
Abstract
The changing role of acute hospital care within modern mental health services places greater responsibility on the patient's family and friends, yet there is a lack of research investigating carer perceptions and involvement with the treatment [1]. The length of hospital stay has decreased and the level of acuity has increased, resulting in greater workloads and demands on available resources [2]. The reduced number of beds and shorter hospital stays mean that those in inpatient care are often seriously ill [3] and that some patients continue to experience acute symptoms even when discharged.
The continuity and collaboration between inpatient and community services and the involvement of patients and carers in all phases of treatment before discharge are crucial to delivering positive outcomes for mental health patients and their carers. The transition from hospital to community is a particularly high-risk period for many patients and during this time continuity of care is of paramount importance. Fortney et al. [4] emphasize that discontinuity of community care places patients at the risk of premature readmission to hospital and involvement in criminal activity. Coordinating post-discharge services can be challenging as patients, carers and health professionals may have different perceptions about which services are needed and what to expect from these services [5]. It is therefore important that the differing expectations of patients and carers are taken into account in discharge planning [6].
The key problems identified in integrating inpatient and community care seamlessly are poor communication and lack of coordination between healthcare workers and inadequate provision of information to patients and carers [7]. Holst and Severinsson [8] report that mental health professionals identified the following needs regarding collaboration between inpatient and community staff: (i) the need for professionals to have a shared understanding; (ii) the need for collaboration within community health and links to inpatient care to evaluate the success of interventions; and (iii) the need for team collaboration to improve the quality of care. Furthermore, carers' input must be solicited and respected [5], [9], whether they are family members or close friends [10].
Clearly, many patients rely on carers for support, mandating carer involvement in discharge planning and community care. However, if carer support is to be viewed as an integral part of mental health care, it becomes necessary for carers to be given relevant and timely information and for healthcare workers to consult with them. Despite the importance of both patient and carer input in achieving positive mental health outcomes, there has been negligible research on the extent of carer involvement and on the differing perceptions of the two groups regarding information and resource needs. This study sought to address these issues by asking the following questions:
Method
Design and setting
In order to obtain a representative sample of patients across an integrated mental health service, all patients being discharged from acute inpatient services over a 3-month period were assessed for eligibility, and in community settings a random sampling method was used. Each of the six community mental health centres in the area were visited at least eight times over a 2-month period, and all patients visiting the centres on those days were assessed for eligibility.
The exclusion criteria applicable to both settings were: patients aged ≤17 years or ≥65 years, non-English-speaking patients and patients diagnosed with early dementia, cognitive deficit, eating disorder or primary substance abuse. Additional exclusion criteria for inpatient settings were a stay of less than 5 days or more than 6 months and patients living out of the area or with no fixed abode. The exclusion criteria specific to community settings were first presentations and admission to inpatient services during the inpatient data collection period. This ensured patients were not interviewed more than once. All patient interviews were conducted face-to-face by the same researchers (MC and AF).
Measures
Versions of the discharge planning survey and the community care survey were developed from a previous study [11]. Both surveys included demographic information. The line ofquestioning then diverged, with inpatient surveys asking about satisfaction with discharge, the provision of discharge-related information, confidence in managing mental health problems post-discharge and information requirements. Surveys administered to patients in community settings asked about the helpfulness of information provided, confidence in managing mental health problems and information requirements.
At the end of the interview, patients were asked to nominate a carer (for the purposes of this study, defined as a parent, partner, relative or friend involved in their care) who had been involved in their care during the previous 3 months. If the carer was able to read, write and understand English, the patient was then asked about their relationship to this person, their living arrangements and whether a questionnaire could be sent to them. Patients were invited to address an envelope and stamps were provided for the survey's return. Carers' surveys were matched by a number, so responses could be compared while protecting the respondent's identity.
In the carer surveys, questions were asked regarding demographic information, employment status, length of time as a carer, frequency and mode of contact with the patient and the impact of caring on key life areas. Other questions required carers to rate their satisfaction with involvement, the information provided to them, and confidence in the patient managing the patient's mental health and information needs. In addition, patients and carers were asked about their support needs and carers were asked about the burden of care; these findings will be reported in a separate paper.
