
Abstract
While the diagnostic systems of DSM-IV [1] and ICD-10 [2] have improved the reliability of psychiatric diagnosis, they inadequately capture the nature and range of dysphoric states, especially in the medical setting [3, 4]. As van Praag [5] suggests, ‘syndromal definition has disappeared from the diagnosis of depression’ (p.767). So while the number of diagnostic categories has increased, evidence for descriptive validity has not.
At the same time epidemiological studies have found more parsimonious models of common emotional disturbance (see, for example [6]). Dohrenwend and colleagues [7] recognized a common distress syndrome – one they termed ‘non-specific’ and likened to Jerome Frank's concept of demoralization [8] – which they believed underpinned much psychiatric disturbance, being ‘generally associated with affective distress but… not specific to any particular psychiatric disorder’ (p.1229).
In our own research, as in our clinical work among patients with physical illness, we have come to see the concept of demoralization to be of central importance. In this paper we explore the phenomena of demoralization and conclude that it is a real and important entity – and one that deserves greater attention by psychiatrists. We argue, however, with Frank, that it is not simply ‘nonspecific distress’ but a clearly defined syndrome of existential distress occurring in patients suffering from mental and physical illness, specifically ones that threaten life or integrity of being. We begin by describing the experience of demoralization as conceived by Frank, and then elaborate concepts important to its understanding: coping; hope and hopelessness; meaning, purpose and despair. Drawing on the research literature, we demonstrate that demoralization is different to depression and is important in the development of a desire to die. Its alleviation is assisted by specific psychotherapeutic techniques as well as through the ‘valuation’ implicitly given in a good therapeutic relationship. In summary, the concept of demoralization is valuable, has descriptive and predictive validity and should be given a place in psychiatric taxonomies.
Demoralization
The dictionary defines ‘demoralize’ as ‘to deprive a person of spirit, courage or discipline; to reduce to a state of weakness or disorder’ [9]. This certainly describes many patients receiving psychiatric care. Frank observed that most people with psychiatric symptoms do not seek treatment (an observation still true today [10]), and those that do are ‘demoralized’. Demoralization, he said, …results from persistent failure to cope with internally or externally induced stresses that the person and those close to him expect him to handle. Its characteristic features, not all of which need to be present in any one person, are feelings of impotence, isolation, and despair. The person's self-esteem is damaged, and he feels rejected by others because of his failure to meet their expectations. Insofar as the meaning and significance of life derives from the individual's ties with persons whose values he shares, alienation may contribute to a sense of the meaninglessness of life… The most frequent symptoms of patients in psychotherapy – anxiety and depression – are direct expressions of demoralization. [8], p.271] Typically, [such people] are conscious of having failed to meet their own expectations or those of others, or of being unable to cope with some pressing problem. They feel powerless to change the situation or themselves and cannot extricate themselves from their predicament. [11], p.35]
In psychiatric literature, demoralization is viewed variably as a self-perceived incapacity to deal effectively with a stressful situation (incompetence) [12], a ‘nonspecific’ distress [7, 13], or a combination of these [14]. Consistent with Frank [8], we use the term here in the more specific way of de Figueiredo [14]. Our model of demoralization, expanded below, is illustrated in Figure 1.
