
Abstract
Since Wing's [1] influential paper that first used the term ‘Asperger syndrome’ (AS), interest in AS has been ignited. Gillberg [2] noted that over 160 papers on AS or autism have emerged since this time. However, only in the last decade has AS been included in the Diagnostic and Statistical Manual (DSM-IV; [3]) as a diagnostic classification. A recent review of the research literature on AS suggests that it is not an essentially different disorder from autism [4]. The primary distinction between a diagnosis of high functioning autism (HFA) and AS is based on whether the child had a significant language-delay problem before 3 years of age. However, research has been conducted on whether delayed language in children with autism can accurately predict later clinical symptoms. Two studies have cast considerable doubt over the use of early language delay as a differential criterion between autism and AS [5], [6]. There is also the opinion among clinicians that contrary to the DSM criteria, if a child meets criteria for both autism and AS, the child is given the diagnosis of AS [7].
Within the normal population there appears to be a high prevalence of anxiety disorders making them one of the most common types of childhood psychopathology [8]. Currently, there is no available data on the prevalence rate of anxiety within the AS population, although it is reported to be a significant problem for many children [9–11].
Attwood [12] believes that anxiety arises in individuals with AS over a range of issues, including changes in routine and expectations, apprehension in social situations and minor environmental changes. Many children with AS experience difficulty with change because they have poor comprehension of occurrences in their surroundings, resulting in uncertainty and anxiety [10]. Children with autistic spectrum disorder (ASD) can experience intense anxiety when prevented from engaging in their usual routines [9] and fear of future change can be a further source of anxiety [10]. The ritualistic, stereotyped characteristics of AS (e.g. echolalia, rocking, hand flapping) may be interpreted as coping mechanisms or alternatively, as outcomes of experiencing anxiety [13].
Although few empirically based studies have investigated the role of anxiety within the AS population specifically, Kim et al. [14] conducted a study that examined anxiety in children with AS and autism. Their data revealed rates of generalized anxiety and separation anxiety significantly higher than the normal population. The level of generalized anxiety was similar for children with classic autism and AS.
Additional research examining anxiety and social worries in children with ASD investigated a wider range of anxiety symptoms: panic and agoraphobia, separation anxiety, physical injury fears, social phobia, obsessive– compulsive disorder and generalized anxiety disorder [15]. This research compared high functioning children with autism, children with specific language impairment and a normally developing sample. Results revealed that the autism group displayed significantly higher overall anxiety and social anxiety than the other groups. Their levels of obsessive–compulsive disorder (OCD), separation anxiety, panic and agoraphobia and physical injury fears were higher than the other two groups [15]. The differences found between types of anxiety for ASD and normally developing children suggest that the pattern of anxiety is different in the two populations.
Clinical experience suggests that people with ASD are often regarded as unreliable informants due to the lack of self-reflectiveness and inaccurate perception of their differences in relation to others [16]. Research using people with high functioning autism suggests that they are less able to understand and express emotions than normally developing people [17], [18] and often lack insight into their social and emotional problems [19].
Koning and Magill-Evans [20] investigated perceived social skills in children with AS and found that they rated themselves considerably higher than did their parents and teachers. The authors suggested that children with AS demonstrate little insight into their difficulties, perceiving normality in their abilities; however, corroborating parent and teacher ratings show this to be inaccurate. It is suggested that parent interviews provide the most accurate and important information [16].
A study of social anxiety in children with high functioning autism also found that parents reported higher levels of social worries in their children than the children themselves [15]. Statistical testing was not employed in this study; however, it provides evidence that some children with ASD experience a lack of insight into the social difficulties that characterize the syndrome. A similar study found children with ASD and their parents differed markedly when rating the incidence of psychiatric disturbances in the children [21].
The current study examines anxiety and social worries in a group of children with AS. Concomitant with previous findings [14], [15] and clinical observation [12] and using parent and child reports, it is predicted that children with AS will be higher on overall levels of anxiety than normally developing children. Based on findings by Gillott and colleagues and using parent and child reports, it is predicted that children with AS will also experience more social worries than normally developing children.
