
Abstract
Psychiatrists tend to neglect tobacco smoking and nicotine dependence in their patients [1]. Similarly, psychiatric researchers tend to ignore the confounding effects of smoking and nicotine dependence in their research [2]. However, all over the world there is now a well documented association between nicotine dependence and psychiatric disorders. This association has been better studied in the US, where a recent survey [3] found that psychiatric patients smoke half of the cigarettes marketed in the US. Furthermore, heavy smoking prevalence increases with the number of lifetime psychiatric diagnoses [3]. Currently, the US general population includes an overrepresentation of smokers who cannot quit because of a high dependence level [1], [4]. Several psychiatric studies pointed out the association between tobacco smoking and mental illness. Hughes et al.'s classic study described that tobacco smoking was more frequent in psychiatric patients than in the general population [5]. The association of depression with increased current smoking and decreased smoking cessation has been known for years [6–9]. Bipolar disorder increased the risk of being an ever and current smoker when compared with the general population [10], [11]. Smoking frequency is even higher in schizophrenia than in mood disorders [10], [12]. Moreover, heavy smoking may be particularly prevalent in schizophrenia [13–15]. By combining results from eight studies in several countries, estimated odds for a patient with schizophrenia to be a current smoker were two times higher than the odds for a patient with other severe mental illness [15]. Alcohol and drug addiction are also associated with smoking [16]. The association between smoking and severe mental illnesses may partially explain the increase in several medical conditions [17] including coronary heart disease [18] seen in patients with severe mental illnesses. Moreover, tobacco smoking clearly appears to contribute to the increased mortality seen in schizophrenia [19].
Therefore, it is important to perform a routine nicotine dependence screening in psychiatric patients [16]. DSM-III-R defined nicotine dependence was found to be associated with depression in several studies [20], [21]. Unfortunately, DSM definitions of nicotine dependence are relatively complex and their applications demand substantial clinician and patient time.
The most widely used tool for nicotine dependence diagnosis and quantification is the Fagerström Test for Nicotine Dependence (FTND) [22]. One of the stronger arguments used to support its validity is that the FTND has been found to predict smoking cessation success [22], [23]. Breslau and Johnson [24] described that the FTND nicotine dependence definition is more practical in depressive patients since it appears to relate to cessation probability while the DSM-III-R definition may be more related to dependence trait and depressive symptom severity. The FTND has six items with a total score range of 0–10 [22]. The two items which may reflect nicotine dependence best [23] are Item 1, which assesses the time to the first cigarette of the day, and Item 4, which assesses the number of cigarettes smoked per day. Both items are scored from 0 to 3. The FTND is the most widely used nicotine dependence measure despite some psychometric problems including weakness of some items, lack of comprehensiveness and unstability of results in factor analysis studies [23],[25–27]. A total score of 6 or higher defines high nicotine dependence [28]. Using this definition in a comparative study, we found that severely mentally ill patients (with schizophrenia and mood disorders) in the US and Spain had similar high nicotine dependence frequencies [29]. Moreover, patients had consistently higher high nicotine dependence frequencies than controls in both countries. This suggests consistency and clinical relevance of the cut-off score of 6 as a point separating non-highly from highly nicotine dependent patients. Ideally, all psychiatrists should use the FTND to assess nicotine dependence level (at least, during the first interview with a smoker patient) and explore with him/her the possibility and interest in quitting smoking. Although the FTND is relatively brief, its completion requires a few minutes. This time may be too much for busy clinicians who need to assess multiple other psychiatric and medical issues. Thus, finding a shorter way than the FTND to screen for nicotine dependence would be beneficial.
