
Abstract
Given the considerable impact substance use problems and mental health disorders have on each other, an understanding of their prevalence in particular settings is essential for service planning, clinician training and skill mix, and for organizing the way in which services relate to each other [1]. Much has been written about the general principles of identifying and managing people with a coexisting mental health disorder and substance use problem and increasingly, the nature of specific combinations of disorders is starting to be understood. The heterogeneity of these combinations, and the impact of different systems of care in different places, means that localized descriptive data are needed to optimize treatment. There is a lack of consistency between the studies of prevalence rates that have been published to date, making generalization of findings to other settings difficult [2]. Such variation may be due to a range of factors, including regional differences in illness prevalence, study design and variations in service entry criteria.
Data from the Australian National Survey of Mental Health and Well-Being showed that having a current substance use disorder significantly increased the probability of having a coexisting mood or anxiety disorder [3], with such combinations associated with greater disability than any one diagnostic category alone [4]. In total, 46% of women and 25% of men with a current substance use disorder also met criteria for an anxiety or mood disorder, with approximately one in seven of those with a substance use disorder seeking professional assistance for that problem during the survey year [5].
Rates of coexisting psychiatric disorders have typically been found to be high in substance treatment settings [6–8]. For example, a UK study found high rates of mental disorder in patients treated in alcohol and other drug (AOD) services, with 85% of those attending alcohol services and 75% of those attending drug services having a coexisting non-AOD psychiatric diagnosis [7]. Rates of non-substance-induced psychotic disorders were relatively high (19% in alcohol services and 8% in drug services), though the prevalence of bipolar disorder within this group was surprisingly low (5% and 1%, respectively), while rates of severe anxiety disorder (32% and 19%, respectively) and depression (81% and 67%, respectively) were also notable. Furthermore, significant rates of pathological gambling, of between 7% and 15%, have been identified in substance treatment settings [8].
There are no published studies of prevalence rates of mental health problems in outpatient AOD settings in New Zealand. Two studies undertaken in the 1980s examined rates of psychiatric comorbidity amongst patients in residentialAODtreatment programs. The first reported that 95% of their sample were found to have a coexisting psychiatric condition [9], while the second estimated that one third were depressed [10].
There is also little data on utilization of mental health services by AOD patients in New Zealand other than the finding that 22% of alcohol treatment patients in a 1980s sample had received past psychiatric treatment [9]. In the UK sample described above over one-fifth of AOD patients had been in contact with community mental health teams in the preceding month, with a similar proportion having contact with a psychiatrist within the AOD service, while a quarter had mental health related contact with a general practitioner [7].
New Zealand is fortunate in having governmentfunded specialist Community Alcohol and Drug Services (CADS) which are generally consistent with respect to their service structure and assessment approaches. These services often form the front door to other treatment services allowing some degree of generalization to be made between them. This paper aimed to explore prevalence rates of coexisting psychiatric disorders in people presenting to CADS units serving two typical larger cities, and to measure rates of mental health service utilization.
Method
Participants
Participants were initially drawn from two outpatient governmentfunded specialist CADS in the cities of Hamilton and Christchurch. The aim was to recruit a representative treatment-seeking adult sample, and for this reason exclusions were kept to a minimum. Patients were excluded if they were aged less than 17 years or were deemed too psychiatrically unwell or cognitively impaired to understand and tolerate the interview procedure. Patients serving a term of imprisonment at the time of assessment were also excluded as this would have markedly affected pattern of recent substance use. Finally, subjects were excluded if they lived more than 50 km from the clinic to avoid unrealistic burden on patients and interviewers with respect to travel time and cost.
Design and procedure
Recruitment
Recruitment at both CADS sites involved identification of all patients presenting for treatment and then selecting a subset using a random number list. Early in the recruitment phase it became apparent that recruitment rate was lower than anticipated in Hamilton and so it was necessary to select all new patients for potential recruitment at this site. Recruitment was carried out by designated research clinicians who were current clinical staff at the participating clinics. Recruitment occurred as a combination of direct approach, letter and phone call, and where necessary, invitation via casemanager.