No research has been conducted that compares children with AS to children who have received a diagnosis of clinical anxiety. The current study proposes to explore whether children with AS have similar levels of overall anxiety to children diagnosed with clinical anxiety and, furthermore, whether differences between these two groups are apparent on six specific anxiety subscales.
In concordance with the literature suggesting a lack of agreement between parent and child ratings, it is predicted that there will be significant discrepancy between child and parent ratings on the anxiety measure for children with AS. It is expected that the parents will rate their children as having more anxiety than do the children.
Method
Participants
The sample consisted of 65 children (55 male and 10 female) aged from 10 to 13 years. Participants were recruited as part of a larger study evaluating the efficacy of an anxiety intervention. Although this program was designed to teach children with AS to manage anxiety, none of the participating children had a diagnosis of anxiety. The children were recruited on the basis of parent-reported anxiety. All participants had a diagnosis of AS from a paediatrician or psychiatrist and were further screened for inclusion in the study using the Childhood Asperger Syndrome Test (CAST; [22]). Only those children who also met criteria for AS on the CAST were included in the current study. Participants were recruited through a children's hospital, psychology clinics and media release within the metropolitan area of Brisbane, Australia.
Data from previous studies were used for comparisons between children with AS, normally developing children and children diagnosed with clinical anxiety. Child self-report data from normally developing children and children diagnosed with social phobia (the clinically anxious group) on the Spence Children's Anxiety Scale (SCAS; [23]) was obtained from Spence [8]. Data from parent reports on normally developing children and clinically anxious children on the SCAS was obtained from Nauta et al. [24]. The current sample was also compared with normally developing children on The Social Worries Questionnaire [25] using both parent and child reports. Comparative data on this measure was obtained from Gillott et al. [15] for this purpose.
Measures
Both parents and children completed questionnaires: parent and child forms of the Social Worries Questionnaire (SWQ; [25]), the SCAS [23] and the CAST [22].
Social Worries Questionnaire – parent and pupil versions
The SWQ was employed to assess behavioural indicators of social anxiety in children. The parent version has 10 items that examine a parent's perception of their child's worry or avoidance of social situations. The pupil version has 13 similar items that are administered to the child. The items in each version are rated in terms of worry experienced in each situation and range from 0 (not true) to 2 (mostly true) with high scores indicating greater worry. Both versions demonstrated high internal consistency (coefficient alpha of 0.82 and 0.85, respectively).
Spence Children's Anxiety Scale
The SCAS is a self-report measure that examines symptoms relating to six types of anxiety in children including separation anxiety, obsessive–compulsive disorder, panic-agoraphobia, social phobia, generalized anxiety and physical injury fears. The SCAS has both a parent and child version each with 38 items. The items are rated on a 0 (never) to 3 (always) scale with high scores representing greater levels of anxiety. The parent and child versions of the SCAS had high internal reliability coefficients (0.92 and 0.91, respectively) with the population in the current study. The internal reliability coefficients for the six subscales of the SCAS ranged from adequate to excellent.
Childhood Asperger Syndrome Test
The CAST examines a number of behavioural indicators that are representative of DSM-IV central features of the autism spectrum, for example, repetitive or stereotyped behaviours and social and communication impairments. The measure consists of 37 items of which 31 are scored and contribute to the total score (maximum of 31) and six are non-scored, filler items. The questionnaire is designed for parents and requires yes or no answers. The cut-off score of the CAST is 15, based on results of the pilot study of this questionnaire, which revealed that normally developing children scored below and children with a diagnosis of AS scored at or above this point [22]. Although the CAST is a new measure it was shown to be an adequate screening measure of the autistic spectrum disorders (22). The internal reliability coefficient for the CAST was adequate at 0.64.
Procedure
The questionnaire administrationwas conducted at the School of Psychology at the University of Queensland (Brisbane, Australia). Questionnaires were administered orally to each child in a quiet room with no distractions. Parents were asked to fill out a general demographics information sheet and their questionnaires in a group setting.
