
Abstract
Objective:
Despite growing literature on psychotic experiences, no nationally representative study has reported on the prevalence of both hallucinatory experiences and delusional experiences in Australian adolescents. Also, while many studies have examined the association between psychotic experiences and certain demographic and clinical correlates, there are more variables of interest to be investigated, including disordered eating behaviour and hours of sleep. The aims of this study were to examine (1) the prevalence of hallucinatory experiences and delusional experiences in Australian adolescents, and (2) the associations between different types of psychotic experiences with a broad range of demographic, clinical, and psychosocial variables.
Methods:
A random sample of Australian adolescents aged 14- to 17-year-olds were recruited in 2013–2014 as part of the Young Minds Matter Survey. Participants completed self-report questions regarding five different psychotic experience types (auditory and visual hallucinatory experiences, and thoughts read, special messages, spied upon) experienced in the past 12 months. Using logistic regression analyses, we investigated associations between psychotic experiences and demographic, clinical, and psychosocial factors.
Results:
The 12-month prevalence ranged from 3.3% (95% confidence interval = [2.6, 4.3]) for special messages to 14.0% (95% confidence interval = [12.3, 15.8]) for auditory hallucinatory experiences. At the bivariate level, each psychotic experience subtype was associated with increased likelihood of major depression, being bullied, psychological distress, low self-esteem, mental health service use and insufficient sleep (<8 hours per night). Multivariate analyses revealed both auditory and visual hallucinatory experiences were associated with an increased likelihood of four of these variables (depression, being bullied, service use, insufficient sleep), whereas associations with delusional experiences were inconsistent.
Conclusion:
Hallucinatory and delusional experiences are common in Australian adolescents. Hallucinatory experiences, rather than delusional experiences, may be more clinically relevant in this demographic. When psychotic experiences are endorsed by adolescents, further assessment is indicated so as to ascertain more detail on the phenomenology of the experiences to better understand their clinical relevance.
Introduction
There has been increasing interest in population-based studies of psychotic experiences (PEs) in adolescents. These experiences, defined as occurring outside the context of sleep or substance use, may be appraised as clinically relevant symptoms (hallucinations or delusions) through to subclinical/subthreshold experiences, not prompting help-seeking behaviour (van Os et al., 2009; Yung and Lin, 2016). While PEs in adolescents are associated with an increased risk of psychosis (Connell et al., 2016; Poulton et al., 2000), they more commonly reflect other forms of mental illness such as depression, cannabis use and anxiety (Dolphin et al., 2015; Scott et al., 2009; Yung et al., 2009). PEs have also been strongly linked to physical health problems (Moreno et al., 2013) and negative environmental exposures, such as bullying and childhood trauma (Kelleher et al., 2013), and are robustly associated with an increased likelihood of suicidal behaviours (Hielscher et al., 2017; Honings et al., 2016). In adolescents, PEs are indicators for an increased risk of current and future poor mental health and psychosocial outcomes.
In a cross-national survey of 31,261 respondents, McGrath et al. (2015) found that 5.8% of the population reported PEs in their lifetime, with hallucinatory experiences (HEs; 5.2%) more common than delusional experiences (DEs; 1.3%). Among adolescents the prevalence was higher, particularly for DEs in younger (< 29 years) versus older respondents (60 + years) after multivariate adjustment, odds ratio (OR) = 2.4; 95% confidence interval (CI) = [1.1, 5.0]. A 19-study international meta-analysis reported a median PE prevalence of 7.5% among adolescents aged 13-18 years (Kelleher et al., 2012). This is consistent with the prevalence reported in Australia.
The prevalence of hallucinations in Australian adolescents has previously been reported as 8.4% (Scott et al., 2009) from the first national youth mental health survey (The Australian National Survey of Mental Health and Wellbeing; Sawyer et al., 2001), which was conducted in 1998. However, there are some existing gaps in the literature. Australian studies reporting the prevalence of other PE subtypes (e.g. persecutory ideation, grandiose thinking, Scott et al., 2008; Varghese et al., 2011; Yung et al., 2009) have been conducted in either young adult samples (18+ years) (Scott et al., 2008; Varghese et al., 2011), or non-representative samples of Australian adolescents (Yung et al., 2009). To date, no nationally representative Australian study of adolescents has reported the prevalence of both HEs and DEs independently.
The relationship between PEs and mental ill health has been reported as bidirectional (McGrath et al., 2016). Adolescents who hallucinated were more likely to have high symptom scores for anxiety, depression and inattention-hyperactivity (McGee et al., 2000). Hallucinations have also been shown to be associated with a Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) diagnosis of depression, and they were three times more likely to occur in those adolescents who had smoked cannabis in the previous month (Scott et al., 2009). However, these studies either examined associations of mental ill health with HEs (Scott et al., 2009), or they collapsed HEs and DEs into one broad PE variable (McGrath et al., 2015). Studies that have investigated the correlates of different PE subtypes have found each one is differentially associated with mental illness and impairment in functioning (Capra et al., 2015; Dhossche et al., 2002; Dolphin et al., 2015). For example, Dhossche et al. (2002) found adolescents who reported auditory but not visual HEs had higher rates of depressive disorders, whereas Dolphin et al. (2015) found those with HEs, but not paranoid thoughts, had higher rates of recent cannabis use. Therefore, it is important for studies to distinguish the different types of PEs as there is variation in their clinical relevance.
While many studies have examined the association between PEs and some demographic and clinical correlates, there remain variables of interest which have not been investigated (Dolphin et al., 2015). Only one study of adults (Koyanagi et al., 2016) has explored the association between PEs and disordered eating behaviour, which reported a strong association (OR = 3.44; 95% CI = [1.85, 6.39]). Given disordered eating often emerges in adolescence (Favaro et al., 2009), there is a need to examine this association in this demographic. Also, despite several studies on the association between PEs and sleep disturbances, as measured by the presence of nightmares or subjective sleep ratings (Lee et al., 2012; Oh et al., 2016), no study to date has investigated the association between PEs and hours of sleep. Adolescents sleeping less than 8 hours per night have an increased risk of a broad range of health and other problems, including poor academic performance, obesity, and increased risk of suicidality (Lui, 2004; Snell et al., 2007). It would be useful to investigate whether this 8-hour cut-off for insufficient sleep is also associated with PEs in adolescents.
To address the gaps in the literature, we had the opportunity to examine the prevalence of auditory and visual HEs, as well as DEs in a nationally representative sample of Australian adolescents. Furthermore, we examined the associations between different types of PEs with a broad range of demographic, clinical and psychosocial variables including disordered eating behaviour and hours of sleep. Finally, we aimed to determine the variability between the strengths of the associations with each type of PE and the demographic and clinical variables so as to ascertain which PEs are clinically important in adolescents.
Methods
Sample
The Young Minds Matter (YMM) survey is a national study of mental health and wellbeing of children and adolescents aged 4–17 years, where data were collected between 31 May 2013 and 10 April 2014. The design, sampling and survey interview methods are described extensively elsewhere (Hafekost et al., 2016; Lawrence et al., 2016). Briefly, the survey employed area-based random sampling with voluntary recruitment and consent of households in scope where there was at least one child aged 4–17 years (up to but not including the age of 18) who were residing in private dwellings in Australia. Children who usually spent more than 50% of their time in another household and less than 50% in the selected household were not in scope. Other exclusion criteria were: The 1% most remote SA1s in Australia (considered standard practice for surveys that aim to yield estimates at a national level); children who were homeless or in institutional care (a completely different approach would be required to represent this population adequately); and children in families where the interview could not be conducted in English. Also, it should be noted that the survey could not produce estimates of mental disorders and service use for Indigenous Australians nor other minority groups (e.g. refugees and asylum seekers) which experience higher levels of distress and trauma than the general population (Silove et al., 2007), and thus would likely report an elevated prevalence of PEs.
