
Abstract
In the last decade there has been a re-appraisal of both the nature and prevalence of bipolar disorders in the community. Traditional bipolar I disorders have a reported lifetime prevalence of 0.45% [1], whereas recent studies assessing the broader bipolar spectrum of disorders have reported figures of up to 6.4% and 7.8% lifetime prevalence [2], [3].
An obvious shortcoming in comparing these results has been the absence of a standard measure of bipolar disorders. This is of particular concern, not only because of the challenge of diagnosing bipolar disorders, where there is usually a 10-year delay in instituting treatment after a person has become symptomatic [4], but there is also an enormous personal and financial impact on people afflicted with bipolar disorders [5–7].
The development of the Mood Disorder Questionnaire (MDQ) [8–11] represents an advance in providing a reliable and valid instrument to assess the prevalence of bipolar I and II disorders. This paper describes the use of this instrument in a non-American sample and reports the results of a survey of a random and representative sample of the South Australian population.
Method
Data were collected in 2004 using a Health Omnibus Survey of both metropolitan and rural South Australians at least 15 years of age using the same method as in 1998 [12]. The Health Omnibus Survey is a user-pays survey for health organizations, which in 2004 included areas such as asthma, arthritis, diabetes, incontinence and medication use. The metropolitan sample was based on the collectors' districts used by the Australian Bureau of Statistics in the 2001 census [13]. Ten dwellings were chosen in each, by selecting every fourth household from a random starting point. Only one interview was conducted per household and, when more than one person over the age of 15 resided in that household, the respondent was the person who last had a birthday.
The rural sample automatically included all towns with a population of 10 000 or more in the 2001 census with the balance selected from towns with a population of 1000. Using the same procedure as for the metropolitan sample, one person per dwelling was selected for interview.
The survey was conducted by experienced health interviewers. For reliability purposes re-interviews for selected questions were conducted on a random 10% of each interviewer's work. Data were weighted by the inverse of the individual's probability of selection, then reweighted to benchmarks derived from the 2001 census and 2002 estimated resident population [14], to provide estimates representative of the South Australian population in terms of age, sex and region (metropolitan, non-metropolitan).
The MDQ [9] was administered as part of the Health Omnibus Survey. It comprises 13 yes/no questions based on DSM-IV criteria and clinical experience and a yes/no question whether the manic or hypomanic symptoms or behaviours were experienced during the same time period. There is also a four-point scale of functional impairment varying from ‘no problem’ to ‘serious problem’. A positive screen for bipolar spectrum disorder is represented by a score of 7 or more with a ‘yes’ response to the symptoms clustering at the same time period and the symptoms had to have caused either ‘moderate’ or ‘severe’ impairment. The instrument has a reported sensitivity of 0.73 and a specificity of 0.90, in a clinical population [9], but a sensitivity of 0.28 and a specificity of 0.97 in a general population survey [11]. Nevertheless, it is considered a satisfactory screening instrument in the community.
Indicators of severity were number of days unable to work or carry out normal duties in the last month because of ill-health, suicidal ideation in the last 2 weeks and use and frequency of use of a range of services in the last month, measured as consultations with specific professionals and other community or hospital services. Respondents were asked whether they had ever taken antidepressants and specific details of any current prescribed medications were recorded. Demographic data were also collected.
Health status was assessed using the Short-Form Health Status Questionnaire (SF-36V2), consisting of 36 questions which measure eight dimensions of health: physical functioning, role limitations because of physical health, bodily pain, general health, vitality, social functioning, role limitations because of emotional health and mental health [15]. Scores range from 0 to 100 and higher scores indicate better functioning. In addition, physical and mental component summary scales can be derived. The SF-36 version 1 has been validated for use in Australia [16] and Australian norms are available for it [17]. Norms are currently being prepared for the SF-36 version 2 (G. Hawthorne, Personal communication). In addition, the SF-36V2 has a global health status question, which was also used in this study.
Quality of life was assessed using the Assessment of Quality of Life (AQoL) instrument [18]. The AQoL comprises 15 questions, which are combined into a utility score, where the scale range is from 1.00 (full health-related quality of life (HRQoL)) to 0.00 (death equivalent HRQoL) and −0.04 (worse than death equivalent HRQoL). The AQoL was developed with Australian weights and population norms are available [19].
Statistical analyses were undertaken using SPSS V 12.0.1 [20]. Respondents were classified as either MDQ-positive or MDQ-negative. The two groups were compared for each demographic characteristic and for medication use variables using the Pearson's chi-squared test. Odds ratios (OR) and 95% confidence intervals (CI) for each of the groups were calculated for the variables measuring health service utilization. A Kruskal–Wallis test was conducted to examine differences in the median number of visits to health services and the number of days off work between the two groups. For the SF-36 subscales and the AQoL utility score, manova were conducted controlling for significant demographic variables (age, sex, marital status and household size).