A shorter definition of high nicotine dependence is also needed for large epidemiological surveys. In the past, most health surveys have focused on tobacco smoking prevalence. However, the epidemiological focus is changing from tobacco smoking to nicotine dependence [1], [4]. In the past, attempts to establish nicotine dependence measures were limited to heavy smoking, which is usually defined as consuming more than 30 cigarettes per day. Heavy smoking is considered a brief but gross indicator of high nicotine dependence. Ideally, the FTND can be used in some surveys but six questions may be too lengthy for surveys including hundreds of other questions. Certainly, these epidemiological surveys require briefer nicotine dependence measures. One that seems to be better than just recording the daily number of cigarettes is the Heavy Smoking Index (HSI) [30]. The HSI is the sum of the scores of FTND Items 1 and 4 and scores from 0 to 6. When we studied FTND scores from 1462 smokers from US and Spain [31], we found that a score of four or higher in the HSI had a relatively good sensitivity (94%) and specificity (88%) to detect high nicotine dependence (defined as an FTND score (6) in severely mentally ill patients and controls. Some questions remain after this study in a relatively large number of psychiatric and non-psychiatric patients. Comparing the HSI to Item 1 or Item 4, is the HSI significantly more effective to screen for high nicotine dependence? Is the HSI cut-off score of 4 optimal? Does the cut-off score of 4 work well in clinically important subgroups such as male and female?
Throughout the article, high nicotine dependence is defined as a score of 6 or higher in the FTND total score [28]. A score of 4 or higher in the HSI will be termed a ‘High HSI’ score [31]. This binary index will be compared with the three following indexes previously used in the literature [32], [33]: A score of 2 or higher [33] in the time to the first cigarette of the day (measured by FTND Item 1), which will be termed ‘Very Early Smoking’. A score of 3 in the number of cigarettes smoked per day (measured by Item 4), which will be termed ‘Heavy Smoking’. A score of 2 or higher in Item 1 or Item 4 [32], which will be termed a ‘High in Either Item’.
The goals of this study were: (i) To compare the effectiveness of the HSI with the effectiveness of Items 1 and 4 alone for the screening of high nicotine dependence; (ii) to investigate the optimality of 4 as a cut-off score for the HSI so that the HSI can be used as a binary indicator of high nicotine dependence; and (iii) to compare the sensitivity and specificity of four binary indexes of high nicotine dependence, namely ‘High HSI’, ‘Very Early Smoking’, ‘Heavy Smoking’ and ‘High in Either Item’. Comparisons were made by controlling for gender, age of onset of regularly smoking and educational background, since these variables were found to influence high nicotine dependence in a previous US study [10] and in a preliminary analysis of the data used in the current study.
Method
Sample
This study analysed FTND scores from 819 current daily smokers who were interviewed in a general population survey conducted in Catalonia, Spain [34]. The survey included a total of 3000 subjects aged 15 years or over from 8 catchment areas in this region. All subjects signed a consent form before interview. A multistage procedure was used to select and survey 66 towns. Within catchment areas, towns were selected according to probabilities proportional to population sizes. Sample sizes for catchment areas were not proportional to population sizes; therefore, statistical analyses were corrected (when appropriate) by assigning to each subject weighting coefficients as functions of catchment areas. Therefore, the smokers sample combines 8 subsamples, each of them being a representative sample of the smokers of a catchment area. As in a prior study [31], an FTND score ≥6 was considered the reference or ‘gold standard’ test for diagnosing individuals as highly nicotine dependent. Statistical analyses were performed without stratification by catchment area, since there were no significant differences in FTND scores (F = 1.5, df = 7, 811, p = 0.2) or high nicotine dependence (FTND ≥ 6) across catchment areas (χ2 = 7.3, df = 7, p = 0.4).
Statistics
Unfortunately, the statistical procedures to achieve the three goals are relatively complex. A Receiver-Operating Characteristic (ROC) analysis was performed [35]. A short description follows for clinicians unfamiliar with this methodology. A good introduction to the concepts of sensitivity (true-positive rate), specificity (true-negative rate) and ROC curves can be found in two brief articles [36], [37]. In this study's context, the sensitivity of a binary index of high nicotine dependence is the probability that a smoker with high nicotine dependence (FTND ≥ 6) be correctly diagnosed by the index. On the other hand, the specificity of the index is the probability that a smoker without high nicotine dependence be correctly diagnosed. For a particular ordinal scale such as the HSI (or the FTND item 1 or 4), each possible cut-off score yields a sensitivity and specificity value. A ROC curve is a plot of sensitivity against (1-specificity), where each point of the plot corresponds to a possible cut-off score. The area under the ROC curve (AUC) measures the potential of the ordinal scale for detecting high nicotine dependence with accuracy. In fact, the AUC measures the probability that a highly dependent smoker will score higher than a non-highly dependent smoker in that scale [35]; thus, the greater the AUC, the higher the likelihood of distinguishing between a highly and a non-highly dependent smoker when using the scale.
