
Abstract
A substantial proportion of patients found in primary care complain of physical symptoms not attributable to any known conventionally defined disease, and which are not adequately supported by clinical or paraclinical findings. We call such symptoms medically unexplained or functional somatic symptoms. A study of the 25 most prevalent physical symptoms among patients who attended an internal medical outpatients' clinic showed that less than 10–15% of the patients presented with symptoms that could be attributed to an identifiable physical disease [1]. This indicates that it is the exception rather than the rule that physical symptoms are caused by identifiable organ pathology in primary care. Studies in the general population have shown that most people experience bodily sensations and symptoms every day [2–6]. Hence, functional somatic symptoms and disorders have to be regarded as a continuum ranging from mild conditions that are difficult to discern from normality to serious conditions that cause suffering and disablement for the patients [7]. Primary care studies on somatoform disorders have reported a huge variation in prevalence figures, which may reflect that different diagnostic criteria and different diagnostic instruments have been used. Based on studies using standardized psychiatric interview, the prevalence may be estimated to be approximately 20% [8–10].
Patients with somatoform disorders have an excessive use of health-care services both in primary care and in the specialized health-care sector [11]. The chronic somatizing patients may over time have gone through numerous hospitalizations, surgical procedures and futile treatments with the impending risk of being exposed to iatrogenic harm [12], [13]. They may be severely disabled and in great emotional pain because of their illness. Somatoform disorders are thus very costly for society, not only because of increased health-care costs, but also through lost working years, early retirement pension and other social expenses. In Denmark, functional somatic syndromes and somatoform disorders accounted for 10–15% of all disability pensions in 2002 [14]. Failure to diagnose and treat these conditions may thus have severe consequences for patients and the society.