As previously described in Hafekost et al. (2016), the survey sample was recruited in two parts. In total, 46,248 households were approached to yield a main sample of 5508 participating families with children aged 4–17 years, supplemented by an additional sample of 802 participating families with 16- to 17-year-olds recruited by approaching 30,358 households. Of the 46,248 households approached for the main sample, 32,526 did not have children aged 4–17 years, 3778 did have children but did not participate, and for 4438, no contact was made. For the supplementary sample of 16- to 17-year-olds, of the 30,358 households approached, 27,800 did not have children aged 16–17 years; 452 did have children but did not participate; and for 1304 no contact was made or it was not possible to determine if they had children aged 4–17 years, yielding an overall response rate of 55%.
Of the final participating sample of 6310 families with children aged 4–17 years, 2251 of the children were aged 14–17 years. Of these, 2004 completed the youth self-report questionnaire (89%) which assessed for PEs. For all these young people, the primary carer completed a survey which included a question on whether the young person had ever been diagnosed with a psychotic disorder. The research protocol for the study was approved by the Australian Government Department of Health Human Research Ethics Committee, and The University of Western Australia Human Research Ethics Committee.
National representativeness of sample
Comparisons with 2011 Census data showed that the YMM sample was broadly representative of the overall Australian population in terms of the following demographic characteristics: socio-economic status indicators, geographic area, gender of child, family structure, household income, country of birth, labour force status and dwelling tenure (Lawrence et al., 2016). The YMM sample only differed from the 2011 Census data in terms of age of the child (higher proportion of 4- to 7-year-olds) and number of children in the household (survey sample under-represented children from families with only one eligible child).
Measures
A self-report questionnaire was completed in the home by survey participants aged 11–17 years. Consenting participants completed the questionnaire in private using a tablet computer. All responses were confidential and not shared with the consenting parent. The questions about PEs were only asked of those aged 14–17 years (n = 2004). This sample was the focus of the current study.
PEs
The 12-month PEs were assessed in the YMM survey using five items from the Diagnostic Interview Schedule for Children (DISC-IV; Shaffer et al., 2000) psychosis module: auditory HEs (‘In the last year have you heard things other people could not hear, such as a voice?’ Yes/No); visual HEs (‘In the last year have you seen something or someone that other people who were present could not see, that is had a vision when you were completely awake?’); thoughts read (‘In the last year, have you ever believed that someone was using special powers to read your mind?’); special messages (‘In the last year, have you ever believed that you were being sent special messages through the TV or radio or that a programme had been arranged for you alone and no one else?’); and spied upon (‘In the last year, have you ever believed that people were spying on you?’). If participants responded ‘Yes’ to any of these questions, a follow-up question was asked: ‘Did these experiences happen when you were taking drugs or drinking alcohol?’ Participants were classified as endorsing PEs if they responded ‘No’ to this question.
Three participants did not complete all the PE questions, and therefore were excluded from the sample. In the parent or carer interview, three respondents reported their child had been diagnosed with schizophrenia or other psychotic disorders. As the focus of the study was on PEs in those who did not reach the clinical threshold for a psychotic diagnosis we also excluded these participants, leaving a final sample for analysis of 1998 adolescents.
Correlates of interest
Potential correlates of interest were selected based on the results of existing reviews or other papers on PEs (de Armando et al., 2010; Dolphin et al., 2015; De Leede-Smith and Barkus, 2013; Scott et al., 2009, 2008). Specifically, we followed the approach taken by Dolphin et al. (2015), where the authors examined the association between PEs and factors from five domains in adolescents. In this study, we considered correlates across seven domains.
Statistical analysis
All analyses were conducted using Stata/IC 14 (Stata Corp., College Station, Texas, USA, 2015). Survey data were weighted using the Stata svyset procedure to represent the full Australian population of 14- to 17-year-olds accounting for sex, age, family size, household income and deliberate oversampling of 16- to 17-year-olds (Hafekost et al., 2016). The statistical analysis was mainly descriptive in nature, where we report on the prevalence of each PE subtype (auditory and visual HEs, as well as thoughts read, special messages and feeling spied upon). Survey estimates and associated CIs were calculated using the method of Taylor Series Linearisation (Wolter, 2007).
The associations between correlates of interest and each PE subtype were investigated using univariate logistic regression, reported as unadjusted ORs. A second multivariate logistic regression analysis was also conducted, including all variables in the model, to ascertain the relationship between PEs and each factor while controlling for potential confounders. There was no evidence of multicollinearity based on standard thresholds for the variance inflation factor.
Results
Prevalence of PEs
Of the 1998 participants, the 12-month prevalence of auditory HEs was 14.0% (95% CI = [12.3, 15.8]) (see Table 1). In terms of the other PE subtypes, 13.8% reported being spied upon (95% CI = [12.1, 15.6]), 10.6% reported visual HEs (95% CI = [9.1, 12.3]), 5.6% reported their thoughts being read (95% CI = [4.6, 6.8]), and 3.3% reported receiving special messages through the television or radio (95% CI = [2.6, 4.3]).
Psychotic experiences among 14-17 years in the Young Minds Matter (YMM) survey, by sex.
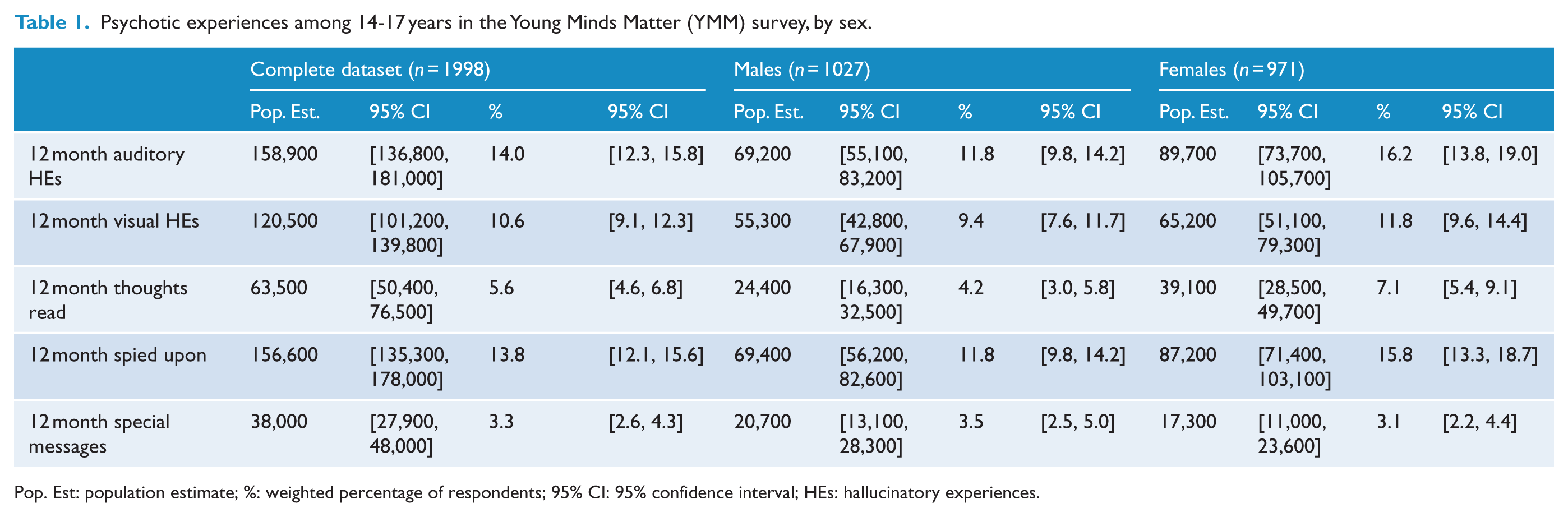
Pop. Est: population estimate; %: weighted percentage of respondents; 95% CI: 95% confidence interval; HEs: hallucinatory experiences.
