
Abstract
Keywords
There are a number of objectives stated in the National Mental Health Policy [1] (adopted in April 1992 and im plemented from 1 January 1993) which impinge on the role of dedicated psychiatric hospitals. One objective is to ‘mainstream’ hospital treatment, that is, ‘To expand the proportion of acute psychiatric inpatient care provided in hospitals rather than separate psychiatric hospitals …’ (p.18). A complementary statement to the ‘mainstreaming’ objective quoted above is ‘to reduce the size or to close existing psychiatric hospitals and at the same time provide sufficient alternative acute hospital, accommodation and community based services’ (p.23). The role of community-based services is also emphasized in a number of other places, for example, decentralizing the location of ‘community based services including crisis, assessment and treatment, rehabilitation/support and domiciliary and outreach services’ (p.23). In addition, attention is also directed to the provision of communitybased accommodation services, that is, an alternative to the accommodation provided by psychiatric hospitals. For an overview, see Whiteford et al. [2].
Thus, the emphasis in the National Mental Health Strategy can be conceived of as being on a spectrum of, and substitution between, institutional alternatives in terms of services and accommodation. One may consider dedicated hospitals to be at one end of such a spectrum of services and accommodation, and community-based services and community-based accommodation at the other end of such a spectrum.
Although there is reason to consider the various objectives mentioned above in an overall context, it is also useful to concentrate on one particular issue. The question addressed in this paper is as follows: ‘is the National Mental Health Strategy responsible for the deinstitutionalization of patients from dedicated psychiatric hospitals?’
The process of deinstitutionalization has not been confined to mental illness but has also been applied in other contexts such as intellectual disability [3], physical disability [4] and multiple disability [5]. It has also occurred in various countries, for example, the UK [6], the US [7] and Australia [8]. Furthermore, deinstitutionalization is not a uni-dimensional process. Talbott [7] suggests that it has the following characteristics: first, preventing inappropriate admissions to mental hospitals; second, discharging patients from mental hospitals after preparation for return to non-institutional living; and third, establishing and providing mental health services in a community setting. This description is somewhat positive whereas others may describe it in somewhat different terms such as ‘a national disgrace’ [9].
In Australia there is no comprehensive account, or treatise, of deinstitutionalization, such as exists for the US [10]. Deinstitutionalization in Australia gains some mention in general medical histories such as Lewis [8], Patrick [11], and more specific history works on mental health such as Dax [12], Lewis [13] and Krupinski and Stoller [14], but deinstitutionalization is not the central focus of any of these studies.
In the US, analysis of data on psychiatric hospitals indicates that deinstitutionalization did not take place in a uniform way. Residents in these hospitals reached a maximum of 558 922 in 1955 and then declined. At the same time admissions increased [10]. Subsequently in 1975, admissions fell. This differing pattern of hospital use has been categorized as two separate policies associated with psychiatric hospital use, namely ‘opening the back door’ and ‘closing the front door’ [15]. (These terms are simply descriptive of hospital activity, and imply no normative connotation.) Morrissey described the former period, characterized by both a falling total size (measured by residents) and rising admissions, as ‘benign’. However, the second period, ‘closing the front door’ (a period of reduction in both residents and admissions) was not benign. This second period has been described as a movement to ‘The Ghetto’ [16] and Reich [9] wrote that ‘… discharging helpless human beings to a hostile community is immoral and inhumane.’ See also Klerman [17] for an account of the quantitative changes in US residents and admissions.
The distinction being drawn in the US experience of deinstitutionalization has also been made for Victoria. Dax [12] has identified two stages, the first being when ‘suitable patients from hospitals could be discharged … to the community’ under various schemes such as trial leave, half-way houses, boarding-out, day hospitals, hostels combined with therapeutic workshops, social clubs etc. The second stage was a period in which patient certification and mental hospital admissions were to be avoided. This second period of deinstitutionalization was ‘… facilitated by the growth of private treatment and private hospitals, [and] the psychiatric wards of the general hospitals.’ Clearly, Dax is describing the two policies of ‘opening the back door’ and ‘closing the front door’. However, Dax was not able to provide any quantitative analysis of this distinction. The availableQueensland data enable such an analysis to be undertaken.