A precondition for the treatment of functional somatic symptoms is that they are identified. In a primary care study, an enormous variation was found in the number of patients diagnosed by the general practitioners (GPs) (i.e. family physicians) as having medically unexplained symptoms (MUS) as the reason for encounter, with prevalence in the range from 3% to 33% [15]. The huge variation seems not to reflect real prevalence differences between practices, as independent measures by questionnaires did not detect any significant prevalence differences between them (16]. Another possibility may be the lack of an appropriate classification for primary care patients presenting with functional somatic symptoms. Thus, every GP has developed his/her own personal practice in labelling these patients.
General practitioners' (GP) recognition of functional somatic symptoms compared to screening questionnaire. Subject to permission from British Journal of General Practice in which the table was published electronically in the December 2003 issue.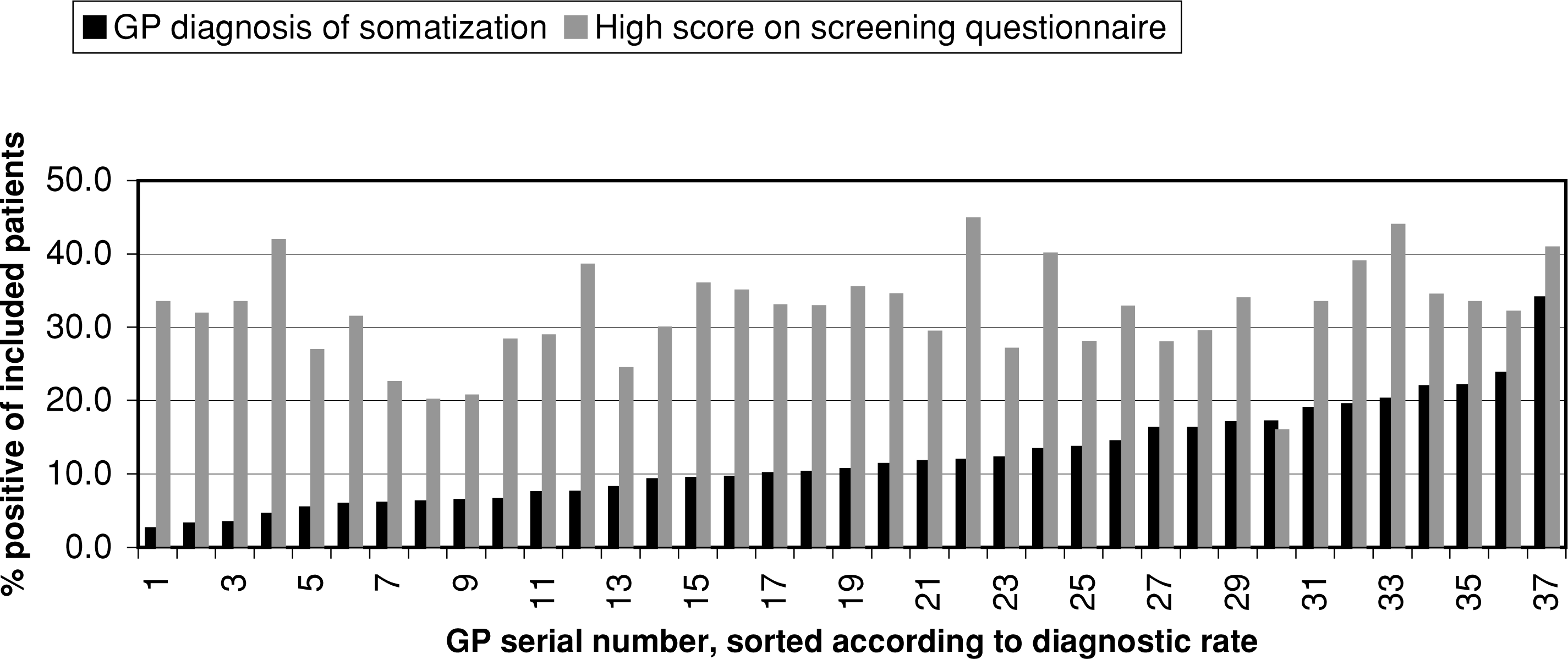
This emphasizes one of the major, present problems, namely that there is no general consensus on how to diagnose and classify patients presenting with functional somatic symptoms. The current ICD-10 and DSM-IV classifications of somatoform disorders lack valid and reliable diagnostic groups for classification of patients with functional somatic symptoms. The current classifications evolved in specialized settings are of little use in primary care. Nor does the International Classification of Primary Care (ICPC), which is derived from the ICD-10 for primary care use, seem appropriate.
The main focus of this paper will therefore be on the problems of the classification, as improvement of this is a precondition for research in functional somatic symptoms and appropriate treatment of the patients.
Diagnostics and classification
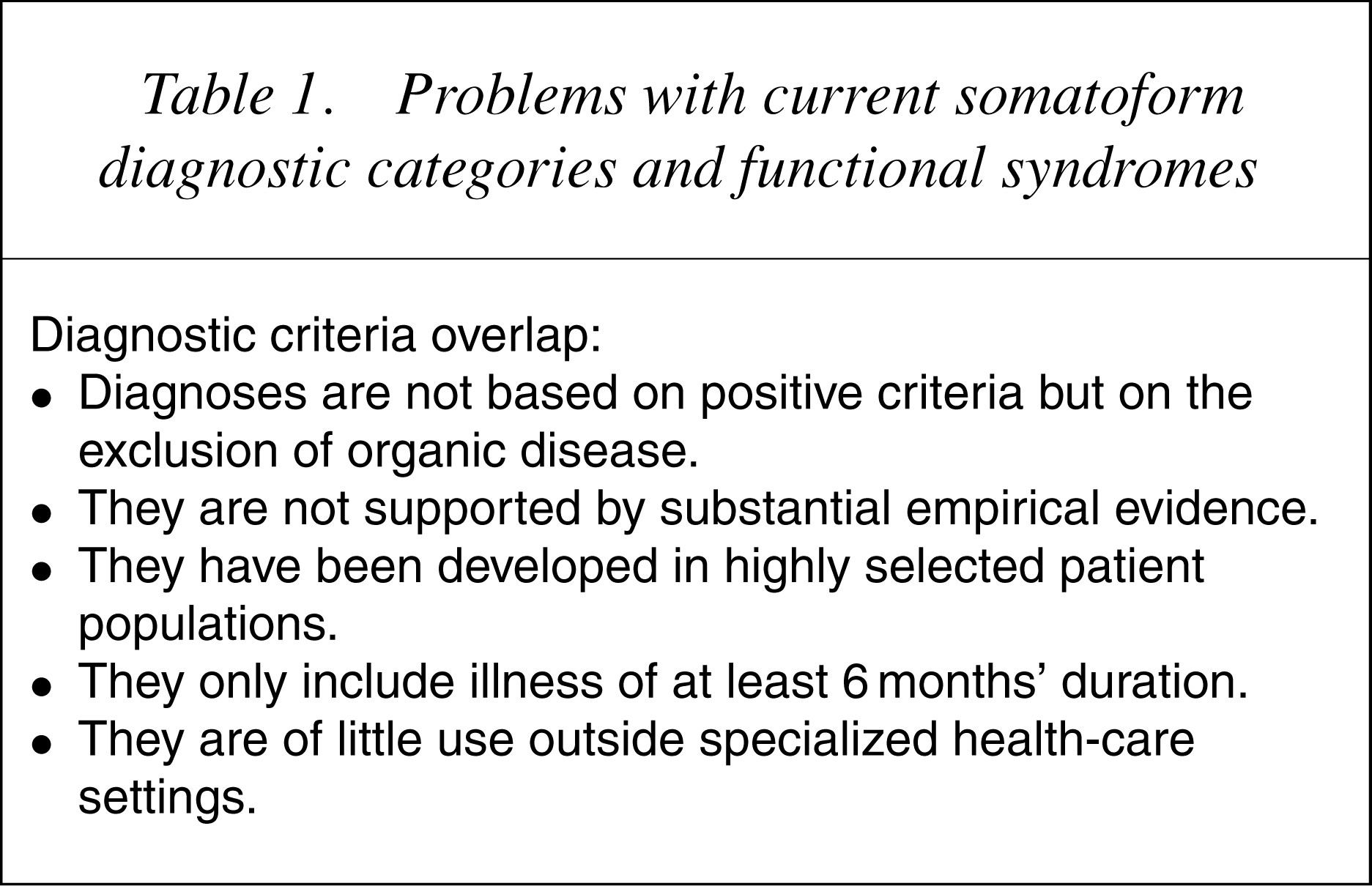
Problems with current somatoform diagnostic categories and functional syndromes
A range of strategies for establishing the validity of clinical syndromes and diagnoses has been suggested [19–21].
