
Abstract
The prevalence and incidence of dementia rise exponentially with age, at least up to age 90 [1]. This exponential rise means that the number of cases of dementia in a population is largely determined by its age structure. It also means that as a population ages, the number of dementia cases will increase disproportionately.
Projections of the future number of dementia cases are useful for service planning and advocacy. Since the mid- 1980s, several projections have been made of the number of dementia cases in Australia. Early work used prevalence rates derived from a single study and combined these with estimates of the future numbers of individuals in various age groups [2]. Subsequent work used rates derived from a meta-analysis of prevalence studies [3],[4]. The last of these projections was made in 1998 using 1995 as the base year.
The purpose of the present study is to produce updated dementia projections for Australia. There have now been several meta-analyses of both prevalence and incidence rates, making it difficult to choose a single set of estimates. A recent study of dementia projections in Europe used average data from several meta-analyses [5]. We have adopted their methodology and applied it to Australia. However, such projections assume that there is no change in prevalence and incidence rates, only a change in the age structure of the population. If there are successful preventive interventions in the future, these will reduce the prevalence and incidence rates and affect the projections. Consequently, we have also made projections under different prevention scenarios, assuming that prevention can delay the average age of dementia onset in the population. These estimates are based on the method of an earlier US study, which modelled the effects of disease delay on prevalence of Alzheimer's disease [6].
Method
Baseline projections
The present analysis is based on population projections for Australia developed by the United Nations (UN) for the period 2000–2050 [7]. The projections were used in preference to those available from the Australian Bureau of Statistics (ABS) because they gave estimates in 5-year age groups up to 95+ years, whereas the ABS projections only estimated up to 85+, and to be comparable to a recent study looking at dementia prevalence in the European region [5]. In these population projections, assumptions were made regarding fertility, mortality and international migration in several projection variants. The present analysis used the main projection (medium variant), which assumes low fertility, normal mortality and normal international migration.
The methodology for calculating prevalence and incidence projections for dementia in the present analysis has been taken from the European study [5]. This study used age-specific prevalence and incidence rates for dementia from eight meta-analyses [8–15] (Tables 1, 2) to estimate future prevalence and incidence projections of dementia.
Prevalence rates (%) of dementia according to meta-analyses
Incidence rates (%) of dementia according to meta-analyses
The method estimated an age- and gender-adjusted prevalence projection across all meta-analyses by first calculating a prevalence projection for each meta-analysis. This was done by multiplying the population projection for each 5-year age band separated by gender with the corresponding age-specific prevalence rate from each meta-analysis. The mean per age band and genders over all studies was then calculated and this was then summed over both gender and all age bands. The projections for both the individual meta-analyses and the overall ageand gender-adjusted projection are reported (see [5] for exact formula).
The same method was used to estimate the age- and gender-adjusted incidence, except that the incidence projections were calculated using the population at risk rather than the population. The population at risk is defined as the population minus the number of prevalent cases.
We also estimated the number of working-age people per person with dementia. As defined by the UN Population Division [7], the workingage population included all people aged 15–64 years.
Projections with prevention
To estimate the effect of interventions to delay the onset of dementia, we first estimated incidence for each gender and 5-year age band. We adopted the exponential function used by Brookmeyer et al. [6]:

Number of prevalent cases in Australia based on different meta-analyses
Number of new dementia cases per year in Australia based on different meta-analyses
We could then assess the likely impact on prevalence of interventions by simple modifications of the incidence function. For example, to simulate an intervention that delayed the onset of dementia by 2 years, we apply the function Ii = α exp[β(Ai − 62)], where Ai is the midpoint of the ith age band, using the estimated values of α, β and the same population and mortality projections. To estimate the impact on future prevalence, we subtract the new projected prevalence from that estimated under the unmodified model, for example, 213 930 in 2010 rather than with themeta-analytic result of 219 200. This is necessary so that the deviations of the model from the meta-analytic data, although small, do not affect the estimated impact.
