mental illness, suggesting a direct (and independent) relationship between status and attempts [45]. These investigators have suggested that mental disorder and suicide attempts should be regarded not only as individual phenomena but also as a consequence of material life circumstances, which may be more challenging for those at the lower end of the social spectrum.
While intra-regional variation exists, rural residents are on average of lower socioeconomic status, older and sicker, and experience higher rates of unemployment compared with urban residents [47]. This is a significant finding, which must be taken into account when attempting to understand the increased rate of suicide in rural residents.
The combination of individual socioeconomic hardship and area-level socioeconomic disadvantage as previously described seems particularly relevant when examining the elevated suicide rates in smaller rural towns.
Another compositional factor that may be of significance in studying rural suicides is particular population groups in rural areas. Two recent studies have looked at such groups. The first looked at migrant groups residing in rural areas. Morrell et al. [48] studied urban and rural suicides among migrants in NSW. When country of birth was taken into account, different patterns of risk were demonstrated for younger versus older males. For older males, most of the increased risk of suicide associated with non-metropolitan residence was due to the relatively high migrant suicide rates in these regions. By contrast, in younger males the excess risk associated with living in rural areas was not related to country of birth.
The second study examined suicide rates among farmers, farm managers and agricultural labourers [49]. Over a 10-year period (1988–1997), 921 suicides were identified. Two-thirds of these were farm managers, half of these occurred in the <55-year age group. Agricultural labourer suicides were more often (62%) in the 15–39- year age group. Age adjusted rates for farm managers ranged from 24.8 to 51.4 per 100 000 and for agricultural labourers from 23.8 to 41.9 per 100 000. The elevated rates found in this study are consistent with studies from several other countries, which have also demonstrated high rates of suicide among farmers [50–55]
These two studies highlight the complexity of the factors that may account for variable suicide rates. Both show that young males in these particular population groups living in rural areas have elevated rates of suicide. However, both also offer a reminder that it is not only young males living in rural areas who are at increased risk, and thus, it is unlikely there is a single or simple explanation for the elevated rural suicide rate. For example, a range of factors have been proposed to account for the high rates of suicide reported for farmers, including mental illness [53], physical illness [56], financial and business-related problems [53, 57], reluctance to seek help [58], ready access to lethal means [53], a more functional attitude toward death [59] and loneliness and isolation [60].
While rates of self-harm and suicide are known to be substantially higher among indigenous groups when compared with other Australians, Cantor and Slater's [8] study of suicide in Queensland from 1990 to 1992, which demonstrated a high suicide rate among Aboriginal and Torres Strait Islander males aged 15–29 years, did not show, however, a higher rate in rural indigenous residents. Similarly, Clayer and Czechowicz [61] in an examination of South Australian Coroner's records for the period 1981–1988 found an increase in Aboriginal suicide rate over the non-indigenous population by a factor of six. However, the rural Aboriginal suicide rate was slightly less than the urban rate.
These are interesting findings and again demonstrate the need for further research into whether unique factors in rural locations are protective against indigenous suicide.
Collective explanations
Collective effects encompass sociocultural and historical features of communities such as shared legal and moral norms, traditions, values and interests. These include psychosocial constructs such as social cohesion and social capital in addition to ethnic, regional and national identity, shared histories, religious affiliation and political ideology [20].
For example, in some cultures, men are taught that power, dominance, competition and control are essential to proving one's masculinity [62]. Thus demonstration or perception of vulnerability, overt expression of feelings and displays of emotions are to be avoided. For different reasons in certain cultures, such as many Asian cultures, emotional control is valued and emotional expressiveness is perceived to be an undesirable trait. This is also exemplified by the traditional stereotypic characterization of the ‘Aussiemale’. Thismale sex-role stereotyping and the ideology of self-reliance is frequently seen in rural areas [63] and may present substantial barriers to help-seeking behaviours for rural males in crisis or turmoil.
