
Abstract
A lot of research in psychiatry is directed towards the development of treatment methods. Unfortunately, many potential users of treatments do not receive them because they do not engage in the treatment process. Some reports suggest that the rate of termination of contacts is higher at the time of the initial contact. The extent of this problem can be inferred from the fact that a proportion of patients ranging from 9% to 63% have only one contact with psychiatric services [1–9]. This wide range in the percentage of patients seen once only in a psychiatric setting could be due to the different criteria used to define once-only contact. Variations are found with respect to: (i) the follow up period, which ranges from 3 months to 3 years in the published studies; (ii) the sources of data (for example psychiatric case register, interviews, administrative data); (iii) the use of either prevalence or incidence rates; and (iv) the different settings and services organizations in which the studies have been carried out. Intuitively, it is likely that onceonly contact patients are quite different from patients who engage in treatment. Only a few of the studies reported above, however, have described the characteristics of such patients. In a study examining attrition among out-patients referred to a clinical psychologist, it was found that patients who attend only once were more likely to be unemployed. They were also more likely to belong to a lower social class and were more likely to have been referred by physicians with whom psychologists had poorer contact [3]. In a recent 8-year cohort study, we found that patients who had had once-only contact with the South Verona out-patient department were older males who had a diagnosis other than schizophrenia, and who had been referred to the department by consultation/liaison or emergency room staff. Compared with patients with more than one contact, they were also of a lower socio-economic status [9]. Unemployment, marital disruption, and living alone have been shown to be more prevalent among people who seek help for emotional problems as compared to the distribution of these characteristics in the general population [10–12]. It may be that some once-only contact patients seek help from mental health services in an effort to compensate for their social isolation and the absence of viable social support, rather than for a psychiatric disorder.
We are not aware of any reported research that has examined the profile of this type of service user or the determinants of once-only contact at different sites. South Verona and Western Australia are both served by psychiatric case registers (PCR) that have been used to monitor population contact with local psychiatric services [13], [14]. This allows us to describe and compare the profile of persons who made once-only contact at both sites.
The aims of the present study are: (i) to describe sociodemographic and clinical characteristics of once-only contact patients in South Verona and in Western Australia; and (ii) to identify the characteristics associated with a high probability of being a once-only contact patients in South Verona and in Western Australia. Conducting the study across two sites may improve the generalisability of the results compared with studies conducted at a single site. Moreover, differences between sites with respect to the pattern of service utilization may reflect differences between services in the provision of care and in the management of patients.
The study will test two hypotheses:
1 once-only contact patients will have a less severe psychiatric diagnosis compared with patients with more than one contact with services;
2 once-only contact patients will have a lower socioeconomic status.
Method
Characteristics of the study areas
Data were drawn from two psychiatric case registers, one in South Verona (Italy) and the other in Western Australia. These areas are different in several respects. South-Verona is predominantly an urban area on the southern outskirts of Verona, a city of about 260 000 inhabitants, located in northern Italy, halfway between Milan and Venice and on the route from Italy to central Europe. The total population of South Verona is about 75 000 (population density 988/km 2).
Western Australia occupies the western third of the Australian continent. It is larger than Western Europe, but has a population of about 1.7 million inhabitants only (population density: 0.75/km 2). Moreover, most of this area is sparsely populated, with 73 per cent of its inhabitants residing in the capital city, Perth.
Over the study period, both areas had a stable population but the distribution of economic activities differed. In South Verona services and industry comprised 97.4% of the economy while, in Western Australia, the figure was 75.0% (the remaining 25.0% was agriculture, forestry, fishing and mining).
The age structure of the population in both areas was much the same. In Western Australia, 29% of the population was below the age of 19 (South Verona, 28%), and 11% was 65 years of age or older (South Verona, 11%).
In Western Australia, a slightly higher percentage was married (55% in Western Australia compared to 52% in South Verona), and more people were divorced (4.5% in Western Australia compared to 1.5% in South Verona).
The percentage of employed people in the adult population (≥ 15 years) was 44% in South Verona and 62% in Western Australia.