Interview
DSM-IV axis I diagnoses were generated using the computerized Composite International Diagnostic Interview (CIDI-Auto) [11]. The CIDI allows for the selection of a combination of individual modules. For this study, the sections utilized were phobic disorders (specific phobias, social phobia, agoraphobia, panic disorder), depressive disorders (including dysthymia), bipolar disorder (bipolar I only), eating disorders, alcohol use disorders, substance-related disorders (excluding alcohol and tobacco), obsessive–compulsive disorder (OCD) and posttraumatic stress disorder (PTSD). The CIDI does not diagnose substance-induced disorders, only counting psychiatric symptoms which the patient does not attribute solely to substance use. As we were interested in the rate of substance-induced mood disorders, interviewers were instructed to complete themood disorder sections for patients who reported that their symptoms were always the result of substance use, and to make a record of this deviation from the usual protocol.
In addition to the CIDI, DSM-III-R diagnoses of conduct disorder and antisocial personality disorder were made using the corresponding sections of the Diagnostic Interview for Genetic Studies (DIGS) [12]. The South Oaks Gambling Scale (SOGS) [13] was used to identify extent of current pathological gambling, with this instrument showing a high correlation and good sensitivity and specificity in identifying DSM-IV pathological gambling in clinical samples when a cut-off score of five or more is adopted. Finally, past 6 months AOD use was recorded using a modified timeline follow-back procedure (TLFB) [14], with responses confirmed by a nominated collateral informant.
Results
In total 62 patients were recruited from CADS Christchurch and 43 from CADS Hamilton. The 105 patients interviewed for the study represent a 25.1% recruitment rate, with 15.3% of target patients declining to participate, and the remaining 59.5% designated as ‘failed to recruit’, in that contact was unable to be made. This rate was seen as a reflection of the ‘naturalistic’ nature of the study as patients were not recruited and interviewed as part of their standard care, nor were they being offered a specific treatment contingent upon cooperation as might occur in a randomized controlled trial. The absence of more extensive exclusion criteria also meant that the target population contained persons with higher levels of social and psychiatric instability than would normally be tolerated in a clinical study.
A minimum dataset was maintained throughout the recruitment phase to gather basic information about those not interviewed. An analysis of these data revealed that those who were interviewed were older, less likely to be Maori, and less likely to be presenting for an alcohol-related problem than those not interviewed. An algorithm was derived which weighted all interviewed participants to represent the true distribution across these three variables for the whole target population. All figures are presented in their adjusted form.
The samples were mostly New Zealand European/Pakeha (71%), and 19% were Maori. The majority were male (68%), with a mean age of 32.7 years (SD=10.6, range=17–71). Only a quarter were married or in cohabiting relationships (27%) and less than a quarter were currently employed, comprising both full-time (15%) and part-time work (7%). Educational level was on average 10.5 years (SD=2.0, range=3–18), 1.5 years short of completing high school, with 28% of the sample reporting 9 or fewer years education, indicating school departure prior to completion of Fifth Form/Year Eleven, when the first national secondary qualification may be gained in New Zealand.
A wide range of DSM-IV substance use disorders were present in the sample, as displayed in Table 1, with pathological gambling included as a behavioural addiction. The most prevalent current diagnoses were alcohol dependence and cannabis dependence, while between 14% and 20% of the sample had a current diagnosis of opioid, sedative, or amphetamine dependence. Forty per cent of the sample met criteria for more than one current substance use disorder, with this rate rising to two-thirds for lifetime diagnoses. Onset age of substance dependence was typically in the early twenties.
