
Abstract
The inclusion of family interventions in the treatment of people with schizophrenia has been developed and studied over the last 20 years. The main benefit reported for such interventions is a reduction in relapse rates. In the early development of family interventions for schizophrenia it was thought that these interventions were particularly beneficial to families with high levels of expressed emotion. However, recent evidence suggests that these interventions may be of benefit to all families [1]. The Patient Outcomes Research Team (PORT) [2] has recommended the inclusion of family interventions in the treatment of schizophrenia. In a PORT review [1] it was found that there are many models of family interventions. The key components of each include: psychoeducation; behavioural problemsolving; family support; and crisis management. Interventions are conducted both with individual or groups of families, in or out of the home and may include or exclude the person with schizophrenia. The length of the interventions vary, as do the phase of illness of the patient at the time of the intervention. Dixon and Lehman [1] distinguish between family education (driven by the self-help family movement) and professionally driven psychoeducation. With respect to professionally driven family interventions, the PORT study and other reviews, including a Cochrane review [3], [4], conclude that most family intervention models have a similar impact on patient outcomes. In contrast, there are no published studies evaluating the effectiveness of self-help family interventions.
Family interventions are not routinely delivered in Australia's public mental health services (M. Leggatt and B. Hocking, personal communication, 2002). In 1998, SANE Australia [5] conducted a survey of services for carers of people with mental illness detailing how each Australian state and territory approached carer support with respect to law, policy, budget allocations, information and education provision and any future developments. In summary, this report found that most family work occurred in the non-government sector in the form of counselling or telephone support services and the provision of written information, with very little if any properly designed and delivered family interventions within designated mental health services. Another recent report evaluating Australia's mental health services also highlighted the lack of family and carer intervention and support [6].
As such it was decided to evaluate the costeffectiveness of the routine introduction of family interventions into Australian mental health services. This study forms part of a larger study, the Assessing Cost-Effectiveness in Mental Health (ACE-MH) study which evaluates the cost-effectiveness of a number of interventions within an Australian mental health context using existing evidence and a common methodology [7]. The key research question of the current study within the ACE-MH framework is: ‘What is the incremental costeffectiveness of routinely introducing family interventions (defined as BFM, MFG or BIF) as an “add on” to current practice, compared to current practice from the economic perspective of the government and the client/ family?’
Method
Ideally, from a health economics perspective, utility-based healthrelated quality-of-life measures should be reported for each intervention considered. Lack of such information requires the development of a method to translate disparate clinical outcomes into a common economic outcome metric. A two-stage approach in the measurement of health benefit is used in all ACE-MH analyses. The first stage involves translation of outcome information into a common metric of health benefit, the disability adjusted life year (DALY) and the second stage involves applying ‘second filter criteria’ to all quantitative analyses (issues not usually considered in quantitative analyses, such as equity). Lastly, the costs of the intervention are determined using uniform assumptions tailored to Australian conditions. The term ‘family intervention’ is an umbrella term for various models of family interventions. We evaluate the cost-effectiveness of three specific types of family interventions which are well described and evaluated. These are behavioural family management (BFM) [8], multiple family groups (MFG) [9] and behavioural intervention for families (BIF) [10].
An economic evaluation protocol written for ACE-MH provides the basis for all evaluations [7]. However, the current analyses required some digression from this protocol due to outcome data published in a format incompatible to the protocol methods.
The interventions
Behavioural family management (BFM) is well specified in a series of training manuals [11]. The intervention consists of the following sequential steps: assessment; psychoeducation; communication skills training (following the principles of social skills training); and problem-solving training.
The first controlled trial of BFM [12] involved the provision of BFM on a declining contact basis. Families are seen weekly (for 3 months), then fortnightly (for 6 months), then monthly thereafter [8]. The intervention spans approximately 2 years (the quantity of family contacts can vary according to family need) and sessions occur in patients' homes. In a review of BFM, Liberman et al. [12] state that BFM can also occur in multiple family groups and can be delivered by a variety of mental health care providers (including nurses, social workers, psychologists and psychiatrists). However the original format of BFM as defined by Falloon [8] is used for the current study.