Since increasing values of the HSI were associated with high nicotine dependence (FTND ≥ 6), lower cut-off scores were associated with higher sensitivity but lower specificity. Similarly, higher cut-off scores yielded higher specificity but lower sensitivity. Correct diagnosis of every smoker who is highly nicotine dependent must use a cut-off of 0 for the HSI, which ensures a sensitivity of 1. However, such a cut-off score would yield a specificity of 0, which is very unreasonable because all smokers without high nicotine dependence would be incorrectly diagnosed. Therefore, two approaches trading off sensitivity against specificity were used in order to find an optimal cut-off score for the HSI. In the first approach, HSI sensitivity and specificity were plotted together as functions of the cut-off score (35]. In the second approach, a kappa statistic is computed for each possible cut-off score [35], [38]. For a particular cutoff score, the kappa statistic measured the agreement between the corresponding binary index of high nicotine dependence and the ‘true’ diagnosis based on the FTND. A kappa value close to 1 meant nearperfect agreement, while a kappa value close to 0 indicated that the agreement was no greater than would be expected by chance [38]. The optimal cut-off score corresponded to the highest kappa [35].
Plot of the diagnostic sensitivity and specificity of the Heavy Smoking Index (HSI) as a function of the cut-off score. Optimal cut-off corresponds to intersection of curves. According to the plot, a cut-off score of 4 is optimal to define a binary index of high nicotine dependence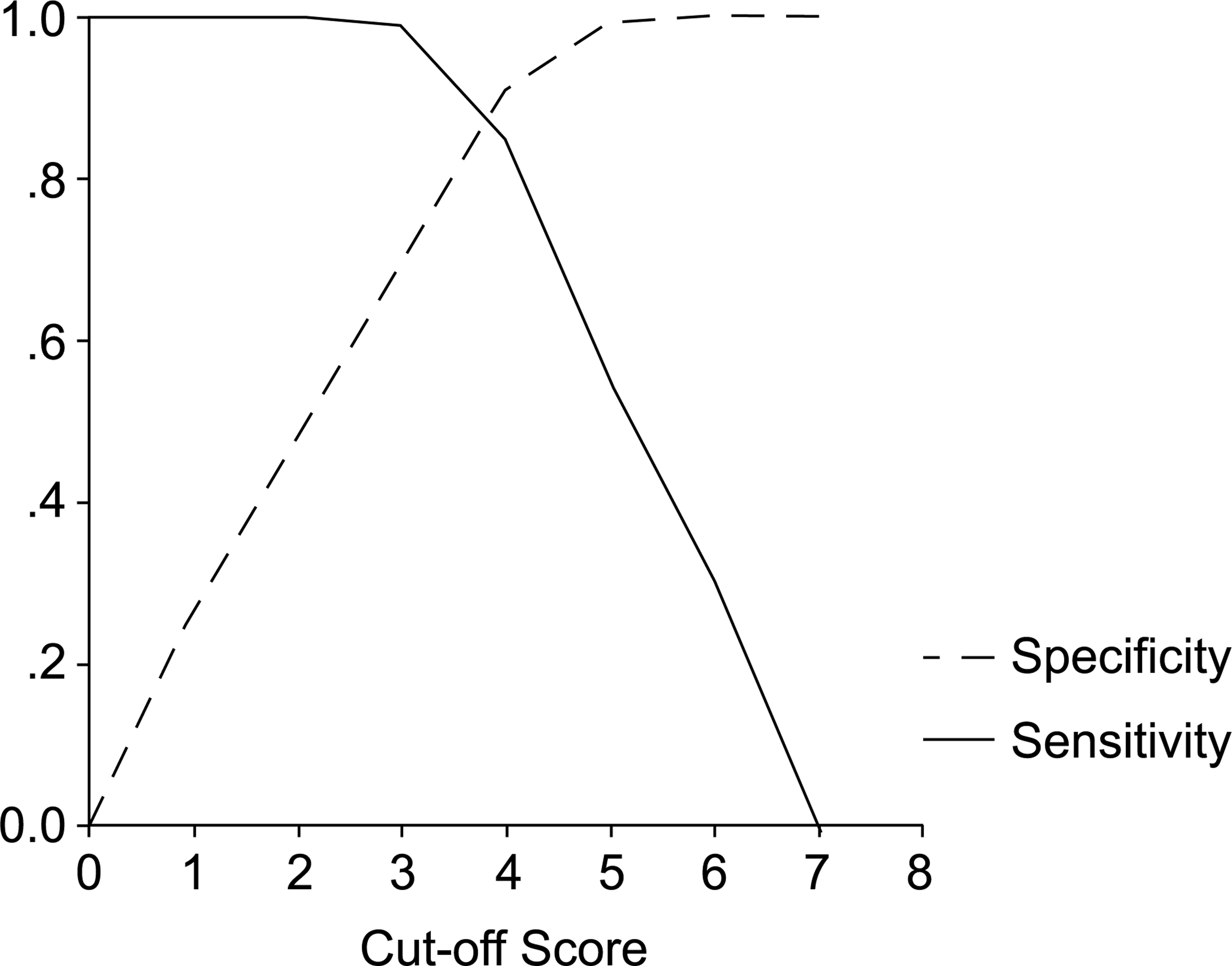