Substance use and pathological gambling diagnoses in an alcohol and other drug outpatient sample(n = 105)
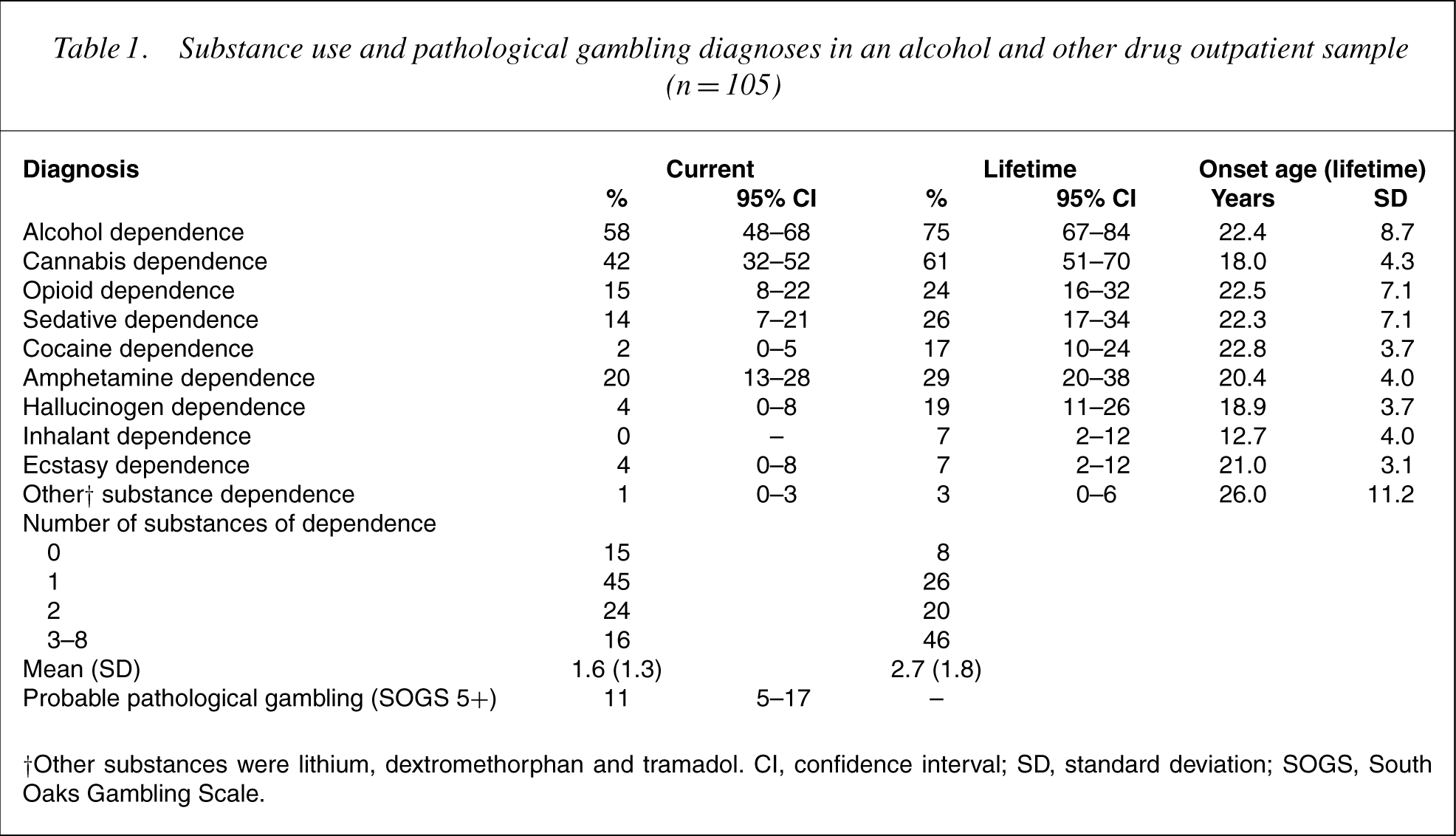
†Other substances were lithium, dextromethor phan and tramadol. CI, confidence Oaks Gambling Scale. interval; SD, standard deviation; SOGS, South Oaks Gambling Scale.
The substances with the highest prevalence of any use in the past 6 months were alcohol (91%), cannabis (64%), stimulants (34%), hallucinogens (26%) and sedatives (18%). In the preceding 6 months substances were used on 68% (SD=33) of non-institutionalized days. Substances were reportedly used every day by 37% of the sample, while 3% of the sample reported use on less than 10% of non-institutionalized days.
In addition to the substance dependencies revealed in Table 1, 73% of the sample reported currently smoking tobacco on a daily basis, while a further 12% had been daily smokers in the past. Identifying probable nicotine dependence as being present in all patients who reported daily use of five or more cigarettes would indicate a probable current nicotine dependence rate of 71% (95% CI=62– 79) and a probable lifetime nicotine dependence rate of 82% (95% CI=75–90).
Current and lifetime psychiatric diagnoses other than substance use disorder or pathological gambling are common and varied, as shown in Table 2. Coexisting axis I psychiatric disorders are the norm for both current (74%) and lifetime rates (90%). Current substance use disorder, mood disorder and anxiety disorder were simultaneously present for 38% (95% CI=28–48%) of the sample. Three axis I diagnoses were present in approximately 30% of the sample (major depressive disorder, social phobia and PTSD) while three further diagnostic groups had a prevalence of approximately 20% (specific phobias, agoraphobia and OCD). The high rate of OCD warranted further investigation. Of the 23 patients diagnosed with OCD, 15 reported obsessive thoughts of harming others, with seven of these also reporting a range of compulsive behaviour. As with substance use disorders, age of onset for psychiatric diagnosis was usually between the late teens and early 20s, with notably earlier mean onset age for specific phobia (8.0 years), social phobia (11.9 years) and panic disorder with/without agoraphobia (13.8/13.6 years).