Results
Data and analyses
Data screening using SPSS frequencies revealed that the distribution was normal and homogenous with no missing data. Analyses were conducted with and without univariate outliers revealing no significant differences, thus all data were retained for analysis. Analyses conducted included independent groups t-tests and anova. A Bonferroni correction was also applied to account for multiple analyses.
Differences in overall reported anxiety: children with Asperger syndrome versus normally developing children, parent and child reports
Independent groups t-tests revealed that children with AS rated their overall levels of anxiety as significantly higher (M=30.49) than normally developing children (M=18.80), t(83)=2.75, p<0.01. According to parent reports, children with AS have more overall anxiety than the normative sample t(324)=17.61, p<0.0001.
Differences in overall reported anxiety and between the six anxiety subscales: children with Asperger syndrome compared to clinically anxious children, parent and child reports
Individual t-tests were conducted to examine total anxiety scores and specific anxiety symptoms in children with AS compared to clinically anxious children using child ratings. No differences between the groups were found on either total anxiety or the subscales.
A significant difference was found between children with AS and clinically anxious children on parent ratings of total anxiety, p<0.001. Parents also reported children with AS as having significantly higher levels of obsessive compulsive symptoms than clinically anxious children, t(547)=2.32, p<0.05 and they were also considered by parents to have higher levels of physical injury fears than clinically anxious children, t(547)=2.18, p<0.05. Results are shown in Table 1 with the normative sample means provided for comparison purposes.
Parent ratings of anxiety in children with Asperger syndrome, clinically anxious children and a non-clinical sample
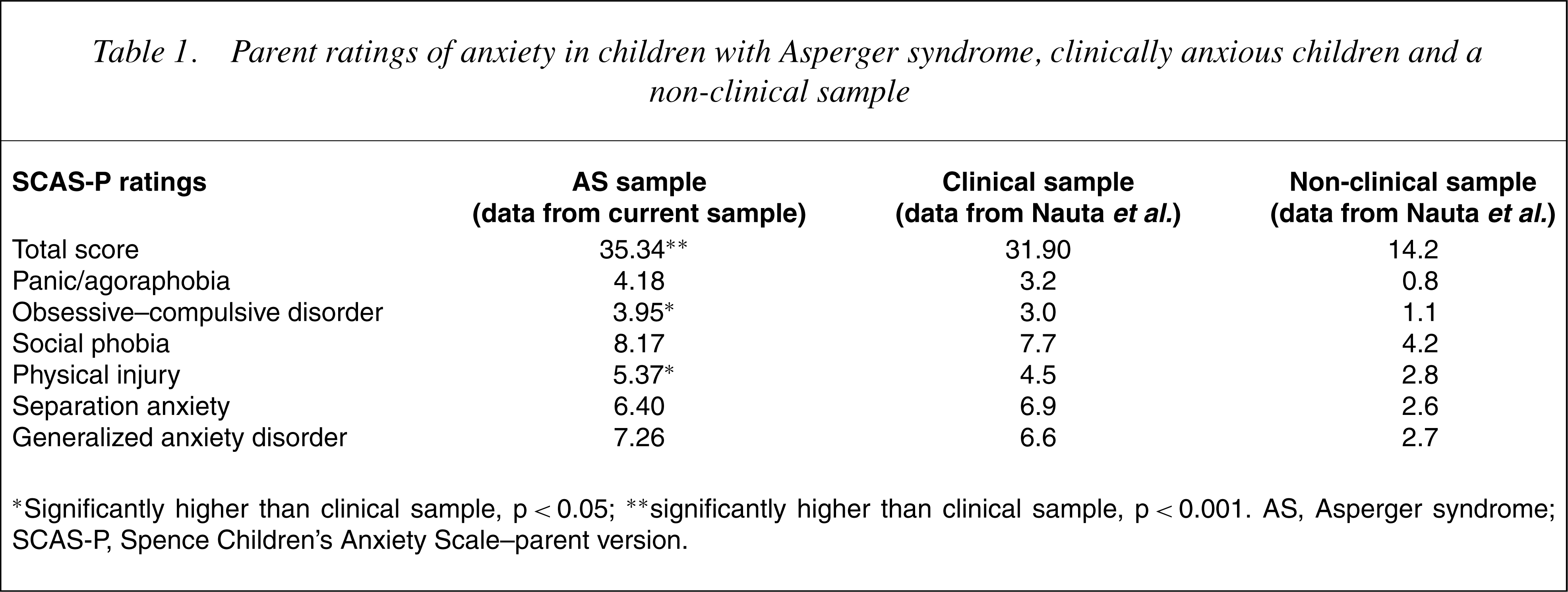
∗Significantly higher than clinical sample, p<0.05; ∗∗significantly higher than clinical sample, p<0.001. AS, Asperger syndrome; SCAS-P, Spence Children's Anxiety Scale–parent version.