For the first goal, to examine whether the HSI is significantly more effective for detecting high nicotine dependence than each of the simpler scales Items 1 and 4, ROC curves and their corresponding AUCs were calculated for the HSI, Item 1 and Item 4. Differences between two AUCs were tested using a bootstrap procedure [39]. ROC analyses were performed using SPSS [40]. The bootstrap procedure was implemented using SAS/IML [41]. 95% confidence intervals (CIs) were computed for the AUCs.
After achieving the first goal of establishing that the HSI performs better than the individual FTND Items 1 and 4, the optimal cut-off score for the HSI was explored for the second goal using the two above approaches (31] studied the sensitivities and specificities of the ‘High HSI’, ‘Very Early Smoking’ and ‘Heavy Smoking’ indexes in different psychiatric and non-psychiatric samples. This new study used a more focused and detailed approach to compare sensitivities and specificities in specific subpopulations of our new, large representative sample of the general population. Age of onset of regularly smoking was split into three categories: Age of onset of regularly smoking ≤ 15 years, age of onset of regularly smoking < 15 but ≤18, and age of onset of regularly smoking < 18. High educational background was defined as a college degree or higher in the head of family. Sensitivity and specificity comparisons of the four brief high nicotine dependence indexes were performed for each of the 6 possible combinations of gender and onset age of regularly smoking (2 genders × 3 categories of onset age of regularly smoking = 6 combinations) and for each of the 4 possible combinations of gender and educational background (2 genders × 2 educational backgrounds = 4 combinations) (31], except that the current study controlled for gender, onset age of regularly smoking and educational background.