A model of demoralization. ∗In truth, our futures are always unknown, which points to the important role of ‘illusions’ in maintaining our sense of control [75]. Clearly also, the particular meaning and significance of the event for the person is critical to the development of demoralization.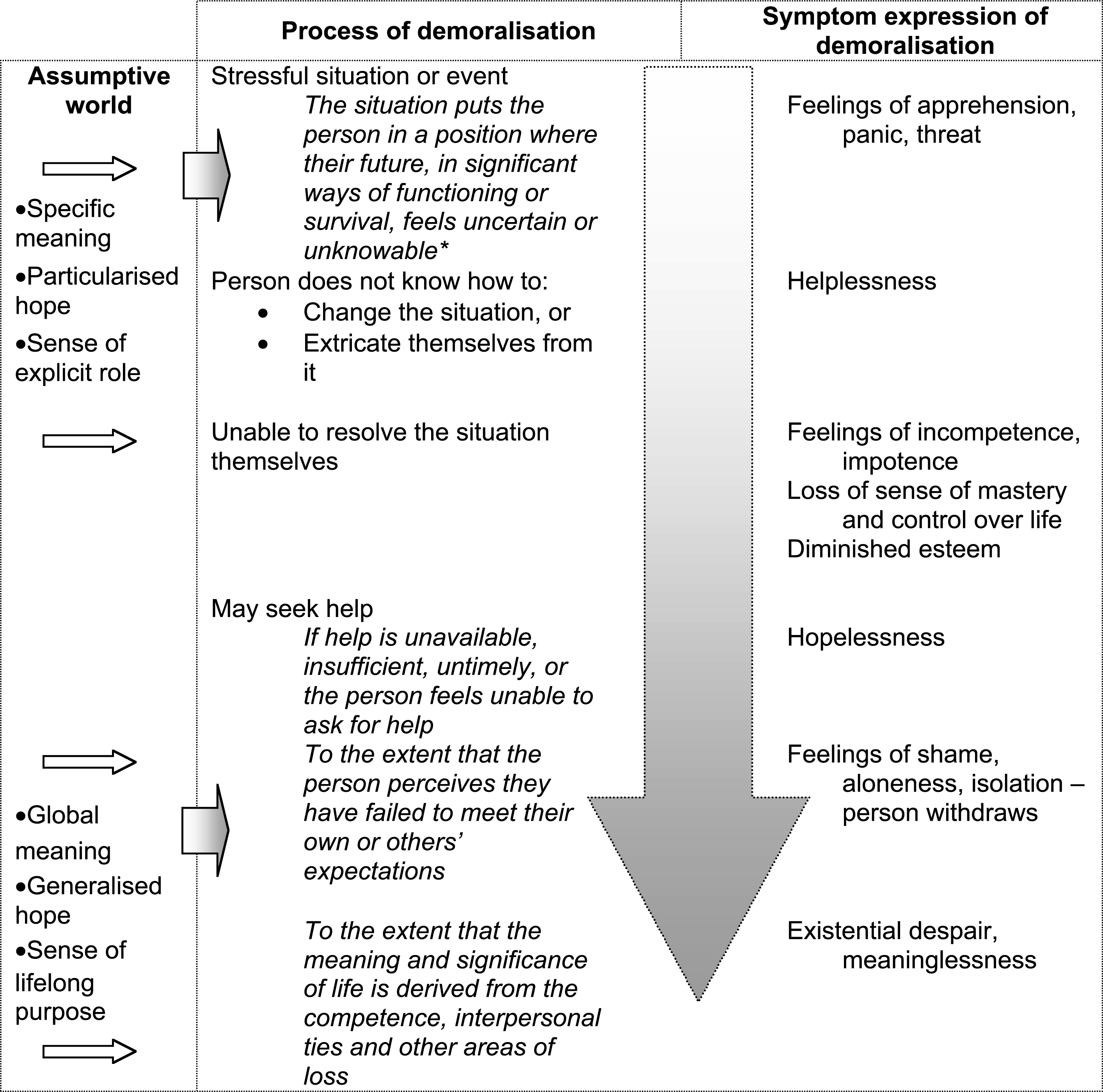
Coping
At the heart of demoralization is a breakdown in coping. Lazarus and Folkman's model of stress and coping [15] entails two key concepts – appraisal and coping. Appraisal involves evaluation of the personal significance of a given event – for instance, whether it is perceived as a threat or a challenge – and the adequacy of one's resources to respond. This appraisal is affected by a person's beliefs, values and commitments as well as their sense of general optimism or pessimism, and selfefficacy. Coping refers to mechanisms that regulate distress and is commonly considered in two categories, ‘problem-focused’ (e.g. information seeking, problemsolving and direct action) and ‘emotion-focused’ (escape, seeking social support, cognitive reframing). When these mechanisms are insufficient, and the person no longer ‘knows what to do’, distress and helplessness ensue. This is the core of demoralization; a feeling of being trapped, not knowing what to do, becoming helpless (see Fig. 1).
