
Abstract
The mental health of young people in Australia has been an issue of increasing concern over the last decade. It appears that the prevalence of mental disorder in this group is increasing [1] and the prevalence of mental illness among adolescents and young adults is higher than that of Australian adults and older people [2, 3].
Peers are often an important source of support to adolescents in times of emotional distress; female adolescents, in particular, are likely to seek help from their friends [4–6]. Yet very little is known about what, if anything, adolescents do to help each other in times of distress.
There are no studies on this issue with Australian adolescents, but one study examined what adult members of the public are likely to do if they are concerned that someone they know may have a mental illness [7]. This study involved a national household survey of adults aged 18 years or over. Respondents were presented with one of four vignettes; a person with depression, depression and suicidal thoughts, early schizophrenia or chronic schizophrenia. They were asked to say what they would do if the person in the vignette was someone they knew and cared about. The most common responses to the open-ended question, for all four vignettes, were to offer social support and recommend professional help (most commonly by a general practitioner or an unspecified doctor). Some respondents said they would either accompany the person to see a professional (ranging from 8.7% for depression with no thoughts of suicide, to 16.7% for chronic schizophrenia) or contact the professional on their behalf (ranging from 3.0% for depression with no thoughts of suicide, to 15.9% for chronic schizophrenia). The most appropriate responses (encouraging professional help-seeking) were given by women, respondents who had low stigma scores and respondents who correctly identified the disorder described in the vignette.
A small number of overseas studies have been conducted with adolescent samples with a focus on responding to suicidal peers, rather than peers with mental illness or emotional distress. In one such study [8] students were asked if they had ever spoken to a suicidal peer, and if so, what they did in response. Of their initial sample, 68.0% of the females and 42.5% of the males knew a similaraged peer who had attempted or completed suicide. Of those who had spoken to the peer when he or she was suicidal, 63.0% talked to the friend, 24.7% engaged an adult and 12.3% had done nothing.
Dunham [9] investigated first aid responses to a suicidal peer using two vignettes; one where suicidal intent was clearly stated and one where suicidal intent was ambiguous. Studentswere asked what theywould do if the person described in the vignette was a friend of theirs. Written responses were coded into one of four categories; talking with the friend (no adult involvement), engaging an adult (such as a parent or teacher) to help, waiting to see if the situation was serious before doing anything, and doing nothing (ignoring the situation or not taking it seriously). Students were also asked if they had any previous experience with suicidal people. Few students responding to the ambiguous vignette said they would talk to an adult – 14.0% of those with no social history of suicide and 33.0% of those with a social history of suicide (the latter group was more likely to talk to an adult). In the unambiguous scenario, students more frequently said they would tell an adult – 64.0% of those with a social history of suicide and 54.0% of those with no history.
No literature exists describing the response of young people to peers experiencing more common mental illnesses. The present paper reports the steps young people claim they would make to help a friend with depression or conduct disorder.
Method
Participants
The results presented in the present paper represent a small part of a large survey conducted in 2003 in South Australia and the Australian Capital Territory. Students involved in the survey were in years 8 (34.8%), 9 (40.7%) and 10 (24.5%), and 51% were male. Students were enrolled in public or private high schools, and participation required consent from the school principal and each student's parent or guardian. Students completed 1137 usable questionnaires, a response rate of approximately 38%.