Data were analysed using the Statistical Package for Social Sciences (SPSS) V 10. Descriptive data are presented as response rates, percentages, frequencies and means. Comparisons were made between hospital and community patients and between patient and carer ratings of the helpfulness of information and confidence levels. Categorical variables were analysed using the Pearson's χ2 test for independence and group differences for continuous variables were analysed using one-way anova.
Results
There were 1085 admissions to all wards visited during the study period. However, because of many patients having more than one admission, this translated to 629 individuals being on the wards during this time. Of these, 53% (n =334) were ineligible for interview for the following reasons: out of area or no fixed abode (n =133, 40%); discharged or on leave within 5 days of admission (n =113, 34%); or fulfilling one of the exclusion criteria (n =88, 26%). Of the 295 eligible patients, 17% were discharged before they could be interviewed and 13% declined to participate. Thus, 207 individuals were interviewed, resulting in an inpatient response rate of 70%.
In community settings, 341 patients were approached, of whom 73 (21%) were ineligible because they were hospitalized during the study period (n =30, 41%), did not understand English (n =23, 32%), experienced their first presentation(n =14, 19%), or were outside the age range (n =6, 8%). Of the 268 eligible patients, 68 (25%) declined to participate, resulting in a community response rate of 75%.
The surveys were not sent to carers who were unable to read, write or speak English (n =29), or if the patient preferred the survey was not sent (n =68). Across both settings, 67% (n =274) of patients identified a carer; 65% (n =177) of these were sent a survey and the response rate was 28% (n =50).
Respondent profile
The patient and carer demographics for inpatient and community settings are presented in Tables 1 and 2. Overall, with the exception of the number of times admitted to hospital, the demographics of patients in inpatient and community settings were not significantly different. There were also no significant differences in the demographics of carers of hospital and community based patients.
Sex, age, country of birth, marital status, accommodation and hospital admissions for inpatient and community participants
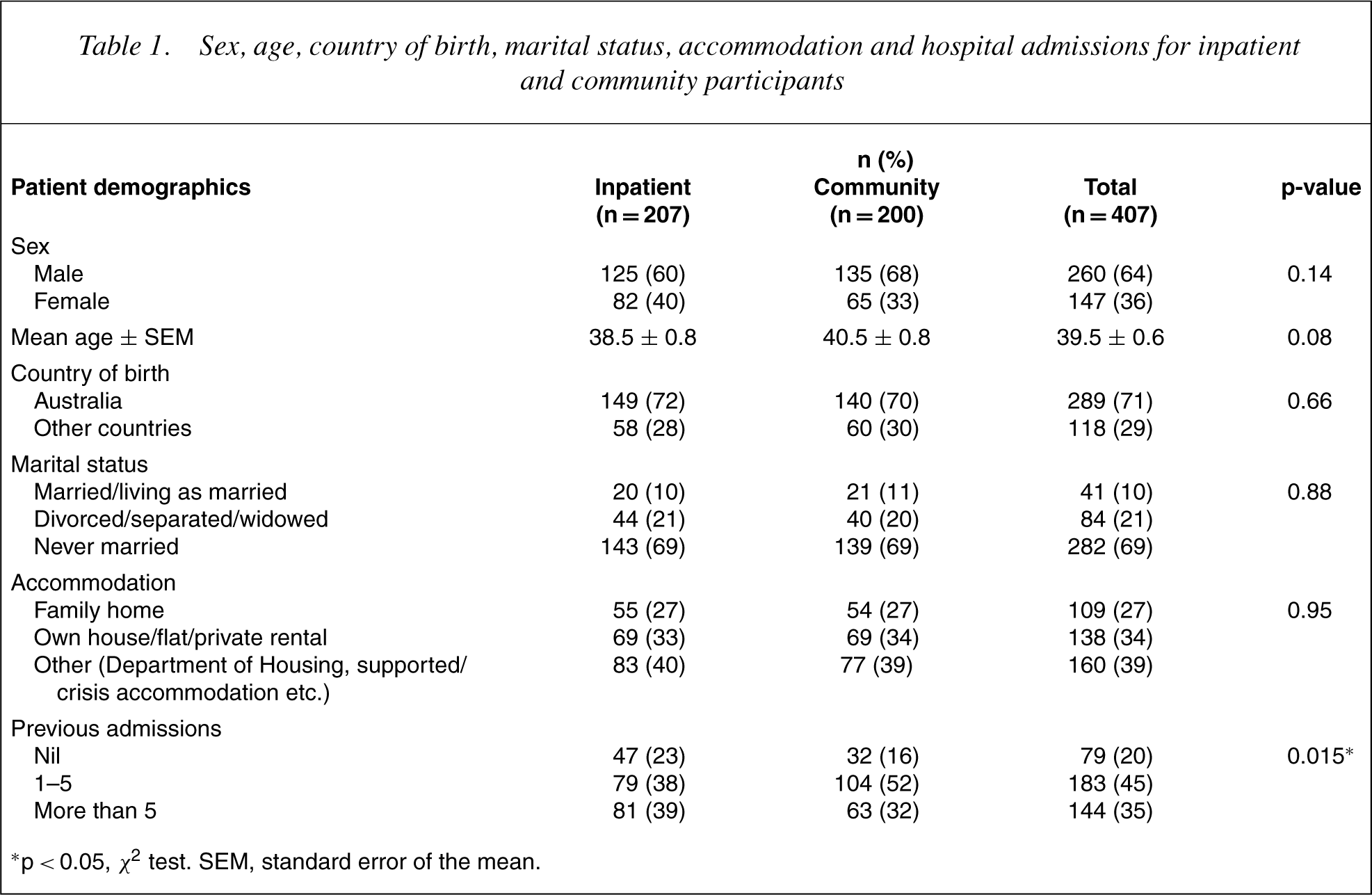
∗p< 0.05, χ 2 test. SEM, standard error of the mean.
Sex, age, country of birth, marital and employment status, number of people in household and length of time providing care for carers of hospital and community patients
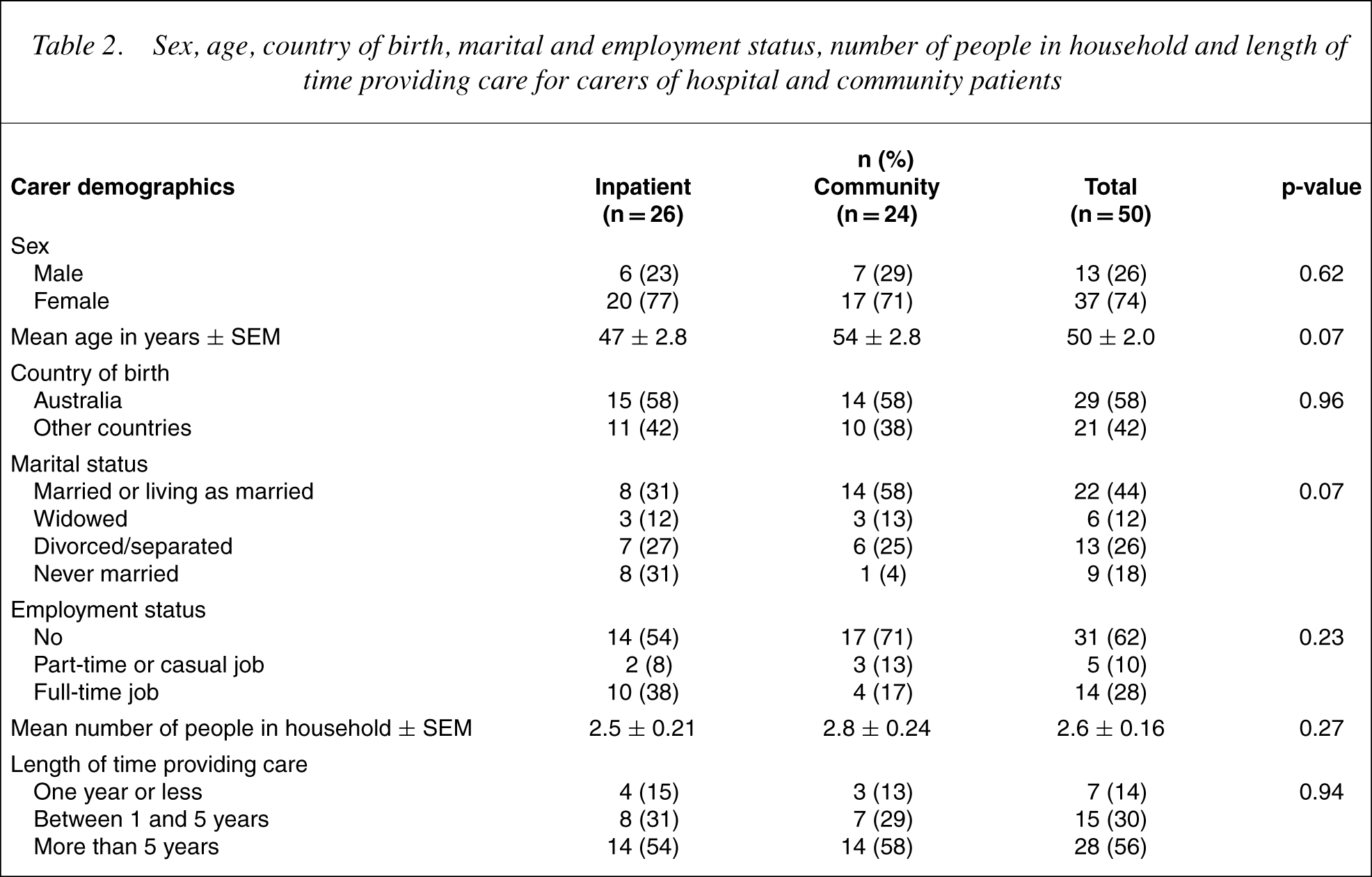