Method
Data
Since the late nineteenth century, Queensland's public psychiatric hospitals have been subject to an Annual Report of some kind which, in part, provided statistics on various dimensions of hospital activity. Over the years this Report has had various titles, such as the Report of the Inspector of Hospitals for the Insane, the Annual Report of the Division of Mental Hygiene etc. Also, in some years this Report was published separately, but for many years it was incorporated in the Annual Report of the Queensland Director-General of Health andMedical Services, as presented to the Queensland Parliament. For convenience these Annual Reports will be referenced below as Division of Psychiatric Services [18]. In some years, for example, 1944–45, there was no (published) report. Also, it is worth noting that missing data for some years were obtained from a (now discontinued) Commonwealth Bureau of Census and Statistic series Statistics of the State of Queensland: Social [19]. More recent data have been provided by Queensland Health [20].
From these sources, we have constructed an annual time series on the number of patients (as at 30 June) and number of admissions (during the financial year) for Queensland's public psychiatric institutions for the period from 1883–84 to 2001–02. These data relate to total patients, irrespective of age, and all diagnoses/conditions of patients (mental illness, intellectual disability and alcoholism). For a discussion of this diagnostic disaggregation in the Queensland data, see Doessel and Scheurer [22]. 21]. For more details, see Doessel and Scheurer [22].
Number of patients and admissions per 10 000 population in ‘Public Psychiatric Institutions’, Queensland, 1883–84 to 2001–02. Sources: Division of Psychiatric Services (various), Queensland Health (2003), Commonwealth Bureau of Census and Statistics (various). Notes: Over this long time period there were some changes in the processes of accounting for transfers between institutions in the ‘total system’. See Division of Psychiatric Services (1971, p.8). Stage 1: ‘opening the back door’; stage 2: ‘closing the front door’.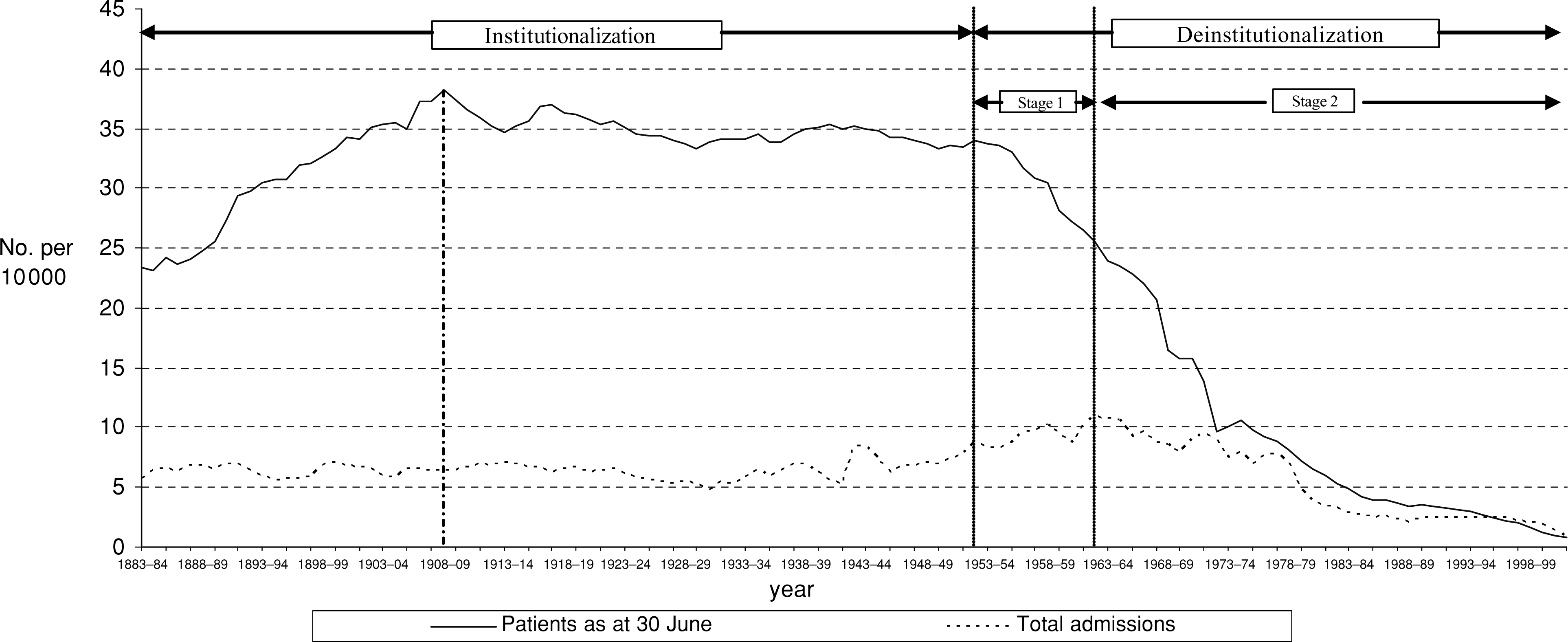
Although the largest relative size of these institutions occurred in 1908–09, when the rate was 38.17 patients per 10 000 people, casual empiricism suggests that the relative size was virtually constant from 1900 to the early 1950s. However, from 1953–54, there is a sustained decrease in the number of patients per 10 000 population. It is this year that we take to be the start of the deinstitutionalization process in Queensland, and specifically the start of ‘opening the back door’, or stage 1, of the deinstitutionalization process. Stage 2 of the process, that is, ‘closing the front door’ begins in the years after admissions per 10 000 population reaches a maximum, that is, 1962–63. This second stage has continued through to the present time, the admission rate being only 0.8 per 10 000 in 2001–02.
