
Abstract
To its critics Alcoholics Anonymous (AA) is at best as a placebo, competing with more effective treatments and at worst a dangerous cult [1–4].
For its supporters the fact that AA received the Lasker Award (America's highest scientific prize for medical progress) seems quite justified [5], p.573]. But for many the jury remains out. If I am to suggest that a program based upon dependence on a ‘Higher Power’ is more like penicillin than it is like the Moonies' Unification Church, I must respect the rules of experimental medicine; I must first elucidate the mechanism of action of AA; I must next offer empirical evidence that AA works better than a placebo; and finally, I must seriously discuss the sideeffects of AA.
Mechanisms of action
Because detoxified alcohol-dependent individuals frequently relapse, the medical and psychological professions do not have a good record of curing alcoholism. Over the long term much of what has been carried out to professionally treat alcoholism is at best a placebo [6]. First, cure from addiction does not come through psychodynamic insight. In a prospective study of Harvard men [7], 26 alcoholics received a total of 5000 hours of psychotherapy, an average of 200 hours for each man. Only one man recovered from alcoholism while in psychotherapy.
Nor is life-saving detoxification effective for very long. As Mark Twain allegedly quipped, ‘I found stopping smoking so easy that I've done it twenty times’. It is the same for alcohol dependence. Indeed, long-term studies show that waiting for treatment (a form of placebo therapy) is almost as effective as detoxification [7]. In addition, cognitive behaviour therapy works less well than we would like it to. Linda and Mark Sobell's 1970s study of training alcoholics to return to controlled drinking [8] was famous worldwide for years – until their patients were followed up at the 10-year mark and found to have fared no better than controls [9].
Disulfiram, too, has failed to cure alcoholism [10]. In the last two decades there are two drugs that have made clinicians in the alcoholism field very hopeful–acamprosate and naltrexone. Many papers point to their shortterm success; but although 15 years have passed, the long-term studies that could prove–or disprove–the efficacyofthese treatmentsstill remain undone.
The reasons for the failure of professional therapy to prevent eventual relapse, and thus alter the natural history of alcoholism, are twofold. First, the hold that drug addiction has on human beings does not rest in our cortex. The hold of addiction on our minds lies in what has been called our reptile brain. The hold comes from cellular changes in midbrain nuclei like the nucleus accumbens and the superior tegmentum. Eventually, loss of plasticity of neuronal response in these centres renders abstinence beyond the reach of willpower, beyond the reach of conditioning and beyond the reach of psychoanalytic insight.
The second reason that often life-saving professional treatment fails to prevent relapse in alcoholism is the same reason that life-saving hospitalization fails to prevent relapse in diabetes. Change in clinical course in both alcoholism and diabetes can only be achieved by relapse prevention and to quote Lady Macbeth's physician ‘Therein the patient must minister to herself’.
There are four factors that are commonly present in relapse prevention for most addictions, be they smoking, compulsive eating, opiate addiction, gambling or alcoholism [11], [12]. The four factors that prevent relapse are external supervision, ritual dependency on a competing behaviour, new love relationships and deepened spirituality. Usually, two or more factors must be present for relapse prevention to occur. The reason that these four factors are effective is probably because, unlike most professional treatments, they do not work to create temporary abstinence or reduced drinking. They work to effect relapse prevention; and, thus, like regularly selfadministered insulin in diabetics, they must be used for a very long time. Elsewhere [7] I have stressed the congruence of these four factors with Marlatt's [13] use of cognitive behavioural techniques to enhance relapse prevention.
External supervision appears necessary because in prospective studies conscious motivation to stop drinking at admission is not associated with outcome [7]. Alcoholics Anonymous, like most personal trainers, provides motivation from without and suggests that clients return again and again. In AA, members are told to find a sponsor to telephone and to visit often. They are encouraged to ‘work the steps’ and to engage in service. Each of these activities provides a daily involuntary reminder that alcohol is an enemy, not a friend. These activities provide external supervision, or in the language of AA ‘keep the memory green’. But AA also understands that compulsory supervision works best if it is from choice. We willingly suffer under the strict rules of our athletic coach, but we evade prohibitions of which we do not approve.