With regard to the relationship of the carer to the patient, half the carers were a parent, 32% were a spouse, partner or other relative (sibling, aunt, uncle, grandparent) and 16% were a girlfriend, boyfriend or other friend.
Inpatient settings: patients and carers
Ratings of information provided
Almost one-third (30%) of inpatients indicated that their discharge arrangements had been explained, 71% were satisfied with their involvement and 72% were satisfied with the arrangements. Twothirds (62%) of inpatients were regularly seeing a mental health worker such as a case manager or psychiatrist before they were hospitalized.
With regard to carers, 32% were consulted or involved in decisions about medication and 40% were consulted or involved in discharge decisions. Less than one-third (31%) of carers were satisfied with their involvement in discharge planning whereas 35% indicated they were not involved or contacted about this issue.
Table 3 presents patient and carer ratings of the discharge information provided. Carers reported that they were given less information than patients and, when it was provided, three-quarters of carers thought it was unhelpful.
Ratings of information provided to patients and their carers
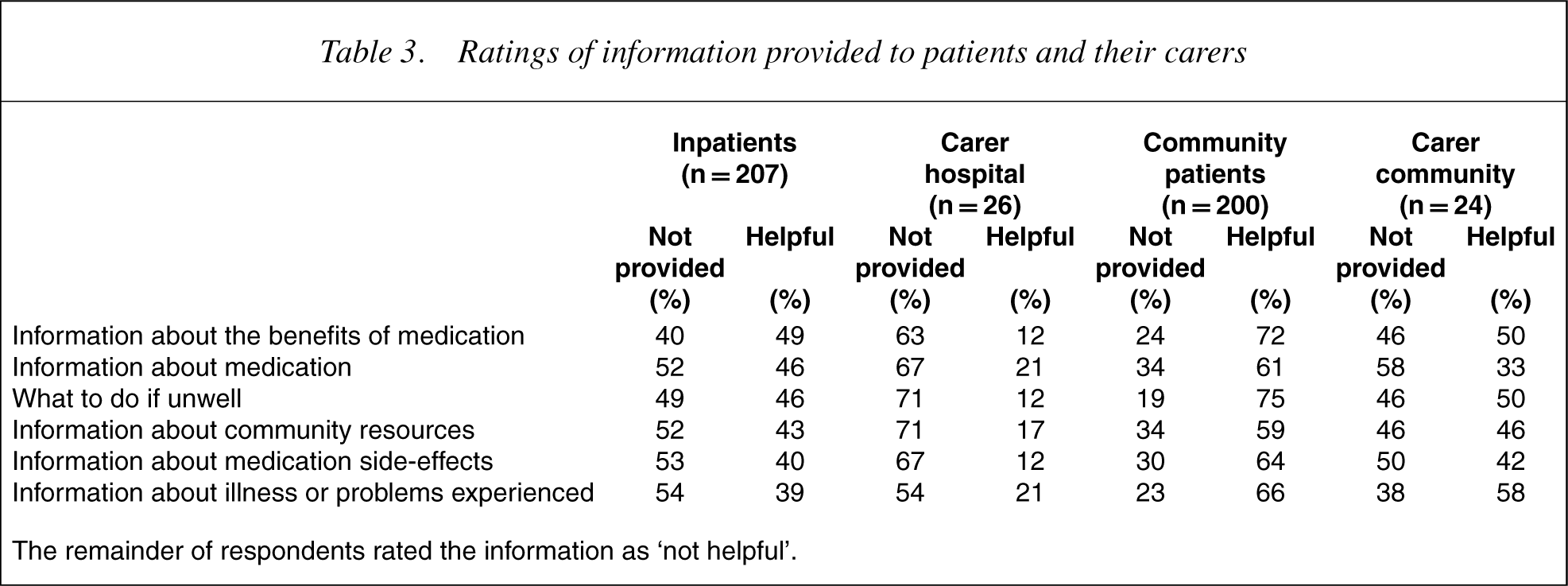
The remainder of respondents rated the information as ‘not helpful’.