Behavioural intervention in families (BIF) was developed by Tarrier et al. ([10] and is similar to BFM but includes other behavioural techniques. The original study by Tarrier et al. (1996) investigated two types of behavioural techniques, enactive and symbolic, but found no differences in outcome. Therefore, the less resource-intensive technique will be modelled (symbolic). Specifically this is a 9-month intervention, comprising: two sessions of psychoeducation; three sessions of stress management; and eight sessions of goal setting.
Multiple family groups (MFG) was initially developed by McFarlane [9]. This intervention comprises: minimum of three sessions of family engagement (usually individual contact); two to three sessions of psycho-education; regular fortnightly sessions for 2 years and regular monthly meetings thereafter.
The groups consist of several patients, their families and two clinicians. Single-family contacts may also occur to help preserve family alliance and to manage crises.
Estimation of population of people eligible to receive the intervention
The prevalent cases of schizophrenia and related conditions for the year 2000 is modelled through a Markov chain with 1-year cycles for a period of 10 years. Diagnoses are defined using OPCRIT ICD-10 specific codes (11–17,19,20) from the Low Prevalence Disorder Survey (LPDS) [13]. We refer to these diagnostic categories as ‘schizophrenia’ but acknowledge that other diagnoses (such as schizoaffective disorder) are encompassed by this term.
It is assumed that each intervention will be appropriate for people with schizophrenia who have ongoing, regular contact with relatives/ family members. We use LPDS to estimate the proportion of people with schizophrenia in Australia who have ongoing regular contact with families. Specifically, people aged less than 65 who state they have either daily or frequent contact with brother/sister, parents, or other relatives, are included. People who only have contact with children are excluded. The age restriction is derived from published literature. Even though many studies only recruit people aged under 45 (e.g [8], [14]), we include older people, since other studies (e.g. [10]) have found positive effects for such people.
Assessment of benefit
In a Markov model, we determine the health benefits of the introduction of family interventions to the eligible population. The model uses cycles of one year at the end of which transition probabilities determine who remains alive with schizophrenia, who remits from schizophrenia and who dies. Mortality hazards include the general population mortality and the excess mortality attributable to schizophrenia. The difference lived between a baseline and intervention scenario determines the mortality component (years of life lost or YLL) of the disability adjusted life year (DALY). Those alive with schizophrenia, contribute to the non-fatal component of the DALY (years lost due to disability or YLD) as each year lived with disease is weighted for disability. Disability weights (DW) range from 0 to 1 and the higher the DW the more disabling the condition is considered.
The DW of the eligible population utilizes the same procedure as Magnus et al. [15]. In summary, we use the DIP-DIS scores [16] in the LPDS as an estimate of functional disability and assume that these scores change linearly with the Dutch Disability Weights for schizophrenia [17]. We anchor the best DIP-DIS score (0) to the best disability weight for schizophrenia (0.36) and conversely the worse DIP-DIS score to the worse disability weight for schizophrenia (0.97). A disability weight can then be calculated for each LPDS respondent.
Table 1 contains the relevant parameters used in the estimation of the base case scenario
Base case parameters for estimating disability-adjusted life years and cost assumptions for each intervention
To calculate the reduction in DALYs associated with family interventions we devised a method whereby reported clinical outcomes can be translated into DW changes (and therefore DALY changes). A generic method used in other ACE-MH studies is reported in Haby et al. [7]. However, this method relies on outcome measures presented as continuous variables. The main measure of outcome in family intervention studies is relapse, usually presented as a dichotomous outcome.
We develop an alternate method, also reliant on the DIP-DIS instrument from the LPDS whereby we use the odds ratio (of relapse rate reduction) to reclassify people into two states: ‘well’ or ‘unwell’. This is achieved by defining two severity states on the DIP-DIS with a cutoff between scores 4 and 5. Using the LPDS, 61.1% of respondents fit into the better state (DIP-DIS ≤ 4) and 38.9% fit into the ‘worse’ state (DIP-DIS ≥ 5). This split between the two severity states is chosen as it resembles findings from developed countries (whereby 41.6% of patients are reported to have impaired social functioning [18]). The odds ratio can then be applied to the proportion of time in a better state, thus deriving a change in average DW due to the intervention.
