
Abstract
Reporting on their comparison of media depictions of mental illnesses (1989 versus 1999) Wahl, Wood and Richards [1] observed that people ‘whose expertise derives from dealing on a daily basis with mental illnesses … are seldom included’ (p.26). Their appraisal of the practices of US journalists resonates with our own concern that media portrayals of people living with mental illness rely on ‘experts’ and other third parties who speak generically, and often unsympathetically, about mental disorders [2], [3]. Mass media reliance on third party sources and the disproportionate valuation placed on bizarre and deviant acts [4] have underpinned depictions regularly described as negative and stigmatizing [2],[5–13]. Published studies of newspaper portrayals of mental illnesses [6], [7], [9], [10], [12], [13] do not mention accounts provided by individuals with a mental disorder.
In a prospective national print media sample [3] we classified a small number of items as personal stories – accounts of a person's experiences of mental illness. The source for most personal stories was a third party; a parent, lawyer, or friend, rather than the person whose experiences were being portrayed. That absence of firstperson accounts may reflect the perceived incompetence of people living with mental illness and their consequent lack of credibility as informants about their own experiences. Journalists may also be convinced by the dominant media depictions and consider that interviews with anyone living with a mental illness would be risky and difficult [14].
This article reports our analyses of the few items in a national prospective sample in which people living with mental illness spoke directly to the journalist or wrote their own story. Being allowed to speak does not ensure that the speaker is positioned as a credible or authoritative source [15]. For that reason we first examined how the speakers were portrayed by performing a propositional analysis [16]. To analyse the speakers' representations of themselves and the society (or world) in which they lived we undertook a discourse analysis [17–19]. As in previously reported work [12], [14], [16], [18], [20], [21] we assumed that readers actively engage with and interpret media materials that interest them. Such engaged readers perform their own kind of discourse analysis, rather than passively receiving a message.
Stories for which people living with mental illness were primary sources, were rare. We identified only five among the 600 collected over a four-week period. The paucity of such items is significant both because it may explain why so many researchers [5–9],[11], [12] have not discussed the possibility of such self-depictions and (consequently) do not appear to have considered what the absence of those voices means for the way in which most people understand and respond to mental illnesses. Although we were analysing a miniscule population, it sufficed to demonstrate both that journalists can present such speakers as credible sources and that the speakers rely on different discursive resources in depicting themselves and their experiences than ‘expert’ or other third party commentators.
Method
A commercial clipping bureau was contracted to provide cuttings of all items with any mental health or illness aspect published throughout New Zealand between 3 February and 2 March 1997. Their contract covered items about mental health or mental illness, people with mental disorders, psychiatric patients, treatments, practitioners and mental health services. Terms informally associated with mental illness (e.g. ‘mad’, ‘insane’) and colloquial phrases (e.g. ‘out to lunch’ ‘go completely bananas’) were also included, resulting in a sample of 600 items that ranged from news briefs to full-page newspaper articles.
Each of the 600 items was read closely and all instances in which a person named as having a mental illness spoke directly to readers or was cited by the journalist who had interviewed them, were identified. We excluded articles in which information about central characters and their experiences was primarily provided by a third party, such as a defence lawyer, personal friend, or family member. Articles about people who were not identified as being, or having been, psychiatric patients or who were not identified as having a mental illness were excluded. Thus we excluded statements from an individual who was imprisoned for paedophilia as that was consistently referred to as a crime not a mental disorder. Similarly, items about a man who was classified as ‘mentally defective’ when he was a child were not included.
Each article was assigned an identifying letter, used when citing or referring to paragraphs within the item. Articles were subjected to propositional analysis [16] examining how individual speakers were presented by the journalists. Items were also subjected to close, repeated readings to identify the discursive resources utilized by the speakers. Through our examination of the identified resources we identified five clusters of mutually coherent discursive resources – words, images and storylines [17]. We refer to such patterns of use as themes.
For simplicity, the propositional analysis is reported first. We then summarize each theme following the outline with our description of how the discursive resources of the theme were utilized in the personal stories.