Correlates of PE subtypes
Tables 2–6 present the bivariate associations between each PE subtype and variables in each of the seven domains. In terms of sociodemographics, thoughts being read (Table 4) and feeling spied upon (Table 6) were the only PEs to be associated with both age and sex; where younger, female respondents were more likely to endorse these items compared to their older, male counterparts. In terms of clinical and psychosocial variables, each subtype was associated with major depression, being bullied, psychological distress, low self-esteem, mental health service use, insufficient sleep, and substance use (except for thoughts being read, which was not associated with substance use at the bivariate level). None of the PE subtypes were associated with parental mental illness. Only auditory HEs and feeling spied upon were associated with social isolation. Two of the three DEs (thoughts read, spied upon) were associated with disordered eating behaviour, whereas HEs (both auditory and visual) were not.
Sociodemographic, clinical, and psychosocial correlates of auditory hallucinatory experiences (N = 1998).
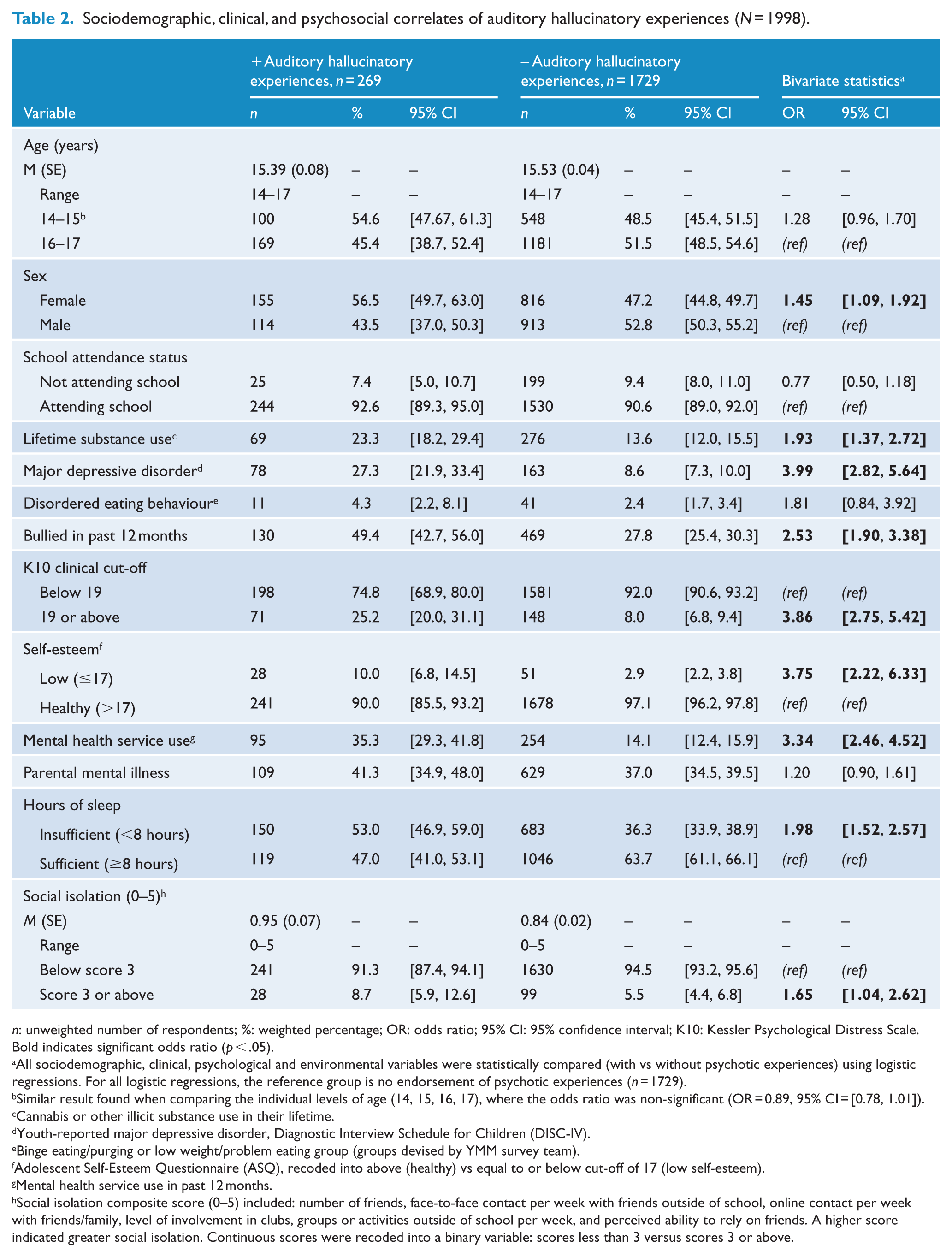
n: unweighted number of respondents; %: weighted percentage; OR: odds ratio; 95% CI: 95% confidence interval; K10: Kessler Psychological Distress Scale.
Bold indicates significant odds ratio (p < .05).
All sociodemographic, clinical, psychological and environmental variables were statistically compared (with vs without psychotic experiences) using logistic regressions. For all logistic regressions, the reference group is no endorsement of psychotic experiences (n = 1729).
Similar result found when comparing the individual levels of age (14, 15, 16, 17), where the odds ratio was non-significant (OR = 0.89, 95% CI = [0.78, 1.01]).
Cannabis or other illicit substance use in their lifetime.
Youth-reported major depressive disorder, Diagnostic Interview Schedule for Children (DISC-IV).
Binge eating/purging or low weight/problem eating group (groups devised by YMM survey team).
Adolescent Self-Esteem Questionnaire (ASQ), recoded into above (healthy) vs equal to or below cut-off of 17 (low self-esteem).
Mental health service use in past 12 months.
Social isolation composite score (0–5) included: number of friends, face-to-face contact per week with friends outside of school, online contact per week with friends/family, level of involvement in clubs, groups or activities outside of school per week, and perceived ability to rely on friends. A higher score indicated greater social isolation. Continuous scores were recoded into a binary variable: scores less than 3 versus scores 3 or above.
Sociodemographic, clinical and psychosocial correlates of visual hallucinatory experiences (N = 1998).