Mental health services and psychiatric case registers
In South Verona, in accordance with the Italian Mental Health Act (1978), care is organized according to a district model which serves a geographically well defined area and is supported by the National Heath Service (NHS). It is extremely rare that residents in this area receive care from services located in another, even adjacent area. The main agency providing psychiatric care for the adult population is the South-Verona Community-based Mental Health Service (CMHS), which is run by the Section of Psychiatry and Clinical Psychology, Department of Medicine and Public Health of the University of Verona.
The CMHS supplies a wide range of well-integrated hospital and community services including an inpatient ward at the University General Hospital, a Community Mental Health Centre providing day care and rehabilitation, out-patient departments, scheduled domiciliary visits, a liaison service for psychiatric and psychological consultations for other departments of the General Hospital, a 24-hour accident and emergency department, a 24-hour staffed hostel and sheltered apartments. With the exception of hospital nurses, all staff work both inside and outside of the hospital. This ensures continuity of care through the different phases of treatment and across the various components of service provision [15], [16]. Since 31 December, 1978, the South Verona Psychiatric Case Register (PCR) has collected information from all these agencies. The main features of this PCR have been described previously [9], [13].
The mental health system in Western Australia is typical of Australia. Public health services are administered by State and local governments. General practitioners and medical specialists are the main providers of ambulatory medical services. Mental health services consist of psychiatric hospitals or wards within general hospitals for voluntary and involuntary patients, out-patient departments, community psychiatric clinics and psycho-geriatric extended-care units. Home and community care services, such as domiciliary nursing and home help services, are provided by a network of non-government organizations jointly funded by State and Commonwealth governments. Residential care in hostels and nursing homes is provided mainly in the private sector and funded by Commonwealth [14].
The Mental Health Information System (MHIS) is a register that has been recording all contacts with in-patient mental health services (private and public) in Western Australia since 1966, and all contacts with State psychiatric out-patients clinics (which also provide community-based mental health services) since 1972; it also maintains records of people who are resident in psychiatric hostels. Other features of this PCR have been described elsewhere [14], [17].
Patients
The study design is an epidemiologically based comparison of mental health service use. We defined the index contact as the first ever contact, or any new contact after at least 365 days without a contact, with a South Verona or Western Australian out-patient units in the period between 1 January 1992 and 31 December 1999.
These out-patient or ambulatory contacts cover face-to-face contacts with a mental health professional, operating in an agency providing psychiatric care and do not include home visits or emergency assessment. Both in South Verona and in Western Australia, the first visits are routinely done by psychiatrist.
It is well known that the criteria chosen for case definition have a marked effect on the results of an epidemiological study. We chose to focus attention on out-patient contacts in order to produce directly comparable data sets between the two sites. The out-patient setting has less variability than other elements of mental health service provision and is the most common model used for monitoring patients in the community.
The most useful definition of the end of an episode of care in the field of mental health care, and one which has been tested using case register data, is ‘90 days or more without any further contact after the index contact’ [6]. We have used this length of time for defining a once-only contact. Using the psychiatric case registers (PCR) of the two sites, each patients was followed-up for 3 months after his/her index contact, in order to identify those who did not have any successive contacts with any psychiatric service within 3 months of the initial contact. These were the once-only contact patients. Since the sample unit we refer to in this study is the contact, not the individual, some patients may appear more than once as a once-only contact patient during the 8-year follow-up period (e.g. a patient could have had a first ever contact in February 1993, then no further contact until February 1994; in this case, the patient would have entered the study two times).
Measures used
Particular care was taken to select and prepare variables for comparison. Variables on both registers that described contact characteristics were identified, and the variables were recoded to produce directly comparable data sets.
For each index contact, we collected socio-demographic information (gender, age, marital status, educational level, employment status, employment status) and diagnosis according to the ICD-10 classification system. Diagnoses were collapsed into six groups: (i) schizophrenia and related disorders; (ii) affective disorders; (iii) anxiety-related and somatoform disorders; (iv) personality disorders; (v) other mental disorders including alcohol and drug dependence and abuse, transient organic psychosis, adjustment reaction, acute reaction to stress, specific-non-psychotic mental disorders following brain damage, mental retardation, and dementia; and (vi) diagnoses other than mental disorders (codes that were not F-codes).