Statistical technique
Given the objective of this paper, an appropriate procedure is to apply regression analysis to the time-series data on patients and admissions per 10 000 population. Essentially, we apply intervention analysis to a time-series equation to determine if there is a structural break between the pre-National Mental Health Strategy period (the years before 1993–94) and the post-Strategy period. This technique was formalized by Box and Tiao [23] in their analysis of the effect of government regulations on air pollution in Los Angeles. Since then this type of analysis has been applied in many policy evaluation contexts such as the effect of decriminalizing drunkenness [24], the introduction of compulsory wearing of seat-belts in cars [25], the abolition of capital punishment [26], antidrinking and driving advertising campaigns [27] etc. For an overview, see Enders [28].
It was resolved to analyse the data from 1953–54, when deinstitutionalization appeared to begin. Linear and polynomial equations (up to the power of 5) were fitted to the per-capita patients' dataset for the 49 years to 2001–02. Autoregressive terms (to AR4) were needed in view of the serial correlation in both datasets. Despite various procedures, there was some remaining heteroscedacity in the estimated equations. (These statistical problems lead to unreliable results.) Examination of the residuals indicated that the heteroscedacity arose from some volatility in the early period, from 1953–54 to 1974–75. It was then decided to analyse the data in five sub-periods, as well as the whole period. Some overall results are indicated in Table 1.
Changes in the slope of patients per 10 000 population, psychiatric hospitals, Queensland, five sub-periods, and the whole period, 1953–54 to 2001–02.
Table 1 indicates that, over the 49-year period, there is an estimated overall annual decrease of 0.69 patients per 10 000 people in Queensland. However, there are some marked differences in the various subperiods indicated in Table 1: the most rapid decline (−1.11) occurred in the 1953–54 to 1973–74 period, the next highest decline (−0.66) was in the next period (to 1984–85) and the lowest decrease (−0.13) occurred in the period to 1992–93. In the post-1993–94 period (the National Mental Health Strategy period) the decline continued but at a higher rate, that is, −0.29 patients per 10 000, than the previous sub-period.