Symptom pattern and clinical presentation
Of particular importance for diagnoses not based on fundamental, aetiologically measurable abnormalities but on clinical observations and subjective symptoms, is that clusters or patterns of symptoms can be established, and that boundaries between related symptom clusters can be identified. In somatoform disorders, the individual diagnoses are poorly and arbitrarily defined causing diagnoses to overlap, which means that the majority of the patients will exhibit clinical characteristics of different diagnostic categories [22–26]. Furthermore, diverse medical specialties have developed their own syndrome labels to classify patients presenting with functional somatic symptoms, as for example, chronic fatigue syndrome (CFS), fibromyalgia, irritable bowel syndrome (IBS) and chronic benign pain syndrome [27]. Studies have indicated a massive overlap in symptoms and diagnostic criteria between various functional syndromes as well as between miscellaneous functional syndromes and somatoform disorders [27–29].
Diagnosis overlap is rooted in an inappropriate research methodological practice such as investigators' propensity to single out particular diagnoses or symptoms pertinent to their specialty, ignoring other symptoms rather than adopting a comprehensive view to facilitate overlap detection. The empirical foundation of the somatoform disorder diagnoses and functional somatic syndromes is poor as it springs mainly from a clinical tradition based on observation of patients in highly skewed specialized medical or psychiatric settings. A longitudinal population-based study showed that patients with multiple medically unexplained general hospital admissions displayed different illness pictures at different times depending on the specialty of the department to which theywere admitted [30]. Likewise, a review of the medical literature showed that the illness picture or the label used varied significantly during history [31]. Thus, the present situation is that patients with identical symptoms and clinical pictures may receive different diagnostic labels depending on the focus of interests of the assessing physician.
However, some somatoform diagnostic categories are so narrowly defined that they defy clinical application, especially in primary care [8],[32–35]. The somatoform diagnostic categories require that the symptoms have lasted for at least 6 months. From a primary care point of view this implies that diagnosed patients are already chronically ill, and the GPs do not have any option for an appropriate classification of the major part of patients who present with acute, subacute or transient disturbances.
Aetiology classification
Medical nosological tradition has primarily aimed to classify disorders according to their cause [19–21], and it was attempted to base earlier permutations of psychiatric classifications on aetiology also. Except for the organically based disorders and a few others, such as posttraumatic stress disorder, the aetiology of psychiatric disorders is unknown as no fundamental, objectively measurable anatomical, biochemical, molecular or psychological abnormalities have yet been identified. The aetiological considerations in earlier classifications were not supported by substantial empiric evidence. As a consequence, the aetiological classification was abolished, and a descriptive classification was introduced by DSMIII in 1980. However, in the section of the somatoform disorders, diagnoses reminiscent of the previous classification still exist, as diagnoses like pain disorder and conversion disorder require psychological factors to be of importance.
The aetiology of functional disorders is unknown, but is probably multifaceted. Different unspecific predisposing factors commonly seen in a wide array of mental disorders, assume importance depending on the person's general vulnerability and coping strategies. More specific predisposing factors for somatoform disorders may include physical or sexual abuse in childhood, parental functional illness and low intelligent quotience (IQ), but these factors are also associated with other psychiatric disorders [36], [37]. Neither parental nor childhood welldefined physical disease seems to be of significance [36]. The reported familial transmission may be rooted in sociocultural variables, but there is also some support for a genetic transmission [38].