Mood, anxiety, eating, conduct and antisocial personality disorder in an alcohol and other drug outpatientsample (n = 105)
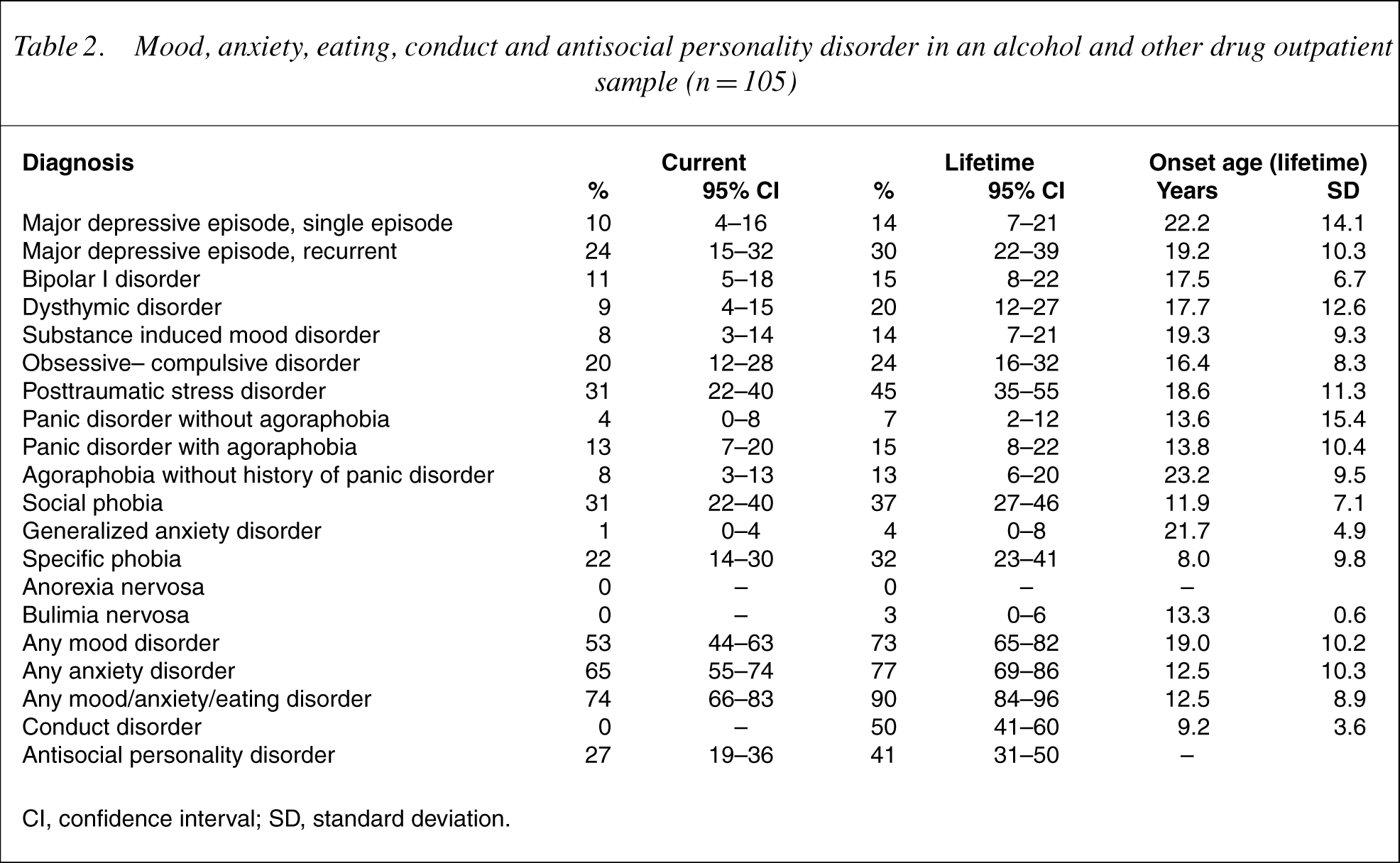
CI, confidence interval; SD, standard deviation.
Mental health service utilization is shown in Table 3. Fewer than 10% reported current outpatient or recent inpatient mental health service involvement. For lifetime inpatient psychiatric admissions, 10% reported one admission and 8% reported two or more admissions. The rangewas 1–14, with amean 2.5 admissions (SD=2.7). Approximately one-third of patients reported a current prescription of psychiatric medication, largely accounted for by the prescribing of antidepressant medication.