Any number of events can threaten a person's sense of independence and competence, including both physical and mental ill health. This is particularly so when the concern persists, does not respond to treatment, or there is no treatment. If help seems unavailable, a sense of hopelessness can descend. Hope and coping are inextricably linked. People who cope, but are without hope, lack vitality. People who have hope but cope poorly are unable to transform their hope into meaningful action [16].
Hope and hopelessness
Hope is a difficult concept to describe. Yet it is a most basic, fundamental and integral part of life. Where there is no hope, death follows [17, 18]. Nunn and colleagues [19] define it as ‘that construction of, and response to, the perceived future in which the desirable is subjectively assessed to be probable’ (p.531). The Macquarie dictionary puts it more succinctly: ‘expectation of something desired; desire accompanied by expectation’ [9]. It is future-orientated and expectant, involving cognitive and affective aspects of longing and believing for something that is not certain, but at least possible [20]. It is both a belief and an attitude, and in this sense inseparable from faith [21].
Hope can be generalized or particularized [22]. Generalized hope preserves the meaning of life when specific hopes are quashed, as with the diagnosis of an incurable cancer, and can enable a person to find value in the most negative situation and to accomplish things others might have thought impossible. In this way the reality of an approaching death may serve as a catalyst to reinvigorated life, to valuing of relationships and to engagement in life with purpose [18, 23].
Meaning and purpose – the assumptive world
Hope is therefore closely related to meaning and purpose. Recently, Folkman and colleagues [24, 25] have extended the model of coping to include ‘meaningbased’ coping, further emphasizing the seminal contribution of meaning in the coping process. Viktor Frankl [17], while prisoner in a concentration camp, understood the discovery of meaning – generally gained through creative endeavour and the appreciation of beauty – to be a particularly important task, and one uniquely human. However, he observed that fellow concentration camp detainees found meaning even when creative and pleasurable pursuits were limited. They displayed their yearning for life through commitments or responsibilities beyond the camp – such as family. Little things, even just being alive, had meaning beyond themselves, sustained by their ‘global meaning’ and values. Frankl called these ‘attitudinal’, referring to values and beliefs about issues that transcend everyday actions and thoughts.
The concept of ‘assumptive world’ described by Frank [11] and others [26–28] is similar, referring to beliefs and understandings about how things work in the world. Such understanding is crucial to our ability to predict the future and sustain a sense of control and security. It is related to the idea of ‘generalized hope’.
These ideas (assumptive world, attitudinal values, global meaning, and generalized hope) all refer to beliefs that transcend the immediate. Religion is an example of this. These beliefs provide stability when our control over things is threatened. However, they can also be seriously challenged by events such as major illness or bereavement, when such beliefs can be questioned and re-appraised. A breakdown in the assumptive world, with resultant loss in meaning, is a component of demoralization.
Hope has sometimes been confused with denial. Hope may be supported by a denial of reality – what has been called false hope, foolish hope or fraudulent hope [29–31]. But hope does not preclude reality. Indeed, genuine hope leads a person to face reality and to confront and overcome obstacles [32]. It has sometimes been said that confronting patients with reality (as in ‘truth-telling’) destroys hope, but this need not be so [33].
On the other hand, depression, pessimism and hopelessness – the very antitheses of hope – are often associated with negative distortions of reality [34]. What is a negative (or pessimistic) distortion and what is a positive (and overly optimistic) distortion is a matter of clinical judgement. Usually there is a range of possibilities; prognosis is never precisely known. Realistic hopefulness will look for a favourable outcome within the reality of possibilities. An optimistic disposition is good for health and wellbeing [35]. Conversely, hopelessness and helplessness are associated with poor health (discussion follows).