Unspecific precipitating factors are stress and strain, for example, bereavement, loss of job, physical disease or other significant events. It is not known whether specific precipitating factors may exist. Besides patient- and illness-related factors, perpetuating factors include social factors (work, family and compensation issues) and iatrogenic factors (i.e. the management provided by the health-care system). The last mentioned may be more specific for somatoform and related disorders.
The way physicians and the health-care system manage and care for patients with functional somatic symptoms appears to be very important for the course of the functional somatic disorders and the probability of the illness becoming chronic. Delay of, or missed, diagnosis may hinder a proper treatment being instituted and keep the patient in the sick role. The patient may go through numerous futile hospitalizations, examinations, interventions and treatment attempts on dubious indication and without relief [11], [13].
There are several reasons why physicians cannot stop this vicious circle of repeated examinations and futile ‘treatments’ despite lack of evidence of organ pathology [12],[39–41]. The physician may fear overlooking a genuine physical disease, even if it seems rather unusual as it happens in only 3–4% of the cases [12], [42], [43]. The fear of being scorned by the media, or being sued by the patient for having overlooked something may also be of importance [44]. The GP may have insufficient knowledge and skills in diagnosing and handling behavioural dysfunctions and mental disorders, and therefore continues to pursue organic possibilities. The GP may also be reluctant to use stigmatizing diagnoses [40]. The lack of accessible competent psychiatric service for second opinion or referral may give the doctor no alternatives but to try treating the patient him/herself [45]. Finally, the GP may, among other factors, find that there is insufficient time to properly assess and manage these patients [41]. Although iatrogenic factors may be very important for functional and related disorders, they cannot be used for classification purposes as they are more a case of poor management.
Cognitive–behavioural model of functional disorders
The cognitive–behavioural model suggests that functional illness is a result of amaladapted reaction to benign normal bodily sensations and banal ailments that are misinterpreted as caused by a physical disease. The model focuses on the patient's symptom perception and the resulting illness behaviour [12], [46], [47]. 12], [41],[47–50]. The model assumes that everybody has a personal sensation or symptom panorama, which the person is familiar with. This knowledge accumulates throughout life in a continuous process. When girls reach puberty they become familiar with new symptoms in connection with menstruation, which they add to their personal symptom panorama. Experiences with symptoms from various diseases throughout life will also form part of the individual's inner frame of reference. People judge their condition primarily through inner evaluation, that is, from their earlier experiences. People may also seek information from external sources, that is, family members, colleagues, medical encyclopaedias, weekly magazines, as well as physicians. External information can initiate the process of the individual changing the interpretation of personally well-known sensations as outlined in Fig. 2, that is, they suddenly interpret symptoms as signs of illness. The new information will cause focused attention on the body part that is suspected to harbour the disease. This may cause new sensations or symptoms to surface, and a cycle of worry and expectation of symptoms will ensue.