Sensitivities (specificities) for four brief indexes of high nicotine dependence by gender and age of onset of regularly smoking. The reference test was a score of 6 or higher in the FTND
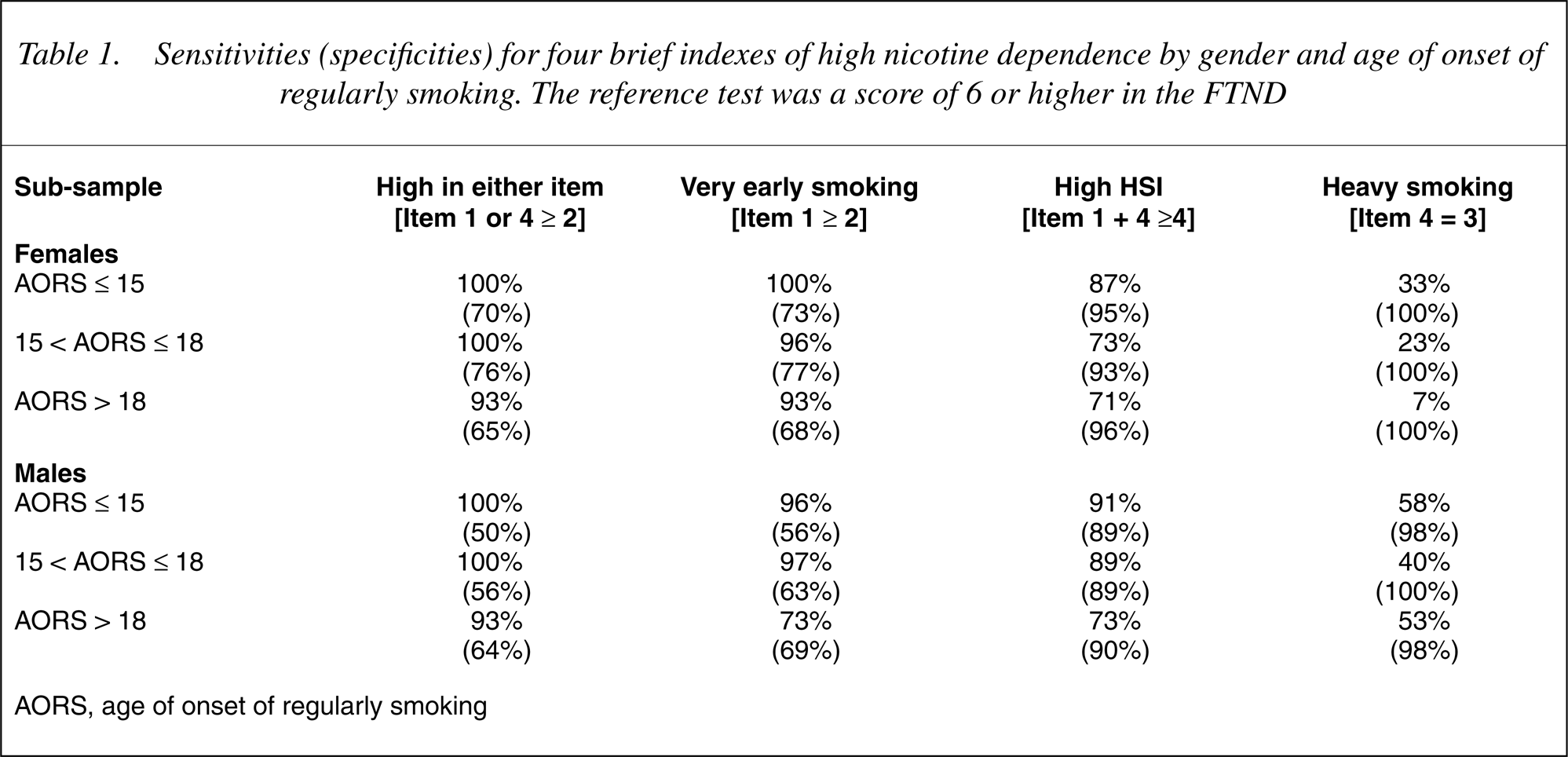
AORS, age of onset of regularly smoking
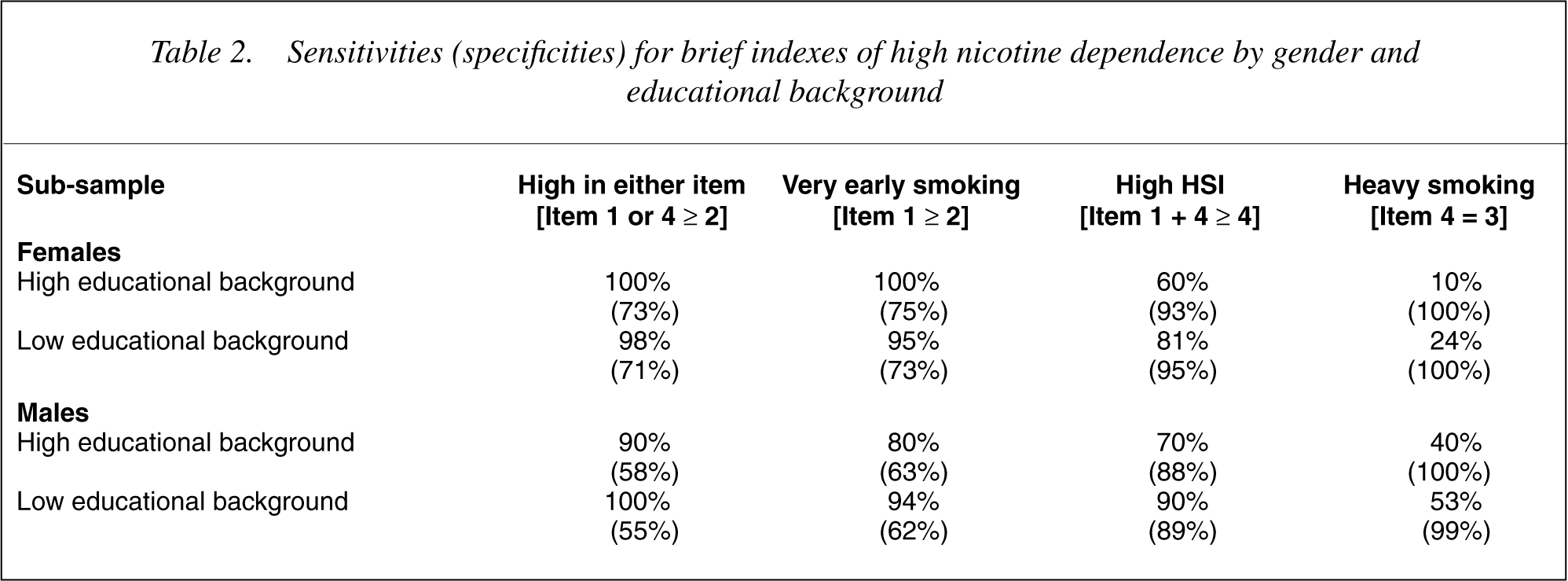
Sensitivities (specificities) for brief indexes of high nicotine dependence by gender and educational background
Results
Comparison of effectiveness of HSI, Items 1 and 4
When using the total sample, the AUC for the HSI was 0.95 (CI = 0.94–0.97), for Item 1 was 0.89 (CI = 0.86–0.91), and for Item 4 was 0.88 (CI = 0.86–0.91). Therefore, the AUC for the HSI was significantly greater than the AUCs for Item 1 (p < 0.05) and Item 4 (p < 0.05). Furthermore, for all the subsamples determined by the combinations of gender and age of onset of regularly smoking, and gender and educational background, the AUCs for HSI were always higher. Thus, the HSI scale was significantly more effective for the detection of high nicotine dependence than Item 1 or Item 4 alone.
Optimality of 4 as a cut-off score for the HSI
