
Abstract
Keywords
The need for continuation treatment to consolidate recovery from depressive episodes and to prevent relapses has been well demonstrated in placebo controlled studies and highlighted in a recent systematic review [1], [2]. Expert opinion and therapeutic guidelines advise that antidepressants should be continued for at least 6 months after a single episode of major depression, as there is a high risk of relapse in this period [3–6].
The two main classes of antidepressant therapy used in Australia during the 1990s were the selective serotonin reuptake inhibitors (SSRIs) and the tricyclic antidepressants (TCAs) [7]. The SSRIs were introduced as safer and better tolerated, although considerably more expensive, alternatives to the TCAs, the previous mainstay of antidepressant pharmacotherapy.
The evidence for improved tolerability of the SSRIs was primarily based on the drop-out rates seen in clinical trials, typically conducted over periods of only 6–12 weeks duration and in highly controlled situations [8], [9]. Some observational studies in the US and UK have also found fewer treatment drop-outs in actual practice among patients on SSRIs [10], [11].
The aim of this study was to investigate the proportion of community-based patients who receive an antidepressant, whatever their diagnosis, that continue on antidepressants for a period consistent with recommended guidelines for major depression, that is at least 6 months.
Here we describe a cohort study tracking individual patients, selected from the Australian national dispensing claims database, to determine specifically the proportion of patients starting on either SSRIs or TCAs who continued treatment 6–8 months after initiation. Intermediate time points at the 2–4 month and the 4–6 month intervals were used to determine when any differences between these two populations, should they occur, become manifest.
We also examined the change between 1996 and 2000 in the proportion remaining on therapy with these two antidepressant classes. Furthermore, for patients starting on either a leading SSRI (sertraline) or TCA (dothiepin), we investigated the proportion that remained on these drugs 6–8 months later and the extent of change to other antidepressants.
Materials and methods
Within the subsidized prescription database maintained by the Australian Health Insurance Commission (HIC) there is a subset of patients who have been, since the beginning of 1996, assigned a unique identification number [12]. The subset comprises individuals receiving social security entitlements and therefore paying a minimal contribution to the cost of the medication (copayment). This entitlement allows the capture in the database of the records of all their antidepressant prescription use (other than private prescriptions). The permanent identification number (PIN) that is assigned represents an individual and allows a patient prescription profile to be assembled; however, it cannot be decoded by the Department of Health and Ageing to identify a particular named patient.
Although people with social security entitlements are overrepresented by the elderly and by females when compared to the general population, a survey of general practice activity in 1998/99 found that the age/sex distribution was close to that of patients who were prescribed antidepressants in Australia [12]. They are also high volume users of prescription medicines in Australia. In 1996, persons covered by concession cards represented 39% of the population but received 64% of the prescriptions dispensed through community pharmacies [13].
From HIC records we identified all individuals (PINs) who were supplied a prescription for an SSRI in the first week of April 2000. From within this group, a cohort of ‘new users’ was defined as those who had not received a prescription for any antidepressant in the preceding 3 months (i.e. January to March 2000). A similar cohort of ‘new users’ who commenced on a TCA in the first week of April 2000 was also established. Length of therapy was assessed by examining the HIC claim records for the subsequent dispensing of either SSRI or TCA prescriptions, respectively, to the patients in these separate cohorts.
Although the ‘new user’ cohorts were selected by having had either an SSRI or a TCA prescription dispensed in a particular week, subsequent re-presentations of these patients' prescriptions would be determined by the individual differences in the doses prescribed and quantities dispensed. The primary key within the dispensing database is the date of supply of medication, not the patient ID, which can only be examined after the initial data extraction phase. Therefore, the time period chosen in which to determine if the patient was still receiving SSRI or TCA therapy needed to be sufficiently broad (in this case 3 months) to be sure of detecting the dispensing of further prescriptions.
The dispensing data are not linked to reason for prescribing in the national dataset. However, surveys indicate that most antidepressants are prescribed for patients with depression, though the diagnosis is not always major depression on DSM-IV criteria [14].
The main outcome measure was the proportion of patients who were still having any SSRI or TCA prescription, respectively, dispensed between 6 and 8 months after initiation (i.e. prescriptions dispensed between October and December 2000). Intermediate time points of between 2 and 4 months (June – August 2000) and between 4 and 6 months (August – October 2000) were also used to examine difference in discontinuations between the two drug classes over time.
