
Abstract
Homeless individuals move in and out of homelessness and between various homeless settings [1]. The homeless population on any one night in Australia is about 100 000 [2]. The number of individuals moving through homeless settings in 1 year is many times greater. The importance of elucidating these movements or ‘temporal patterns’ has been clearly articulated: ‘Only when we understand the dynamics of exits and re-entries into homelessness will we be able to successfully intervene and prevent recurrences’ [3]. This is especially true for homeless persons with mental illness where duration, stability and mobility have direct relevance to the level of disability, engagement with services and effective treatment.
It is not easy to maintain contact with homeless persons over time, making longitudinal studies difficult. Retrospective accommodation histories, although limited by the accuracy of recall, are the most practical way of collecting information on the temporal patterns of accommodation use. Chamberlain [4] found that 30–40% of a population of youth homeless were homeless for less 2 weeks, and 15–25% for more than a year. The 2001 Australian census, using data on persons staying in Supported Accommodation Assistance Program (SAAP) facilities, estimated that 60–70% of homeless persons remain so for at least 6 months [2]. The census was unable to provide any temporal data on shelterless persons, people using private boarding houses or staying temporarily with friends.
Research into the patterns of accommodation use in homeless people with mental illness is not well developed. Early descriptive studies, such as that by Fischer and Breakey [5] defined subgroups of the ‘situationally homeless’ and the ‘chronically mentally ill street people’, the former being seen as entering the homeless sector for a short time after a change in circumstances and the latter being long-term homeless. Arce [6] interviewed patients attending an adult emergency shelter for 2 months and categorized them into three groups with increasing durations of homelessness: those in acute crisis, episodic homeless and habitual street people. In his cohort, age, past psychiatric hospitalization, prevalence of psychotic symptoms, and need for treatment all increased with the duration of homelessness.
Persons with psychosis make up between 18% and 29% of the homeless population [7], [8]. Managing homeless persons with mental illness repeatedly reinforces the importance of accommodation type, mobility and stability in determining outcome. Despite this observation, no research had been conducted on the patterns of accommodation use in patients with mental illness and how these relate to management outcome. Our aim was to study the relationship between pattern of accommodation use in patients with psychosis managed by an inner city mental health service and its relationship with management outcome. We expected that a history of accommodation instability and mobility or a history of homelessness would be associated with decreased length of engagement with mental health services and discontinuity of care at discharge.
Method
Setting
The study was conducted in the Inner West Area Mental Health Service (IWAMHS). The IWAMHS is a public psychiatric service covering the central business district and inner northern suburbs of Melbourne, Australia, comprising a population of approximately 173 000 persons [9]. The service includes a continuing care team, a crisis assessment team, a mobile support team, a homeless team and an inpatient unit.
Sample and data collection
The study population included all patients with psychosis accepted to the IWAMHS for case management during the 2001 calendar year. Referrals were received from other area mental heath services, primary care settings, homeless services, or following crisis assessment and were accepted for case management if the patient was resident in the catchment area and not adequately engaged and managed by primary care or private psychiatric services. Patients were eligible for entry to the study if they were aged 18 or greater, had adequate English language skills, were able to give consent and had a primary diagnosis of a psychotic illness. Data was collected during the initial psychiatric assessment, with use of the patient record and collateral history. Discharge information was collected at the end of the 2003 by reference to the patient's record and an electronic database of mental health service patient contacts.
Measures
The psychiatric diagnosis was reached after clinical assessment by a psychiatry trainee or consultant psychiatrist using the DSM-V categorical system [10]. Data was collected for each accommodation used during the 12 months prior to assessment, and included the type of accommodation, the duration it was used, and its geographical location. This data was used to place the patient in categories of homelessness (type, chronicity) and provide measures of accommodation mobility and stability.
The categories of accommodation type recorded incorporated the system of primary, secondary and tertiary homelessness used in the Australian Census [1] and mapped to those used in the low prevalence component of the National Study of Mental Health and Wellbeing [11]. Primary homelessness included sleeping shelterless, in a car or in a ‘squat’. Secondary homelessness described people using emergency accommodation, temporarily staying with friends or relatives. Tertiary homelessness referred to the use of boarding houses, caravans, motels or rooming houses. The categories for chronicity were determined in reference to previous literature [4], [6], [12]. They were based on the total time spent in homeless settings, which may have involved one or more discontinuous episodes. Short-term homelessness was defined as up to 2 months, long-term homelessness as more than 2 but less than 12 months and chronic homelessness as more than 12 months. Mobility was calculated by summing the time spent in each geographical category. The categories available were inner urban, outer urban, rural, interstate and international and defined in reference to the location at the time of assessment. For example, time spent interstate in a rural setting was recorded as interstate. Stability was measured by counting the number of different accommodations used in the 12-month period.