HSI scores range from 0 to 6. Therefore, there are five possible cutoff scores for the HSI that could be used to define a binary index of high nicotine dependence (1–5). Among these possible scores, a score of 4 was optimal according to the plot of specificity and sensitivity together as functions of cut-off scores (Fig. 1). Thus, a score of four or higher is the best indicator of high nicotine dependence based on the HSI. The kappa statistics also suggested that 4 was optimal. The optimal cut-off score, 4, corresponded to the maximum kappa, 0.71.
Comparison of sensitivities and specificities of brief indexes
Table 1 shows sensitivities and specificities for the four brief, binary indexes of high nicotine dependence by gender and age of onset of regularly smoking. In Table 1, it is apparent that sensitivities tend to decrease from left to right within all six subsamples. Similarly, specificities increase from left to right. Similar patterns are observed in Table 2, where comparisons are made within the four combinations of gender and level of education.
Tables 1–3 show that among the four brief indexes, ‘High in Either Item’ had the largest sensitivity but the smallest specificity. In contrast, ‘Heavy Smoking’ had the largest specificity but the smallest sensitivity. Table 3 suggests that ‘High HSI’ performs better than the other indexes in terms of percentages of disagreement. In fact, ‘High HSI’ had the highest kappa agreement with the reference test (FTND ≥ 6).