Reported differences in social worries: children with Asperger syndrome versus normally developing children
Independent groups t-tests were used to compare parent reports of children with AS and parent reports of normally developing children on number of socialworries. Analysis revealed that parents of childrenwith AS reported significantly higher levels of social worries than normally developing children (t(78)=5.44, p<0.001). Comparison of children's reports revealed no significant difference in social worries between the two groups. Results can be seen in Table 2.
Social worries for children with Asperger syndrome (AS) and a normal sample using parent and child ratings
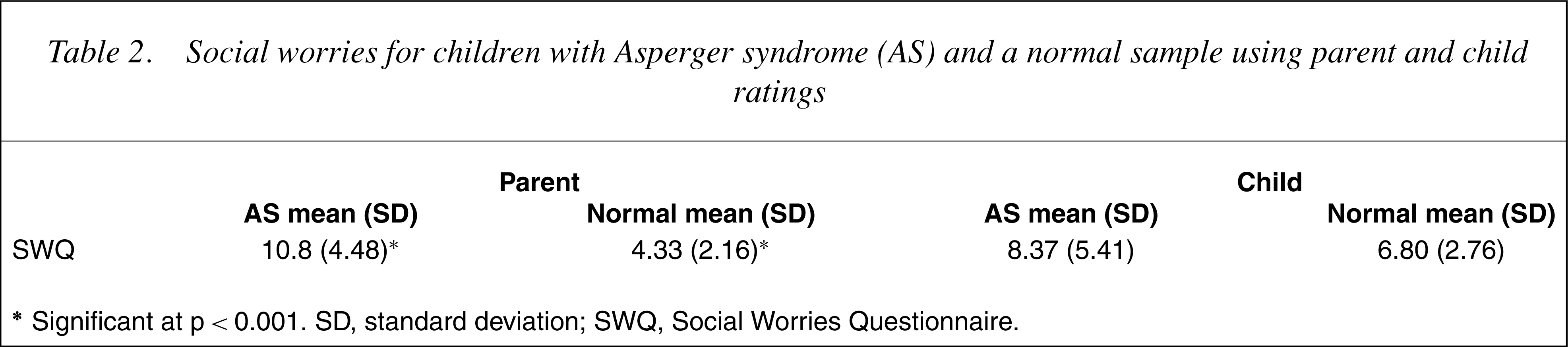
∗Significant at p<0.001. SD, standard deviation; SWQ, Social Worries Questionnaire
Parent versus child ratings on the six anxiety subscales of the Spence Children's Anxiety Scale
To compare child and parent ratings on the SCAS, anova was used with two levels of rater (parent and child) and six levels of anxiety (six subscales). A significant rater×anxiety subscale interaction was found F(3, 61)=31.31, p<0.0001. Post-hoc comparisons revealed a significant difference between parent and child ratings of separation anxiety, (p<0.0001), obsessive compulsive symptoms, (p<0.0001), social phobia, (p<0.0001) and generalized anxiety, (p<0.01) with parent ratings significantly higher on each occasion except for obsessive compulsive symptoms (Fig. 1).