Figure 1 contains a worked example of the method.
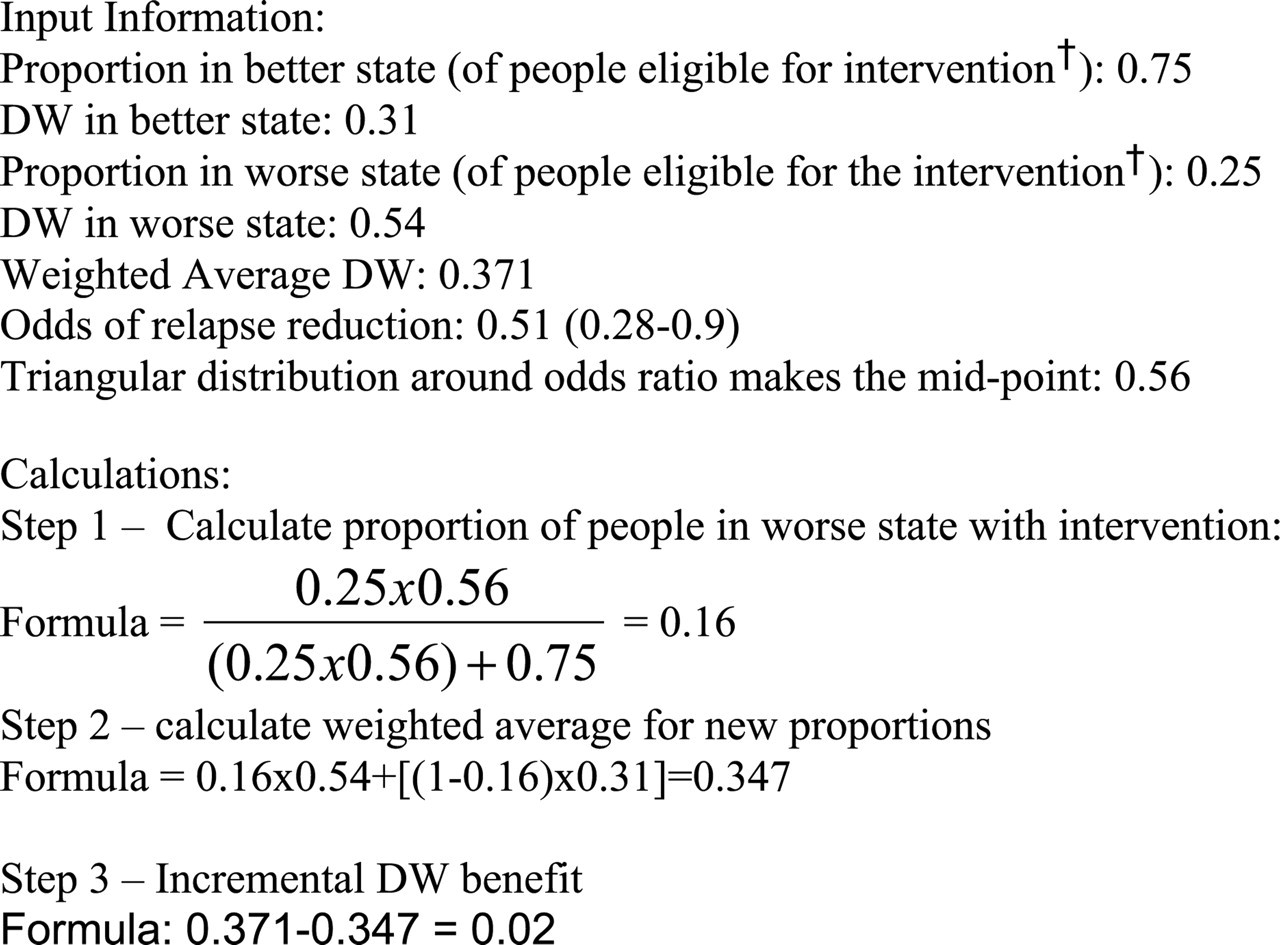
Method used to translate relapse rate reduction presented as an odds ratio into a disability weight change. † Please note that these proportions refer only to people in the LPDS meeting the eligibility criteria for the interventions, not the total cohort of people with schizophrenia.