Results
In the corpus of 600 items only five articles (0.8%) offered readers access to thoughts, explanations and depictions provided by people living with a diagnosed mental disorder. Among those five were three backgrounders (A, B, C), a contributed opinion piece (D), and a Letter to the Editor (E). All except E were placed late in the edition among other feature articles.
The articles were:
1
2
3
4
5
Describing the depictions
Of the 148 paragraphs in the five items there were 86 (58%) in which an individual with a mental disorder spoke directly to the reader. That rate is considerably higher than expected for typical ‘nonexpert’ sources [22]. In the full corpus (600 items) lay witnesses were frequently unnamed and their standing as an eyewitness authorized by being introduced as neighbour or participant. In contrast, when ‘experts’ are first cited, they are identified by first and family names together with their title and/or position. After that introduction, ‘experts’ are named using an honorific and their family name [23]. That practice was followed in item A. (Table 1) where three named speakers were introduced (refer to Table 1 for organization names).
Item A. The New Zealand Herald (A19, 15/2/97)
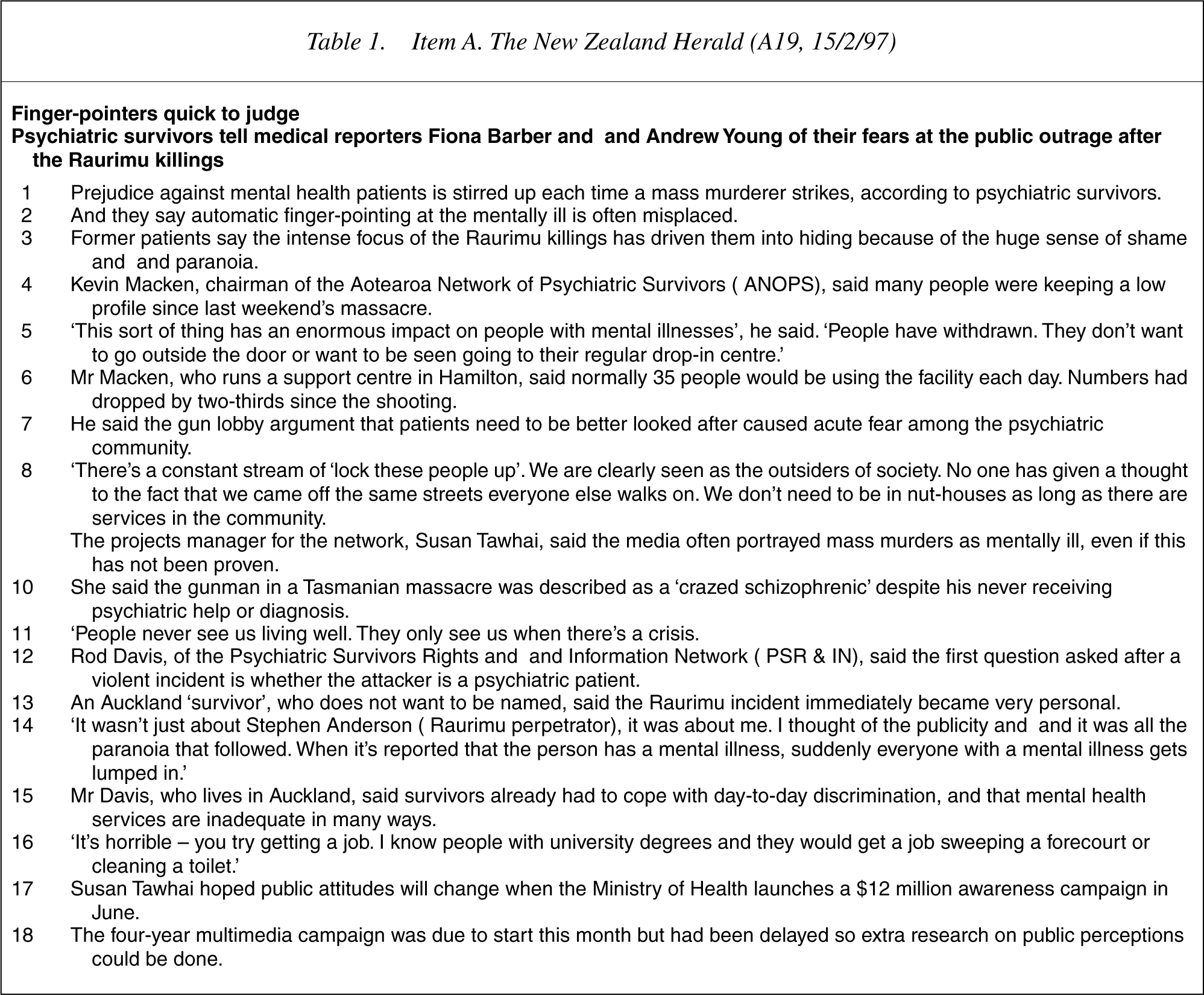
Kevin Macken chairs Aotearoa Network of Psychiatric Survivors (ANOPS), Susan Tawhai is projects manager for ANOPS and Rod Davis is a member of Psychiatric Survivors Rights and Information Network (PSR & IN). The men become Mr Macken and Mr Davis thereafter. Susan Tawhai may not have become Ms Tawhai when next reported (17 August), because The New Zealand Herald discouraged use of ‘Ms’ at that time. However, the writers did not name her merely as ‘Susan’, an overly familiar usage that in factual genres undermines a person's expert standing, though some writers have argued that such familiarity encourages readers to empathise with the source [24]. Within A, the manner in which those speakers were named should be contrasted to the anonymous survivor who described how, ‘the Raurimu incident immediately became very personal’ [9].