Means comparison of parent versus child ratings of anxiety on the Spence Children's Anxiety Scale (SCAS) and SCAS-P subscales.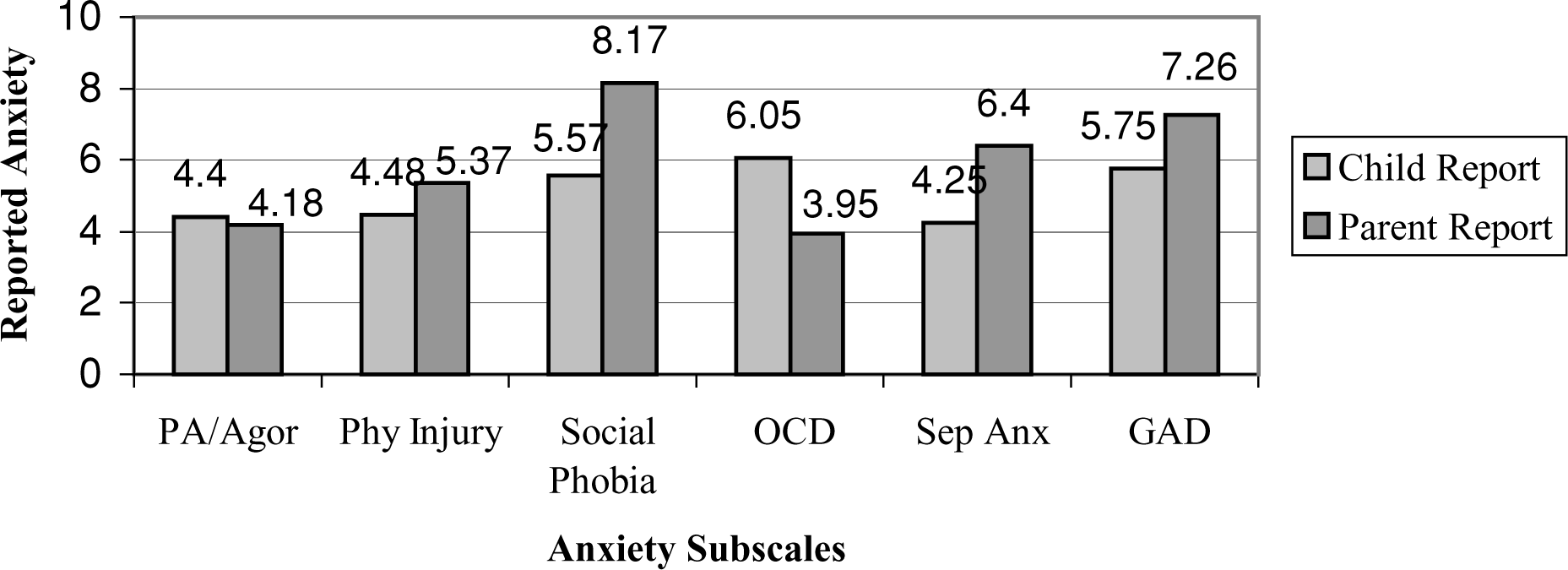
Discussion
The current study examined parent and child reports of anxiety in children with AS compared with normally developing and clinically anxious children. Parent and child reports of anxiety in children with AS were also compared.
Anxiety and social worries in children with Asperger syndrome according to parent and child reports
According to parent and child reports, the results support the hypothesis that childrenwithASexperience more overall anxiety than normally developing children, supporting previous findings [15]. Support was found for the suggestion that children with AS experience more social worries than normally developing children according to parent ratings; however, this result was not found for child ratings. These results only partially support previous research which found that in a sample of children with autism, both the parents and the children reported more social worries than a normally developing sample [15]. The current finding supports the view that children with AS may lack insight into their difficulties [17–20] and that parent reports are more accurate [16].
An aim of this study was to examine the degree of anxiety experienced by children with AS compared to a clinically anxious sample, using both parent and child reports and to investigate whether differences exist between specific subtypes of anxiety for these two groups. Results revealed no differences on child ratings between children with AS and clinically anxious children on either overall anxiety or specific subtypes. Children with AS described themselves as being just as anxious as a clinically diagnosed group of anxious children.