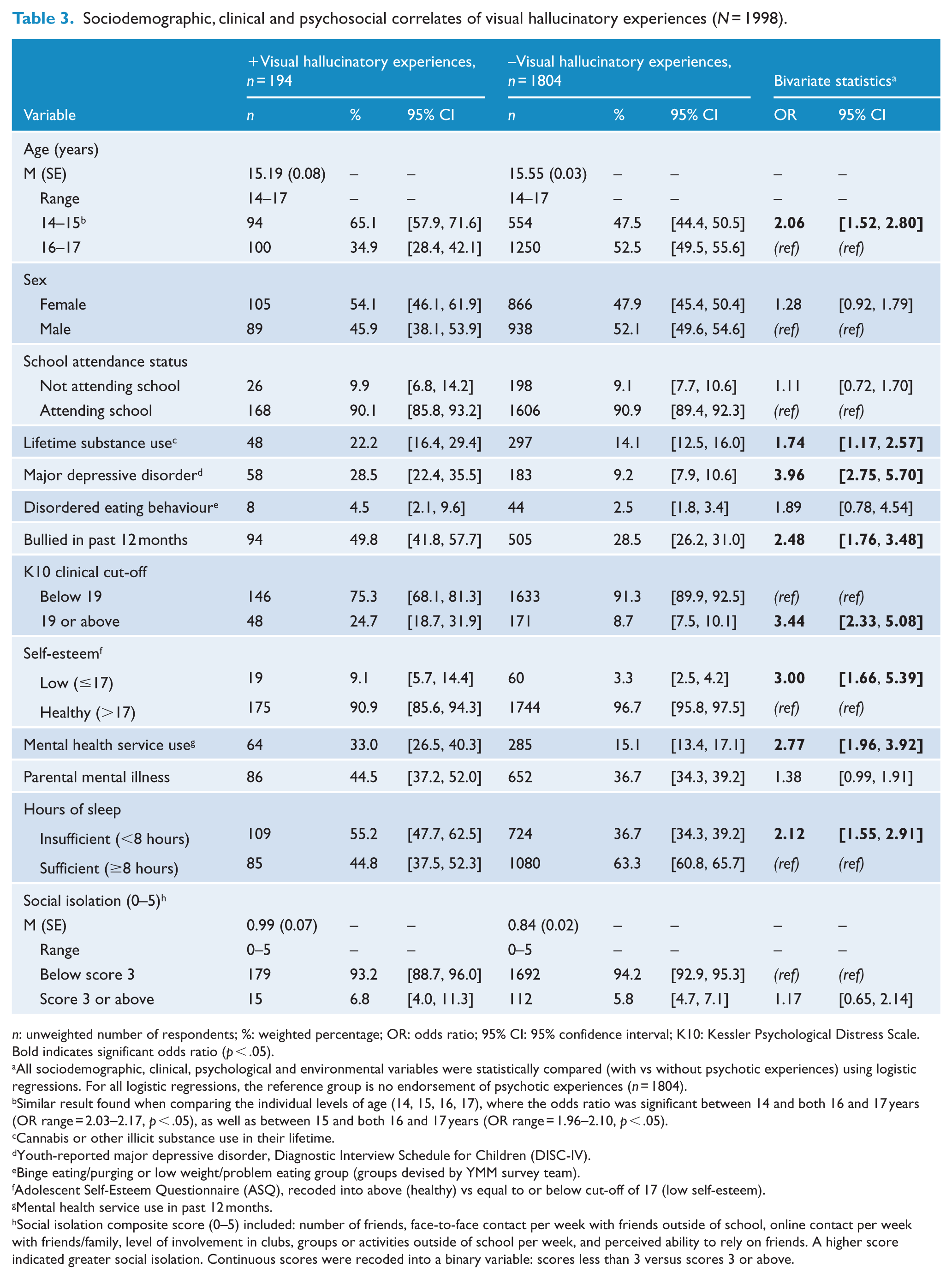
n: unweighted number of respondents; %: weighted percentage; OR: odds ratio; 95% CI: 95% confidence interval; K10: Kessler Psychological Distress Scale.
Bold indicates significant odds ratio (p < .05).
All sociodemographic, clinical, psychological and environmental variables were statistically compared (with vs without psychotic experiences) using logistic regressions. For all logistic regressions, the reference group is no endorsement of psychotic experiences (n = 1804).
Similar result found when comparing the individual levels of age (14, 15, 16, 17), where the odds ratio was significant between 14 and both 16 and 17 years (OR range = 2.03–2.17, p < .05), as well as between 15 and both 16 and 17 years (OR range = 1.96–2.10, p < .05).
Cannabis or other illicit substance use in their lifetime.
Youth-reported major depressive disorder, Diagnostic Interview Schedule for Children (DISC-IV).
Binge eating/purging or low weight/problem eating group (groups devised by YMM survey team).
Adolescent Self-Esteem Questionnaire (ASQ), recoded into above (healthy) vs equal to or below cut-off of 17 (low self-esteem).
Mental health service use in past 12 months.
Social isolation composite score (0–5) included: number of friends, face-to-face contact per week with friends outside of school, online contact per week with friends/family, level of involvement in clubs, groups or activities outside of school per week, and perceived ability to rely on friends. A higher score indicated greater social isolation. Continuous scores were recoded into a binary variable: scores less than 3 versus scores 3 or above.
Sociodemographic, clinical and psychosocial correlates of thoughts being read (N = 1998).
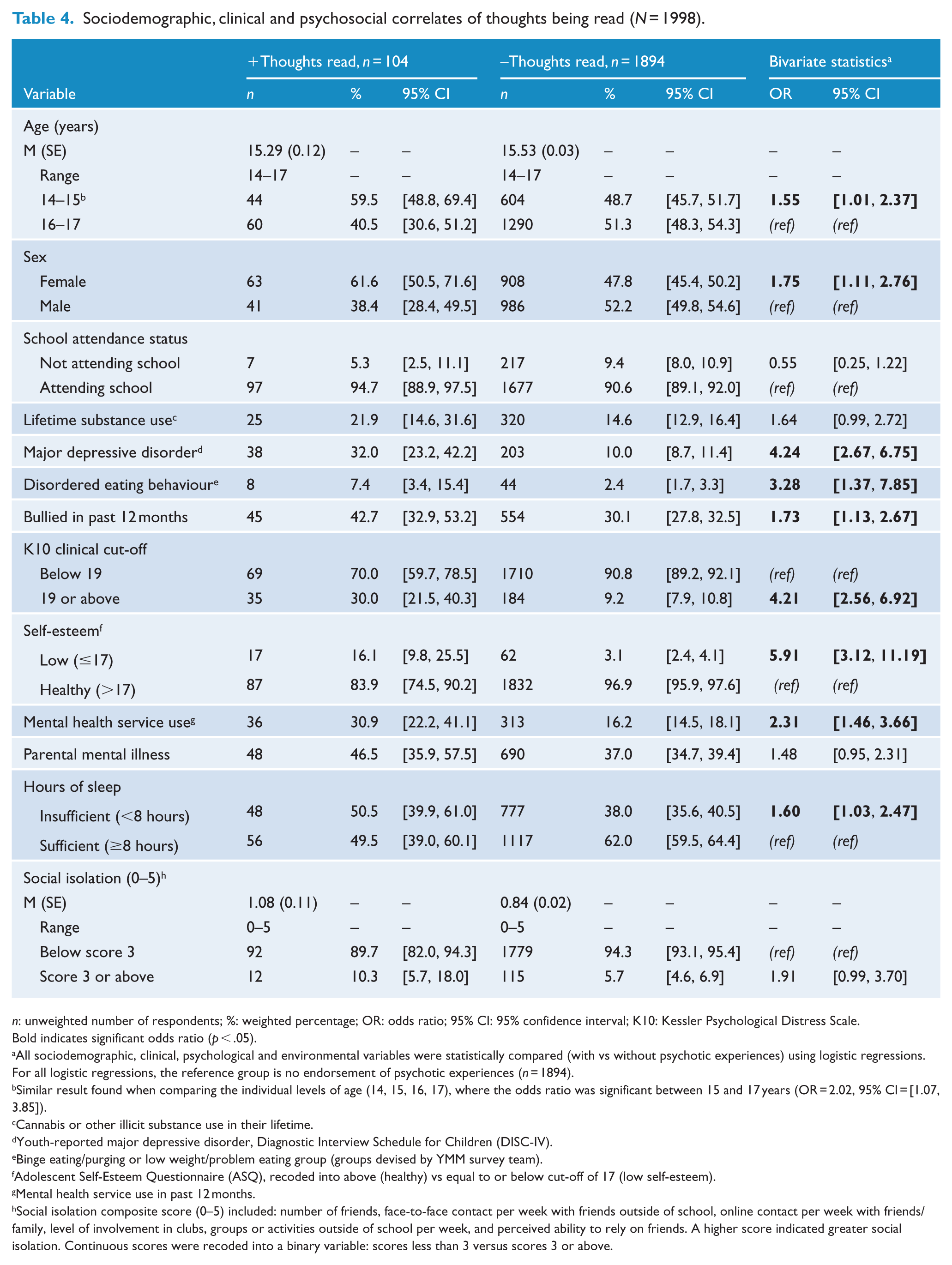
n: unweighted number of respondents; %: weighted percentage; OR: odds ratio; 95% CI: 95% confidence interval; K10: Kessler Psychological Distress Scale.