Results
Baseline projections
The projections of future prevalence are shown in Table 3. In 2000, therewere 171 950 (age- and gender-adjusted mean) prevalent dementia cases in Australia. In the next 50 years, the prevalence of dementia is estimated to rise 241% to 587 650 dementia cases in 2050. As indicated in Fig. 1, dementia prevalence is projected to increase at a much greater rate than both the total population and the elderly population. The reason is that the old–old are the fastest growing age group and also have the highest prevalence rate.
Projected increases in dementia cases, elderly population and total population for Australia, 2000–2050.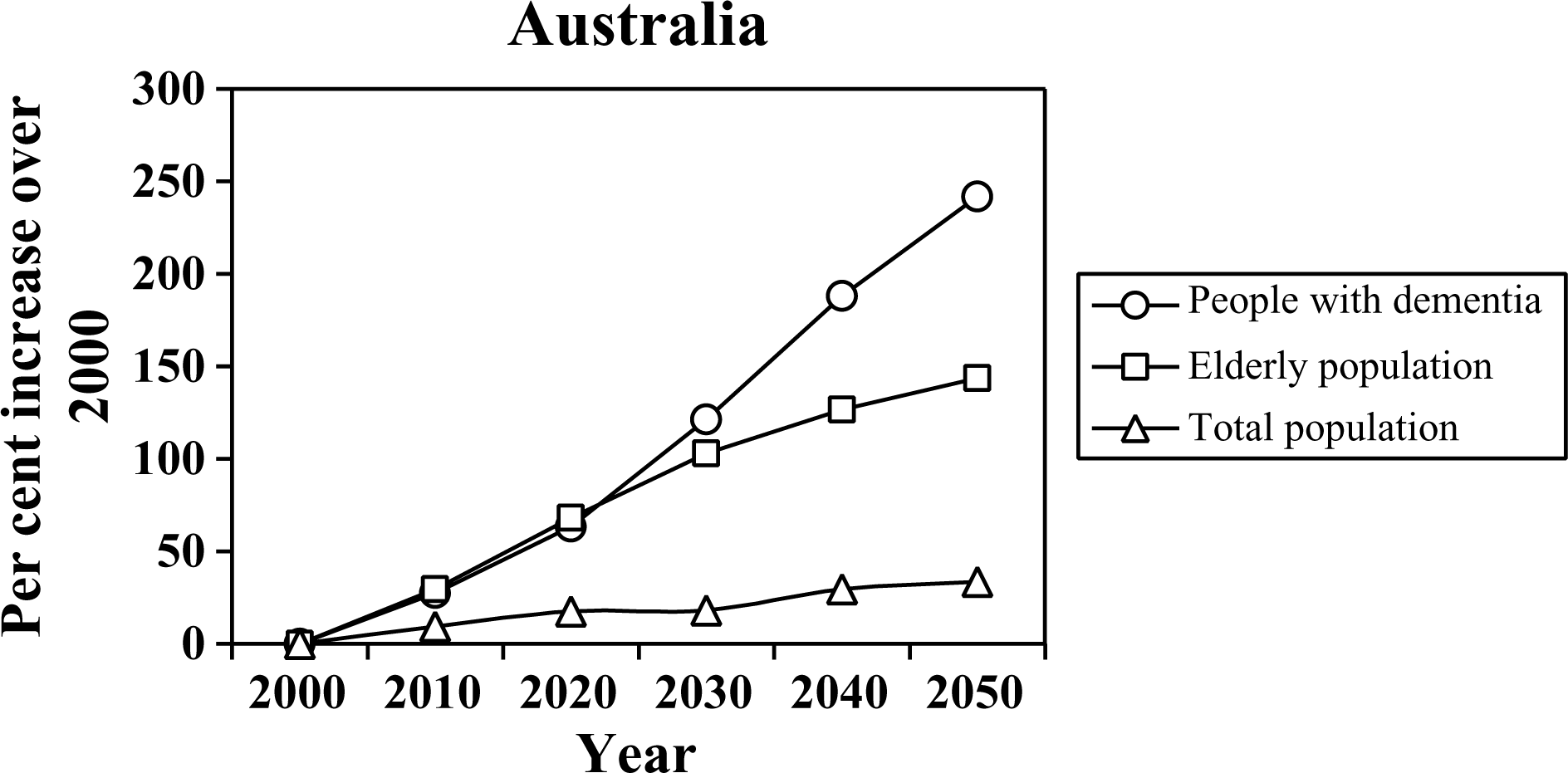
The annual number of new (incident) cases in Australia is estimated to rise from 43 170 new cases of dementia in 2000 to 142 910 new cases in the year 2050 (Table 4). This rise represents an estimated 231% increase in new dementia cases per year in the next 50 years.