Procedure and instruments
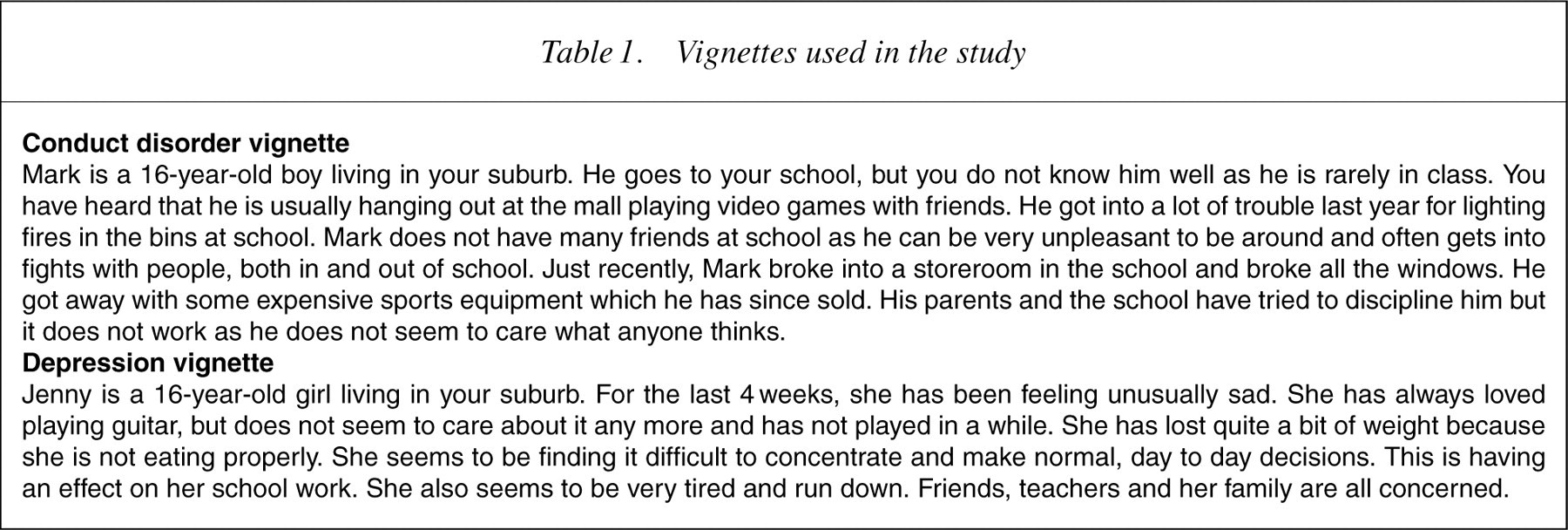
Students were presented with one of two vignettes, one describing a young man meeting criteria for conduct disorder, and the other describing a young woman meeting criteria for a major depressive episode. Vignettes met both ICD-10 and DSM-IV criteria for the disorder described (Table 1). The questionnaire, based on the original instrument by Jorm
Vignettes used in the study
The most common type of step listed was for a young person to provide positive social support for their friend but not discuss it with anyone else. This included both practical help (at school) and emotional support. This type of step is hereafter described as ‘positive social support’.
The second type was to seek further information. Typically, this involved asking for advice from a teacher, parent or school counsellor, looking for information on the Internet or from an unnamed source. This type of step is described as ‘information seeking’.
The third type of step described was ‘passive referral’ to an adult for help, without actively engaging the help of the adult named. Typical examples include suggesting the friend speak to a teacher, parent or counsellor, or a more formal helper such as a doctor.
‘Active referral’ is a step in which the respondent described actively engaging an adult helper. Typically, the step described taking the friend to see the school counsellor, discussing the problem with a teacher, or asking parents to contact the friend's parents. This is generally the most functional strategy available to a young person [9].
The next type of step is labelled ‘distraction’. These steps were generally an enjoyable activity such as shopping, sport or spending an evening out.
Inappropriate steps posed a problem in terms of coding into categories. Some of the inappropriate steps listed were probably not intended to be taken seriously, and some were. A number of respondents wrote that they would purchase marijuana or alcohol for the distressed friend. In some cases, this was probably a joke, but in other cases it was likely that the respondent considered the use of recreational drugs to be an effective coping mechanism in times of stress. Other inappropriate steps listed by respondents were violence. Some of these are probably misguided humour on the part of the respondents, but for others, the use of violence when trying to intervene with someone who is known for violence might seem appropriate.