To determine if these proportions have changed over time, an analysis of similar cohorts established in 1996, four years earlier, was conducted.
A subgroup analysis to determine the extent of change to other antidepressants was also performed on the two most commonly prescribed antidepressants (sertraline and dothiepin) within the year 2000 SSRI and TCA ‘new user’ cohorts. The proportion remaining on antidepressant therapy (both of the initiating drug and for any other antidepressant) 6–8 months after initiation was determined.
Although the PIN separately identifies the primary card holder from any dependants also covered, the PBS safety net that reduces the patient copayment after a specified number of prescriptions have been dispensed is a family-based system. Any PIN that reached safety net status during the study period was excluded from the analysis to overcome the possibility of contamination with the prescription use of dependants.
Two-sample tests of proportion, measured at the 5% significance level, were conducted using the STATA statistical package [15].
Results
Differences between SSRI and TCA groups
In the SSRI cohort, there were 53 066 individual patients with a permanent identification number (PIN) who had a prescription dispensed for an SSRI antidepressant in the first week of April 2000. Of these, 6752 had not previously received a prescription for any antidepressant in the 3 months prior to April (i.e. January to March 2000 inclusive).
Excluding any patients that reached PBS safety net status within the 2000 calendar year produced the study cohort of 6026 patients.
These patients were defined as SSRI ‘new users’ and represented people who were starting therapy for a new or initial episode and not merely switching to SSRIs from another antidepressant. An identical method produced the TCA ‘new user’ cohort in the year 2000 of 4158 patients.
Of the 6026 SSRI ‘new users’ in the first week of April 2000, there were 2267 (37.6%) still receiving SSRIs 6–8 months later, that is between October and December 2000. For the corresponding cohort of 4158 TCA ‘new users’ in the first week of April 2000 there were 1269 (30.5%) still receiving TCA prescriptions 6–8 months after initiation.
This statistically significant difference (p < 0.001) in favour of patients remaining on therapy with the SSRIs was also evident at the intermediate 2–4 month and 4–6 month time intervals (Fig. 1). Interestingly, all the differentiation between the SSRI and TCA ‘new user’ cohorts occurs early, by the 2–4 month time interval. There was no statistically significant difference (p = 0.23) in the proportions staying on therapy from this time through to the end point at 6–8 months.
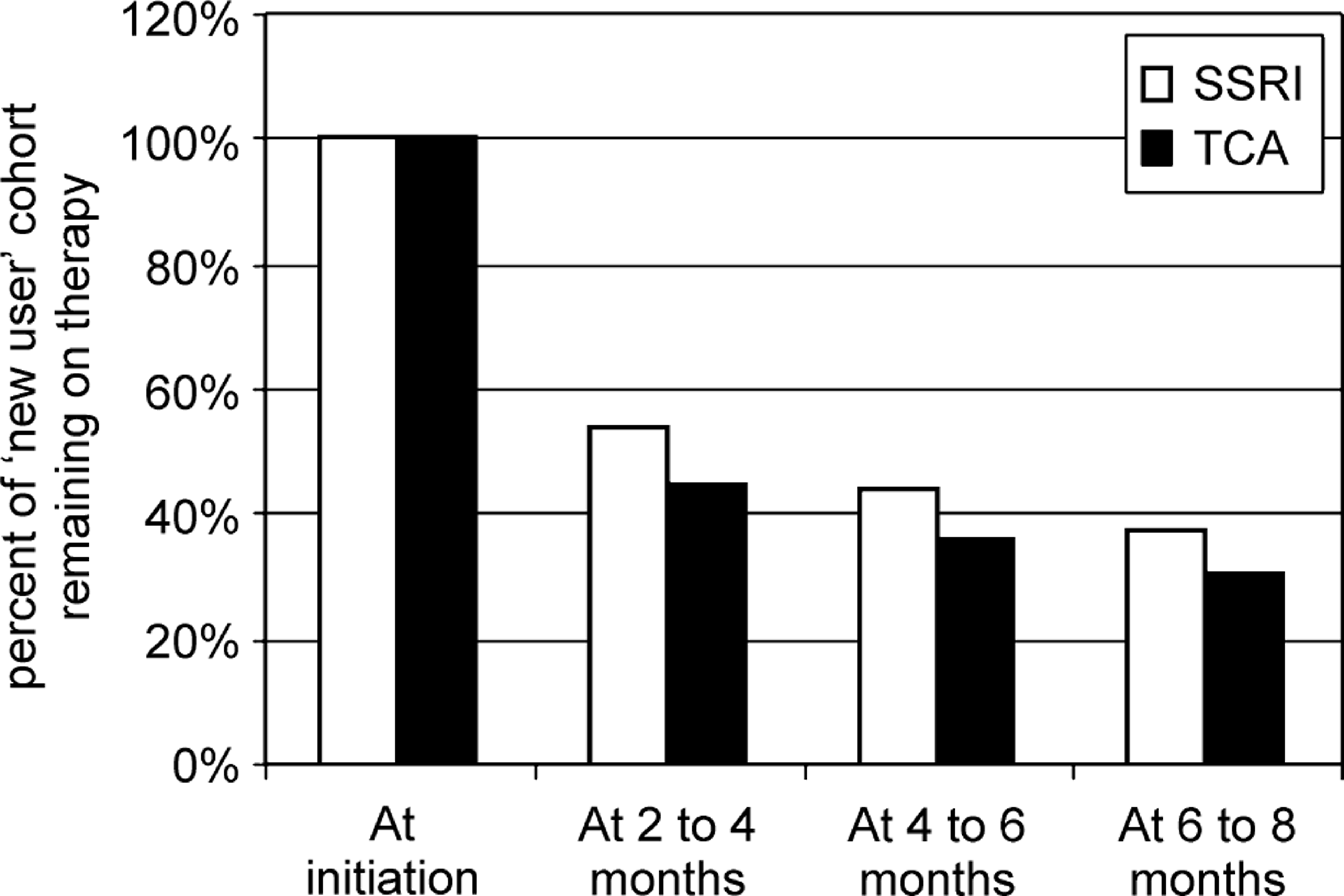
Proportion of the SSRI (6026) and TCA (4158) ‘new user’ cohorts remaining on either SSRIs or TCAs, respectively, at: 2–4 months; 4–6 months; and 6–8 months after starting therapy.