Results
Of the 4700 households selected, 127 were found to be vacant dwellings. From the remaining dwellings, 3015 interviews were conducted (65.9% response rate). Non-response was because of refusal (n=945), contact not being established after six visits (n=366), language barrier (n=82), the selected respondent being absent for the duration of the survey (n=58), illness (n=62), inability to gain access to dwelling (n=39) and termination of the interview (n=6).
A total of 76 respondents were MDQ-positive (mean age=37.1 (SD=13.6) years) and 2939 (97.5%) were MDQ-negative (mean age=45.5 (SD=18.9) years). Cases were more likely to be male (61% vs 39%; χ2 =4.1, df=1, p=0.04). MDQ-positive people were significantly more likely to live alone (χ2 =14.7, df=4, p<0.01) and to have either never married, be separated or divorced (χ2 =27.2, df=3, p<0.001). There were no significant differences between the two MDQ groups with respect to country of birth, Aboriginality, metropolitan or rural residence, education attainment, working status or total household income.
Regarding health status, as measured by the global health question, significantly more MDQ-positive respondents reported their health status to be fair or poor when compared with MDQ-negative respondents. For all SF-36V2 scales MDQ-positive cases scored significantly lower as shown in Table 1. As assessed by the AQoL, MDQ-positive cases obtained HRQoL scores significantly lower than MDQ-negative cases.
Health status and quality of life characteristics of MDQ-negative and MDQ-positive respondents (weighted data)
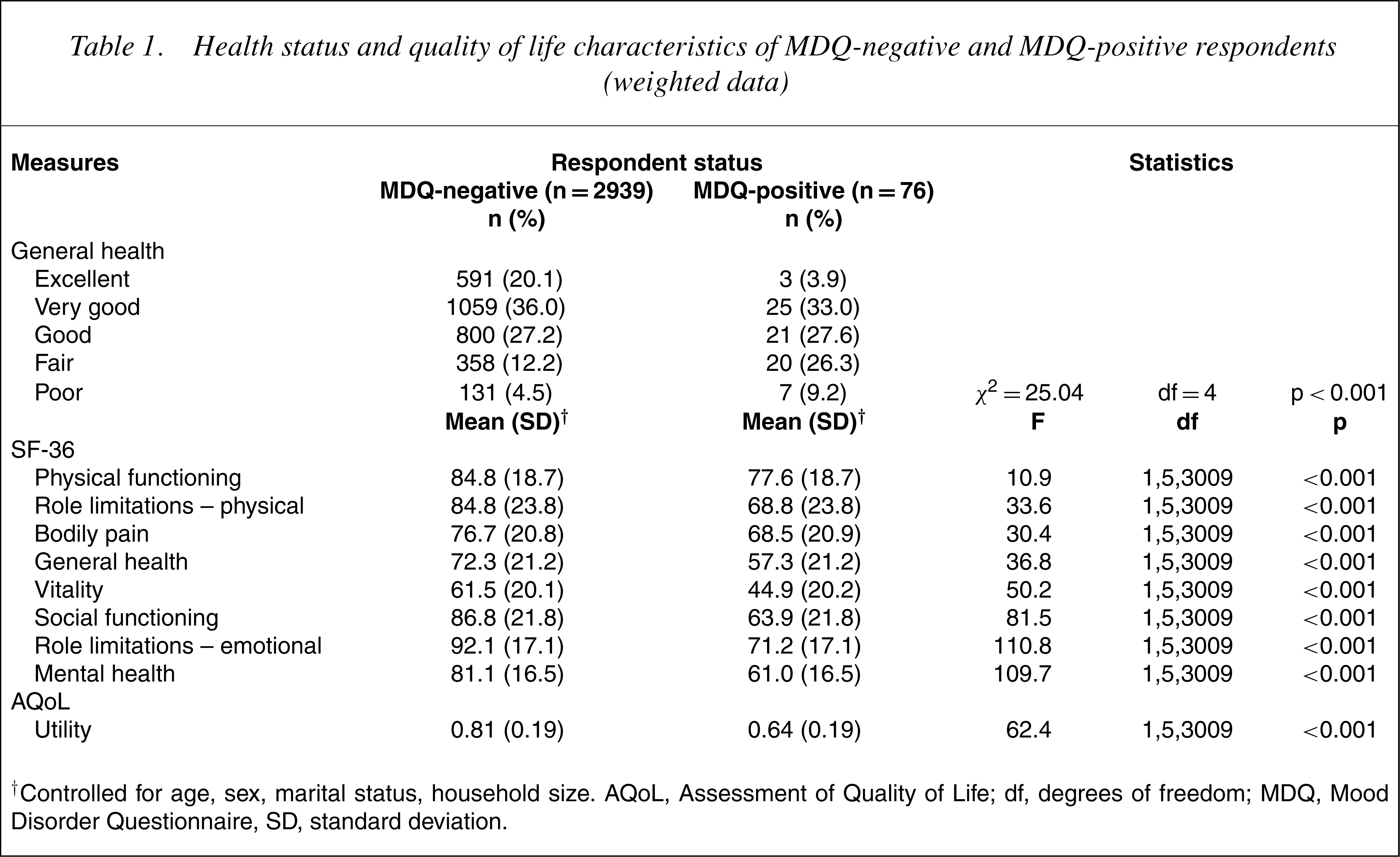
†Controlled for age, sex, marital status, household size. AQoL, Assessment of Quality of Life; df, degrees of freedom; MDQ, Mood Disorder Questionnaire, SD, standard deviation.