The current analysis assumes that compliance to the interventions is lower than that observed in trials (approximately 85%). Consistent with other interventions analyzed in ACE-MH, we assumed the compliance varies between that in trials and 50%.
We derived an estimate of the impact from studies included in a Cochrane review of family interventions [3]. The odds ratio used is 0.51 (0.28–0.9) which is slightly different to the published ratio in the Cochrane review [3] as we used a random effects model, rather than the fixed effects model (refer to Haby et al. [7]). We used the same effectiveness for each of the three types of family interventions.
One trial has measured outcomes for up to 8 years of follow-up and continued to find lower relapse rates in the intervention group [19]. Considering there are no published data detailing how long the benefit of family interventions lasts beyond the few small studies with longer term follow-up, we assumed the benefit of all the interventions will last for 5 years and taper off to no benefit after a further 5 years. A 20% reduction in benefit every year after the first 5 years was modelled so that at 10 years post-intervention there is no benefit.
Given the assumptions required to estimate DALY health benefit we also calculated an ICER based on cost per relapse averted. Relapses averted are determined by dividing the total eligible population by the numbers needed to treat (to avert a relapse) estimate published in Pharoah et al. [3].
Costs
The costs of the three interventions are derived by estimating the per person cost of delivering each intervention. We assume the interventions will be delivered by a senior public sector clinical psychologist. The weekly salary of a year 3, level 2 public psychologist is A$1411 (including 30% oncosts).
Table 1 contains details of the cost assumptions. We also assumed that non-compliers will accrue costs (though no benefit) and that interventions will be provided in the same quantities and formats as specified by the key authors.
Cost-offsets as well as out-of-pocket costs to families have not been factored into the analyses. Previous studies of family interventions suggest there may be some cost savings [12], [20]. There is no published information about the cost of schizophrenia relapse in Australia. We investigated the costs of psychotic relapse versus the costs of people who do not relapse in the LPDS by regressing illness severity against resource utilization. In summary, illness severity is not very predictive of resource utilization. Social and Occupational Functioning Assessment Scale (SOFAS) scores, disability weights and diagnostic categories each predicted less than 7% of the variation in health service utilization, whether inpatient or outpatient care. Therefore we did not define a drop in resource utilization associated with a reduction in severity.
We also calculated time costs for both people with schizophrenia and their families in attending these interventions. We did not value production losses but rather the value of time per se (as time has an opportunity cost). There is no ‘gold standard’ method of valuing time [21]. We followed the simplest method specified in Jacobs [21], and determined a weighted hourly wage rate of $15.59 as a proxy for the value of time (adjusted for the proportion of total Australian population employed and unemployed). Differential rates were initially used for patients and families (based on different proportions employed). However, this was considered inequitable and discriminatory by the steering committee and rejected. Refer to Mihalopoulos [22] for further details.
The calculation of time costs was determined by assuming that each intervention contact lasts 1.5 hours. For interventions that require families to attend the clinic (BIF and MFG), a 40-minute round trip of travel time was factored into the time requirements (increasing the total time required to 2.2 hours). All these time requirements are estimates since no published information is available. The same assumptions regarding the total numbers of contacts required for each intervention as specified in Table 1 were made in the derivation of time costs. The time costs of non-completers were not estimated as these are trivial.
All costs and benefits were discounted at 3% as advised by the US Consensus Panel on Cost-Effectiveness [23]. Following the same source of advice we presented all figures to two significant digits only.
Sensitivity analysis
The robustness of the results are tested utilizing probabilistic sensitivity analysis with the @RISK software. This is a type of multiattribute sensitivity analysis whereby multiple parameters of the model are allowed to simultaneously vary. This type of analysis determines an empirical distribution around the ICER. This is accomplished by applying distributions to the specified ranges with subsequent samples randomly drawn from these ranges to simulate uncertainty [24]. A set of common methods were derived for uncertainty testing across all interventions in ACE-MH [7]. However, each intervention also includes a unique set of uncertain variables. Table 2 contains details on which parameters of the main model (excluding time costs) are simultaneously varied. We also varied the discount rate using 0, 5% and 7%.