A more formal approach to analysing such constructed credibility and authority is to conduct a propositional analysis [16]; breaking each speaker's statements into constituent propositions that are classified by the kind of information provided. Propositional information may be classified as primary (what happened), secondary (explaining why it happened), tertiary (what was it like), evaluations, and recommendations [22]. In a substantial Canadian media database, expert speakers provided more explanations, evaluations, and recommendations compared to lay speakers who were typically limited to primary and tertiary information [22]. The text of Item A (Table 1) is provided so readers may follow the analytic process. The analysis, summarized in Table 2, shows that the named speakers in item A were presented as credible authoritative sources.
Results of propositional analysis of item A
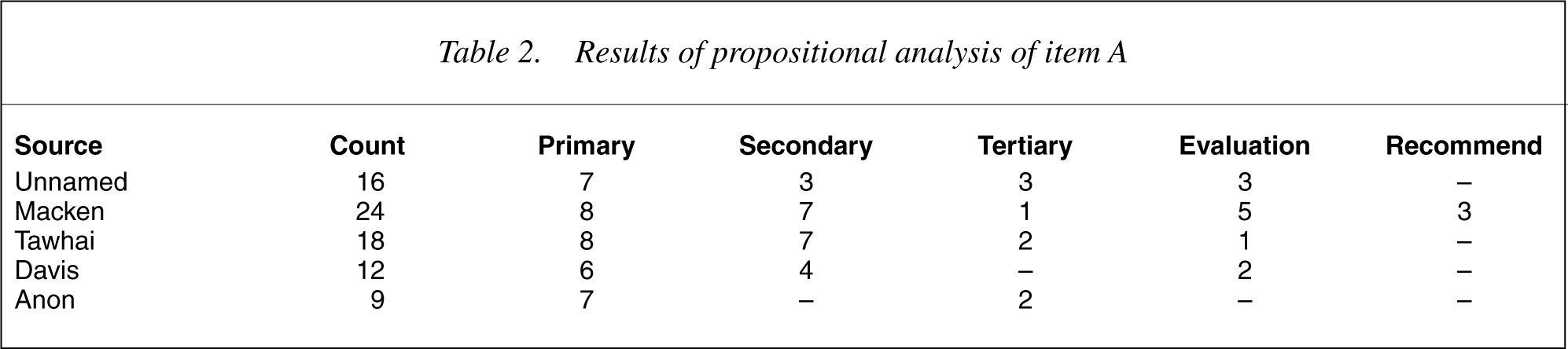
Item A began with three paragraphs that incorporated 16 propositions, listed below, that were attributed to unnamed ‘psychiatric survivors’. Our classification of those propositions, identified as primary (1), secondary (2), tertiary (3), evaluations (E), or recommendations (R) was:
There is prejudice (1) Prejudice is against survivors (1) Prejudice is stirred up (2) A person kills many (1) The killing stirs prejudice (2) There is finger-pointing (1) Finger-pointing is automatic (2) It is (often) misplaced (E) Killings were at Raurimu (1) There was focus on those killings (1) It was intense (E) Survivors felt driven (3) Survivors hid (1) Survivors had a sense of shame (3) Survivors felt persecuted (3) The shame was huge (E)
The statements constituted by these propositions were attributed to the unnamed psychiatric survivors but we cannot recover what else those informants said as the journalists have chosen what was included and how it was presented to readers in their printed story. The predominance of primary and tertiary information (10 of 16 propositions) usually marks eyewitness accounts. Here the ‘what happened’ and ‘what it was like’ propositions established that the speaker(s) did have the requisite experience, a simple form of accrediting. However, the number of explanatory propositions (3) and evaluations (3) mark these speakers as more than just eyewitnesses (see ‘Unnamed’ in Table 2).