Bold indicates significant odds ratio (p < .05).
All sociodemographic, clinical, psychological and environmental variables were statistically compared (with vs without psychotic experiences) using logistic regressions. For all logistic regressions, the reference group is no endorsement of psychotic experiences (n = 1894).
Similar result found when comparing the individual levels of age (14, 15, 16, 17), where the odds ratio was significant between 15 and 17 years (OR = 2.02, 95% CI = [1.07, 3.85]).
Cannabis or other illicit substance use in their lifetime.
Youth-reported major depressive disorder, Diagnostic Interview Schedule for Children (DISC-IV).
Binge eating/purging or low weight/problem eating group (groups devised by YMM survey team).
Adolescent Self-Esteem Questionnaire (ASQ), recoded into above (healthy) vs equal to or below cut-off of 17 (low self-esteem).
Mental health service use in past 12 months.
Social isolation composite score (0–5) included: number of friends, face-to-face contact per week with friends outside of school, online contact per week with friends/family, level of involvement in clubs, groups or activities outside of school per week, and perceived ability to rely on friends. A higher score indicated greater social isolation. Continuous scores were recoded into a binary variable: scores less than 3 versus scores 3 or above.
Sociodemographic, clinical and psychosocial correlates of receiving special messages (N = 1998).
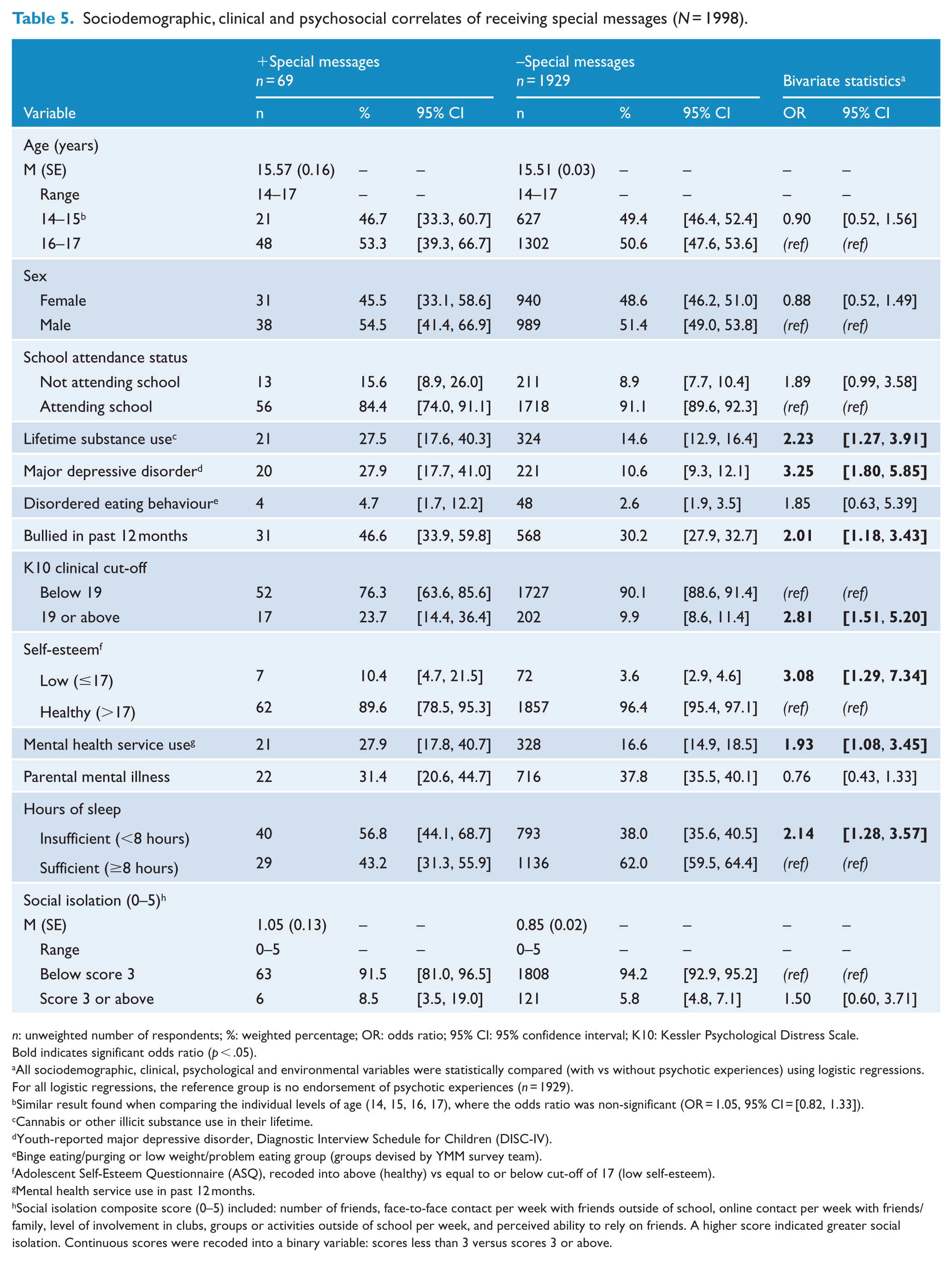
n: unweighted number of respondents; %: weighted percentage; OR: odds ratio; 95% CI: 95% confidence interval; K10: Kessler Psychological Distress Scale.
Bold indicates significant odds ratio (p < .05).
All sociodemographic, clinical, psychological and environmental variables were statistically compared (with vs without psychotic experiences) using logistic regressions. For all logistic regressions, the reference group is no endorsement of psychotic experiences (n = 1929).
Similar result found when comparing the individual levels of age (14, 15, 16, 17), where the odds ratio was non-significant (OR = 1.05, 95% CI = [0.82, 1.33]).
Cannabis or other illicit substance use in their lifetime.
Youth-reported major depressive disorder, Diagnostic Interview Schedule for Children (DISC-IV).