Changes over time
To examine for any change in practice over time, the proportions still on therapy after 6–8 months in 2000 were compared with those of two similarly established SSRI and TCA ‘new user’ cohorts in the first week of April 1996, a time period 4 years earlier. For the 1996 SSRI ‘new user’ cohort, 693 patients (36.8%) were still receiving SSRI prescriptions and 1383 (29.5%) of the TCA cohort were still receiving TCAs 6–8 months after initiation. The small increases in the proportion of patients reaching this endpoint in the 2000 cohorts were not statistically significant for either the TCA (p = 0.29) or the SSRI (p = 0.53) ‘new user’ cohorts.
Switching between antidepressants
With many new antidepressants available on the market, some measure of the level of switching between antidepressants that occurs during therapy was sought. To examine this, a subgroup analysis was conducted within the SSRI and TCA ‘new user’ cohorts of patients starting on either sertraline or dothiepin. These agents were chosen as they were the ‘market leader’ SSRI and TCA, respectively. The proportions that remained on these drugs, or had changed to other antidepressants by the end of the study period, was then determined.
Of the 2538 sertraline ‘new users’ in the first week of April 2000, 831 (32.7%) were still receiving sertraline at the 6–8 month interval, while a total of 1038 (40.9%) of these patients were receiving some type of antidepressant therapy at this endpoint. Of the patients that had changed antidepressant therapy (207), the most frequent changes were to: venlafaxine 45 (21.7%); citalopram 44 (21.2%); and paroxetine 24 (11.6%).
Of the 1018 dothiepin ‘new users’ in the first week of April 2000, 307 (30.2%) were still receiving dothiepin at the 6–8 month interval, while a total of 385 (37.8%) of these patients were receiving some antidepressant therapy at this endpoint. Of the patients that changed antidepressant therapy (78), the most frequent changes were to: sertraline 18 (23.1%); paroxetine 14 (17.9%); and equally venlafaxine 13 (16.7%) or citalopram 13 (16.7%).
There was no significant difference between the sertraline and the dothiepin ‘new user’ cohorts in the proportion of patients that either remained on the initial drug (p =0.14) or had changed to another antidepressant (p =0.6) at the study endpoint.
Discussion
The focus of this study was on the continuation phase or length of therapy following the index episode of antidepressant drug use. Controlled studies have found that the initial duration of antidepressant therapy is an important determinant in relapse episodes, with the risk of relapse decreasing as treatment time increases [16], [17]. Consensus guidelines recommend that antidepressants should be continued for at least 6 months after a single episode of major depression [4], [6], and longer for those with recurrent depression.