Mental health service utilization by an alcohol and other drug outpatient sample (n = 105)
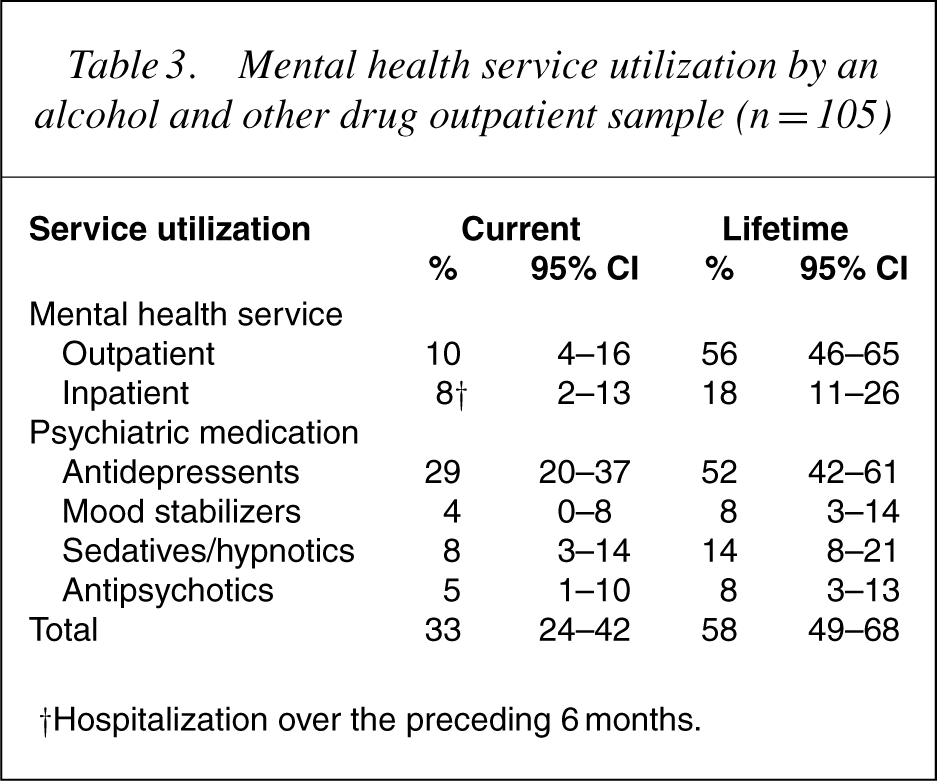
†Hospitalization over the preceding 6 months.
Discussion
This is the first systematic diagnostic survey of a representative outpatient AOD treatment sample in New Zealand. In total 28 axis I and II psychiatric diagnoses are presented in Tables 1 and 2 (including nicotine dependence as referred to in the accompanying text). The three most prevalent disorders are substance-related disorders (nicotine, alcohol and cannabis dependence, respectively). This is not surprising given the population from which this sample was drawn. The five next most prevalent diagnoses are all non-substance related disorders (major depressive disorder, social phobia, PTSD, antisocial personality disorder, and specific phobia). This highlights not only the high rate of coexisting psychiatric disorder per se in this sample but also the prominence of disorders other than substance use disorders on a diagnosis-by-diagnosis basis.
Of the coexisting psychiatric disorders diagnosed, particular heed should be paid to the rates of social phobia, PTSD and bipolar I disorder. Social phobia and PTSD, when presenting concurrently with a substance use disorder, are likely to be significantly entwined with the substance misuse, as there is evidence that substances may be used to manage symptoms for both social phobia [15] and PTSD [16], and that either diagnosis is associated with a more severe substance-related presentation [15, 17]. As a consequence, it has been suggested that disorder-specific interventions may be an important element of successful treatment for these patient groups [17, 18]. Furthermore, we suggest these disorders may present significant difficulties in the delivery of treatment for substance misuse, with group-based treatment programs and self-help groups unacceptable to many socially phobic patients, and to some patients with PTSD, while patients with PTSD may additionally have significant interpersonal issues which, for example, may preclude working with male clinical staff in the case of patients with a history of sexual or physical abuse by male perpetrators.