Binge eating/purging or low weight/problem eating group (groups devised by YMM survey team).
Adolescent Self-Esteem Questionnaire (ASQ), recoded into above (healthy) vs equal to or below cut-off of 17 (low self-esteem).
Mental health service use in past 12 months.
Social isolation composite score (0–5) included: number of friends, face-to-face contact per week with friends outside of school, online contact per week with friends/family, level of involvement in clubs, groups or activities outside of school per week, and perceived ability to rely on friends. A higher score indicated greater social isolation. Continuous scores were recoded into a binary variable: scores less than 3 versus scores 3 or above.
Sociodemographic, clinical and psychosocial correlates of feeling spied upon (N = 1998).
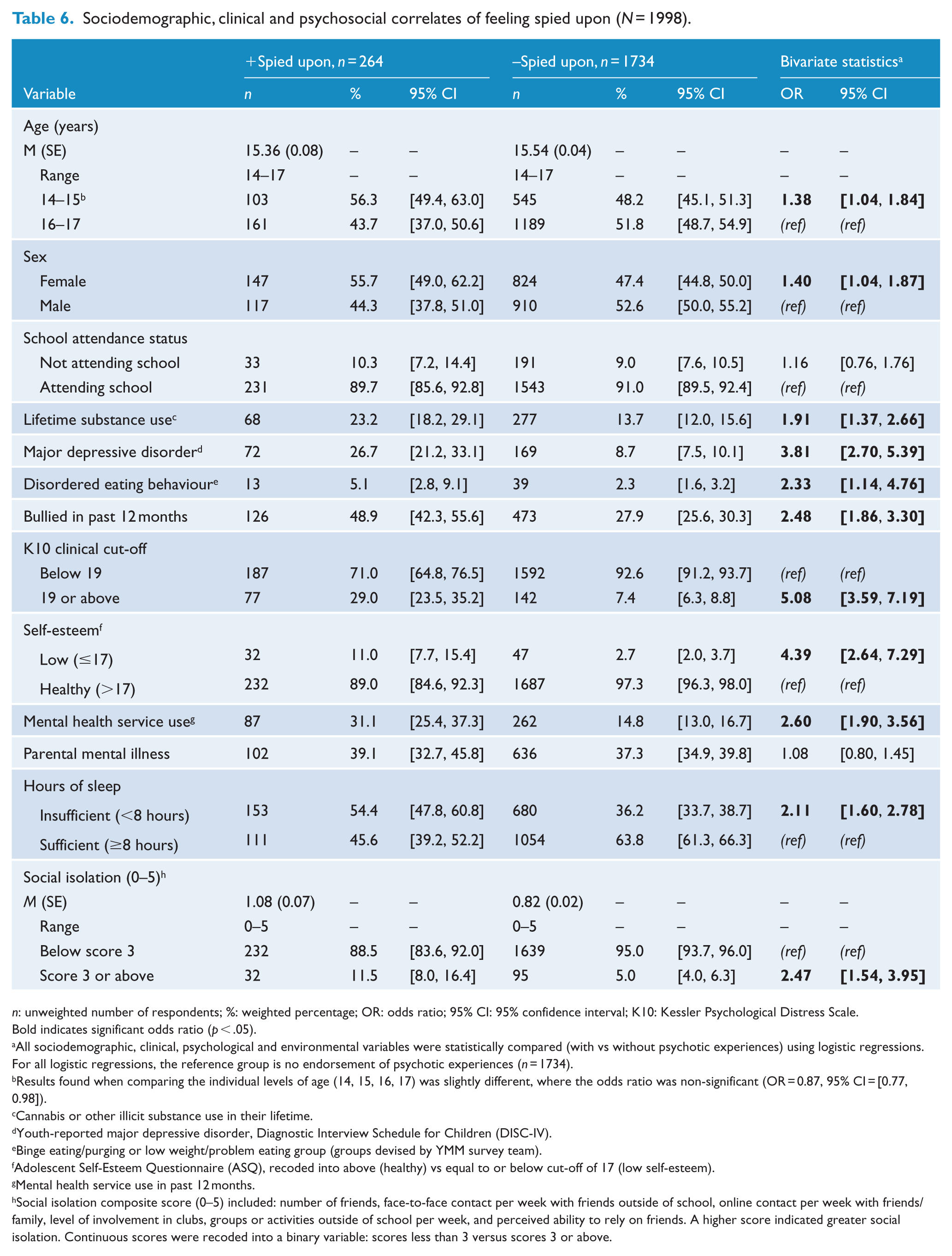
n: unweighted number of respondents; %: weighted percentage; OR: odds ratio; 95% CI: 95% confidence interval; K10: Kessler Psychological Distress Scale.
Bold indicates significant odds ratio (p < .05).
All sociodemographic, clinical, psychological and environmental variables were statistically compared (with vs without psychotic experiences) using logistic regressions. For all logistic regressions, the reference group is no endorsement of psychotic experiences (n = 1734).
Results found when comparing the individual levels of age (14, 15, 16, 17) was slightly different, where the odds ratio was non-significant (OR = 0.87, 95% CI = [0.77, 0.98]).
Cannabis or other illicit substance use in their lifetime.
Youth-reported major depressive disorder, Diagnostic Interview Schedule for Children (DISC-IV).
Binge eating/purging or low weight/problem eating group (groups devised by YMM survey team).
Adolescent Self-Esteem Questionnaire (ASQ), recoded into above (healthy) vs equal to or below cut-off of 17 (low self-esteem).
Mental health service use in past 12 months.
Social isolation composite score (0–5) included: number of friends, face-to-face contact per week with friends outside of school, online contact per week with friends/family, level of involvement in clubs, groups or activities outside of school per week, and perceived ability to rely on friends. A higher score indicated greater social isolation. Continuous scores were recoded into a binary variable: scores less than 3 versus scores 3 or above.
Although a significant U-shaped association has been reported between sleep duration and several morbidities (obesity, diabetes, cardiovascular disease; Léger et al., 2014), there was no significant association with any of the PE subtypes and excessive sleep (equal to or above 11 hours per night; Snell et al., 2007).
Multivariate regressions
Table 7 presents the factors associated with each PE subtype at the multivariate level. Factors independently associated with both auditory and visual HEs were: younger ages (14–15 years), depression, being bullied, mental health service use and insufficient sleep. The associations with DEs were less consistent: feeling spied upon and thoughts being read were the only subtypes associated with younger ages, whereas only special messages and thoughts being read were associated with depression. Feeling spied upon was the only delusional subtype associated with being bullied, psychological distress and insufficient sleep, and none were associated with mental health service use at the multivariate level.
Multivariate regression analysis of correlates of 12-month psychotic experiences, using odds ratios adjusted for each variable (n = 1998).