Second, it is important to find a substitute dependency or a competing behaviour for the addiction. You cannot easily give up a habit without having something else to do. For example, disulfiram, often prescribed because it makes the ingestion of alcohol sickening, fails as a cure because although it takes alcohol away, disulfiram offers no replacement. Eventually the patient stops the medicine. However, competing dependencies–for example, methadone maintenance in heroin abuse–facilitate relapse prevention because they offer a carrot as well as a stick. In contrast, imprisonment per se did not reduce relapse to heroin abuse [12]. For punishment alone does not alter deeply ingrained habits.
Alcoholics Anonymous understands what all behaviourists know and what many doctors and parents forget: bad habits need substitutes. Alcoholics Anonymous provides not only supervision, but also a gratifying schedule of social and service activities in the presence of supportive and now-healed alcoholics, especially at times of high risk, like holidays.
Third, new love relationships are important to recovery. It seems important for ex-addicts to bond with people whom they have not hurt in the past and to whom they are not deeply emotionally in debt. Indeed, it helps for them to bond with people whom they can actively help [14]. Alcoholics Anonymous meetings are filled with sober former pub-crawlers with whom to befriend but to whom one does not owe money. Similarly, an AA sponsor, analogous to a new spouse, can promote relapse prevention better than some long-suffering family member whom they have tortured for years.
As a speculative aside, since it is doubtful that our prehistoric ancestors shot dope, the brain circuitry underlying addiction may have evolved originally to facilitate human attachment, social cohesion and spiritual community [15]. Brain opiates are released during the attachment behaviours of social grooming and during the social bonding of mother rat–pup reunions [16], [17].
The fourth common feature in recovery from addiction, the discovery or rediscovery of spirituality, is the most controversial. Inspirational, altruistic group membership and belief in a power greater than ‘me’ seems important to recovery from addiction. In The Varieties of Religious Experience, William James [18] first articulated the close relationship between religious conversion and recovery from intractable alcoholism. As Carl Jung [19] directed the cofounder of AA, Bill Wilson: ‘Spiritus contra spiritu’. The universal model that Jerome Frank [20] describes in his book, Persuasion and Healing, for effective psychotherapyclosely resembles spiritual healing. In Frank's model the sanctioned healer should have that status (e.g. several years of abstinence), be equipped with an unambiguous conceptual model of the problem (e.g. AA's Big Book) and should create in the patient an expectancy of cure. Alcoholics Anonymous meetings, after all, are the only places in the world that are densely populated by alcoholics with stable sobriety. Finally, Frank, reminds us that in group therapy healing came from caring for each other, not oneself. The Twelfth Step of AA carries the same message.
But there are other reasons that in the addictions spirituality is valuable for relapse prevention. First, there is a critical difference between a healing connection in spiritual communities and with a hierarchical religious leader or psychotherapist. In medicine and authoritarian religion, the wise powerful doctor or priest asks the sick, sinful or unenlightened patients to wallow in dependency and relive their past angers and losses. In contrast, in AA and other democratic spiritual communities–the playing field is level. One of the early Akron drunks, to whom Dr. Bob and Bill Wilson brought their message of alcoholic recovery, expressed this reciprocity very well: ‘All the other people that had talked to me wanted to help me, and my pride prevented me from listening to them… But I felt as if I would be a real stinker if I didn't listen to a couple of fellows for a short time, if it would cure them’ [5], p.185].
Second, spirituality affects our behaviour not through sweet reason but by its appeal to emotion. Four major longitudinal studies [21–24] have provided evidence that, after controlling for variables like prohibition of alcohol consumption, religious involvement when young reduces alcohol and cigarette consumption when adult. Religious prohibition of alcohol use (e.g. Mormons in Utah and Islam in Saudi Arabia) has been remarkably successful. In contrast, governmental prohibition against alcohol consumption has been less effective (e.g. prohibition in the US in the 1920s and in the Soviet Union in the 1990s).