Resources that would help with discharge planning and confidence following discharge
Overall, carers wanted resources to help with discharge planning more frequently than patients. Resources identified were: steps to take if feeling unwell (patients 49%; carers 100%); meeting the case manager before discharge (patients 48%; carers 69%); information about medication and side-effects (patients 47%; carers 81%); written information about discharge arrangements (patients 43%; carers 77%); ideas about how other people deal with similar problems (patients 40%; carers 62%); opportunity to attend information sessions about discharge issues (patients 40%; carers 58%); written agreement between key people involved with care (patients 37%; carers 46%); and discussing discharge arrangements with a consumer consultant (patients 33%; carers not asked).
Table 4 presents the results of patients' and carers' ratings of confidence in undertaking a range of activities. Across all activities, the patients' confidence ratings were higher than those of carers.
Confidence in community living between carers and patients
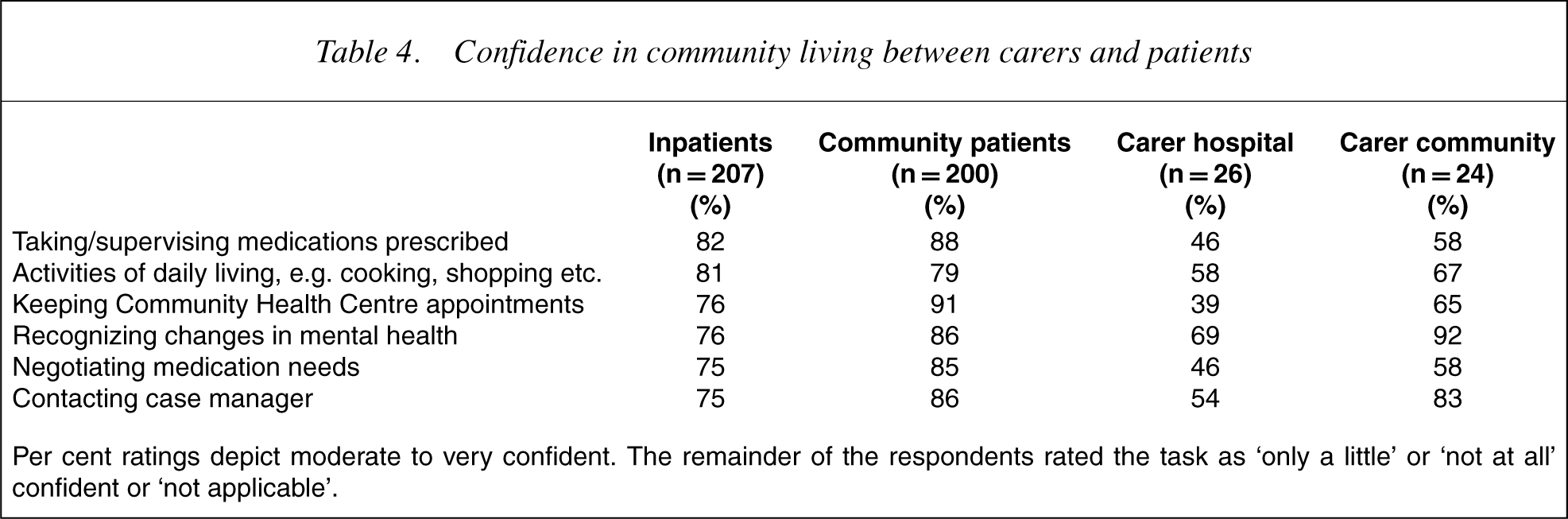
Per cent ratings depict moderate to very confident. The remainder of the respondents rated the task as ‘only a little’ or ‘not at all’ confident or ‘not applicable’.