The manner in which lay witnesses and ‘experts’ are accorded different propositional loadings (as in [16], Table 3, p. 586) was exemplified by the difference between the anonymous speaker [9], [10] and Rod Davis [8], [11], [12]. There were nine propositions in the former's statement, seven of which described what happened (primary) and two what that was like for him (tertiary). In contrast, a third of the propositions in Mr Davis' statements were explanatory (secondary) as he attempted to convey the prevalence of discrimination that affects ‘everyone with a mental illness’ [10]. Kevin Macken [1–4],[23] was deployed to explain the consequences of inappropriate finger-pointing and a third of the 24 propositions identified in his statements were classified as primary – what happened. However, almost as many propositions (7) were explanatory and he was the only speaker who offered recommendations (3), each closely related to his evaluations (5).
Susan Tawhai's statements were the most difficult to analyse and classify. When first introduced [5], [6] she argued that media always implicated mental illness in mass murders even when the requisite proof was lacking. We adjudged that she presented her four ‘what happened in Tasmania’ propositions as evidence that the media report without requiring proof and we categorized them as explanatory. When she talked of the new ‘awareness campaign’ [13], [14], the information in the propositions was primary – she said what will happen. However, at the time she was interviewed, that information was not public knowledge and hence her description concurrently positioned her as an insider – one who knows about changes and the reasons for them – rather than merely being a witness to events.
Describing clusters of discursive resources
While this was not a large body of talk (only 148 paragraphs) we identified a range of discursive resources only some of which were familiar from previous analyses of factual genres of print media [14], [16], [19], [23]. At least as important as the use of novel resources was the clustering of those resources. In this small body of discourse we identified five themes, all of which were new to us. Each of those themes is named and briefly described and we then indicate the ways in which the theme's resources were utilized by the speakers.
Ordinariness/Living well
The speaker presented those living with a mental illness as ordinary (unremarkable) members of society who not only do everyday things well but who recognized themselves as being productive and having social standing.
That ordinariness, represented by Kevin (‘we came off the same streets everyone else walks on’) (A, 8), was typified by routine actions such as cooking, washing, ironing, and organizing a life. Such routine competence was complemented by references to personal responsibilities – chairman, projects manager, author and motivational speaker, or organiser of support services – that were performed effectively. Effective performance of such roles was understood to add standing as they demonstrated personal skills and strength. Some of the performances included among the self-portrayals were very unexpected, as when Desiree claimed to be ‘capable of putting anyone in an armlock and strangling them if need be’ (C, 35). Such extra-ordinary capabilities were represented as the speaker's personal response to being victimized or abused and as having enabled the speaker to move from passivity to ‘living well’ (A, 11). Five of the eight speakers in these items clearly and repeatedly utilized elements of this theme.
Vulnerability
The speaker constituted people living with mental illness as helpless, unable to control their own lives, and as subjected to the prejudices of the wider society.