Demoralization and depression
In establishing the validity of demoralization as a construct, an important task is to differentiate it from depression more generally. de Figueiredo [14] has described the features that distinguish depression and demoralization; the former characterized particularly by anhedonia – the diminished ability to experience pleasure [36] – the latter by a feeling of subjective incompetence and helplessness. A depressed person has lost the ability to experience pleasure generally, whereas a demoralized person, while being unable to look forward with pleasant anticipation, may laugh and enjoy the present moment. The demoralized feel inhibited in action by not knowing what to do, feeling helpless and incompetent; the depressed have lost motivation and drive even when an appropriate direction of action is known.
This distinction is confirmed by a study of distressed patients in a primary care setting [37]. Here, hedonic capacity was preserved in the ‘distressed’ but not in the depressed patients. In our own study of psychiatric morbidity among medically ill patients, exploratory analyses of latent symptom structure identified separate dimensions of demoralization and anhedonia [38, 39]. The validity of the distinction between depression and demoralization is further supported by evidence showing that suicidal ideation, or the wish to die, is differentially associated with hopelessness and depression.
Demoralization and the wish to die
This relationship, between hopelessness and suicidal ideation, was first shown in a study of suicide attempters by Aaron Beck [40]. Since then it has been demonstrated in a number of studies of physically and mentally ill persons expressing the wish to die. For instance, Wetzel and colleagues [41] found that suicide intent in psychiatric inpatients correlated more strongly with hopelessness than with depression. In this case, when the effect of hopelessness was removed statistically, there was no association between suicide intent and depression. Studies in adolescents, however, suggest that both depression and hopelessness are independently important factors in suicidal ideation [42]. In medically ill populations it has similarly been shown that hopelessness and depression contribute independently to the desire to die [43–46].
Demoralization and physical illness
By their very nature physical illnesses are demoralizing, particularly if prolonged or difficult to treat. Such illnesses threaten the integrity of the body and the mind, and challenge a person's mastery and control. Acutely ill patients become dependent. Indeed, some degree of ‘regression’ is adaptive in acute illness, and not necessarily associated with hopelessness [47]. However, continuing illness causes patients to reduce social roles, and deprives them of avenues for satisfaction and competence. With reduction in personal efficacy, and uncertain prognosis, patients easily become demoralized. This can be further intensified through isolation if important ‘others’, as a defence against their own discomfort, withdraw emotional or material support.
Greer and Watson [48] have described helplessness and hopelessness as one of five characteristic reactions of patients to the development of cancer – the others being the development of a fighting spirit, avoidance or denial, fatalism (or stoic acceptance), and anxious preoccupation. These reactions are determined by the patient's view of their illness, their perceived control over it, and their understanding of the prognosis. Patients with early stage breast cancer and high scores on the helplessness/ hopelessness scale were shown to have increased risk of relapse and death at 5, 10 and 15 years [49]. Hopelessness has also been found to be important in other physical disease states, associated with an increased risk of hypertension [50], atherosclerosis [51], and myocardial infarction [52]. Again, this risk is independent of depression.
One of the earliest and clearest descriptions of hopelessness and helplessness occurring in the medically ill is presented by Engel [53] in the ‘Giving Up–Given Up’ syndrome. Interested to study psychological states that might predispose people to becoming sick, he and his colleagues observed this syndrome preceding the onset of physical illness. It was commonly precipitated by a loss and was characterized by a physiological slowing of bodily function (e.g. a reduced heart rate) and the affects of helplessness and hopelessness. A large literature now describes an association between depression and related dysphoric states and poor illness outcomes (e.g. [54, 55]). It is always difficult, of course, to be sure of the direction of any causal relationship – whether physical illness leads to depression or hopelessness or vice versa – but the evidence suggests that both occur.
Demoralization and suffering
We have described demoralization as not simply a syndrome of symptoms – of mixed depression and anxiety – but as a personal experience of not coping and not knowing what to do; a frightening experience that attacks one's self-efficacy and esteem. In cancer patients this is sometimes described as ‘existential distress’ [56]. It is reminiscent of the description given by Eric Cassell of ‘suffering’.