Overall, carers also wanted more general information than patients: in relation to community resources (patients 40%; carers 73%); how to access general practitioners (patients 40%; carers 58%); patient support groups (patients 39%; carers 39%); mental health problems (patients 37%; carers 77%); training or employment opportunities (patients 34%; carers 46%); physical health (patients 34%; carers 50%); how to get on with family and friends (patients 33%; carers 58%); housing issues (patients 30%; carers 50%); and making new friends (patients 30%; carers 50%).
Community settings: patients and carers
Ratings of information provided
As with inpatient settings, more carers than patients indicated that information was not provided (Table 3). Where information was provided, a similar percentage of patients and carers rated the information as ‘not helpful’, and the percentage of patients and carers rating information as helpful was higher than in inpatient settings. The difference in the proportions of patients and carers rating information as helpful was not as pronounced as in hospital settings, although percentages were still higher for patients than carers.
Resources that would help with community living and confidence in managing
Overall, more carers than patients wanted resources to help with community living. Areas identified were: steps to take if feeling unwell (patients 34%; carers 71%); information about medication and side-effects (patients 32%; carers 67%); ideas about how other people deal with similar problems (patients 28%; carers 50%); opportunity to attend information sessions about key mental health issues (patients 27%; carers 46%); written information about community health services (patients 26%; carers 54%); a written agreement between key people involved with care (patients 18%; carers 42%); and meeting with a consumer consultant or staff member from the community team (patients 18%; carers 63%).
Seventy-one per cent of carers were moderately or very confident in managing the patient at home. Similar to the findings in inpatient settings, patients were more confident in managing community living than carers, although differences between patients and carers were not as pronounced (Table 4).
Patients and carers were also asked about other information considered important. Again, more carers wanted information than patients: community resources (patients 30%; carers 92%); mental health problems (patients 26%; carers 62%); physical health (patients 26%; carers 54%); training or employment opportunities (patients 25%; carers 54%); housing issues (patients 25%; carers 42%); consumer support groups (patients 23%; carers 42%); getting on with family and friends (patients 20%; carers 42%); and how to access general practitioners (patients 19%; carers 58%).
Discussion
The importance of facilitating active carer involvement in mental health care is borne out by the fact that nearly one-third of patients surveyed in the current study were living in the family home and a similar proportion had been admitted to hospital more than five times. In hospital settings, we found that more than 50% of carers reported that information was not provided and, when it was, manyindicated it was unhelpful. Similar results were recorded in community settings, although the percentages of patients and carers rating information as helpful were higher. The hospital staff may be prevented from providing more information because of the unpredictable and stressful environment and short stays [2]. Alternatively, information may be provided in different formats in hospital and community settings. The fact that staff–patient relationships are not time-limited in the community may also provide greater opportunity for the sharing of information. Carers have a more positive view of hospital care when they feel informed, have the opportunity to discuss treatment and know its aims; furthermore, for many patients, family involvement is reassuring [12].