Symptom perception and illness understanding.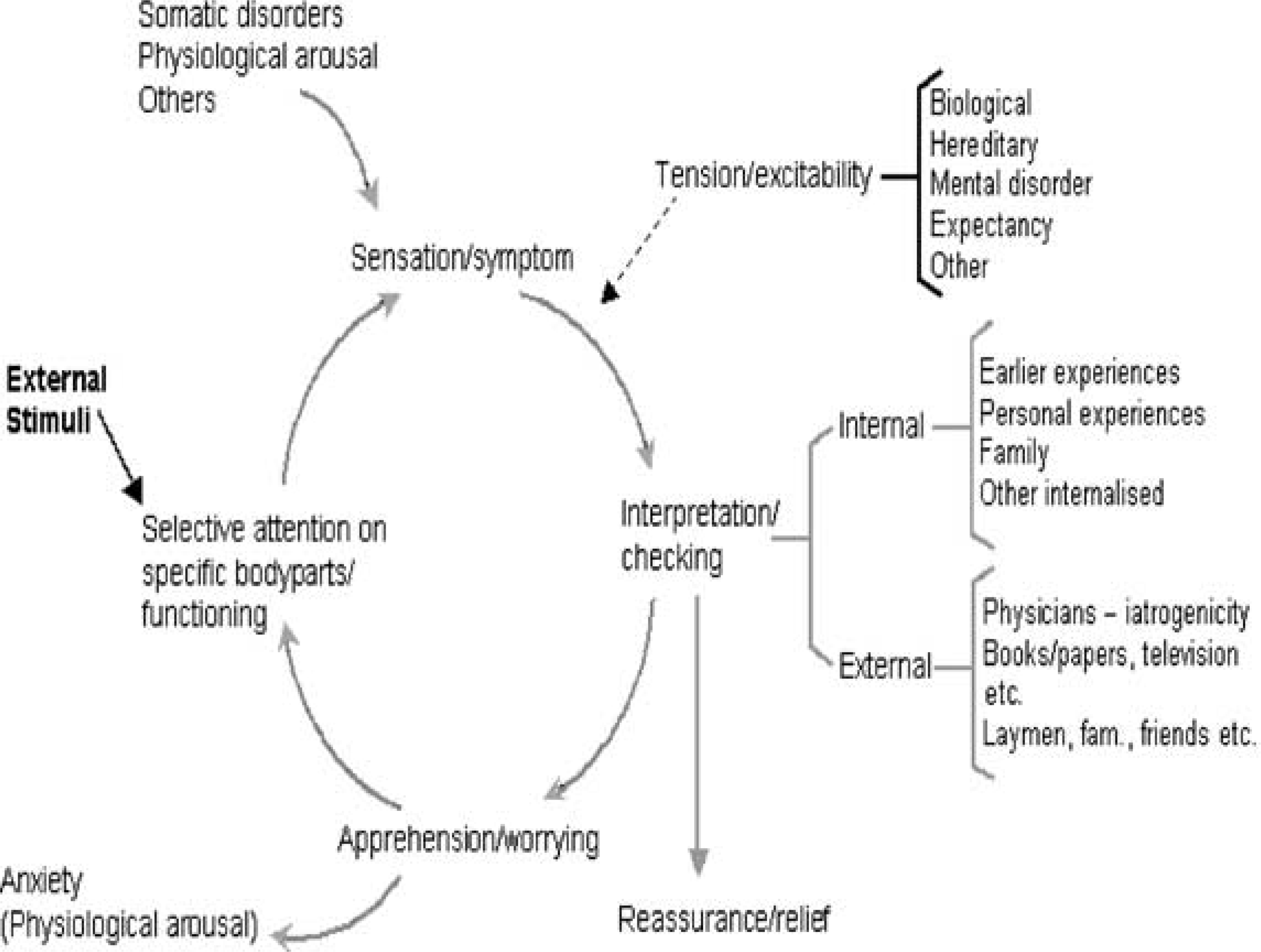
The process outlined in 51].
Even if this, in combination with biological factors, may be the basic pathology of hypochondriasis, we still need much more knowledge to be able to use it for classification. Moreover, research has indicated that patients' illness perceptions are helpful in understanding people's reactions to diseases in general, and that illness perceptions are crucial to people's morbidity and functional level – not only in hypochondriasis. Thus, it is of dimensional character rather than categorical.
Biological model
Studies have indicated that biological mechanisms and pathophysiological changes may be of importance in functional disorders [52]. The multisymptomatic illness pattern found in functional disorders may be caused by the patients' intensification of all bodily sensations because of afferent stimuli to the brain not being suppressed, or because of an increased sensitivity of the central nervous system (CNS) structures [52–55]. Also, the stress response mediated by the hypothalamic–pituitary– adrenocortica (HPA) axis may be involved [56].
Treatment response and establishment of distinct course or outcome
Another strategy to identify and validate diagnostic categories is to establish a distinct treatment response, or to establish a distinct course or outcome. Studies on cognitive–behavioural therapy, interpersonal therapy and treatment with antidepressants have indicated that these may be at least as effective in the treatment of somatoform disorders and functional somatic syndromes as in the treatment of other psychiatric disorders [57–59]. However, these treatments do not seem to be specific for any diagnostic category, but usable for a wide range of disorders and syndromes. High quality rigidly designed randomized clinical trials (RCTs) on well-defined patient groups are needed before we are able to show specific diagnosis-related treatments.
Studies on diverse somatoform disorders and functional somatic syndromes have shown that the disorders are often persistent and that the prognoses are poor [11], [60]. However, again this seems to apply to several categories and be of little use for differentiating between categories.
New classification
Because of the problems with our current somatoform diagnostic groups, it has been suggested that the whole concept of somatoform disorders be abolished [61]. However, the concept is of great importance in practice and therefore indispensable, even if presently the diagnostics have not been defined in a satisfactory way. Until we are much wiser than now, a certain amount of obscurity is more useful than brilliant pseudoclarity.
Thus, we suggest that the whole spectrum of phenomena, including the functional somatic syndromes, are re-evaluated while the current somatoform diagnosis concept is kept as a separate category. This process must comply with methodological ground rules as to nosology and epidemiology, and it must be founded on empirical research as well as on sound clinical assessment, that is, not based on questionnaires or lay interviews. As diagnoses are the foundation of all medical practices, the only way to get rid of unfounded syndromes and diagnostic labels is to introduce an improved classification with more valid and acceptable diagnostic categories. This must also encompass the needs of primary care.
Below, we outline a framework for a new descriptive classification of functional somatic symptoms and unfounded illness worrying, covering the whole spectrum of severity. This classification is for clinical use and for further evaluation in research.