Further statistical tests have been undertaken on estimated equations for three sub-periods from 1974–75, that is, 1974–75 to 1984–85, 1985–86 to 1992–93 and 1993–94 to 2001–02. The analysis indicates quite clearly that these three sub-periods are quite different and distinct in terms of the decreases in patients per 10 000 population. Thus, there is reason to have considerable confidence in these estimated equations. In otherwords there is strong confirmation of the aggregate results reported in Table 1, and the visual impression from Fig. 1. These further results are available from the authors on request.
Results
Figure 2 presents not only the actual number of psychiatric patients per 10 000 population, but also a plot of the predicted numbers obtained by the three estimated equations (not reported here), for the period 1974–75 to 2001–02.
Predicted and actual numbers of patients per 10 000 population, Queensland psychiatric institutions, 1974–75 to 2001–02.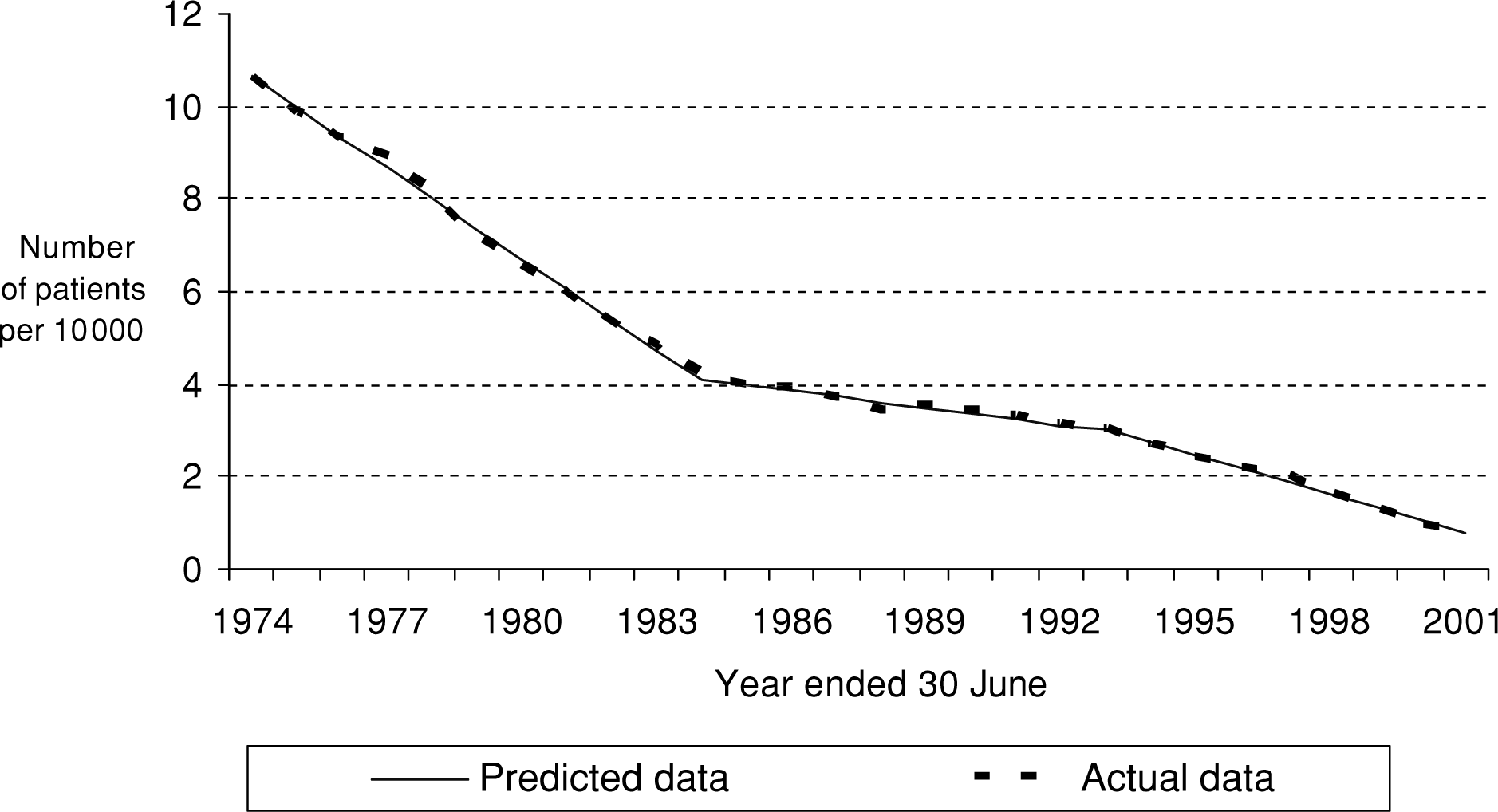
It was also found that three equations very adequately described the data for admissions per 10 000 population, the variable to which attention is drawn in the context of evaluating stage 2 of the deinstitutionalization process, that is, the policy of ‘closing the front door’. The actual and predicted values for admissions are shown in Fig. 3. The statistical results for the analysis of the policies of ‘opening the back door’ (stage 1) and ‘closing the front door’ (stage 2) are also available from the authors on request.
Predicted and actual numbers of admissions per 10 000 people, Queensland public psychiatric institutions, 1974–75 to 2001–02.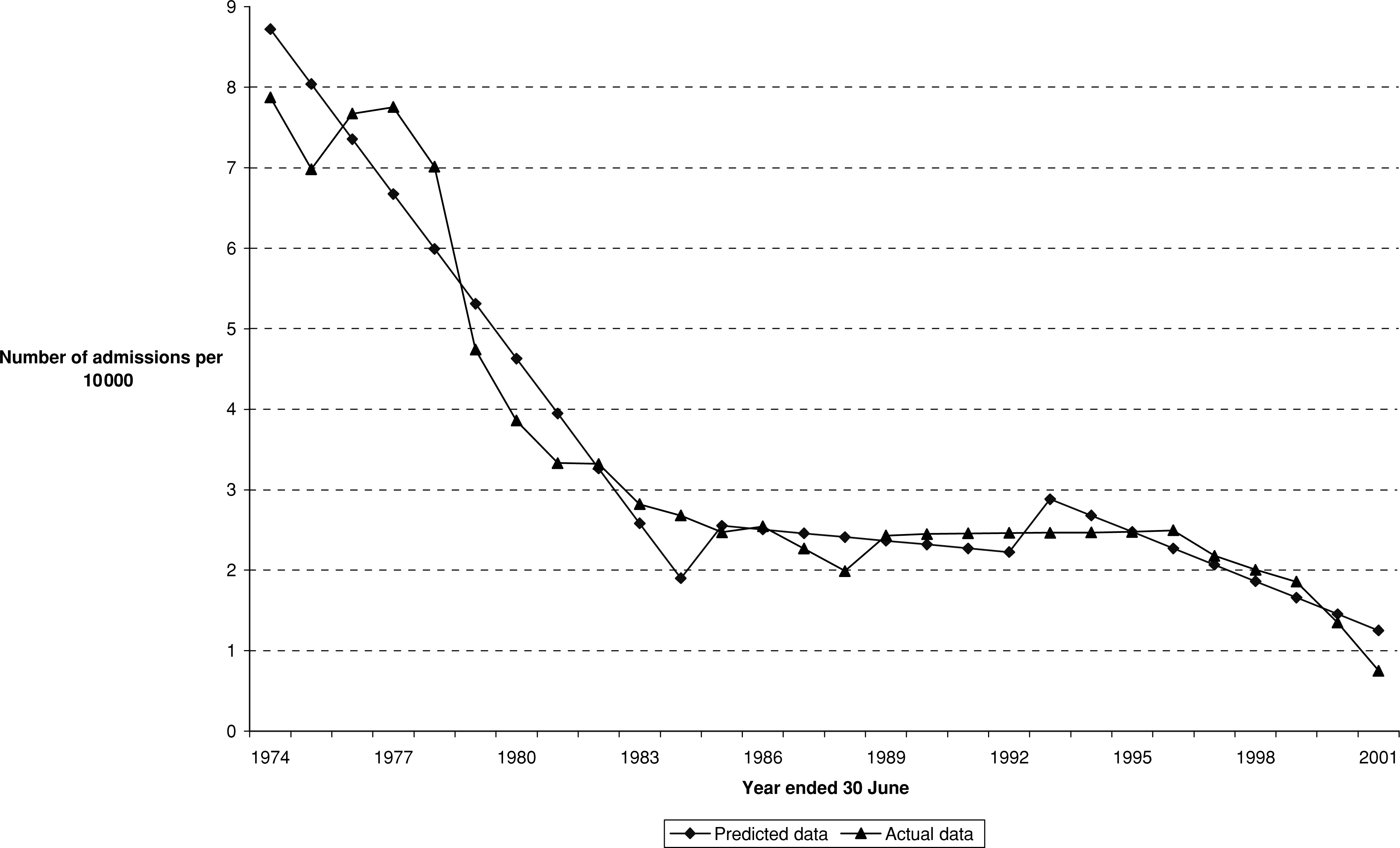
Discussion