Third, alcoholics, unlike most sinners, are not merely annoying. Alcoholics have often inflicted enormous pain and injury on others. Thus, when sober, the alcoholic may experience almost insurmountable guilt from the torture that they have inflicted on others. Although a poor tranquilizer and a worthless antidepressant, alcohol is perhaps the most powerful solvent for a guilty conscience that modern pharmacology has yet devised. Therefore, absolution from guilt mediated by a ‘power greater than ourselves’ provides an alternative to alcohol and becomes an important part of the alcoholic's healing process.
Finally, spirituality, like human attachment–both mediated by limbic circuitry and the temporal lobe–may be a worthysubstitute for drugs. In other words, spirituality and religion provide an alternative to the high produced by drugs. Religion, Marx's ‘opiate of the people’ and Jung's spiritus, may be an indirect way that we have of stimulating our limbic brain and its endorphins.
Efficacy of Alcoholics Anonymous
Unfortunately, empirical information on the efficacy of AA is hard to come by. First, as an organization AA is uninterested in research. Second, because of ideological differences and unconscious rivalry, medical researchers sometimes have difficulties in assessing AA without bias. Finally, in the course of their long and chronic disorder, alcoholics encounter many different kinds of interventions, often simultaneously. Therefore, unlike the case with most formal drug trials, there is no way that one can do a truly controlled study. Until recently, it was unclear whether AA attendance caused abstinence or whether AA attendance was only a manifestation of abstinence and greater compliance with professional therapy.
The overall evidence, however, that AA works as an effective ‘cure’ is quite convincing. First, multiple studies that collectively involved a thousand or more individuals, suggest that good clinical outcomes are significantly correlated with frequency of AA attendance, with having a sponsor, with engaging in a Twelve-Step work and with chairing meetings [25].
Second, for 35 years I have been Director of the Study of Adult Development. This community study has followed two cohorts of men, 268 college men and 456 socially disadvantaged inner-city men, for 60 years [7], [26]. As 26]. Nor did an abundance of risk factors for alcoholism, like alcoholic heredity, hyperactivity in youth and sociopathic behaviour, predict chronicity. Nevertheless, it was noteworthy that the men in the good outcome groups reported attending about 20 times as many AA meetings as the men in the poor outcome groups (Table 1).
Characteristics of alcoholics at age 70 who either met criteria for stable abstinence or lifelong chronicity
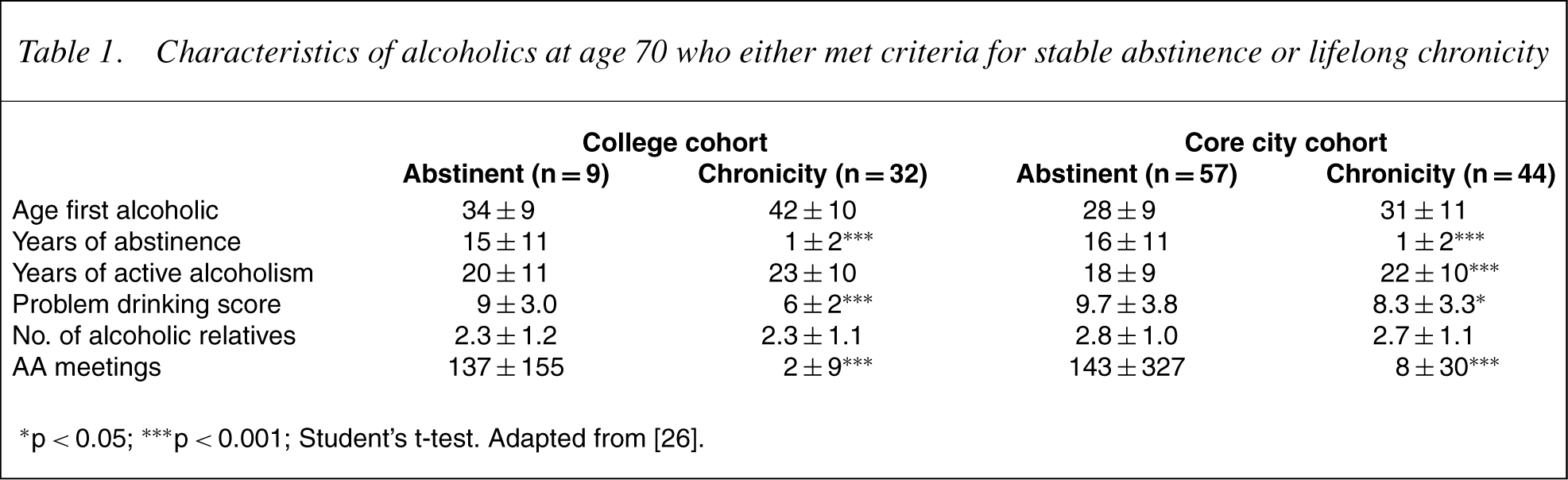
∗p<0.05; ∗∗∗p<0.001; Student's t-test. Adapted from [26].