A recent systematic review recommended that patients at ‘appreciable risk’ of relapse after this interval would benefit from continuation treatment well beyond this point [2]. However, the clinical trials involved were conducted mainly in secondary or tertiary care settings whereas the majority of antidepressant prescribing (and its initiation) occurs in primary care [18].
In the present study, approximately 40% of the patients initiating treatment with a commonly prescribed SSRI (sertraline) or TCA (dothiepin) were still taking some form of antidepressant therapy at least 6 months later.
As for between class differences, our analysis has found that the proportion of SSRI ‘new users’ remaining on SSRI therapy for at least 6 months was significantly higher than that for TCA ‘new users’ remaining on TCAs. The difference in persistence with therapy occurred early (within 2 months) with no significant difference in the drop-out rate between patients on either SSRIs or TCAs from this time up to the study endpoint at 6–8 months. This early expression of difference may reflect the period when the TCA side-effects are at their worst, whereas some of the side-effects of the newer antidepressants such as sexual dysfunction become more apparent with time [19].
Pooled results from randomised controlled trials conducted over a short time-frame (generally 4–6 weeks) have found that overall discontinuation rates were either significantly (though not dramatically) lower on SSRIs than TCAs as a group [8], [9] or did not differ significantly [20]. Internationally, some prescription database analyses have found that the duration of treatment did not differ significantly between patients taking SSRIs or TCAs [21], while other observational studies in primary care found that discontinuation rates were significantly lower for patients on SSRIs than those on TCAs [10], [11].
When we examined a specific commonly prescribed SSRI (sertraline) and TCA (dothiepin), there was no significant difference between the two groups in continuation on therapy with the initial drug, or in the proportion of patients changing to another antidepressant by the study endpoint. The proportion changing drug therapy was similar in both cohorts (around 8%) and most often to a drug from one of the newer antidepressant classes (specifically venlafaxine or one of the SSRIs). A similar level of switching between antidepressants has been seen in prescription database studies overseas [21].
Females overall and the elderly were over-represented in the source population from which the study cohorts were drawn, two groups that are likely to be more compliant with medication [22]. However, the source population was similar to that of the population prescribed antidepressants in primary care, and the elderly face countervailing compliance difficulties due to greater number of prescribed medicines, physical limitations and cognitive decline [23].
There has been no significant increase in the proportion of patients remaining on therapy for at least 6 months in 2000 when compared with a similar period in 1996 for either of the SSRI or TCA ‘new user’ cohorts. However, the proportion staying on antidepressant therapy for at least 6 months here is certainly higher than the 23% of patients in Australian general practice staying on antidepressant therapy for a similar length of time in the mid-1980s [24].
In summary, the main findings that emerged from our study were as follows: (i) only 40% of patients started on an antidepressant continue to be prescribed some antidepressant therapy 6–8 months later; (ii) patients were more likely to continue on SSRIs as a class than on TCAs; (iii) the difference in continuation between these two classes occurs early, in the first 2 months of therapy, however; (vi) a patient starting on an individual TCA appears no more likely to change antidepressants than a patient starting an individual SSRI, with the direction of change in each case to venlafaxine or an (another) SSRI.
This study was conducted within a dispensing claims database that contains no link to diagnosis. However, earlier work in primary care had shown that the majority of use was in the management of depression, although more so for the SSRIs than the TCAs [14].
The experience in Australia appears similar to the results seen from studies and reviews in Europe and the US that indicate fewer than 50% of treated patients receive the recommended duration of 6 months of continuation therapy [25], [26].
There are two possible interpretations of this. First, it may be that this indicates inadequate practice, with a higher rate (as recommended) and education to this end being desirable. Many patients with major depressive disorder are probably not receiving maintenance antidepressants for the recommended time interval, whether TCAs or SSRIs. The extent of under-treatment in terms of duration of therapy is uncertain because the dispensing database and the other sources of GP survey data do not permit a precise diagnosis in the primary care setting.
Second, from GP national survey data, possibly as many as 80% of patients managed for depression in general practice may not have ‘major depressive disorder’, depending on how GPs apply the diagnostic criteria for this condition [18], so the rate seen in this study may not be inappropriately low. The recommended guideline of at least 6 months continuation therapy is derived from studies in psychiatric practice, and may not be necessary in the less severely depressed population seen in the primary care setting.