In 2000, therewere an estimated 12.87 million people in theworkingage population in Australia. There were also 171 950 people with dementia, which equates to a ratio of 74.84 people in working-age per one person with dementia. Given the ageing population of Australia, dementia prevalence is increasing at a greater rate than that of the working-population, and in 2050, this ratio will be only 26.05 people in working-age per one person with dementia (Table 5).
Working-age population and number of working-age people per one person with dementia (= ratio) in Australia using age- and gender-adjusted mean numbers of prevalent cases
Projections with prevention
The estimated incidence function was: Incidence (% per year)=1.95 exp[0.115(age−60)], with a relative mortality risk of 3.42. This model approximates the projected prevalences and incidences with a root-mean-square relative error of 2.36%.
The likely impact on dementia prevalence of delays in onset of dementia was also calculated. Table 6 shows the projected prevalence of dementia with delays in onset of 0.5, 1, 2 and 5 years. If the age of onset could be delayed by 5 years, there would be 80 800 fewer people with dementia by 2010, and 249 810 fewer people with dementia by 2050. In 2050, this represents a reduction in dementia prevalence of 43.7%. Even delaying the onset of dementia by 6months would have a noticeable impact on dementia prevalence. There would be 10 330 fewer people with dementia by 2010, and by 2050 therewould be 31 920 fewer people with dementia, a reduction in dementia prevalence of 5.6%.
Impact on prevalence of delays in onset of dementia
Discussion
This study has quantified the effects of population ageing on the prevalence and incidence of dementia in Australia and demonstrated that quite modest prevention efforts could lessen this impact.
Projections of this sort make certain assumptions. The first is that the prevalence rates for Australia are close to those of European countries that have provided most of the data on prevalence. What limited data we have from Australia confirms that rates are not dissimilar to those in Europe [16]. Second, the method relies on the accuracy of the UN projections for the population. Population projections make assumptions about birth rates, immigration and mortality. However, for older age groups, birth rates are not an issue because the elderly of 2050 have already been born and can be counted. Similarly, immigration assumptions are unlikely to have much effect on estimates of older age groups. The key assumption ismortality. For example, if an emerging disease were to greatly increase mortality in younger age groups and fewer survived to older age groups, this would affect the present projections.
The present projections have been for the dementia syndrome rather than for Alzheimer's disease or other diseases causing dementia. This is in contrast to a recent study by Access Economics that examined projections for Alzheimer's disease specifically [17]. The reason for the broader focus on dementia is that in the very elderly there are often multiple diseases summating to cause dementia and it becomes difficult to attribute the dementia to a single disease state [18]. Another reason is that Alzheimer's disease and vascular dementia were formerly thought of as involving separate mechanisms, but this is now being questioned, with vascular factors thought to play some role in Alzheimer's disease [19]. Finally, the social impact of various dementing diseases is similar, so that it is the total burden that is important rather than the diseasespecific burden.
Our statistical model estimates that delaying onset by even a few years can have an impact on future numbers of dementia cases. How realistic is the assumption that dementia onset can be delayed? There is presently no strong evidence that dementia can be prevented, but there are some promising leads, with a number of preventive trials either underway or recently completed. Potential interventions include anti-inflammatory medication, antioxidants, antihypertensive and cholesterol lowering medication, use of folic acid to lower homocysteine levels, and antiplatelet medication for individuals with a history of vascular disease [20].