The rate of bipolar I disorder (11% current, 15% lifetime) is at the upper range of prevalence rates found in a review of nine studies of patients in treatment for substance use problems [19]. The higher rates of bipolar I disorder found in this study may be due to the use of the CIDI, which has been found to identify higher rates than less structured methods [20], and could also reflect a greater tendency for substance using patients with bipolar I disorder to present to AOD rather than mental health services in New Zealand compared to other settings.
It is unclear how many of the cases of bipolar I disorder diagnosed in this study by the CIDI were also diagnosed clinically. Bipolar I disorder and substance use disorders may interact powerfully toworsen the course of each [21–23], and the recognition of bipolar disorder is important to allow appropriate treatment, such as mood stabilizers. Mood stabilizing medication was currently being prescribed to only 4% of patients in this study, indicating that a number of patients with bipolar I disorder were not receiving appropriate medication.
Despite the high level of coexisting psychiatric disorder identified, only a small minority of patients were engaged in treatment at a separate mental health service at the time of undertaking treatment, although close to one-third were being prescribed psychiatric medication, predominantly antidepressants. These figures are comparable to, or somewhat lower than the rates for other recent substance treatment populations [7, 24], while the lifetime rate of mental health service contact is higher than that was found in an earlier New Zealand sample [9]. The low rate of current mental health service engagement suggests that AOD services need to be able to deal with such presentations, by conducting a comprehensive assessment and treatment planning and, where appropriate, engagement with mental health services. These clinical and systems issues have been identified as key barriers to effective treatment for patients with coexisting disorders in New Zealand [1].
The most surprising diagnostic finding was the high rate of OCD, diagnosed in approximately one-fifth of the sample. Rates of OCD in substance misusers have generally been found to be low [25], although two studies [9, 26] have found rates of 13% and 12% respectively in alcoholic treatment samples.
These findings notwithstanding, it is possible that the CIDI may have overdiagnosed OCD in this sample. To minimize false positives in substance misusing populations the CIDI explicitly excludes the diagnosis if ruminations are exclusively in relation to ‘concerns about getting, using, or recovering from drugs or other substances’. The diagnosis of OCD has been found to have the highest inter-rater reliability and concordance with expert diagnosis of the anxiety disorders in an anxiety disorder unit sample using the CIDI-Auto [27]. A CIDIgenerated OCD diagnosis was also found to have moderate test–retest reliability [28].
Examination of the obsessive thoughts reported by those diagnosed with OCD revealed that the majority reported obsessive thoughts of harming others, while none of the obsessive thoughts centred on the most common themes typically found in OCD of fear of contamination, repeated doubts or the need to have things in a certain order [29]. Thus, it would seem that the OCD questions of the CIDI have highlighted high rates of dangerousness, even though this was not the purpose of the interview.
A methodological weakness of the study was the low rate of recruitment (25.1%) which lead to an underrepresentation of Maori, youth and alcohol misusers. However, biases introduced by the low recruitment rate have been identified and corrected for in a rigorous manner, with the sample adjusted to match the profile of the full potential recruitment pool on these variables. These adjusted values are comparable to figures obtained from a national telephone survey of AOD services [30]. Statistical adjustment was only possible for variables that were measured in both samples however, and so it is possible that the recruited sample differed in other significant ways from those not recruited. Furthermore, as a sample drawn almost exclusively from District Health Board (i.e. government-funded mainstream health service) services, it is not clear how well the profile presented here will generalize to patients treated in non-DHB settings. Non-DHB services treat a minority of AOD patients in New Zealand [30] and it is possible that due to being less integrated with other mental health services such patients may be less likely to present with coexisting disorders, and may be less likely to be engaged with mental health services.
Conclusions
Three-quarters of the AOD clinic patients recruited to this study were diagnosed with a current coexisting psychiatric disorder, with 90% of the sample meeting criteria for a lifetime psychiatric diagnosis. This provides strong support for the notion that AOD patients should be considered to be part of the larger population of mental health patients, with coexisting psychiatric conditions the rule, not the exception. This has clear workforce and service delivery implications, supporting the assertion that the AOD treatment workforce in New Zealand must develop an adequate skill base to enable high quality comprehensive assessment and management planning to become routine, and that better integration with wider mental health services is needed in order to maximize treatment outcomes [1].
Footnotes
Acknowledgements
This study was funded by the Alcohol Advisory Council (ALAC) and could not have been undertaken without the support of management and staff at the two participating services. Appreciation is expressed for the hard work of the research clinicians: Naomi Malcolm, Adele Muirhead-Smith, Rosemary Brown and Rada Nedeljkovic.