Uncertainty parameters in the @Risk modelling simulations
Second stage filters
Readers are referred to Haby et al. [7] for details on the precise methods followed in the assessment of the second filter criteria for ACE-MH. The second stage involved the assessment of issues that influence the degree of confidence placed in the ICERs (such as the quality of the available evidence), or broader issues that need to be considered in decision-making about resource allocation (such as equity and acceptability to stakeholders). The filters chosen for ACE-MH were:
•
•
•
•
Results
All ICERs fall below the cut-off of A$50 000 per DALY which has been selected by the ACE-MH study as a guide to ‘value for money’ in the Australian context (refer to Table 3).
Results of cost-effectiveness analysis
With respect to time costs, unsurprisingly BIF incurs the least time costs (A$12m), followed by BFM (A$22m) and lastly MFG (A$52m). The ICERs incorporating time costs are A$11 000 per DALY (for BIF), A$35 000 per DALY (for BFM) and A$43 000 per DALY (for MFG).
Variation in the discount rate does not change the ordering or magnitude of the ICERs to any significant extent (refer to Table 3).
Furthermore, the incremental cost per relapse averted for BFM is A$22 000 (A$12 000–A$34 000), for BIF A$8000 (A$5000–A$13 000) and MFG A$10 000 (A$6000–A$17 000).
Second stage filter considerations are:
•
•
•
•
Discussion
The interventions assessed in the ACE-MH study fall into two major groups. Those defined as ‘value-formoney’ at an ICER less than A$50 000 per DALY and those above this benchmark (or ‘shadow price’). It is important to note that judgements about ‘shadow price’ are community judgements about what a society wants from its health care system and what share of GDP should go to health. The ‘shadow price’ is normally set having regard to anticipated funding levels and how resources are currently utilized in the health sector. It is offered as a guide only and should not be over interpreted.
All three types of family interventions for people with schizophrenia have favourable ICERs. It is unfortunate that such interventions are not receiving much attention in Australian mental health services.
Behavioural interventions for families is the most costeffective family intervention, followed by MFG and BFM. However, if time costs are also considered BFM appears to be more cost-effective than MFG (BIF remains the most cost-effective). A number of caveats must be expressed with respect to these findings. First, the evidence with respect to the effectiveness of each intervention is not compelling. Even though a conservative estimate of effect is utilized, the trials upon which this result is based on are all relatively small. It is not inconceivable that a large trial failing to show any effect may dramatically change the odds ratio derived from the meta-analysis. Another important consideration is that some of the trials only included families/relatives with high expressed emotion. The current analysis assumes that the interventions are beneficial to all eligible people (as per PORT recommendations). This assumption is probably realistic since there are no differences in outcome between studies which only include high expressed emotion families and those with broader inclusion criteria.
Another important consideration in the interpretation of these findings is the cost of each intervention. It is unsurprising that the BIF is the least costly, given it is the shortest and least intensive contact intervention. The current study modelled the cost of each intervention as incremental to the public mental health services currently offered. There is an inherent assumption that existing mental health staff cannot incorporate family interventions in their current full-time work loads. The costs of family interventions determined in this study could be either specified family workers undertaking these interventions or supplementary case-managers, so that case-managers carry out the interventions (with the assumption that their case-loads will reduce to allow time for family interventions). Falloon et al. [8] suggests that family interventions are best undertaken by existing case-managers; however, there is no definitive evidence on this issue. A fundamental problem requiring attention is the lack of training in such interventions for mental health staff, both at graduate and post-graduate levels (training costs have not been considered in this study). Regardless of who delivers the interventions (casemanagers or family workers), there is little reason to believe the ICERs will change as the financing of both types of workers is likely to be very similar.
The assumption that the interventions will be provided by public sector psychologists infers that patients treated in the private sector (e.g. by GPs or private psychiatrists) will be referred to the public sector for the provision of family interventions. The likelihood of this is debatable under current health service arrangements. A single clinician delivering the intervention has been modelled for BFM and BIF; however, there may be occasions where two clinicians are required (such as home visits where the family and/or patient presents some risk). This will of course increase the costs of the interventions.