Violence and recreational drug use made up the bulk of the inappropriate responses, but there was a third kind, best described as manipulation. These included threats to withhold friendship if behaviour did not change, telling the friend to ‘get over it’ and ignoring the problem. Because there is noway to distinguish between an inappropriate helping step which was meant to be taken seriously and one that was not, they were all included in the same category. These are described hereafter as ‘inappropriate help’.
The next step in the coding process was to establish helping styles from the steps. Four exhaustive and mutually exclusive helping styles were identified.
The first style is insular peer support. A student assigned this label listed helping steps which may have included positive social support, passive referral, information seeking and distraction, but no active referral. This was the most common type of helper, representing more than half of the sample.
The second style identified, and the most desirable, was adultoriented helping. A student assigned this label listed at least one active referral step, engaging an adult to help with the problem. This type of helper represented approximately a quarter of the sample.
A very small group listed actions which were likely to be well-meant butwere inappropriate. This group listed mainly stepswhich constituted ‘positive social support’ but also listed one inappropriate step which did not involve violence or recreational drugs.
The fourth type of help is no helper at all. This group either did not list any steps, or listed only inappropriate steps, or referred to violence or recreational drugs. This group was labelled ‘ineffective helpers’.
Statistical methods
All analyses were conducted through logistic regression incorporating gender, grade at school, and an interaction between the two, so that all significance levels are reported after controlling for year group differences. Where a school year by sex interaction was detected, further analyses were undertaken to determine which sex and school year differences were significant. All analyses used SPSS version 12.
Results
Overall, 53.0% of respondents were classed as insular supportive helpers, 23.0% were adult-oriented helpers, 3.5% were inappropriate but well-meant helpers and 20.5% were ineffective helpers.
Students responding to the depression vignette were more likely to describe insular positive social support (58.5% of those responding to the depression vignette compared to 47.6% of those responding to the conduct disorder vignette, p<0.01). Students responding to the conduct disorder vignette were more likely to report an adult-oriented helping style (27.4% compared to 19.1% for depression, p<0.01).
More females than males described an insular helping style (59.7% compared to 46.7%, p<0.01). More females than males described an adult-oriented helping style (28.1% compared to 18.6%, p<0.01).
More males than females described inappropriate but well-meant help (4.7% compared to 2.0%, p<0.05) and more males than females could be described as ineffective helpers (30.0% of males compared to 10.2% of females, p<0.01).
Males did not vary their helping style according to problem type. By contrast, females responding to the depression vignette were more likely to describe a positive social support helping style (67.8%, compared to 51.8% for conduct disorder, p<0.01), while those responding to the conduct disorder vignette were more likely to describe an adult-oriented helping style (35.1%, compared to 21.0% for the depression vignette, p<0.01). There were no significant differences in helping style in different grades at school.
Discussion
Female students were more likely than male students to engage an adult to help when concerned about a friend's mental health. It is of particular interest that male students did not vary their helping style depending on the type of problem described. The females in the sample, however, were more likely to engage an adult to help if the problem being experienced by the friend was behavioural. This may reflect a lack of confidence in dealing with a friend who is unpredictable and at times violent, or a sense that personal safety may be an issue if no adult is involved.
It is of concern that one in five students would take no appropriate actions to help a friend. Some of these young people may involve a distressed friend in recreational drug use, others would do nothing. Some young people may fear that they will worsen a situation by doing the ‘wrong thing’. Others may not care about the distress of a peer, lacking the emotional maturity to empathize.
A limitation to this study is the low response rate. As only those students who returned a consent form were allowed to participate, it is not known whether a more inclusive sample might have yielded different results.
It would be valuable to develop a program of research to examine the experiences of young people responding to distressed peers in the ‘real world’, particularly in relation to common disorders. It would also be beneficial to explore the experiences of young people with mental illness, focusing on the responses they have had from peers in response to their distress.
Footnotes
Acknowledgements
The authors thank Michael Sawyer, Jane Burns and Kevin White for their input into the design and implementation of this survey. They also thank the schools and students who agreed to take part. This research was funded by an NHMRC program grant.