Bodily sensations and symptoms are so frequent in the general population that they have to be regarded as a normal part of human life [2–6]. They will only have clinical pertinence if the symptoms are distressing, or if the individual seeks medical care. If such bodily sensations or symptoms attract medical attention, we call them MUS or functional somatic symptoms.
Functional somatic symptoms may generally be regarded as a basic mechanism mankind has for expressing stress. Other common responses to stress and strain are mood symptoms, anxiety and cognitive disturbances including sleep disturbances and lowered energy. Those reactions are probably each of dimensional nature on a spectrum from everyday experiences to severe illness [62]. Each type of responses is likely to be mediated by specific CNS and hormonal pathways. This implies that the symptoms introduced by each biological system are not necessarily a reaction to a stressor, but may be caused by an organically based dysfunction in the mediating pathway. For example, in depression, ‘idiopathic’ or endogenous types are well known, that is, where no significant precipitating stressor can be identified. This implies that an emotional or behavioural disturbance does not necessarily have to be shown to establish the diagnosis.
Because of the probable dimensional nature of these common responses to stressors, it may be a hypothesis that they often mix together in the individual people, and in mild cases a mix of symptoms from different dimensions are probably more the rule than the exception. In severe cases, the symptom picture may differentiate into an established disorder like anxiety, depression or a functional somatic disorder. Why some people mainly respond with symptoms from one dimension, as in depressive disorder or anxiety disorder, has still to be explored, but pure types are probably rare. Patients with, for example, a depressive disorder usually also report anxiety and physical symptoms [63]. From a classificational point of view, it therefore seems inevitable that symptoms from other dimensions are included in the diagnostic criteria if they are established on the basis of highly selected groups of patients with a given characteristic as, for example, patients admitted to a psychiatric hospital for depression.
From a clinical point of view, this gives a differential diagnostic problem. Thus, 50–95% of patients with mood disorder primarily present with physical symptoms rather than emotional symptoms to their GP [64], [65]. These cases have been called facultative or presenting somatizing or somatized mental disorder [34], [66]. However, as the symptoms are fully explained in the context of their well-defined psychiatric disorder, and the patients will accept the correct diagnosis when made, these diagnoses do not belong to the same group of disorders. It is, however, important that the physician knows this psychiatric differential diagnosis and knows how to inquire about it to avoid unnecessary physical examinations and inappropriate treatment.
Table 2 outlines a framework for the categorization of patients presenting with functional somatic symptoms and unfounded illness worrying, with the main focus on primary care.
A. Health advice. This includes patients consulting for check-ups for trivial complaints without indication of illness and without significant impact on functioning or wellbeing. The patients consult to be reassured that they do not have any significant disease, and they are not requesting any treatment. This is a common patient type in primary care, and it may be discussed whether it is a mild form of hypochondriasis or if it is a normal behaviour. The behaviour may be appropriate from a medical point of view as the patients are encouraged by campaigns for early detection of, for example, cancer or hypertension, and therefore it can hardly be viewed as pathological. For clinical use it may be appropriate to state the primary symptom that is in focus of the consultation, that is, cough, headache. A large group of patients also have complaints that are judged by the physician to be caused by a physical disease, for example, a benign virus, but as the diagnosis cannot be confirmed at clinical examination, the precise nature remains uncertain. The complaints are minor and not alarming, and the physician may choose to wait and see whether further investigation and treatment are necessary.
It may thus be appropriate to categorize the patient group presenting with minor or banal symptoms into subclassifications of the patients with probably physical disease and patientswith probably functional symptoms.
B. Natural (dis)stress reaction. A reaction to psychological traumas or strains as, for example, loss of job, divorce, or owing to bereavement. The reaction does not exceed what would be expected given the event or psychological trauma. If the symptoms are persisting, another diagnosis must be considered.
C. Undifferentiated (dis)stress disorder. Patients with disturbing, unspecific, physical, emotional or cognitive symptoms. The symptoms are not so severe or persistent that the patient qualifies for a mood, anxiety, somatoform or other specified psychiatric disorder. Common bodily symptoms are arousal symptoms from the cardiovascular and pulmonary systems, gastrointestinal symptoms or musculoskeletal symptoms including pain, and the patients usually complain of a high overall number of functional bodily symptoms [Fink, P: unpublished observations] [67]. Common cognitive symptoms are difficulties in concentration, memory, sleep disturbances, irritability etc. Dominating emotional symptoms are mood and anxiety symptoms. Symptoms from different domains often mix together, but one domain may be predominating and subtypes with primarily depressed mood, with anxiety and with functional somatic symptoms may be specified. In the current DSM-IV adjustment disorder diagnosis, the first two subcategories are specified, but we suggest inclusion of a functional somatic subtype as well. Besides, we suggest that the diagnosis be based on the symptom presentations rather than on aetiology, and to omit the DSM-IV requirement of presence of an identifiable stressor or event, even if it is often present.