Comparison of high nicotine dependence defined by FTND ≥ 6 versus four brief indexes (N = 819)
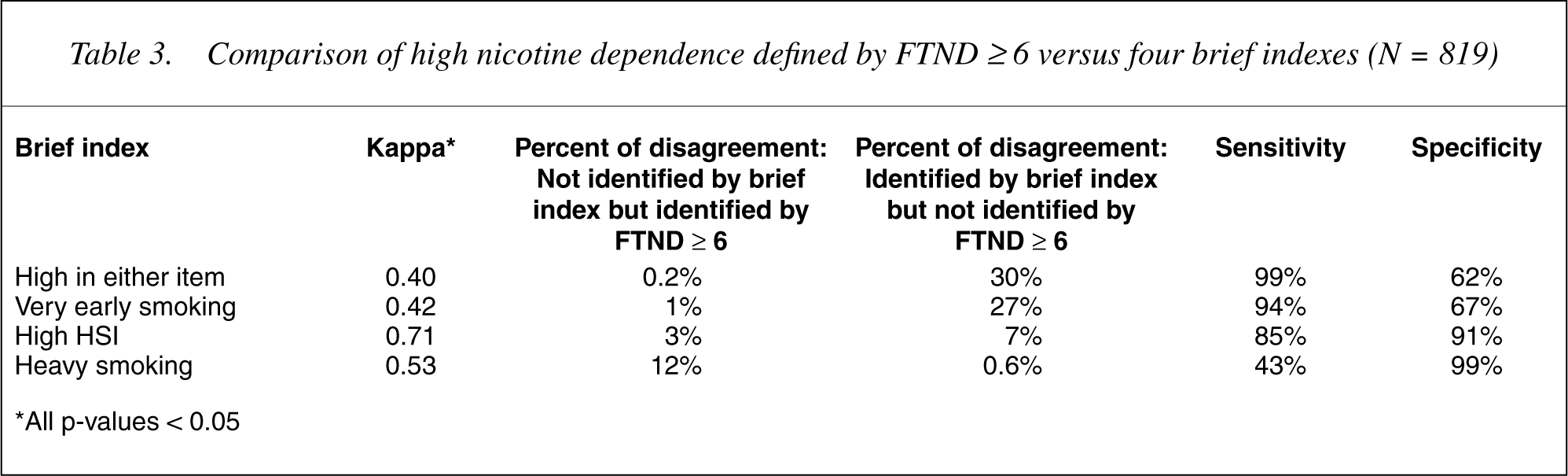
∗All p-values < 0.05
Discussion
Comparison of effectiveness of HSI, Items 1 and 4
The AUC method suggested that the HSI outperforms the effectiveness of its individual constituent items, namely FTND items 1 and 4, for detecting high nicotine dependence.
Optimality of 4 as a cut-off score for the HSI
31]. Essentially the same results were found.
Comparison of sensitivities and specificities of brief indexes
This new study verified our previous results that ‘High HSI’ has good sensitivity and specificity [31] and further extended them establishing that this index keeps its good sensitivity and specificity across different subclassifications in the population. Having a good sensitivity and specificity in both males and females is important since, for instance, a standard brief measure of alcoholism screening did not appear to function well in females [42]. Another brief instrument had to be developed for screening alcoholism in females [42]. In contrast, the ‘High HSI’ index should screen for nicotine dependence well in both genders.
Usefulness of the high HSI
In summary, the main conclusion of this study is that ‘High HSI’ is a relatively good screener for high nicotine dependence. It has a relatively good sensitivity and specificity in a variety of populations including psychiatric patients [31], and outperforms other brief indexes of high nicotine dependence. Clinicians may want to utilize it to obtain a quick and relatively accurate screener of high nicotine dependence (43–45].