It is clear from the data on Queensland public psychiatric institutions that, during the National Mental Health Strategy, dedicated psychiatric hospitals were operating at a fraction of their prior (say, in the 1950s) activity levels, as measured by ‘patients’ and ‘admissions’. But it is also clear that the significant decrease in their populations (however measured) pre-dated that Strategy: although the data indicate that deinstitutionalization was a continuing (but minor) process during the Strategy period. Thus, both dimensions of deinstitutionalization, that is, the policies of ‘opening the back door’ and of ‘closing the front door’ had become operative well before the time the Strategy was introduced. Although the Strategy was associated with a considerable increase in total community mental health resources (as measured by recurrent expenditure) [2] from 1992–93, there is little information suggesting resources followed patients into the community under the pre-Strategy deinstitutionalization. That such an extensive deinstitutionalization had occurred before the Strategy suggests that the expansion of nonmental hospital services during the Strategy was, in large part, needed to provide services for patients discharged before the Strategy began.
Conclusion
This study has been concerned with putting the recent policy changes associated with the National Mental Health Strategy, which commenced in 1992–93, into a broader perspective. More particularly, the perspective taken is a historical one: the analysis uses some timeseries data (for Queensland public psychiatric institutions) since 1883–84.
Some of the objectives of the National Mental Health Strategy have been concerned with the roles of different institutions (dedicated psychiatric hospitals, ‘mainstream’ acute hospitals and community centres) in the provision of mental health services. Thus, some attention has been placed on the spectrum of institutional settings formental health services. The common term for changes associated with this process of substitution is ‘deinstitutionalization’. For discussions of various dimensions of deinstitutionalization see, inter alia, Warner [29] on other countries and Rosen et al. [30] for New South Wales. Does this mean that the National Mental Health Strategy has been the driving force behind deinstitutionalization in Australia? This study indicates that the answer to this question is ‘no’.
The empirical analysis relates to rates for two different measures of psychiatric hospital activity, namely ‘patients’ and ‘admissions’. Overseas studies have found that these two measures of activity do not behave in the same way through time; ‘patients’ is a measure that indicates something about hospitals' discharge policy, whereas ‘admissions’ indicates hospitals' disposition to admitting patients. That the two measures of hospital activity do not coincide indicates that deinstitutionalization is not a single process: these two dimensions of activity imply that there may be several stages of deinstitutionalization.
The empirical analysis indicates that these two stages occurred in Queensland. Further analysis indicates clearly that both dimensions of the deinstitutionalization process were, in large measure, completed by the commencement time of the National Mental Health Strategy. In large part, the deinstitutionalization process was completed by the time the Strategy was implemented: thus, it was not a causal factor.