Discharge information was collected for all patients as of 31 December 2003. The date of discharge, reason for discharge, continuity with psychiatric follow up, the type of follow-up psychiatric service and discharge to primary care was recorded for patients discharged from the service. For those patients still managed by the IWAMHS their length of contact was calculated to the discharge assessment date and they were assumed to have maintained continuity of care with a public psychiatric service. Continuity was seen to have occurred when there was a planned transfer of care to an appropriate follow up service which had engaged and accepted the patient.
Analysis
Patient accommodation information was entered into a spreadsheet. The sum of days in each type of accommodation and geographical location was calculated for each patient. The time spent shelterless, in emergency accommodation and single room accommodation was summed and used to place the patient in temporal categories of non-homeless, short-term homeless, long-term homeless or chronic homeless.
Statistical analysis was conducted using the SPSS statistical package [13]. Chi squared analysis was used to determine the categorical differences between homeless groups. A two tailed t-test was used to determine differences in parametric measures between homeless and non-homeless populations and ANOVA for parametric measures between the four categories of homelessness. A Pearson correlation was used to determine the relationship between duration of homelessness and duration of engagement.
Results
Study population
There were 198 new patients with a primary diagnosis of psychosis taken on for management by the IWAMHS during the study period. One hundred 43 of these patients were recruited. The sample comprised 99 males, mean age 35.4 years, and 44 females mean age of 45.3 years. Ninety four patients were recruited from the continuing care team and 49 patients through the homeless team. There was no statistical difference between recruited and non-recruited patients in terms of age or gender.
Diagnoses
One hundred and five patients had a diagnosis of schizophrenia; 19 had schizoaffective disorder, 16 had bipolar disorder with manic illness and three delusional disorder. Bipolar illness was present in only three patients with a history of homelessness, which was significantly less than those without a history of homelessness (p = 0.018).
Homelessness
Fifty-six patients (39%) were homeless at the time of assessment. Seventy patients (49%) had spent at least 1 day in a homeless setting during the 12 months prior to assessment. Of patients with a history of homelessness, 41% had short-term homelessness (less than 2 months), 46% had long-term homelessness (more than 2 but less than 12 months) and 13% chronic homelessness (greater than 12). Looking at the population as whole, 23 percent of the previous 12 months had been spent in a homeless setting.