Suffering, says Cassell [57], ‘is experienced by persons, not merely by bodies, and has its source in challenges that threaten the intactness of the person as a complex social and psychological entity’ (p.639). In discussing pain (experienced by the body) and suffering (experienced by the person) he says; Suffering can include physical pain but is by no means limited to it. The relief of suffering and the cure of disease must be seen as a twin obligation of a medical profession that is truly dedicated to the care of the sick. Physicians’ failure to understand the nature of suffering can result in medical intervention that (though technically adequate) not only fails to relieve suffering but becomes a source of suffering itself. (p.639)
It is possible to treat the cancer or the pain, and to increase the suffering by not attending to the broader illness experience and its meaning. Suffering grows from any loss of a person's sense of control over their symptoms, their hope concerning their prognosis, and their expectation of other people's response to them as an ill person – whether they are accepted, even liked.
Just as physicians may concentrate on the body, so too may psychiatrists focus on the mind, treating it like an organ of the body. We observe symptoms, and in so doing may ignore the experience. Thus, psychiatrists, despite being interested in non-bodily things, may equally ignore the person – and thereby the suffering. Psychiatrists, while treating depression or other mental illness, may consequently increase a person's suffering. We are proposing here that demoralization, as one form of suffering, is experienced by the person. It cannot be fully comprehended, nor is it easily described. No structured interview or symptom checklist will truly capture its essence. People suffer and become demoralized because they have lost, or feel they are losing, something critical to their sense of self. The affects (depression and anxiety), as Cassell points out, are merely the outward expression of injury, not the injury itself.
Demoralization and mental illness
Demoralization also occurs within the traditional psychiatric setting. Frank observed, ‘Most people do not seek therapy solely because they hallucinate, fear snakes, or enjoy a few drinks too many…. Most patients are in therapy because, whatever their complaints, they or persons around them are also demoralized’ [11], p.36]. In a chronic institutional psychiatric setting, Gruenberg [58] described the failure to cope leading to feelings of impotence, isolation, despair and impaired esteem. He termed this the ‘social breakdown syndrome’. More recent work has suggested that the depression often seen in schizophrenia is related to patients’ perceptions of controllability of illness, and might usefully be considered a demoralization [59].
Engel's group, who observed ‘giving up’ in the period preceding physical illness also observed it in the context of acute psychiatric illness [60], although they also noted that it occurred at times without being followed by either physical or mental illness [53].
Frank [8] observed that anxiety and depression are the common and direct expressions of demoralization. Other psychiatric symptoms (e.g. anhedonia, hallucinations, obsessions, delusions, feelings of emptiness, psychomotor disturbance) may have a variety of explanations – genetic, neurobiological, degenerative, psychic conflict, developmental. Indeed, at times depressive and anxiety symptoms have these explanations. But, whatever the explanation, demoralization adds to the distress of the symptoms and reduces a person's coping capacity. Frustration at persisting and intrusive symptoms, the inability to find relief, the loss of hope that things will ever be different, and the loneliness of the experience leads ruthlessly to demoralization – a form of personal suffering.
We have already described the strong link between demoralization and suicidal thought and action. We believe that the common factor in people expressing the wish to die, be they depressed, personality disordered or with cancer, is demoralization with its ultimate features of hopelessness and giving-up. The tragedy of suicide is that in order to overcome some adversity in life with its attendant hopelessness and powerlessness, a person resorts to extinguishing life itself.
Helping a demoralized person
The validity and usefulness of demoralization as a construct will be determined most importantly by whether or not it guides effective intervention. There are a number of ‘ways of helping’ the demoralized person which immediately suggest themselves. Frank certainly believed that demoralization was that which responded par excellence to psychotherapy and was the reason people sought psychotherapy. We have used the phrase ‘ways of helping’ because we believe there is a risk of over-professionalizing the task of helping. Empowering and assisting the demoralized person is something that every health professional can do – be they a physician, social worker or physiotherapist (e.g. see discussion of Slavney [61]). It is done in tandem with the other healing roles. Cassell makes the point that, patients… need to talk about their illness and its effects on them… Assigning the task of listening to the patient to a psychiatrist or social worker may serve other functions, but it does not replace the patient's need to speak to the doctor caring for the disease. [62], p.247]
Having said that, there will be times when physicians and other health professionals will not feel competent to assist a severely demoralized person, and some specialist skills may be required. In Table 1 and below we sketch an outline of the most important therapeutic tasks.