Third, a multimillion-dollar controlled study, Project Match [27], [28], compared the effects of three treatments upon almost 2000 alcoholic patients and arrived at several interesting conclusions. Project Match revealed that during the first year AA alone was as effective as the two most effective professional alternatives: cognitive behavioural and motivational enhancement therapies. Indeed, AA in some respects was superior to cognitive behavioural therapy. Second, the Match followup also showed that regardless of the original treatment arm (cognitive behavioural, motivational, or Twelve Steps) the more AA meetings attended the better the outcome.
Perhaps the most convincing controlled study of the efficacy of AA came from an 8-year follow-up by a behavioural psychologist, William Miller [29]. The purpose of Miller's therapy program had been to return alcoholics to safe drinking practices, not to produce abstinence and certainly not to involve them with AA. In addition, the patients in his study had been self-selected for motivation to return to controlled drinking, not to achieve abstinence. Nevertheless, after 8 years most of Miller's good long-term outcomes were abstinent and not controlled drinkers. In contrast to a long-term abstinence rate of 20% among the 81 clients who went to less than 100 meetings, 53% of the 13 clients who had subsequently made more than 100 visits to AA were eventually stably abstinent–a statistically significant difference.
Finally, at Stanford, a collaborative 8-year prospective study [30], [31] underscored the value of AA in contrast to professional treatment. In 8 years, the two outcome goals of less drinking and more abstinence were only weakly related to days of professional inpatient treatment, but robustly related to AA attendance. In short, the effect of AA did not just rest on compliance with treatment.
Certainly, AA is not a magic bullet for every alcoholic. In my own follow-up studies, there were a few men who attended AA for scores of meetings without improvement. Nor is it that professional treatment is ineffective. Session for session I suspect that alcohol professionals and AA meetings are equally effective. Rather, the efficacy of AA is like the use of insulin and digitalis; AA does not stop once the patient leaves the clinic.
Side-effects
The third ‘scientific’ question I must address is: Even if AA does cure alcoholism, is it safe? What are the sideeffects of AA? Certainly, AA has its detractors. Designed to affect the reptile brain, the rhetoric and the emotional language of the spirituality of AA leads journalists and social scientists to understandably fear that AA is a religion or cult [4], [32]. Cults can lead to demagoguery and exploitation. Religion can lead to exclusion, bigotry and even war. Individual alcoholics attending incompatible AA groups or allying themselves with unfortunate sponsors sometimes tell horror stories about the fellowship. Manyof the beliefs that AA members express about alcoholism, are like the tenets of any faith tradition not based on science. For example, if men are followed for 30 or 40 years it is found that alcoholism is not a ‘progressive disease’.
What makes AAsafe is that as an organization it is not a religion; and AA has deliberately incorporated principles to avoid cultic abuse. Religions like nationalism draw circles that draw others out. Alcoholics Anonymous and internationalism draw circles that draw others in. The spiritual foundation of AA evolved from the intellectual experience of three men deeply mistrustful of all organized religions. These three men, William James with his Varieties of Religious Experience, Carl Jung with his prescription ‘Spiritus contra spiritum’ and Dr. Robert Smith, cofounder of AA, were each devout students of what was truly healing among all religions. Such spirituality, I believe, usually leads only to love, tolerance, humility and awe toward the universe. These are qualities that deepen human relationships and not distort them as do cults.