Accommodation type
The percentage of time spent in each accommodation type used during 12 months prior to assessment, stratified by category of homelessness, is summarized in Fig. 1. Subjects with a history of homelessness spent significantly more days on average shelterless (40.7 vs 0, p = 0.000), in crisis accommodation (31.9 vs 0, p = 0.000), single room accommodation (58.3 vs 0, p = 0.000), hostels (53.7 vs 18.3, p = 0.019) and as a psychiatric inpatient (9.5 vs 2.2, p = 0.000).
Percentage of time spent in each type of accommodation over previous 12 months, according to category of homelessness (n = 143)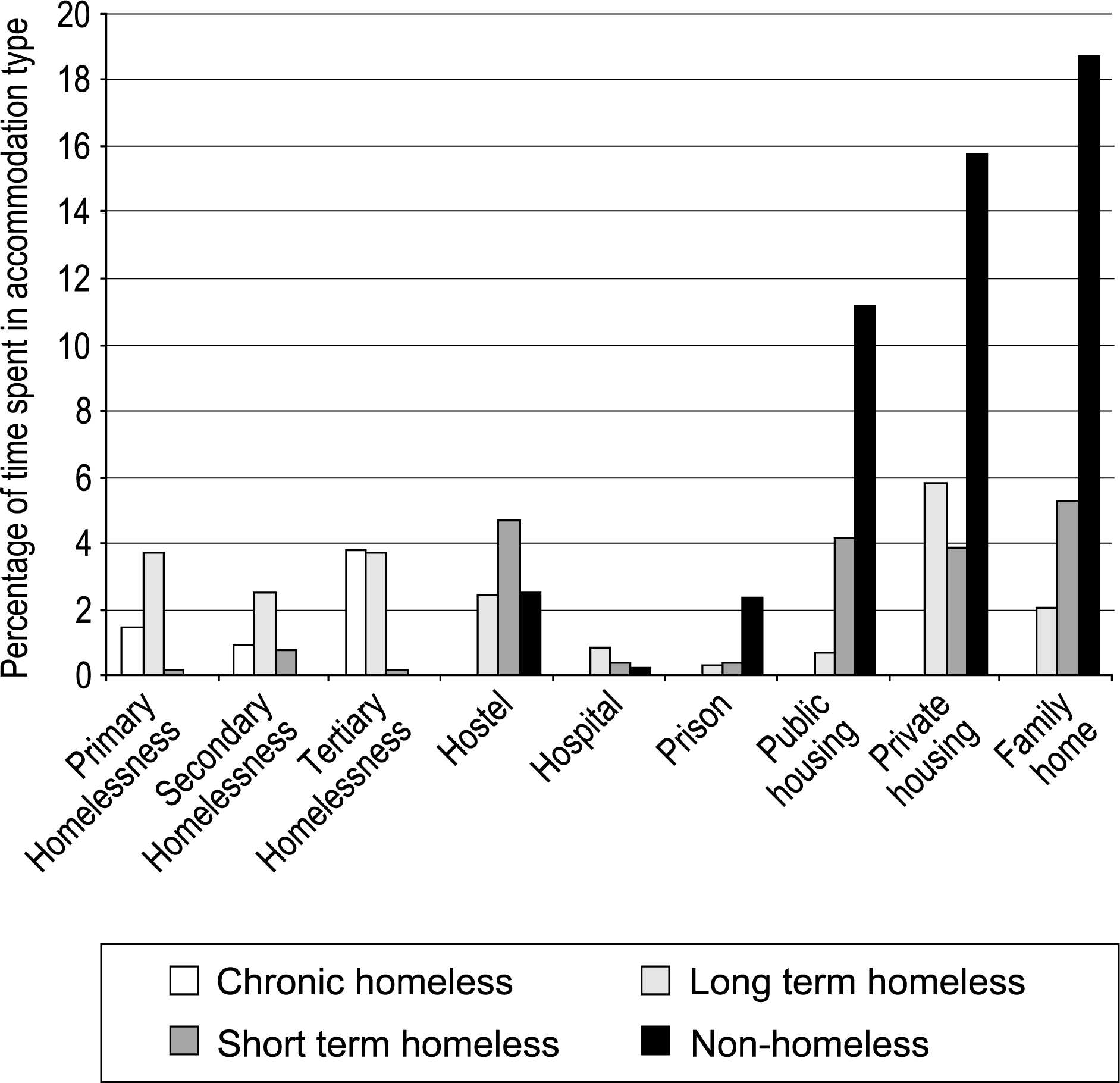
Accommodation stability
The population as a whole had on average 2.8 accommodation settings in the past year. Subjects with a history of homelessness had a significantly greater mean number of accommodations (4.1 vs 1.8, p = 0.000) than those without a history of homelessness. The number of accommodations was lowest for the-non-homeless (mean = 1.8) and highest for the long-term homeless (mean = 4.5), with short-term and chronic having on average 3.8 and 3.6 episodes of accommodation per year, respectively. Stability was not significantly different between temporal categories of homelessness.
Accommodation mobility
Subjects with a history of homelessness spent significantly more days on average in rural areas (24.6 vs 0, p = 0.016) and interstate (81.3 vs 4.9, p = 0.000), and significantly less days in outer urban settings (88.8 vs 151.9, p = 0.016) during previous 12 months.
Discharge outcome
Patients with a history of homelessness had a shorter duration of engagement with the service as compared with patients with no history of homelessness (385 days vs 535 days, p = 0.016). The duration of contact with the service was inversely correlated with the duration of homelessness in the past 12 months (r = −0.292, p = 0.001). This association was replicated in the temporal categories, where in the duration of engagement decreased between short-term, long-term and chronic homeless groups. The duration of contact was also inversely correlated with time in the inner urban (r = −0.31, p = 0.001) and interstate settings (r = −0.37, p = 0.001) and with stability (r = 0.188, p = −0.037).
Patients with a history of homelessness were more likely to experience a discontinuity of care at discharge (29% vs 10%, p < 0.01). Interstate mobility was higher in those patients with discontinuity at discharge (Mean days interstate = 126 vs 16, p < 0.01). Homeless patients were more likely to be discharged to a public psychiatric service than patients without a history of homelessness (74% vs 57%, p < 0.05) and less likely to be discharged to primary care (17% vs 38%, p < 0.05).