Compared to MDQ-negative respondents, MDQ-positive people also reported significantly greater use of psychiatrists (OR=18.4, 95% CI=9.0–37.9), psychologists (OR=14.4, 95% CI=6.2–33.2), social workers (OR=7.7, 95% CI=3.4–17.6), other counsellors (OR=4.0, 95% CI=1.4–11.8) and hospital outpatient services (OR=2.6, 95% CI=1.5–4.6) in the last month. There were no significant differences for visits to general practitioners, community health services, inpatient hospital services, other specialist doctors or therapists (including naturopaths and herbalists).
The median number of attendances at health services in the last month for MDQ-positive respondents was 2.0 compared with 1.0 for the MDQ-negative group (χ2 =13.8, df=1, p<0.001).
About two-thirds (67.1%) of the MDQ-positive group and 18.1% of the MDQ-negative group reported taking antidepressants in the past (χ2 =108.8, df=1, p<0.001). Self-reported use of individual prescribed medications showed that 23.4% of MDQ-positive and 6.2% of MDQ-negative people were currently taking an antidepressant of any type (χ2 =35.8, df=1, p<0.001), 1.3% and 0.0% were currently taking lithium (χ2 =18.4, df=1, p<0.001), and 3.9% and 1.0% were currently taking an anticonvulsant (χ2 =6.18, df=1, p<0.05).
MDQ-positive respondents had an average of 4.2 (SD=7.9) days in the past month that they were totally unable to work or perform usual daily activities, compared with 0.9 (SD=3.8) day for MDQ-negative people (the medians were 0.00 for both groups, the interquartile range was 0.00 for MDQ-negative cases and 5.00 for MDQ-positive cases; Kruskall–Wallis χ2 =66.43, df=1, p<0.01). Suicidal ideation in the preceding 2-week period was reported by 15.8% of MDQ-positive and 2.4% of MDQ-negative respondents (χ2 =49.3, df=1, p<0.001).
Discussion
These results are consistent with epidemiological studies elsewhere which have delineated a greater prevalence of bipolar disorders when a broader spectrum concept has been used. The overall prevalence of 2.5% lifetime bipolar I and II disorders is of the same order as the 3.4% (non-adjusted for non-response bias) of Hirschfeld et al. [11] in an American sample, using the same MDQ. The results are also consistent with the 2.4% lifetime prevalence of the Netherlands Mental Health Survey and Incidence Study [21]. However, they are less than the 6.4% reported by Judd and Akiskal [2] and the 7.8% reported by Angst and Gamma [3]. They are also less than the revised Netherlands data of 5.2% for lifetime bipolar and cyclothymia conditions [22].
The challenge of comparing studies is illustrated well by referring to the only other Australian epidemiological survey of bipolar disorders. Mitchell et al. [23] reported a 12-month (not lifetime) prevalence of bipolar I and II disorders of 0.5%. However, in addition to the different time period to that used in this study, they acknowledged that their figure was an underestimate because a technical problem meant that data from one of the two probe questions of their assessment instrument, the Composite International Diagnostic Interview (CIDI), could not be used. It is also pertinent that the version of the CIDI used in their survey has a number of questionable criteria which preclude a mood disorder diagnosis [24]. Bearing in mind these differences, we believe that the 2.5% lifetime prevalence for bipolar I and II disorders represents a credible assessment in this Australian population.
It is of note that there were more males classified as cases, which is consistent with the Hirschfeld et al. [11] survey reporting 3.8%males and 3.0% females compared with 3.1% and 2.0% in the current study. It is evident that those who were positive for bipolar disorders on the MDQ had a significantly greater use of health care services, more time out of role, increased suicidal ideation, reduced physical and mental health status and poorer quality of life. These findings are consistent with other studies from the US [25], the UK [26] and the Netherlands [27].
The shortcomings of the present study are acknowledged. The response rate of 65.9%, while acceptable for a population survey of this nature, may have led to an underestimate of bipolar disorders since it would exclude all those unwilling to participate because of their illness, and those in residential care, such as hostels or hospitals. It is also fair to state that the MDQ has not been specifically validated in an Australian population. However, it is free of jargon and it used DSM-IV terminology, which is widely accepted throughout Australia. Notwithstanding these caveats, we believe that the present results add to the international literature which indicates that bipolar disorders are more prevalent than had hitherto been recognized and that they represent a significant health care burden on the community.
Footnotes
Acknowledgements
This study was supported by unrestricted grants from Eli Lilly Australia, Janssen-Cilag, Lundbeck Australia, Organon Australia, Sanofi-Synthelabo, Wyeth Australia and Ramsay Health Care Australia. None of these organizations participated in the design of the study or in the analysis of data.