Statistical analysis
All statistical analyses were conducted separately on both data sets (the South Verona and Western Australian data sets), using the characteristic of the contact episode (that is whether the contact was a onceonly contact or not a once-only contact) as the dependent variable. Univariate association between the dependent variable and covariates was measured using Pearson's chi-square and the unadjusted (crude) odds ratio. The probability of being a once-only contact patient was assessed by a logistic regression model. Odds ratios were used as rough approximations of risk ratios (odds ratios are good estimates of risk ratios for rare events) [18]. Univariate and multivariate analyses were undertaken using Stata 7.0.
There were some data missing on the registers. Three fields on the Western Australian register in particular – level of education, occupation and employment status – were affected by missing data. There was no systematic pattern in the distribution of missing values by either once-only contact status or diagnosis.
Because of missing data on the register, we used multiple imputation by chained equation (MICE) [19], [20] which is available for use with the statistical package S-Plus to impute missing data. This technique allowed us to model the missing data, assuming both missing at random and missing completely at random. The number of imputed datasets used was 20 and the number of interactions in the MICE algorithm was set at 25. After the imputation stage, a logistic model was estimated for every dataset. In these models the dependent variable was patient status (1 = once-only contact, 0 = more than one contact) and the independent variables were the socio-demographic and clinical characteristics of patients. Finally, the results were matched together using the procedure proposed by Rubin [19], and implemented by the Stata implogit command [21]. Variable selection was performed by stepwise (backward) selection.
Results
From 1 January 1992 to 31 December 1999, a total of 2446 new episodes of care met the inclusion criteria of the study in South Verona. Of those, 734 (30%) were once-only contacts with services according to our definition. The total number of patients was 2144; therefore, about 12.5% of these patients had entered the study more than once. In the same period, a total of 36475 new episodes of care met the inclusion criteria of the study in Western Australia. Of those, 8863 (24%) were once-only contacts with services according to our definition. The total number of patients was 34566; therefore, about 5% of these patients had entered the study more than once.
The rate of once-only contact was higher in South Verona. When these data are considered in relation to the population served, onceonly contact patients were also more predominant in South Verona (Table 1). In South Verona, the proportion of once-only contact patients increased over time whereas, in Western Australia, the proportion of once-only contact patients remained relatively stable.
Number, percentage and rate of once-only contact (OOC) episodes with the South Verona and Western Australia out-patients department during the specified years
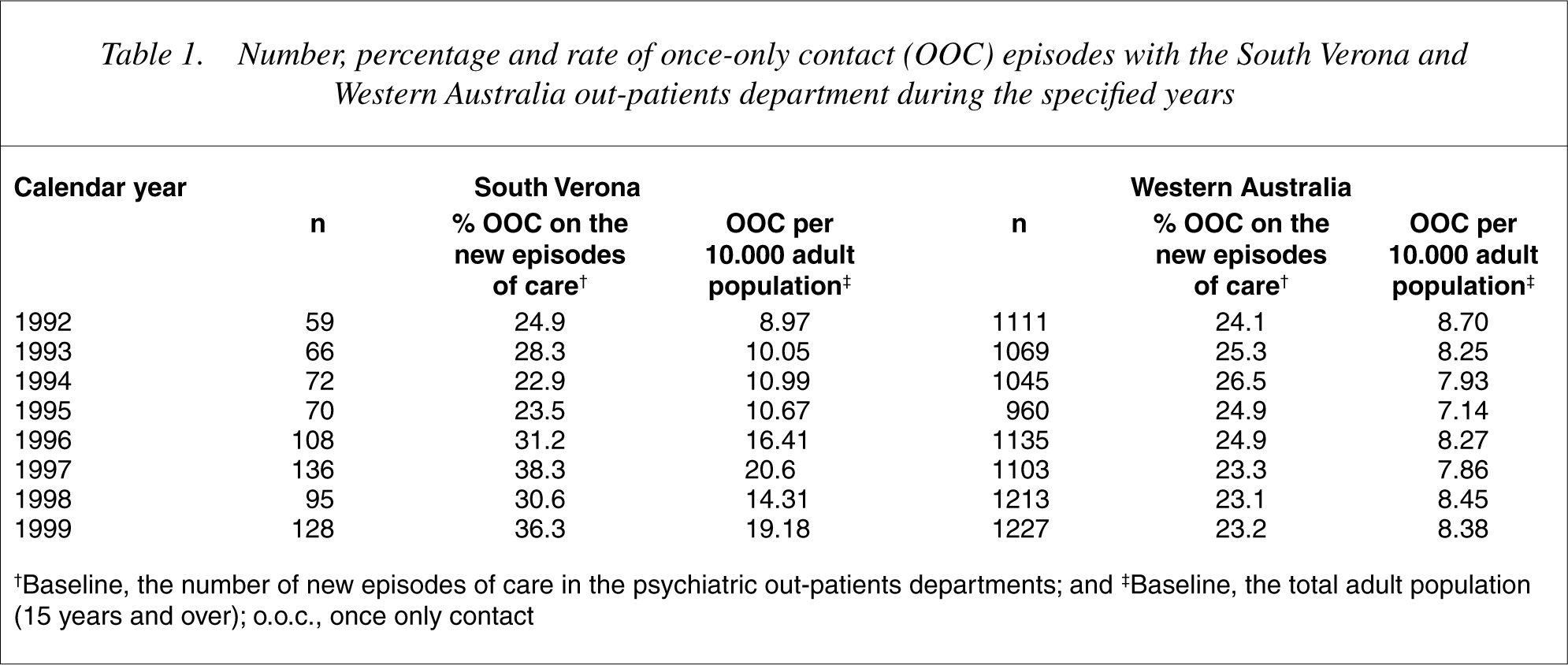