Symptomatic relief is obviously pertinent. The relief of physical and mental symptoms – be they constipation, pain, depressive anhedonia, agitation or hallucinations – is the quickest way to abort the process of demoralization. Offering a specific physical treatment will also give hope. A cognitively based therapy can give information and reassurance, undertake reality testing and problem-solving, explore appraisals and particularized meaning, identify and challenge cognitive distortions, and explore global meaning, roles and purpose. A behavioural component links this exploration of meaning and purpose with goal setting and the scheduling of positive activities. These activities will assist the redevelopment of a sense of mastery and control, and encourage a re-engagement in relationships and an enjoyment of aesthetic pleasures. Perhaps the most important component is the empathic understanding of the patient, together with the time and attention given, which reduces alienation and aloneness and reinforces their value as a person.
Strategies for helping a demoralized person
This style of therapy draws on standard techniques and principles of psychotherapy. What we emphasize, however, is the value of ‘being with’ the patient, explicitly talking about those things that bring purpose and meaning to a person, and examining the ‘assumptive world’. This can raise anxieties as a person faces the need to reexamine long held assumptions. The discussion will very likely lead to spiritual and religious beliefs – an area that many psychiatrists and health professionals feel uncomfortable entering [63]. Nevertheless, in order for patients to have the courage to face some of life's most critical issues, therapists need to feel comfortable discussing these areas. We have found that patients facing the end of life often need to review aspects of their life and relationships, deal with unresolved grief and resentments, and talk about the giving and receiving of forgiveness [64, 65].
Moreover, clinicians are in a powerful role with respect to patients, who are conversely very vulnerable [66]. Just as the demoralized person can be helped, so too can they be hindered by the withholding of help. Clinicians very easily make demoralization worse by inadequate symptom relief, tactless communication of progress, inadequate listening to concerns, a dismissive attitude that devalues the patient as a person, avoidance (literally staying away), or an inability to converse on matters of importance. This can, in part, be secondary to the clinicians own demoralization and helplessness, and is why multidisciplinary teams and peer support for clinicians are very important, together with working environments that encourage reflective practice [67].
Where does demoralization fit in psychiatric classifications?
We have described demoralization as being evidenced by dysphoric symptoms (depression, anxiety, meaninglessness, hopelessness, helplessness), but in essence being an experience of a person – one of ‘not coping’, feeling distressed and alienated from others and the world. It is a process, so a person may move towards more severe demoralization and back. It is differentiated from depression but can occur in a depressed person, as well as one with psychosis, cancer or personality disorder. While often comorbid, it can occur alone, with no other disorder. In cancer patients, depressed adults, and adolescents, it has been shown to be related to the wish to die. Demoralization is therefore a concept of importance, with descriptive and predictive validity.
However, it is not a condition currently acknowledged in psychiatric classifications, and there is a problem in finding the best place for it in these classifications, which are categorical and based strongly on the principle of mutual exclusivity. Despite the recent emphasis on ‘comorbidity’ [68], it remains inappropriate to give two diagnoses that are hierarchically related or which share significant numbers of symptoms – such as Major Depression and Adjustment Disorder with Depressed Mood. Consistent with this approach, Fava and colleagues [69] do not permit a dual diagnosis of Major Depression and demoralization. In an earlier consideration of this subject [70], we also operationalized, for research purposes, that demoralization be excluded (‘trumped’ if you like) by the presence of Major Depression. This is a pragmatic solution but does not adequately represent the clinical observation that demoralization can coexist with depression – just as much as it can with cancer.