Discussion
This study describes the association between accommodation history in patients with psychosis and treatment outcome. The findings support long articulated notions about the relationship between homelessness, accommodation instability, mobility and difficulty maintaining continuity of care. The study also provides an insight into the dynamic nature of homelessness and provides baseline information about accommodation type, mobility and stability in patients with psychosis accessing in inner city public mental health service.
The outcome of an episode of care with the mental health service was significantly affected by the pattern of accommodation use during the previous 12 months. The length of homelessness inversely predicted the duration of contact with the service. This was not an unexpected finding given the relationship between homelessness and accommodation instability. There was also a higher incidence of discontinuity of care and a decreased likelihood of discharge to primary care in patients with a history of homelessness. This finding has significance for the longterm management of these patients suggesting that they are at risk of becoming stuck in cycles of engagement and disengagement within the public psychiatric system.
There was significant accommodation instability in patients with psychosis. Movement occurred in and out of homelessness. Patients with a history of homelessness only spent 36% of the previous year in homeless settings. The remainder of the time was spent in the full range of accommodation types, including rental properties and the family home. Movement also occurred between different homelessness settings. This movement presents both a challenge and an opportunity for mental health services. On one hand regular changes of accommodation makes engagement and follow up more difficult. On the other hand movement through crisis accommodation services provides an opportunity for detection and referral.
Shelterlessness is the most severe end of the homeless spectrum. Shelterlessness is associated with poor access to community supports [14] and an increased risk of physical ill health and nonaccidental injury [15]. In our sample, 5% of the time in the past 12 months was spent shelterless. This figure is 250 times higher than the point prevalence of shelterlessness in the general population of inner urban Melbourne, measured at 0.02% [2]. Our figures equate to eight patients having spent an entire year on the streets, or approximately 25% of the shelterless population. In fact 26 different patients had had an episode of shelterlessness in the year prior to assessment. This finding goes against the notion that shelterless persons with psychosis are ‘street people’, at least in inner urban Melbourne. Rather, patients spend a variable time on the streets, from a few days to many months.
Homeless persons in the study group were more mobile when compared with the non-homeless group. Twenty-nine percent of patients with a history of homelessness had been interstate in the previous 12 months. Time spent interstate correlates strongly with discontinuity at discharge. None of the patients with a history of interstate travel were discharged to primary care. Clinical experience of working with homeless patients is that interstate travel often occurs with little planning. Travel may be as a part of a long standing pattern, in response to a breakdown in accommodation or an attempt to avoid psychiatric services. Currently management of these patients occurs in an ad hoc manner. There may be a role for a more co-ordinated national approach to this group of high mobility patients involving the identification of a centralized point of contact for interstate services seeking patient information and the flagging of high mobility patients.
The strength of this study relates to the use of an accommodation history to provide measures of accommodation use, mobility and stability over time and its application to a patient population moving through an inner city mental health service. The calculation of these parameters required the novel use of spreadsheet, database and statistical software which once developed has been easy to apply to new populations. The use of a dynamic population allowed for a greater representation of patients with unstable accommodation histories and a history of homelessness providing enough power for the analysis of the relationships between these parameters and discharge outcomes.
The study may be criticised with regards to the population used. The study was not a cross sectional prevalence survey. A cross sectional survey would have included a greater representation of stable long-term clinic patients, and fewer patients with a history of homelessness. At any one time the service population as a whole will be more stable, less mobile and more adequately housed than the population that is moving through the service. Certain patients were not included in the study, including patients managed in primary care, private psychiatry or not engaged with services.
The measures used in the study are open to challenge. The reliability of a 12 month accommodation history in patients with psychosis is not known. Those patients who gave an inconsistent or unconvincing history were excluded, but the details of the history are unlikely to be fully accurate, especially in cases with significant accommodation instability. The psychiatric diagnosis was based on clinical assessment, rather than by semistructured interview. Finally, the outcome measures related to service use rather than symptoms levels or measures of disability.
Conclusion
Patients managed by the IWAMHS have a wide range of accommodation profiles. Some experience of homelessness is common and is a predictor of future management discontinuity. The homeless are not nearly as ‘hidden’ as is presumed. Furthermore, the notion of a ‘homeless population’ as a stable disparate group of individuals is inaccurate and may inhibit service development. For mental health services to best engage and manage patients with psychosis they need have knowledge of their patient's temporal patterns of accommodation and be aware that homelessness adversely affects management outcome.