†Baseline, the number of new episodes of care in the psychiatric out-patients departments; and ‡Baseline, the total adult population (15 years and over); o.o.c., once only contact
The structure of the sample is shown in Table 2.
Socio-demographic and clinical characteristic for once-only contact (OOC) and more than one contact in South Verona and Western Australia
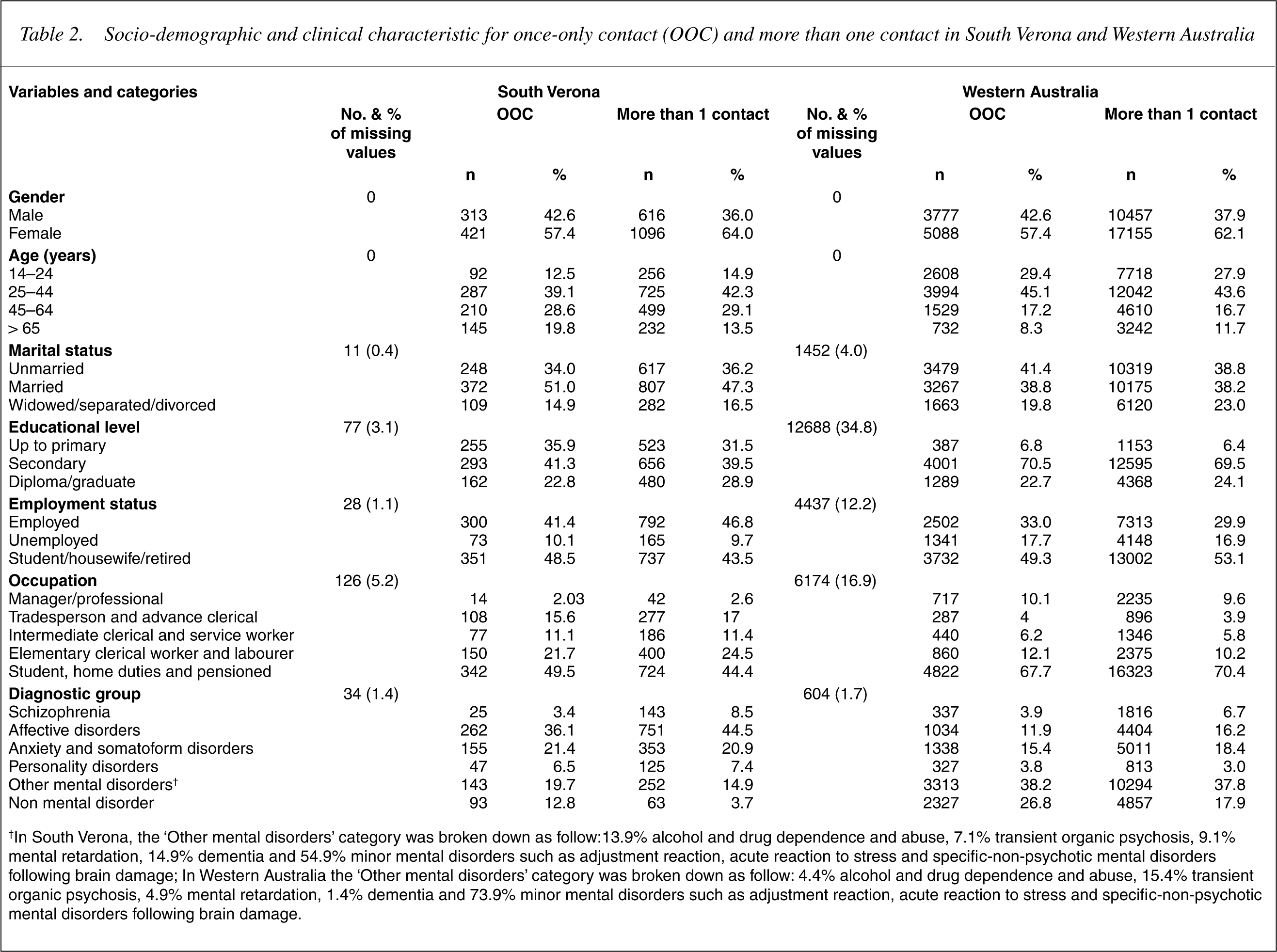
†In South Verona, the ‘Other mental disorders’ category was broken down as follow:13.9% alcohol and drug dependence and abuse, 7.1% transient organic psychosis, 9.1% mental retardation, 14.9% dementia and 54.9% minor mental disorders such as adjustment reaction, acute reaction to stress and specific-non-psychotic mental disorders following brain damage; In Western Australia the ‘Other mental disorders’ category was broken down as follow: 4.4% alcohol and drug dependence and abuse, 15.4% transient organic psychosis, 4.9% mental retardation, 1.4% dementia and 73.9% minor mental disorders such as adjustment reaction, acute reaction to stress and specific-non-psychotic mental disorders following brain damage.
The complete multiple logistic model estimated for the odds of being a once only contact is shown in Table 3. For the South Verona sample, stepwise selection suggested that gender, age, diagnostic group and educational level be entered into the model.
Logistic Regression Model for once-only contact in South Verona and in Western Australia
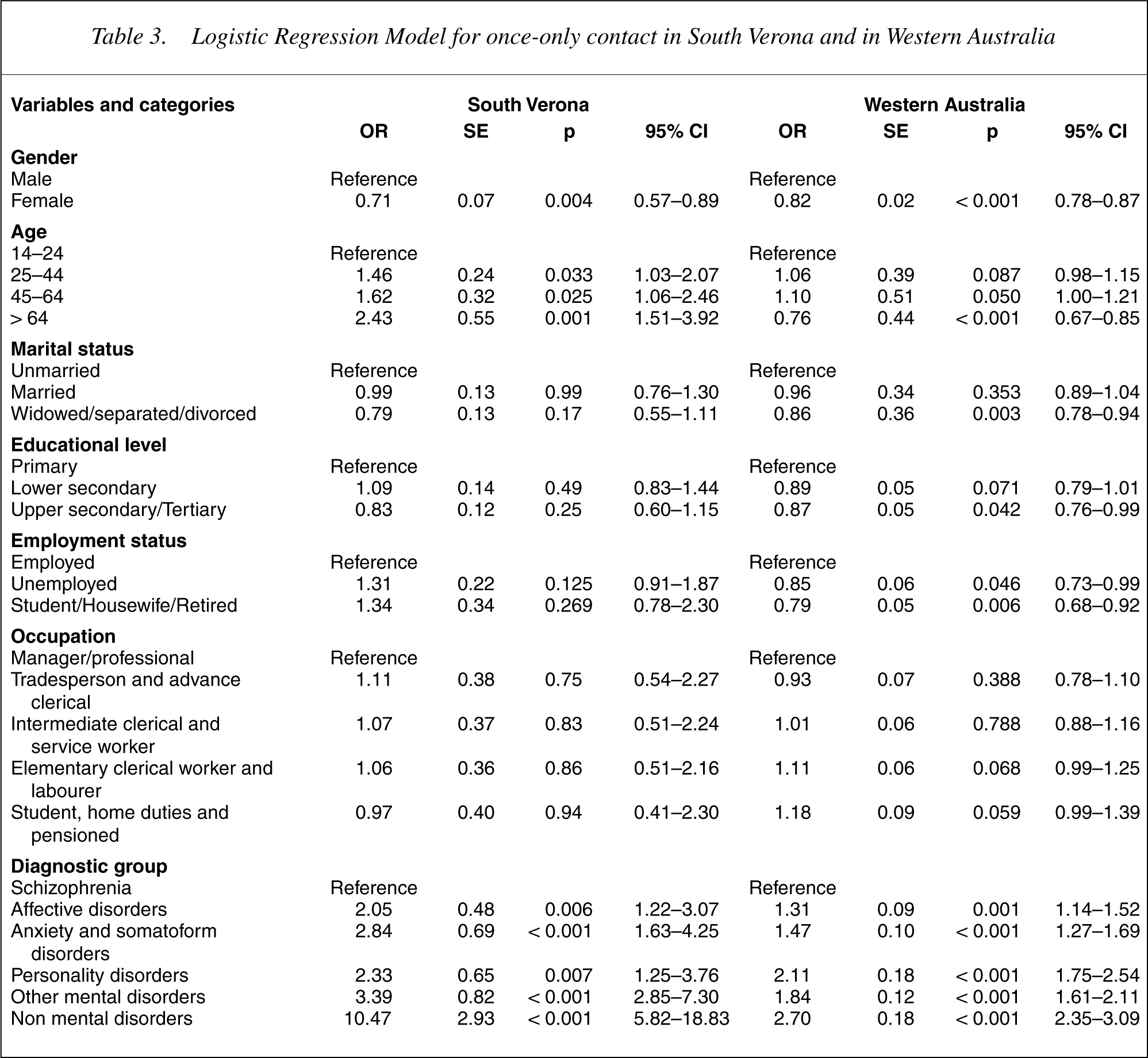
Gender, age and diagnosis were significant determinants of onceonly contact with services. In particular, older age and being male increased the probability of once-only contact with services. Being seen once-only by services was not associated with other sociodemographic characteristics. In terms of clinical status, our results showed that patients in all other diagnostic groups were more ‘at risk’ of a once-only contact with services compared to patients with schizophrenia. In particular, being one of a group of patient seen by services who did not meet the ICD-10 criteria of a mental disorder was the most important predictor of this pattern of service utilization.
For the Western Australia sample, the same selection procedures were used as described for the South Verona sample and the same variables were retained in the multivariate analysis (see Table 3). Gender, age, marital status, employment status, educational level and diagnosis were determinants of having a once-only contact with services. Being older and female decreased the probability of onceonly contact with services in this sample. Being widowed, separated or divorced, all decreased the odds of once-only contact, as did having a higher level of school education. Employment status was also associated with once-only contact with services: being employed increased the odds. In terms of clinical status, our results showed that patients in all other diagnostic groups were more ‘at risk’ of having a once-only contact with services compared to patients with schizophrenia. As in the South Verona sample, although not as markedly, being a patient who did not meet the ICD-10 criteria of a mental disorder was the most important predictor of once-only contact with services.