D. Functional somatic disorder or bodily distress disorder. The patient usually presents with multiple functional bodily symptoms. The same bodily symptom pattern as mentioned under C may be characteristic for the patients, but whether this can be used as positive identification of the diagnosis must await further investigations. The symptoms are severe and persistent with significant impact on the patient's wellbeing and functioning. It still has to be established whether subgroups may be identified, for instance, patients with predomination of symptoms from one domain, for example, a gastrointestinal subtype, cardiovascular subtype and a musculoskeletal subtype. Patients currently classified as having somatoform disorder, undifferentiated somatoform disorder, pain disorder, neurasthenia or CFS are among others included under this heading.
E. Hypochondriasis or health anxiety disorder. This is characterized by an excessive inappropriate worry and preoccupation with the fear of having a serious physical disease. Recently, newdiagnostic criteria forming a distinct diagnostic entity for hypochondriasis or health anxiety disorder have been suggested [68]. This includes the symptoms obsessive rumination with intrusive thoughts, ideas or fears of harbouring illness that cannot be stopped or can only be stopped with great difficulty, plus at least one of the following five symptoms: (i) worrying about or preoccupation with fears of harbouring a severe physical disease or an intense attention on bodily functions, physical sensations, physiological reactions or minor bodily problems that aremisinterpreted as serious disease; (ii) suggestibility and autosuggestibility, that is, the patient is inclined to fear having a disease because of reading or hearing about it; (iii) excessive fascination with medical information; (iv) an unrealistic fear of being infected or contaminated by something touched, eaten or a person met; and (v) fear of taking prescribed medication.
F. Dissociative disorder. In the motor and sensory type, the patients present with physical symptoms, simulating a neurological disorder such as paralysis, blindness or confusion. The onset is sudden and closely associated in time with an identifiable emotionally traumatic event, insoluble and intolerable problems or disturbed relationships. Less severe cases are probably quite common, and even mentally stable and previously healthy individuals may react with dissociative symptoms when exposed to disaster. The condition is usually transient and with sudden spontaneous remission. Defined as here the disorder is rarely seen in primary care.
G. Factitious disorder. The patients feign illness or deliberately inflict a disease upon themselves. In contrast to malingering, there is no apparent external incentive for producing the symptom(s) and the motive is unconscious and only understandable in a psychopathological context. Patients who suffer from factitious disorder often have a severe personality disorder where the patient borders on psychotic breakdown. The disorder is rare but attracts much attention and is often confused with malingering.
A framework for categorization of patients presenting with functional somatic symptoms in primary care
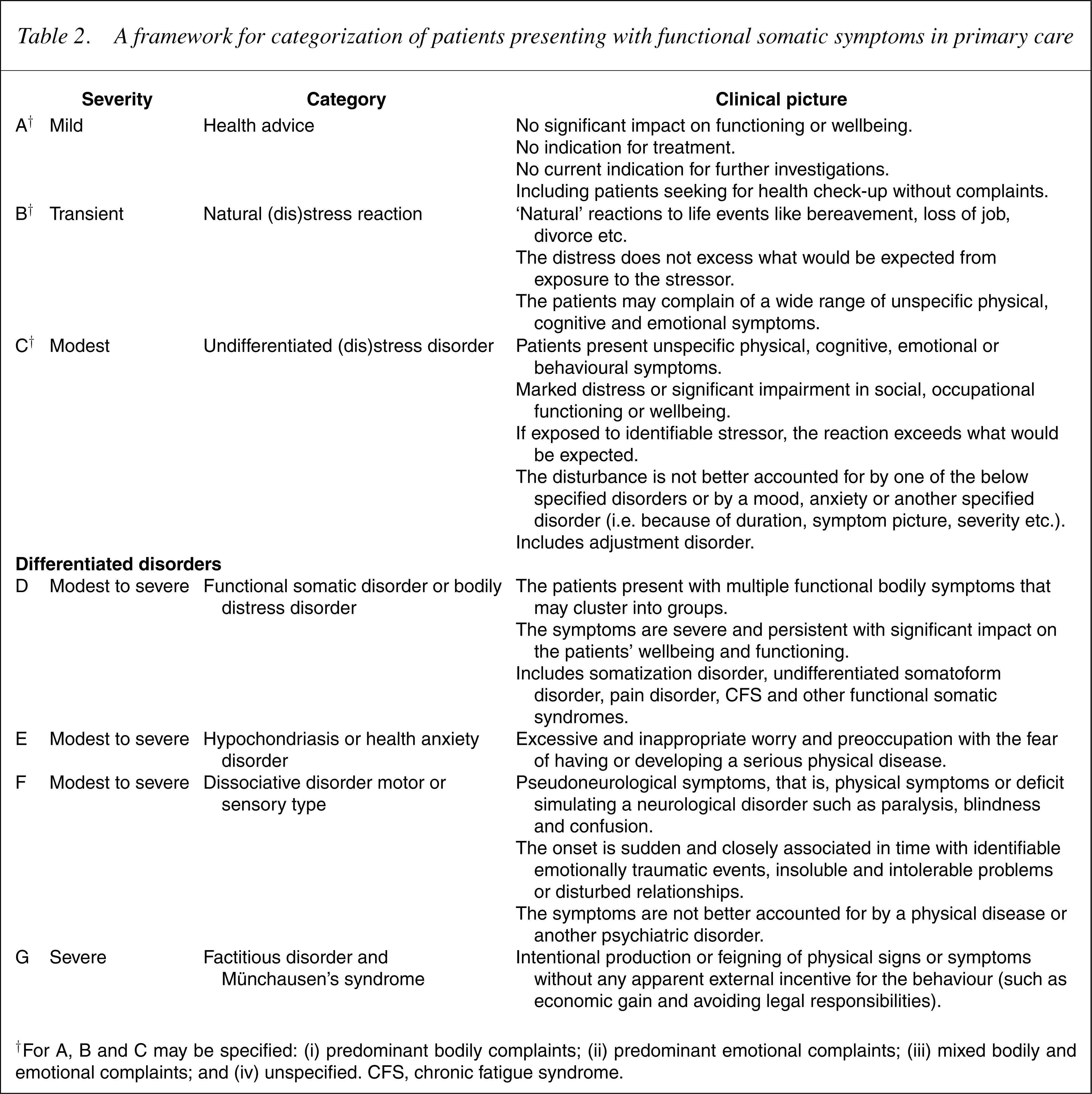
†For A, B and C may be specified: (i) predominant bodily complaints; (ii) predominant emotional complaints; (iii) mixed bodily and emotional complaints; and (iv) unspecified. CFS, chronic fatigue syndrome.
Implications for research, management and education