Research suggests that linking patients to community services while they are in hospital, improving communication between hospital and community teams and increasing the involvement of family and friends in discharge planning are essential strategies in navigating the high-risk transition from hospital to the community [13]. Over the 3-month study period, 42% of the 1085 admissions recorded were readmissions and only a small percentage of patients said their discharge arrangements had been explained to them. This could, in part, be attributed to the difficulty of predicting how close to discharge respondents were. This might also explain why so few carers were involved in discharge decisions and consulted about medication, leading many carers to feel dissatisfied with their involvement.
The patients also wanted clearly communicated, individually tailored information. Inadequate information is recognized as a source of dissatisfaction among health service users [14]. Dissatisfaction can also be related to the expectations of the patient and therefore may be addressed by providing appropriate services [15]. Information should be given at the right time, in a form that can be easily understood and based on assessed need [14].
Regular communication and exchange of information throughout the process oftreatment has the potential to increase carers' confidence, prevent them feeling excluded and improve their resilience and coping abilities [14]. Patients in hospital and the community were more confident than carers in managing their mental health and looking after themselves. This difference was not as pronounced in community settings, possibly because carers were less confident when their relative or friend had just been through a period of acute illness. The only area in which many carers felt confident was in recognizing changes in the patient's mental health.
Overall, patients' and carers' perspectives also differed in terms of their priorities for more information. Overall, carers wanted more information than patients and placed a higher priority on knowing about mental health problems than patients. Possibly, this was because patients had personal experience of the illness or because they received more information about it. Our findings illustrate that patients and carers were in agreement about wanting informationon what to do when unwell, and regarding community resources. These have implications for enhancing recovery and preventing relapse, and accords with previous research which found that effective communication about community resources is valued by patients and carers [6]. Information about medication and medication side-effects was also desired, especially by carers; addressing this need is important because it has the potential to enhance medication adherence and reduce admissions [3], [16], [17].
Despite the acknowledged benefits of providing adequate information and increasing carer involvement, barriers to these include carer hopelessness, stigma, guilt and shame, the patient not wanting family involvement, and communication problems between the family and patient [18]. There are other obstacles. One may be the use of the term ‘carer’ which can be viewed by carers as inaccurate or even derogatory by minimizing the significance of the relationship with the person to whom support is provided and implying a level of dependency [19]. There are also language barriers, so provision must be made for people from non-English-speaking backgrounds. Nearly one-third of patients and 42% of their carers in our study were born overseas. Finally, collaboration demands a significant commitment both in time and resources and there may be concerns about mental health services putting the needs of the family before the needs of patients [20], [21]. Greater involvement of carers in the treatment of their family member or friend is important to improve the quality and responsiveness of services as well as to help patients accept their illness and envisage a life beyond their symptoms [22], [23].
The study had several strengths. First, the study described a representative group of patients through consecutive sampling at all sites completed during a period of standard clinical practice. Second, the same two research staff conducted all patient interviews across the health service(hospital and community). Third, by not using staff who provide direct care to the patients, the data collected were more likely to reflect patients' actual perceptions. Fourth, instruments used were reviewed and endorsed bypatients employed by the Area Mental Health Service to keep the focus on what patients deemed important. Finally, carer opinions were canvassed using the same instrument as that used for patients, thus allowing comparison.
The study is not without limitations. In inpatient settings, it was not always possible to predict discharge accurately as some patients were waiting for accommodation or chose to leave against medical advice. As patients and carers may not always have accurately recalled information about the care received, the fidelity of the results may have been affected by recall bias [24]. Similarly, access to carers was dependent upon patient consent and their ability to recall their carer's contact details. The carer response rate was disappointing and may reflect the reliance on a mail reply. In addition, these results are from an Australian(Sydney) inner-city catchment area and the level of carer availability and support may vary in settings with different cultural and socioeconomic characteristics.
Conclusions
This study provides information about the presence of carers and the willingness of patients to have carers involved in their management. Most carers were not provided with mental health information and they were less confident than patients about managing the patient's mental health in the community. Both patients and carers consistently reported wanting more information about what to do when the patient becomes unwell, medication and medication side-effects and community resources. Responding to these information needs has the potential to improve the quality and outcome of mental health services.
Footnotes
Acknowledgements
The project was supported by an Educational Grant from Eli Lilly Australia. We thank participants for completing surveys and the staff who facilitated this process.