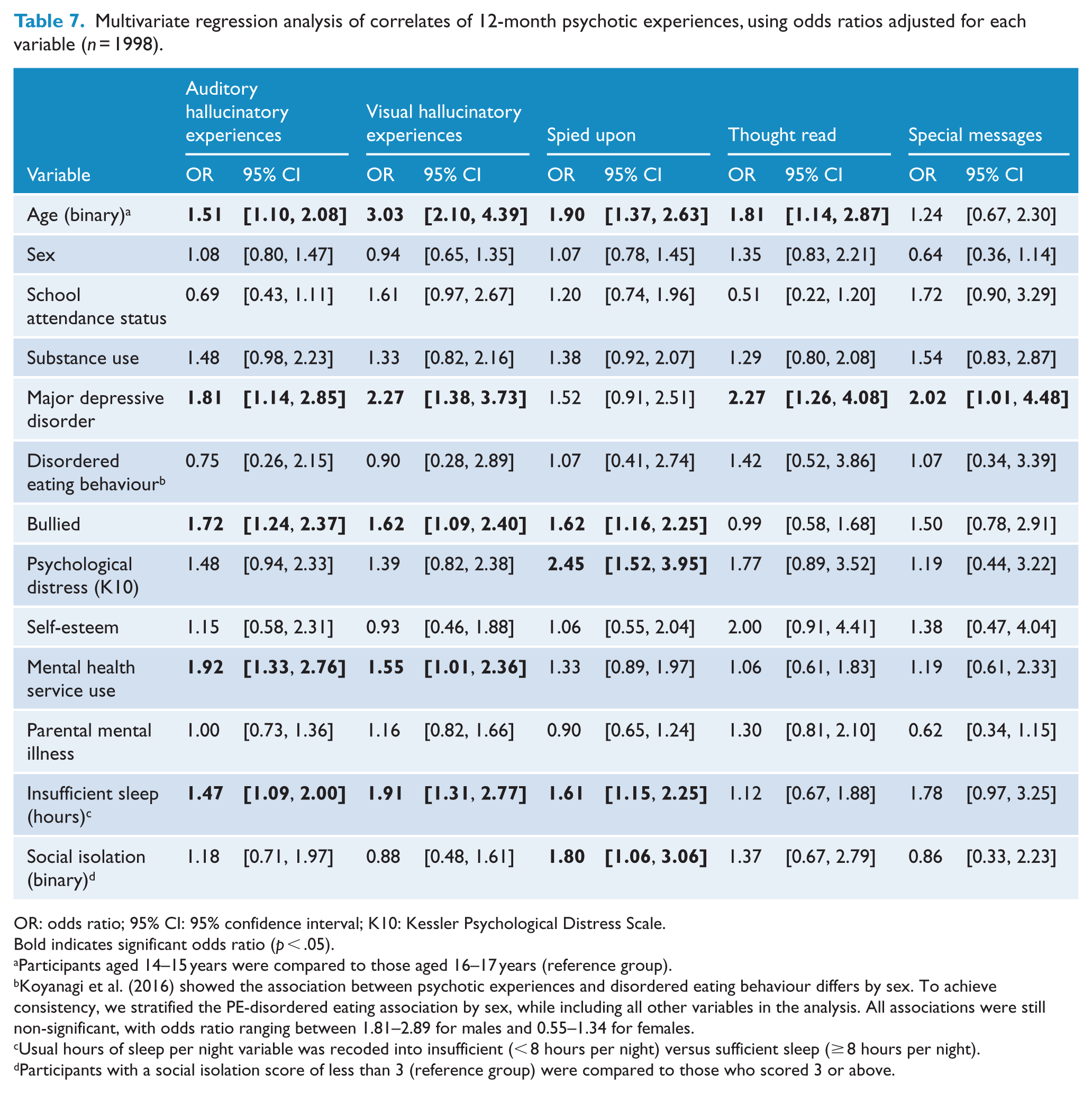
OR: odds ratio; 95% CI: 95% confidence interval; K10: Kessler Psychological Distress Scale.
Bold indicates significant odds ratio (p < .05).
Participants aged 14–15 years were compared to those aged 16–17 years (reference group).
Koyanagi et al. (2016) showed the association between psychotic experiences and disordered eating behaviour differs by sex. To achieve consistency, we stratified the PE-disordered eating association by sex, while including all other variables in the analysis. All associations were still non-significant, with odds ratio ranging between 1.81–2.89 for males and 0.55–1.34 for females.
Usual hours of sleep per night variable was recoded into insufficient (< 8 hours per night) versus sufficient sleep (
Participants with a social isolation score of less than 3 (reference group) were compared to those who scored 3 or above.
Supplementary analyses
To further our understanding of the above associations, we repeated the analyses in the subgroup of participants who reported DEs alone (i.e. without HEs). Many of the associations presented in Table 7 persisted indicating that the associations were with DEs and not with HEs, which are commonly present in those with DEs (see Supplementary Material II). Specifically, the factors associated with DEs alone at the multivariate level were as follows: younger age, being bullied, psychological distress, insufficient sleep and social isolation. In contrast, HEs alone (auditory or visual) were associated with younger age, major depression, being bullied, mental health service use, and insufficient sleep.
The focus of the paper has been the prevalence and correlates of each PE subtype (HEs, thoughts read, special messages, spied upon). To enable comparisons with previous studies, Supplementary Material (III) reports on the main results for the ‘any PE’ variable. The results were generally consistent with those already reported in this paper. At the multivariate level, any PE was associated with a range of symptoms of mental illness and adverse psychosocial factors including a twofold to fourfold increased likelihood of depression diagnosis, being bullied, psychological distress, low self-esteem, and mental health service use.
Discussion
This study reports on the prevalence and correlates of PEs in a nationally representative sample of Australian adolescents aged 14–17 years. PEs were highly prevalent, with 12 month prevalence ranging from 3.3% (95% CI = [2.6, 4.3]) for special messages to 14.0% (95% CI = [12.3, 15.8]) for auditory HEs. This is higher than reported in the first national mental health survey, where Scott et al. (2009) found 8.4% of adolescents (13–17 years) reported hallucinations which were assessed by clinicians reviewing the descriptions of the experiences provided by respondents.
Consistent with international studies (Dolphin et al., 2015; Kelleher et al., 2012), younger adolescents were more likely to endorse HEs and DEs, with the exception of special messages. The other demographic and family history variables (sex, school attendance and parental mental illness) were not associated with each PE subtype at the multivariate level. In terms of the other domains (mental disorders/problems, psychological, environmental, intervention factors), the results supported existing evidence that subtypes are differentially implicated in psychosocial functioning (Barragan et al., 2011; Dhossche et al., 2002). At the bivariate level, each subtype was associated with increased likelihood of depression, being bullied, high levels of psychological distress, low self-esteem, mental health service use, and insufficient sleep. All these associations (except for distress and low self-esteem) persisted in the multivariate model for auditory and visual HEs, but not for DEs. Feeling spied upon was the only delusional subtype associated with numerous (being bullied, high levels of psychological distress, insufficient sleep) at the multivariate level, highlighting that the presence of HEs may have more clinical relevance than DEs in adolescents.
To our knowledge, this is the first study outside of England (Koyanagi et al., 2016) to investigate the relationship between PEs and disordered eating. Unlike Koyanagi et al. (2016), we did not find a significant association between disordered eating behaviours and any type of PE; even when stratified by sex as in the previous study (Koyanagi et al., 2016) (see Table 7). This was also the first study, to our knowledge, to investigate the association between PEs and hours of sleep, as opposed to broader sleep disturbances (Lee et al., 2012; Oh et al., 2016). We showed that adolescents sleeping less than 8 hours were almost twice as likely to report HEs or DEs, compared to adolescents sleeping eight or more hours per night. This association persisted in the multivariate analysis (for HEs and feeling spied upon) and is consistent with the broader literature which has found adolescents sleeping less than 8 hours are at increased risk of a broad range of health problems (Lui, 2004; Snell et al., 2007).