Indeed, AA is not about religion at all. The preface to Alcoholics Anonymous flatly states: ‘Alcoholics Anonymous is not a religious organization’. The only requirement for membership is an honest desire to stop drinking. Alcoholics Anonymous passes the test of universality so necessary to distinguish safe spirituality from potentially divisive religion, namely that religious conviction does not prevent AA membership. Over the last 20 years AA membership has increased 10-fold in Hindu India, in Buddhist Japan and in Catholic Spain. Membership has also risen exponentially in atheistic Russia. Per capita there are three times as many AA groups in Costa Rica and El Salvador as in the US [33]. Today, one-third of AA members are women and one-quarter are less than 31 years old. Research has failed to identify clear personality differences between alcoholics who do and do not attend AA [7]. Neither social class nor education, neither extroversion nor mental health distinguishes those who use AA from those who do not. The only consistent variable that distinguishes AA members from alcoholics who only attend professional treatment centres is that AA members tend to have had more symptoms of alcoholism.
It is worth noting, however, some of the specific ways that AA has avoided becoming a cult. First, from the beginning, AA has made no clear distinction between God and ‘the fellowship of AA’. There has always been a tacit, if not explicit, permission to replace the concept of God, with the ‘home group’.
Second, the spirituality of AA does not compete with medicine. Alcoholics Anonymous published work is very clear that it is ‘wrong to deprive any alcoholic of medication which can alleviate or control other disabling physical and/or emotional problems’ and that ‘no AA member plays doctor’ [34], p.11].
Third, some worry that AA, like cults, exerts mind control and removes freedom of action. New York psychiatrist, Mark Galanter [35], has defined cults as charismatic groups ‘characterized by a high level of social cohesion, an intensely held belief system and a profound influence on its members’ behavior' (p.543). As Galanter noted, this is quite true of AA. But there is an important caveat. The purpose of AA's ‘Twelve Steps’, like the rigidity of post-coronary exercise programs, is not, as is the case of cults, to take away autonomy, but only to provide a disciplined set of ‘suggestions’ so that you won't relapse and die.
Finally, a major difference between all cults and AA is their governing structure. Cults are characterized by charismatic leaders with infallible powers and an autocratic governing structure. In AA ‘Our leaders are trusted servants; they do not govern’. Most of the AA service positions are unpaid and all jobs are frequently rotated so that the consolidation of power cannot occur. The organizational chart of AA that has evolved is a pyramid on its head. Positions of responsibility within AA are defined as ‘service without authority’ and the legislative processes of AA are democratic to a fault.
In AA, but not in cults or religion, minority opinions are respected. Just as the American Constitution gave as many senators to Delaware and Rhode Island as to the more populated states of New York and Virginia; so AA in its organizational deliberations pays particular attention to minority opinions.
Acriticism of both AA and cults is that they encourage dependence. And so it is important to distinguish the dependence engendered by AA from the dependence engendered by cults. Dependencies can weaken or strengthen us. We are weakened by dependence on cigarettes, slot machines and junk food. We are strengthened by dependence on exercise, vitamins and our families.
Finally, AA's Twelve Traditions reflect founder Bill Wilson's 20-year effort to embrace spirituality and yet protect AA from becoming a cult. Alcoholics Anonymous, like the early Christian Church, successfully strives to stay poor. Unlike cults, universities and religious orders, AA owns no property. Alcoholics Anonymous traditions also include personal anonymity in public settings–a good antidote to cults of personality.
Alcoholism, if not interrupted, is a cunning, baffling and persistent foe that kills 100 000 Americans a year [36]–far more people than are killed by breast cancer. However, a review of the world literature suggests that professional medicine can do little to halt alcoholism long term. In contrast, available research suggests that AA is the most effective means of long-term relapse prevention in the physician's armamentarium.