Never admit the pain
Bury it deep
Only the weak complain
Complaint is cheap
Cover thy wound
Fold down its curtained place
Silence is still a crown
Courage a grace
‘Never Admit The Pain’—Dame Mary Gilmore (1865– 1962).
Although much is assumed and taken as folklore, there is limited empirical data describing the knowledge and attitudes of rural and remote people about mental health problems, services and treatments. Rost et al. [64] in a study in the USA found that stigma in rural communities was a much stronger deterrent to seeking mental health care than in urban residents. The authors attributed the effect in rural areas to a lack of anonymity when seeking help, but lacked empirical data to support this belief.
In Australia, Wrigley and colleagues [65] studied attitudes toward seeking help for psychological problems among rural residents. The study was conducted in Echuca, a rural town of approximately 10 000 people in Northern Victoria. They found that higher perceived stigmawas associated with more negative attitudes toward seeking help. However it was not associated with less willingness to discuss mental health issues with a general practitioner. Causal attributions were also predictive of attitudes toward seeking psychological help. In particular, greater perceived belief in weakness of character as a cause of depression was associated with more negative attitudes toward help seeking.
Perceived weakness of character as a predictor of negative attitudes toward help seeking could be seen as consistent with the male rural stereotype. However, it is of interest to note that the Wrigley and colleagues [65] sample was made up of two-thirds females and only one-third males. Furthermore, gender did not predict attitudes toward seeking professional psychological help or whether respondents would feel comfortable discussing mental health issues with their general practitioner.
These findings are of considerable interest. Wrigley and colleagues [65] demonstrated that while members of the general population hold negative attitudes toward help seeking, these do not necessarily act as a barrier to seeking help, at least from a general practitioner. This is of particular importance in rural areas where general practitioners are usually the first, and often the only, provider of mental health treatment.
The possession and use of firearms in rural communities is a significant factor that must be explored when looking at contributory factors in rural suicide. Firearms are an immediately lethal method of suicide that usually does not allow the possibility of resuscitation or second thoughts. Owning and using firearms is more common among rural residents compared with their urban counterparts. In rural communities attitudes to death may be influenced by frequent experiences with sick and injured animals, and firearms are commonly part of dayto- day experience. The use of guns is also part of rural folklore and male culture. Thus, with such desensitization perhaps, it is not surprising that firearms are often the chosen means of suicide by rural residents [3]. In their 1997 publication, Dudley and colleagues [4] reported that firearm suicide rates for males aged 15–24 had risen inmetropolitan areas and large cities from 1964 to 1988 but declined a little from 1988–1993. By contrast, rates of suicide that involved firearms rose steadily from 1964 to 1993 in towns with population <4000. The greatest proportion of deaths in those locations was by firearms.
Perhaps coinciding with changes in community attitudes to firearm ownership (and prescriptive requirements for safe storage of guns) throughout Australia, a later study [9] reported that rates of suicide in those aged 15– 34 involving firearms had fallen two- to threefold between 1988 and 1997. This decrease was seen for both males and females, and these declines were most marked in non-metropolitan settings [9]. Nevertheless, firearm suicide remained much more common among those living in non-metropolitan (population ≤20 000) than metropolitan areas.
The role of firearms in rural suicide deaths is further demonstrated in a study of farmer suicides by Page and Fragar [49]. Firearms accounted for 51% of all male farm suicides, compared with 23% for the wider Australian male population for the same period (1988–1997).
An interesting proposition has been put forward by Cantor and Slater [8], who have suggested that without the greater availability and acceptability of firearms in rural areas the overall rural rates might be lower than in urban areas. These authors propose that firearms and other methods of suicide, such as usage of carbon monoxide gas, drugs and poisons, are not interchangeable. The authors imply that if the means are not readily available, deaths may not occur. However, addressing the role of firearms in suicide in rural areas may not be straightforward. In addition to the their important role in folklore and male culture, firearms have an accepted role for controlling pests such as rabbits and foxes in rural areas, as well as putting down injured or sick stock on farms.