Strengths and limitations
This study was nationally representative, and we were also able to report on several PE subtypes, which is valuable considering they have different underlying mechanisms and treatment implications (Bak et al., 2005; McCarthy-Jones et al., 2014). No previous Australian study has reported on the prevalence and correlates of both HEs and DEs independently in adolescents; existing Australian studies have already reported on both of these experiences when collapsed into one broad PE variable (Lin et al., 2011; Yung et al., 2009).
This study was limited by the cross-sectional self-report data, where there may be overreporting or underreporting of certain experiences compared to an interview-based survey. However, Kelleher et al. (2011) have shown some self-reported PEs, in particular auditory and visual hallucinatory DISC-C items (with similar wording but different potential responses to the current items, e.g., ‘Have you ever heard voices or sounds that no one else can hear’: yes definitely, maybe, no never), have high concurrent validity with clinician-rated symptoms in adolescents. However, a lower prevalence was reported in the first national mental health survey (8.4%; Scott et al., 2009), where the authors used a two-stage method whereby HEs were classified by clinicians to exclude those experiences of no clinical significance. This, in addition to the difference in item wording between the DISC-IV and the Youth Self-Report (e.g. ‘I hear sounds or voices that other people think aren’t there’; Achenbach, 1991), could explain the discrepancy in PE rates between the first and second national survey. International studies report higher and more comparable 12-month PE prevalence rates, ranging from 5% to 28% in adolescent community samples (Kelleher et al., 2012; van Os et al., 2009). Major depressive disorder was the only diagnosis assessed using information from the adolescents gathered by a diagnostic instrument and therefore other youth-reported diagnoses were unavailable. This included eating disorders, where symptoms of disordered eating behaviour were assessed using questions (e.g. ‘During the past 12 months, how often did you make yourself throw up (vomit) to lose weight or avoid gaining any weight?’) answered by the adolescent participants, together with their self-reported BMI (see Supplementary Material I for details). Finally, the YMM survey did not collect data on a history of childhood trauma, which has been shown to predict PE occurrence in adolescence (Kelleher et al., 2013; Norman et al., 2012).
Future research and clinical implications
Future epidemiological surveys should explore additional dimensions of psychosis that have been largely overlooked, including cognitive and negative symptoms (e.g. disorganised speech, affective flattening, avolition; Barragan et al., 2011; Bromet et al., 2017), although symptoms such as affective flattening are difficult to assess in epidemiological studies and typically require a multi-method approach (Kring et al., 1994). Barragan et al. (2011) attempted to capture a range of different negative symptom subtypes in adolescents using the Community Assessment of Psychic Experiences (CAPE), where social withdrawal and avolition were associated with depressive symptoms while affective flattening was not. In addition to a limited PE scope, many epidemiological surveys (including the current one) cannot distinguish between a single fleeting episode and recurrent PEs, and so future studies should continue to further investigate the frequency and predictors of persistence versus remission of PEs (DeVylder et al., 2015), as there is growing evidence that frequent PEs which persist over time are more specific predictors for psychotic disorders (Dominguez et al., 2011; Poulton et al., 2000), as well as other clinical or functional impairments later in life, including increased levels of depressed mood, self-harm, and general psychopathology (Connell et al., 2016; De Loore et al., 2011).
The current study demonstrated that PEs are common in Australian adolescents, and that HEs have the greatest clinical relevance in this demographic. However, it is important to recognise that epidemiological surveys generally capture dichotomous assessments of PEs without precise characterisation of the phenomenological quality of the experience. Stanghellini et al. (2012) reported on the qualitative attributes of experiences in a clinical (23 patients with schizophrenia) and non-clinical sample (n = 60 Spanish university students). In the clinical sample, hallucinations were intimately related to the person’s identity and disrupted self-world relationship, whereas experiences in the non-clinical group were related to a circumstantial event (e.g. mourning) or were reported as an isolated phenomenon. It is likely that in the YMM survey, and in other epidemiological surveys, the endorsement of HEs and DEs captures a broad construct inclusive of true hallucinations and delusions but also responses that misinterpret the phenomenological dimensions being sought. For example, an adolescent who has reasonable concerns about privacy in school or online might report feeling spied upon with the accompanying mislabelling of these individuals.
Even though these concerns about diagnostic mislabelling are warranted, this broader and heterogeneous PE construct is clinically relevant in this demographic. van der Steen et al. (2018) explored PEs endorsed on the Composite International Diagnostic Interview (CIDI) survey that could not be confirmed by clinical interview (i.e. false-positive PEs). The authors found that these experiences were not truly ‘false’ as they indexed risk for the development of clinically relevant psychotic symptoms, development of mood/anxiety disorders, and overall reduced functioning over time. Self-reported PEs, even unconfirmed, warrant monitoring and follow-up (van der Steen et al., 2018) but also further clinical assessment of the experience beyond determining their presence or absence (Kendler, 2008). As recommended by Kendler (2008), initial screening for hallucinatory or delusional symptoms should be followed-up by clinicians with a detailed phenomenological analysis of these young people’s experiences to fully understand their context, clinical significance and, if necessary, appropriate treatment options.
Conclusion
This study found that HEs and DEs are common in adolescents and those who endorse these experiences are more likely to report behavioural/emotional problems (major depression, insufficient sleep), stressful life experiences (being bullied), and recent mental health service use, compared to those without PEs. Furthermore, this study showed variation in clinical relevance with the different types of PEs, whereby HEs were associated with an increased likelihood of depression, being bullied, mental health service use, and insufficient sleep at the multivariate level, whereas these associations with DEs were inconsistent. Overall, this study highlights the importance of screening adolescents for HEs, which have been consistently shown to be associated with an increased risk of current and future mental health and psychosocial problems in adolescents.
Supplemental Material
Supplementary_Material_III_30June2018 – Supplemental material for Prevalence and correlates of psychotic experiences in a nationally representative sample of Australian adolescents
Supplemental material, Supplementary_Material_III_30June2018 for Prevalence and correlates of psychotic experiences in a nationally representative sample of Australian adolescents by Emily Hielscher, Melissa Connell, David Lawrence, Stephen R Zubrick, Jennifer Hafekost and James G Scott in Australian & New Zealand Journal of Psychiatry
Supplemental Material
Supplementary_Material_II_30June2018 – Supplemental material for Prevalence and correlates of psychotic experiences in a nationally representative sample of Australian adolescents
Supplemental material, Supplementary_Material_II_30June2018 for Prevalence and correlates of psychotic experiences in a nationally representative sample of Australian adolescents by Emily Hielscher, Melissa Connell, David Lawrence, Stephen R Zubrick, Jennifer Hafekost and James G Scott in Australian & New Zealand Journal of Psychiatry
Supplemental Material
Supplementary_Material_I_30June2018 – Supplemental material for Prevalence and correlates of psychotic experiences in a nationally representative sample of Australian adolescents
Supplemental material, Supplementary_Material_I_30June2018 for Prevalence and correlates of psychotic experiences in a nationally representative sample of Australian adolescents by Emily Hielscher, Melissa Connell, David Lawrence, Stephen R Zubrick, Jennifer Hafekost and James G Scott in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
The authors wish to express their gratitude to the 6310 families who participated in the survey.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The second Australian Child and Adolescent Survey of Mental Health and Wellbeing was funded by the Australian Government Department of Health. Emily Hielscher is supported by the Dr F and Mrs ME Zaccari Scholarship, Australia. Associate Professor James Scott is supported by a National Health and Medical Research Council Practitioner Fellowship Grant (grant number 1105807). Professor Stephen Zubrick is supported by a Centre of Excellence grant from the Australian Research Council (CE140100027).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.