Such vulnerability, the person as object of another's actions, was exemplified in Desiree's story about returning from a cooking lesson (C, 29–30) when the taxi driver ‘showered her with unwanted attention by kissing her on the lips’ after he had dropped her at her doorstep. She clearly saw his act as an invasion:
If I had been able to see it coming [Desiree is blind] I would have given him a blow to the chops, but he took advantage of my defencelessness…
Among the identified elements of this cluster were being scared of being introspective and ‘obsessive about going downhill’ (B, 32), being ‘mucked up’ by drugs that make one feel awful (B, 26), committals, depression, and feeling that no one cares. Also included in this theme were references to being or feeling different from others, elements that apparently related to the speaker's vulnerability to being unmasked and identified as ‘mentally tainted’ [25]. We interpreted those statements as depicting a vulnerability that was a direct consequence of the widely held, stigmatizing beliefs about people living with a mental illness. In analyses of prime-time dramas we identified a similar theme [18] but, in those fictional portrayals, vulnerability was often associated with a level of personal incompetence that was dangerous to that character and those about them. As depicted by these speakers, vulnerability was not associated with such dangerousness.
Stigma
The speakers constructed themselves and fellow consumers as living with the effects of stigmatizing beliefs and prejudices about mental disorders.
Speakers emphasized that they faced ‘unwarranted fear and condemnation’ (B, 15), were ‘scared of what… they'll think’ (B, 3), and that their ‘illness is always a secret’ (D, 10). They stressed the negative consequences for other sufferers: ‘[they] don't want to go outside the door’ (D, 5), ‘facing daily discriminations and prejudices struggling for acceptance’ (E, 3) and having ‘people pander to her condition’ (C, 49). Societal discrimination was exemplified by accommodation; ‘living in substandard conditions’ (D, 3) and employment; ‘people with university degrees… sweeping a forecourt or cleaning a toilet’ (A, 16) or doing ‘only menial jobs’ (D, 14). Interpersonal discrimination, ‘[they] treat me like a little girl’ (C, 50) was represented as resulting from other people's fears of those with a mental illness (D, 10) and, like many mental health professionals, the speakers argued that media fed those fears. ‘Justice Heron commented on the danger of untreated schizophrenics’ (B, 28), ‘tragic consequences which are well publicised’ (E, 17), and ‘suddenly everybody with a mental illness gets lumped in’ (A, 14).
Crisis
Speakers utilized this cluster of resources to construct two kinds of crisis, one kind of crisis was portrayed as initiating or as part of the disorder; the second kind was created by publicity about events in which a person with a mental disorder acted in ways that confirmed stereotyped representations of mental illness.
The first kind of crisis was exemplified by paranoia about family plans to kill the sufferer (B, 1), serious damage in preadult years (D, 11), lack of information (C, 48), disruptions in patients' lives (E, 15), and suicide attempts (C, 19). Such crises were constructed in conjunction with the following theme (5. Disorder/Treatment) in ways that enabled them to be acknowledged without having the crisis dominate the story or their self-depiction.
The second kind of crisis arose from public fears that persons with a mental disorder were criminally violent. Such fears were animated or confirmed by summaries of actual events ‘sentencing two sufferers to jail, one had stabbed a woman’ (B, 28), ‘suffering from paranoid schizophrenia before and up to the time she killed her grandmother’ (B, 29). Portraying their experiences of such media-led crises speakers included critiques of media practices; ‘over reporting’ (B, 15), ‘intense focus’ (A, 3). They also expressed anger over misuse or misappropriation of psychiatric terms, ‘[the] gunman in a Tasmanian massacre was described as a ‘crazed schizophrenic’ despite never receiving psychiatric help or diagnosis' (A, 1, 10). In constructing the stigma and discrimination that were such a powerful forces in their lives, speakers drew on themes identified in earlier work as dangerousness and threat [18], [19].
Disorder/Treatment
The speakers used elements of this theme in constructing their personal account of their disorder and the treatment they needed or had experienced.