The most important caveat to these findings is the methodology utilized to derive the health benefit. A number of assumptions have been made in converting a dichotomous, disease-specific outcome (odds of relapse) into a gain of health-related quality-of-life as measured by the diability weight used in the calculation of DALYs. However, the issue of translating clinical outcomes into associated DALY changes is central to all ACE-MH interventions. The methods developed for ACE-MH are largely innovative and require further validation. Future research must consider the effects of such interventions on health-related quality-of-life and include such measures in trial data. Furthermore, other benefits to families, such as reduction in carer burden and even improvements in carer quality-of-life have not been included in the analyses.
Most Australian states/territories allocate some funding (to variable degrees) for carers of people with mental illness (not specifically schizophrenia). A SANE Australia survey [5] found that services and funds available for carers of people with a mental illness are highly variable. For example, in 1998 Victoria had an allocated budget of A$1.3m for respite care and A$3.1m for a carer crisis support fund (used mainly for respite activities). In contrast, South Australia allocated A$13 600 to the non-government sector to support carers and the Northern Territory allocated A$56 000 to the same sector. Many states and territories (e.g. NSW and ACT) had no specific budget allocated and services offered were ad hoc and uncoordinated. Even though this survey is outdated, it is unlikely that things have changed dramatically (B. Hocking, personal communication, 2003). The incremental cost of implementing family care to governments may be smaller if some existing funds (particularly in Victoria) are utilized for this purpose, although the opportunity costs require consideration. The provision of financial incentives to services which undertake this work may be another way to improve the likelihood of family interventions being offered.
The relevance and appropriateness of these interventions to people in rural and remote areas is unknown. Given that the interventions presuppose face-to-face intensive contact with mental health service providers, how this would work in practice in rural/remote areas is unknown and poses an equity of access issue. A solution may be to use tele-psychiatry, although the costing of the interventions presented above has not included such costs. It is therefore advisable to pilot such interventions in rural/remote areas before full implementation to ensure feasibility and acceptable cost-effectiveness.
Conclusions
The provision of all three models of family interventions appear to demonstrate acceptable ICERs, although further research needs to consider the effect of the interventions on health-related quality-of-life. Given issues surrounding the levels of evidence, feasibility and acceptability of the routine introduction of such interventions within mental health services in Australia, it is advisable that implementation should be accompanied by collecting local evaluation data to confirm costeffectiveness in the Australian context. The introduction of such interventions into routine mental health services must receive the full support of governments, area mental health managers and senior clinicians to increase the likelihood that they are offered in a comprehensive and effective manner.
Caveat
The ACE–Mental Health project was jointly funded by the Australian Department of Health and Ageing, Mental Health and Suicide Prevention Branch and the Department of Human Services, Mental Health Branch, Victoria, in recognition of the importance of research into the cost-effectiveness of interventions in mental health treatment and care. This work draws upon, but is also limited by the available research and the assumptions necessary to complete the work.
The results of the analyses provide valuable material, likely to contribute to future policy deliberations by all service providers. Conclusions drawn from the economic evaluations should be considered within the context of the second-stage filter process, which qualifies the results, taking into account issues of equity, feasibility, strength of evidence and acceptability to stakeholders. This second-stage filter process addresses some of the practical considerations required for changes in actual service practice.
Footnotes
Acknowledgements
We thank the ACE–Mental Health Steering Committee: David Barton, Graham Burrows (Chair), Sue Caleo, Vaughan Carr, Dermot Casey, Joy Easton, William Hart, Barbara Hocking, Helen Herrman, Assen Jablensky, Tony Jorm, Lyn Littlefield, Patrick McGorry, John McGrath, Paul Morgan, Lorna Payne, Deb Podbury, Kristy Sanderson, Suzy Saw, Bruce Singh, Bruce Tonge, Harvey Whiteford. We also thank Margaret Leggatt, Brendan O'Hanlon and Jeff Young for input and advice.
The present report is based on data collected in the framework of the Collaborative Study on Low-Prevalence (Psychotic) Disorders, an epidemiological and clinical investigation which is part of the National Survey of Mental Health and Wellbeing, Australia 1997–1998. These data were provided by the Data and Publications Committee of the Low Prevalence (Psychotic) Disorders Study Group. The views of the authors may not necessarily reflect those of the Study Group.