Since the results of this study suggest that clinical characteristics alone were significant determinants of this pattern of contact with services consistently at both sites, we compared the socio-demographic characteristics of each diagnostic group of patients in order to explore possible differences between these groups. This analysis showed that, in South Verona only, patients in the ‘over 64 years age’ group were significantly more at risk of being once-only contact patients in all diagnostic categories. In Western Australian only, being unemployed increased the ‘risk’ of once-only contact for persons with a diagnosis of personality disorder.
Discussion
This study, using case register data, identified patient characteristics associated with being a once-only contact patient in South Verona and in Western Australia. As the study was conducted in catchment areas covered by case registers, it was possible to operationalize inclusion criteria for the once-only contact group, and to include PCR data collected in routine clinical practice for the selected patients. The results should be interpreted with the following limitations in mind. First, register data monitor the number of contacts with specialist services but do not provide reasons for the failure to follow-up an initial contact. As such, they do not allow us to distinguish between patients who had single contact with services because of a decision made in conjunction with the treating clinician that they did not required further psychiatric care and those who dropped out of treatment for other reasons. A second limitation of this study is that we cannot exclude completely the possibility that the PCRs may have missed some contacts. As a result some patients could be wrongly identified as a once-only contact. Finally, our study did not include follow-up details of patients who came under the treatment of a private psychiatrist or private psychologist, or those who sought care from general practitioners. These limitations are common to studies based on case registers, as case registers do not usually include data from these sources.
Rates of once-only contact
The goals of community psychiatry are to identify people suffering from psychiatric problems and to provide care for as long as it is required. Therefore, the rates of patients who do not return after the first visit could be considered as key outcome indicators in this setting (e.g. as a proxy for poor engagement in the treatment process). In the present study we found that a large percentage of new episodes of care resulted in an extremely brief encounter with services both in South Verona and Western Australia. Over the study period, 30% (734) of new episodes of care in South Verona and 24% (8863) in Western Australia, were for patients who did not have any further contacts during the 3 months following this first contact with services. One could question whether the definition of those patients, as seen only once within 3 months, is the most useful one. However, a sensitivity analysis was performed on the South Verona data using longer periods before re-contact (4, 5, 6, 12, 24 months) and showed the validity of this definition, as the results did not changed increasing the length of time without contacts.
In South Verona, the proportion of once-only contacts was higher than in Western Australia and, when considered in relation to the respective catchment populations served, the picture is even more accentuated, since onceonly contact patients were clearly predominant in South Verona (see the rate per 10 000 adult population in 22]. Again, data from the PCR show that, in the period covered by the present study, 10% of residents of South Verona sought mental health care from services other than South-Verona CMHS. This could explain to some extent the 6% differences between the South Verona and Western Australia rates of once-only contact episodes.
Furthermore, the proportion of once-only contact patients seems to have increased over time in South Verona, while in Western Australia it has remained stable. In the last 25 years, in many developed countries there has been a gradual shift from hospital-centred to community-based mental health care. Such a trend has occurred at different speeds in different countries. The situation in Italy is unique with rapid changes toward a community-based system of psychiatric care following legislation for deinstitutionalization in 1978 [23], which replaced the traditional hospital-based system [24] and increased accessibility to community-based services. The trend in South Verona, with increasing rates of once-only contact patients, may therefore be the result of a greater uptake (compared with Western Australia) in the use of out-patient and community-based mental health services.
In Western Australia, difficulty accessing psychiatric services in rural communities due to distance [25] could potentially introduce a different form of bias. To assess this problem, we repeated the analyses using the Western Australia urban subsample; the results confirmed those found for the whole sample. Dear [26] has noted that there are a number of dimensions to accessibility to mental health services, and that distance from the service is only one of these. Other dimensions include the notion of a ‘catchment’, ‘social distance’ and ‘relative location’. It is possible that the inclusion of these variables in the analyses may have resulted in a positive relationship with once-only contact with psychiatric services.