We found that this theme was dominated by routines; ‘[being] diagnosed as having schizophrenia’ (B, 2), ‘being cared for by trained staff’ (E, 14), taking ‘lithium tablets daily for the rest of her life’ (C, 21), and desirable ‘treated as a whole person’ (D, 6), or undesirable experiences ‘being unable to understand the experiences’ (C, 19). In this cluster we included references to research findings, ‘[schizophrenia] affects 1 in 100, interferes with personality and everyday functioning’ (B, 5), and ‘many schizophrenics recover totally or substantially’ (B, 31) because the speakers were enlisting the disinterested authority of science to support their depiction of their condition. Also included here were legal definitions associated with committal, ‘mental disorder… an abnormal state of mind… poses serious danger to the health or safety of the person or others, seriously diminishes the capacity… to take care of himself or herself’ (E, 6–8).
While the described elements were consistent with speakers positioning themselves as patients they drew on other themes and discursive resources to portray what they needed to live well with a mental disorder. Foremost among such resources was support, ‘necessary support and caring (D, 2), ‘services in the community’ (A, 8), ‘delivering care and wellbeing to psychiatric patients’ (E, 1). Respite care, for sufferers and/or caregivers, was viewed as central to such support by two speakers Lynne (D, 16) and the letter writer (E, 5, 14–16). In this body of talk, representations of families were mixed; Desiree portrayed her family as responsible for her manic depression and her sister's suicide (C, 40–46), while the letter writer (E, 12, 16) portrayed families as treatment resources.
Discussion
Like the speakers in the analysed stories our analyses and interpretation should be viewed against the negative stereotypes of ‘persons with a mental illness’ that dominate media depictions [2],[5–13]. We were disappointed that so few articles met our inclusion criteria although that rarity probably explains why researchers have not previously discussed the self-depictions of those living with a mental disorder. Nevertheless we demonstrated that these speakers not only offered qualitatively different depictions of mental illness in newspapers compared to those previously described [2], [3], [6], [7], [9], [10], [12] but also that they were presented as credible sources by the journalists. Given the miniscule set of analysed items we do not regard our account as definitive especially as the analysed materials pre-date sustained efforts to address the stigmatization of mental illnesses in New Zealand and Australia.
The qualitative difference between these depictions and those more typically described depended primarily on two themes, neither of which had been previously described. We called those themes Ordinariness/Living Well, and Stigma. Consistent with television producers' efforts to construct persons with a mental illness as ordinary [26], speakers sought to portray themselves as everyday people. Unlike Henderson's producers [26], these speakers utilized diverse resources such as; having positive self-esteem, overcoming adversity, and being productive and effective, to represent themselves as ordinary. Further, the speakers deployed their depicted ordinariness in conjunction with portrayals of stigma to represent negative media portrayals of mental illnesses as inappropriate and unjust. Through the resources of the Ordinariness/Living Well theme speakers addressed the technical problem of communicating that they were people like the reader and were not to be defined or limited by the disorder with which they lived [26], [27].
Drawing on resources from the Vulnerability, Stigma, and Crisis themes speakers constructed the rather forbidding social world within which they found themselves. That construction required speakers to exercise considerable care as paranoia is a symptom of ‘classical madness’ [10], p. 15] and readers might be predisposed to interpret a speaker's portrayal of society as dangerous and threatening as ‘being paranoid’. In our previous work we had highlighted the dominance of dangerousness and criminality in media depictions of mental illnesses [18–21],[23] and noted, like other authors [28–30], that many of those individuals were portrayed as fearsome. The analysed speakers made some use of dangerousness and criminality resources (Crisis theme) both to direct attention to media constructions of events, and to portray their own experience of living in a society where those stereotypes had wide currency. They talked about the personal implications of media reportage and of feeling even more stigmatized by such coverage. In constructing themselves as recognizably similar to the readers they were able to portray unthinking, stereotypedriven responses as ‘finger pointing’ (A, 2) that was unjustified and personally disabling.
Our analysis of these five items served two purposes; it established that, when given the chance, consumers depicted themselves and their experiences in accessible and recognizably human ways; it also demonstrated that, at least some, journalists can interview consumers and have their work published. The paucity of items underlined the importance of changing the culture and practices of journalism that appear to discourage such reporting [4]. That the speakers depicted themselves as normal, human, and understandable is consistent with international efforts to destigmatize mental illnesses in that they enabled readers to meet consumers as individuals who revealed themselves as much like readers [27], [31], [32].