Slavney [61] has considered demoralization to be a ‘normal response to adversity’ (p.325), below Adjustment Disorder in the diagnostic hierarchy, and he concludes that it should be placed among the V Codes in DSM (i.e. as a normal reaction that is the focus of clinical attention). We believe this minimizes the importance of demoralization and find ourselves agreeing with de Figueiredo [71] that ‘although demoralization may at times be understandable,… [it] is always abnormal’ (p.449). It is clinically relevant, and deserves both recognition and treatment. de Figueiredo's solution is to place demoralization on Axis IV, identifying it with associated psychosocial and environmental stresses, ‘not to be confused with pathology’ [72], p.156]. However, we perceive this placing of demoralization with things occurring ‘outside the individual’ (Axis IV) as opposed to things occurring ‘inside the individual’ (Axes I and II) unhelpful and conceptually illogical. Demoralization is very much something happening within (an experience of) a person, albeit within the context of their environment and their coping resources. Like pathological grief, demoralization is an important clinical entity, depending on the level of disturbance and impairment. Psychiatric classifications are inadequate in both these areas [73]. Demoralization is defined by the presence of pathological symptoms in the areas of mood, hope and subjective competence. It seems ludicrous to relegate such a condition to V codes, Axis IV, or as at present, not to include it at all. We contend that it rightly belongs to Axis I. Neither, however, is it the same as an Adjustment Disorder, which, though loosely described, is a mild disturbance hierarchically below Major Depression. Demoralization can be severe leading to a desire to die, and can coexist with depression.
We recommend adoption of a diagnostic category of Demoralization Syndrome to ensure both recognition and treatment of this morbid mental state. Perhaps the issue of where it goes is not as important as if it goes. Our view is that a diagnosis of demoralization should be allowed comorbidly with diagnoses of depression, schizophrenia or any other major category. Some creative thought is required here to allow these levels of elaboration of disorder and to include dimensional concepts [74].
Conclusion
Depression, or dysphoric states in general, are familiar responses to stressful situations and commonly observed in people suffering physical or mental illness. We have described here the phenomena of demoralization that many such people experience. It occurs in the context of a severe threat that causes marked anxiety, in which the person does not know the solution. This brings feelings of helplessness, which if not assisted can lead to hopelessness and the feeling of being ‘unable to cope’. Alternatively, there may be a perception of loss of direction, role or sense of purpose, leading to feelings of pointlessness. These lower a person's self-esteem and, when coupled with social isolation or a feeling of ‘uniqueness’ (that no-one else shares the experience), leads to a sense of alienation, existential distress and severe demoralization. Frank summarizes this well: For many people the distress of a crisis or a social breakdown is compounded by the feeling that they are somehow unique, that no-one else has ever been through a similar experience, and that therefore no one really understands them. Some severely demoralized persons feel unable to control even their own feelings, and this gives rise to the fear of going crazy. The demoralized person clings to a small number of habitual activities, avoids novelty and challenge, and fears making longterm plans. The state of demoralization, in short, is one of hopelessness, helplessness, and isolation in which the person is preoccupied with merely trying to survive. [12], p.35]
Helping a demoralized person is the role of every health professional and is achieved most importantly through a relationship characterized by empathic resonance, combined with good physical care and symptomatic relief. However, even in the absence of a cure or full relief of symptoms, suffering can be substantially relieved by a restoration of self-esteem and self efficacy that comes through increased competence and human connectedness. For patients adjusting to a life threatening disease, a re-appraisal of life's goals in a way that gives coherence with global meanings, hopes and beliefs, and empowerment through attainment of these objectives will increase morale. For severely demoralized people, special psychotherapeutic support needs to be given to assist with this re-appraisal and adjustment. Much can also be done by every clinician who responds to the existential needs of a patient by staying ‘present’, and remembering that demoralization can be reinforced by apparent abandonment, criticism or dismissal.
Footnotes
Acknowledgements
This work was funded by the National Health and Medical Research Council of Australia and the Bethlehem Griffiths Research Foundation.