A brief interview for the diagnosis of high nicotine dependence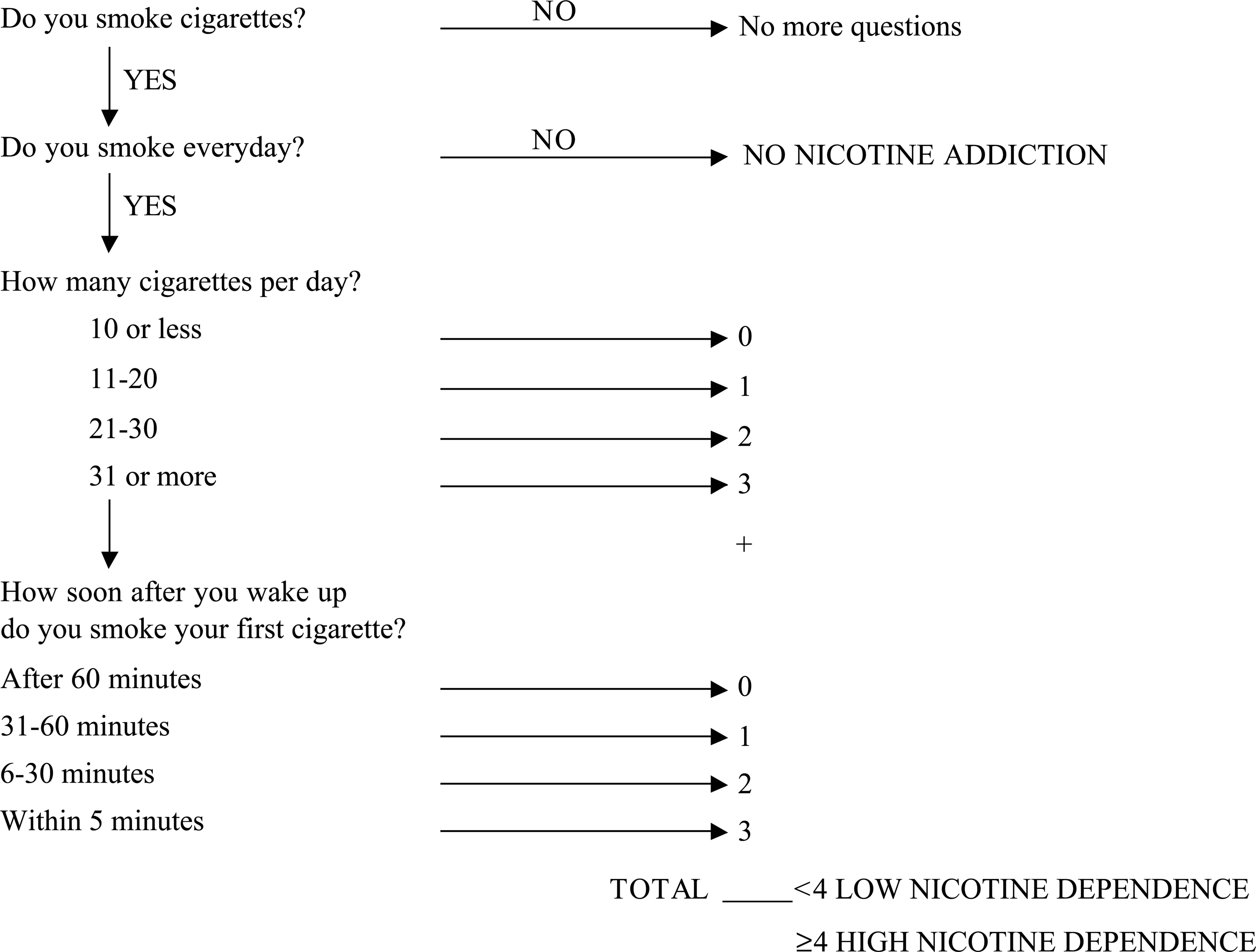
Health surveys usually include a question for current smoking and, if the patient is a current smoker, another question for the number of cigarettes smoked per day. Epidemiologists developing questionnaires for new health surveys may want to add a question regarding the time to the first cigarette of the day, since this simple addition will improve the screening of nicotine dependence.
Psychiatric researchers, particularly those studying schizophrenia and mood disorders, also need to seriously consider adding at least four questions (2].
In conclusion, with four questions and minimal calculations (Figure 2), it is possible to screen whether a smoker suffers from high nicotine dependence. This brief measure should probably perform similarly to the better validated FTND total score. If other studies in other populations and settings verify this finding, this brief measure might be an ideal instrument for busy clinicians, epidemiologists developing questionnaires for health surveys and psychiatric researchers.
Footnotes
Acknowledgements
The research was supported by the Generalitat de Catalonia.