Determinant of once-only contact in the two sites
The results of the multiple logistic regression analysis of patient characteristics on the dependent variable indicated that only clinical characteristics were significant determinants of a once-only contact pattern of service utilization consistently at both sites. In fact, apart from being male, which was associated with an increased odds of using services once only, no other socio-demographic variables predicted this pattern of service utilization in the same way, in both South Verona and Western Australia. In South Verona, being over 64 years of age increased the odds of having a once-only contact with services. Moreover, comparing the socio-demographic characteristics of patients in each diagnostic group, we found that, in South Verona, those in the ‘over 64 years age’ group were significantly more at risk of being onceonly contact patients for all diagnostic categories. A possible explanation is that there is a tendency in Italy to care for elderly patients in geriatric institutions outside the psychiatric system [23]. In Western Australia, we found the opposite: those aged 64 or more were less ‘at risk’ of a once-only contact. Although we found that, in Western Australia, being unemployed increased the ‘risk’ of once-only contact for the group with a diagnosis of personality disorder, whereas in South Verona there was an opposite effect, these findings are likely to be based on a skewed sample and must be interpreted with caution. Not only were the rates of personality disorder low at both sites but, given that these diagnoses are generally made over time and not on first contact, it is likely that personality disorder has been under-diagnosed in the once-only contact groups. In Western Australia, social factors appeared to play a more important role in determining who would be seen only once by services. Both being employed and having a lower level of education were associated to this type of service utilization. We did not find any association between once-only contact and these variables in South Verona. However, the present study supports the findings that there is a strong relationship between severe psychopathology and consumption of services as reported in other studies [1], [2]. At both sites, the multivariate analyses showed that diagnosis was the most significant determinant of once-only contact with the services: the less severe the patient's diagnosis, the more likely the patient was to have a once-only contact with services. In South Verona, in particular, the odds that patients without a mental disorder as defined by the ICD would have a once-only contact was approximately 10 times greater than the odds for a patient with schizophrenia. These findings could be explained in part by the setting in which these contacts took place. The out-patient department is the first and simplest entry point into the health care system; patients can refer themselves to this facility without a previous consultation with a general practitioner. For this reason, it is possible that a large number of patients are assessed as having ‘no psychiatric problems’ at their first contact and correctly redirected to other services. It was possible to examine this in greater detail using the Western Australian sample, as ICD-10 codes were available for those Western Australia patients who were recorded has having no psychiatric disorder. For these patients, the more frequently recorded ICD-10 codes at the time of contact were those related to psychosocial circumstances including marital and parental issues, symptoms and conditions for which no specific diagnosis can be made, as well as codes for general psychiatric examinations requested by authorities or for administrative purposes.
Conclusion
In summary, this study shows that a large proportion of persons seeking care from two public mental health services had an extremely brief encounter with both of these services.
In terms of patients' characteristics, we found that, both in South Verona and in Western Australia, there was a significant difference in diagnostic severity between once-only contact patients and patients who remained in contact with services. These results are consistent with those of our previous studies in South Verona, showing that patients who did not engage in treatment after the first visit, or who dropped out after treatment was underway, had a less severe disorder than those who remained in contact with services [9], [13]. This result confirms our first hypothesis and lends empirical support to common sense. Clinical judgement would predict that patients who have little distress are more likely to stop treatment. At the same time, clinicians are less likely to make further appointments for patients experiencing minimal distress. This may well indicate good screening at the initial point of contact by both sets of mental health service providers. Regarding our second hypothesis, there does not appear to be a strong relationship between socio-economic status and onceonly contact; when we use educational level, employment status and type of occupation as a proxy of patients' socio-economic condition.
The phenomenon of patients who terminate contact after a single visit, however, needs to be studied further. It is important to clarify how many of these patients had an inappropriate and extremely fast termination of care (early drop-out) and how many sought care from other services (private or alternative providers). One of the most pressing health policy issues in developed countries is how to provide access and continuity of mental health care for people with emotional problems. Followup studies and the parallel use of primary care and specialist care records would reveal more about these issues. In particular, longitudinal studies with a much longer follow-up period are needed to provide greater insight into the vulnerability of those patients who do not engage in the treatment process.
Footnotes
Acknowledgements
This study was supported by the Veneto Region. Progetto: I pazienti che abbandonano il servizio dopo un solo contatto (once-only contact): studio epidemiologico retrospettivo e messa a punto di un modello di prevenzione secondaria. Grant number: 3604.