Parent ratings also revealed no differences between the two groups on overall anxiety, although parents of children with AS endorsed significantly more obsessive–compulsive symptoms and physical injury fears than the clinically anxious children. The higher levels of OCD could be interpreted as a reflection of the general characteristics of the syndrome (i.e. unusual and repetitive routines or behaviours). Previous literature has suggested children with AS may use their repetitive, ritualistic behaviours as a means of reducing their anxiety [26] or that they occur as a consequence of experiencing anxiety [13]. Despite the fact that no child in the present study was diagnosed with clinical anxiety, they presented with similar and in some cases greater anxiety than the clinically anxious sample.
Physical injury fears were also endorsed more frequently in children with AS than clinically anxious children. The reason for this may be that children with AS have a heightened physical sensitivity to noise and touch and can often find touch of any kind distressing [12]. Children with AS often become distressed by the normal activities of the school environment and are also at increased risk of being bullied. These situations may provoke anxiety and fear surrounding the possibility of physical injury.
Although the children with AS reported levels of social phobia similar to clinically anxious children, they did not report high levels of anxiety on the social worries measure. As suggested by Gillott et al. [15] the items on the SCAS relate to covert internal states (i.e. worries about other's perceptions) while the SWQ examines worry surrounding overt actions (i.e. asking a group if I can join in). Children with AS are known to approach others to play, join in games or start conversations [12]. They may experience little social anxiety during initial social interactions but distress may result from rejection [13]. The children in the current sample may be too young to recognize that lack of social skills and unusual social interaction may be the explanation for their social rejection. It is suggested that as children grow up they will eventually identify this pattern and may display anxiety surrounding the more overt social actions. This may explain why the children with AS reported less anxiety surrounding engaging in social interaction but reported more anxiety surrounding the internal, ‘feeling’ state reflected in the SCAS.
Comparison between parent and child ratings of anxiety in children with Asperger syndrome
The current study predicted that parents would report more anxiety in their children than the children themselves. The results partially support this hypothesis, revealing significant differences between parent and child ratings on four of six anxiety subscales. Parents rated their children with significantly more separation anxiety, social phobia and generalized anxiety than did the children. This finding is similar to previous suggestions that there is often little concordance between children and parents regarding diagnoses [27]. The children may be under-reporting, supporting suggestions that children with AS may have reduced insight into their difficulties [17–20] and that parent reports are more reliable [16].
Conversely, the children rated themselves as having significantly higher levels of obsessive–compulsive symptomatology than did the parents. Obsessive–compulsive symptoms are often covert and children could be experiencing high levels of these covert symptoms without parents being aware, explaining the discrepancy in the results.
Clinical implications
The results of this study offer some support for the suggestion that children with a diagnosis of AS may exhibit heightened levels of anxiety. If this is the case then further study of the impact of both psychological and pharmacological interventions for the population is warranted. A cognitive behaviourally based program developed specifically for children with AS has shown very promising results [28]. This study used both interventions with the child in a small group setting and training of parents as cotherapists. A small study that trialled the use of selective serotonin re-uptake inhibitors (SSRIs) in children with pervasive developmental disorders (PDDs) found mixed results [29]. Although several children showed improvement in symptomatology as reported by parents, others showed a worsening of symptoms. The author concluded that the higher functioning children such as thosewith AS responded better than those with a more severe presentation. Amore recent study also examined the effectiveness of SSRIs with a small group of children and adolescents diagnosed with PDDs and found that 66% showed improvement in anxiety symptoms [30].
Limitations and future research
One limitation of this study is that none of the children with AS had a clinical diagnosis of anxiety. As suggested here and by others (e.g. [16]), childrenwith AS are known to be poor at acknowledging and reporting anxiety. However, considering the parent reports on the SCAS-P, with no differences found between the children with AS and children diagnosed with clinical anxiety, it suggests that many of these undiagnosed children may meet criteria for an anxiety disorder.
It should be acknowledged that while the measures used showed good internal reliability, there were no external measures of validity and so the findings should be viewed with some caution. The sample size used in this study while adequate is not large and further data should be collected to clarify some of the issues raised regarding specific subtypes of anxiety such as obsessive–compulsive tendencies.