The high prevalence of functional somatic symptoms makes it unrealistic to aim at treatment of all these patients in specialized care. Furthermore, these patients are often reluctant to accept referrals to a psychiatrist or psychologist, as they believe their problem is of physical and not psychological nature. Neither does it seem expedient to aim at specialist treatment of all these patients. A brief intervention at first encounter may prevent the patient becoming chronically ill. The vast majority of patients presenting with functional somatic symptoms are thus to be managed by primary care physicians. However, severe persisting cases usually need specialist treatment and in chronic cases a close cooperation or shared care between the psychiatrist and the primary care physicians may be most effective. An agreement on the treatment between the specialist and primary care provider is necessary. Otherwise, a patient's pathological health-seeking behaviour caused by a belief in organically founded disease may cause harm to them because of the various investigations and treatment attempts on dubious indication.
A common language for all branches of medicine is necessary to strengthen cooperation in treatment and to interchange knowledge between disciplines. A diagnostic system as outlined here would be necessary to facilitate this, and an appropriate and comprehensive system shared by all physicians is a must if we shall improve our research in these diseases and promote better theoretical and practical teaching [69]. Thus, an appropriate classification may be the first step to ensure that functional somatic disorders are treated as seriously as other disorders, and that the patients receive the same quality of treatment as other patients. Today functional somatic and related disorders are widely neglected by all medical disciplines including psychiatry, and this is especially serious for primary health care and for outpatients' clinics [45], even though it has been shown that the disorders can be treated at least as effectively as other psychiatric disorders [57–59]. One reason for this is that only few psychiatrists and psychologists have the necessary expertise and knowledge to treat these disorders. In most countries, psychiatry mainly deals with psychosis and other severe orthodox mental disorders, and are only infrequently confronted with patients with functional disorders [45].
Therefore, there is a need for training in diagnosing and managing these disorders on all levels of specialization and in most branches of medicine. This implies that pregraduate training in medical schools as well as postgraduate training is needed. The postgraduate training needs to be tailored to the specialty. In primary care, relatively brief, tailored evidence-based educational programs have been developed. By use of these, GPs are successfully trained in skills important for recognition and treatment of patients presenting with functional somatic symptoms.
A precondition for effective training in diagnosing and managing functional somatic disorders is that we have a reasonably valid diagnostic system for clinical use aswell as for research. There is a need for further clarification, research and validation of the presented classification of functional somatic symptoms before we proceed to newepidemiological and interventional studies in general practice, and it is important to ensure that a newdiagnostic classification covers thewhole spectrum of disorders seen in primary health care.