Conclusion
Suicide is still a relatively rare event, but its impact on families, friends and society in general is enormous. As with all uncommon events, and especially when the main person in the tragedy of suicide is not available to give information, the causes for a particular suicide episode, and the understanding of this phenomenon in general, remain speculative and imprecise.
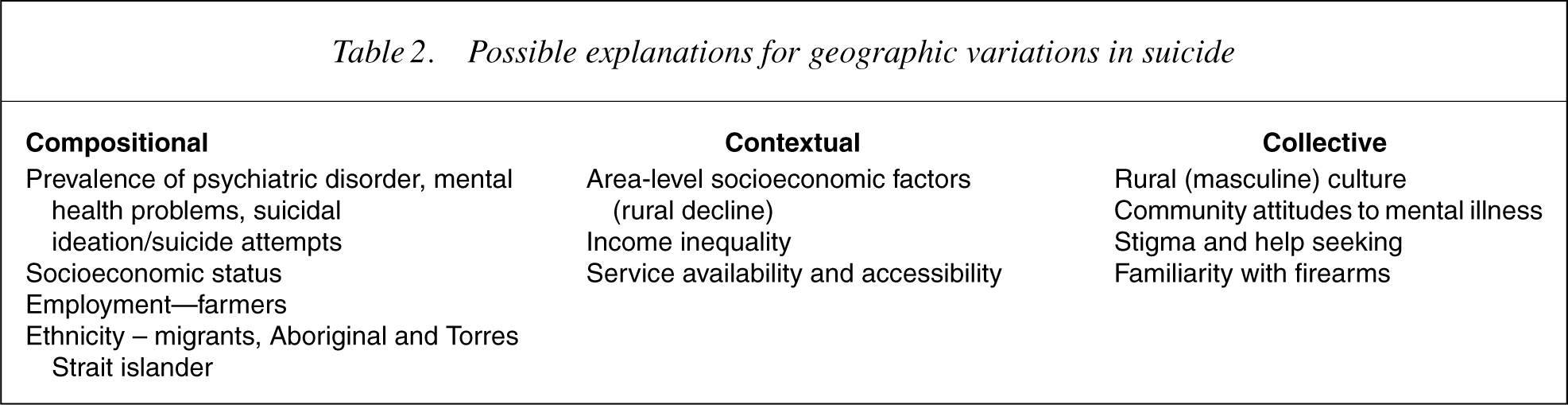
This paper has attempted to look at available literature that has focused on suicide in rural areas. While mental illness of various types is known to be strongly associated with suicide attempts and completed suicide, the available evidence suggests that mental illness in rural areas is not appreciably higher in rural communities compared with large urban populations. However, young males living in very small rural locations are clearly at much greater risk of dying at their own hands than their urban counterparts. The possibility has been raised that place may be an important factor in explaining suicides in this group. An explanatory model looking at the variables of composition, context and collective social factors in suicide has been put forward as one way in which a better understanding of suicide in defined geographical areas may be evaluated and studied (see Table 2).
Possible explanations for geographic variations in suicide
The data examined suggest that living in a declining area has a negative effect on mental wellbeing (it does not seem to be productive of increased rates ofmental illness) but rural decline over the last two decades has not been uniform, which makes generalization difficult. There is evidence of less health service utilization in certain rural areas, possibly due to poor service availability, lack of access, or community or cultural attitudes to illness and help seeking. Stoical young rural males may be particularly at risk of not seeking help for problems when they arise, and with the ready availability of a lethal method of self-harm by way of accessibility to firearms, a higher likelihood of taking one's life in this way may not only be postulated, but is supported by available evidence.
While there has been considerable effort in recent times to highlight the problems of depression and other mental illnesses that have been hidden or neglected for far too long, this literature review points to a broader focus of effort looking at the contextual and collective characteristics of communities that may hinder assistance to those in turmoil and distress. Beneficial results accruing from campaigns or interventions targeted to these factors could be reasonably expected.