
Abstract
Over the past two decades criteria for depressive disorder in adults have come to be widely applied in both adolescent and childhood depression [1–3]. It is now clear that, in females, depressive symptoms become common after puberty and rates of incident disorder rise steeply from the mid-teens [4–6]. Depressive disorder is estimated to be the leading cause of disease burden in young Australian females [7], and in adults of both sexes a leading cause of disease burden in Australia and other developed countries [8,9].
Most available information on the symptom profile in adolescent depression derives from patients seen in psychiatric settings [1]. In this group, psycho-motor and melancholic symptoms appear relatively uncommon and on this basis the profile of depression in adolescents has been assumed to differ from that in older people [1,10,11]. However, patients in clinics differ from community cases in the severity of disorder and the presence of comorbid conditions, and consequently the symptom profile found [12]. Community-based studies should be better able to provide an indication of whether criteria developed for adults are applicable to younger subjects. Such information is particularly relevant in considering strategies of early detection and intervention that rely on optimal identification of subjects.
There has, to date, been only one population-based study describing symptoms of adolescent depressive disorder [13]. The extent to which depressed adolescents consistently report symptoms outlined in adult diagnostic criteria remains little explored. Nor is it clear which symptoms may be most useful either in the identification of young people with depressive disorder or in guiding treatment responses. These questions are addressed in a descriptive study of a large population-based sample of Australian adolescents.
Method
The study used a two-phase design with the first phase set within the Victorian Adolescent Health Cohort Study [14]. This six-wave study took place in the State of Victoria, Australia between August 1992 and July 1995. The State has a population of 4.4 million of whom 63% live in the capital city, Melbourne [15]. The first phase (cohort) sample was defined using a two-stage sampling procedure. Forty-five schools were randomly selected from a stratified frame of all schools in the state (Government, Catholic and independent strata) with a probability proportional to the number of year nine students in the schools in each stratum in the state (total number 60 905; average age at study entry 14.5 years). Two classes were selected from each school to constitute the phase 1 (cohort) sample. One class from each school entered in the latter part of the ninth school year (wave 1) and the second 6 months later, early in the tenth school year (wave 2). Data were collected in a total of six waves at 6-monthly intervals. One school from the initial sample participated at wave 1, but was unavailable for the cohort study leaving a total sample of 88 classes from 44 schools, of which 24 were Government, 11 Catholic and nine independent private. The second phase of the study was implemented at each wave except the first (Fig. 1).
Design and participation in a two phase study of depressive disorder in Victorian secondary students. Total intended sample = N1 + N2 = 2032; total achieved sample = 1947 (96%).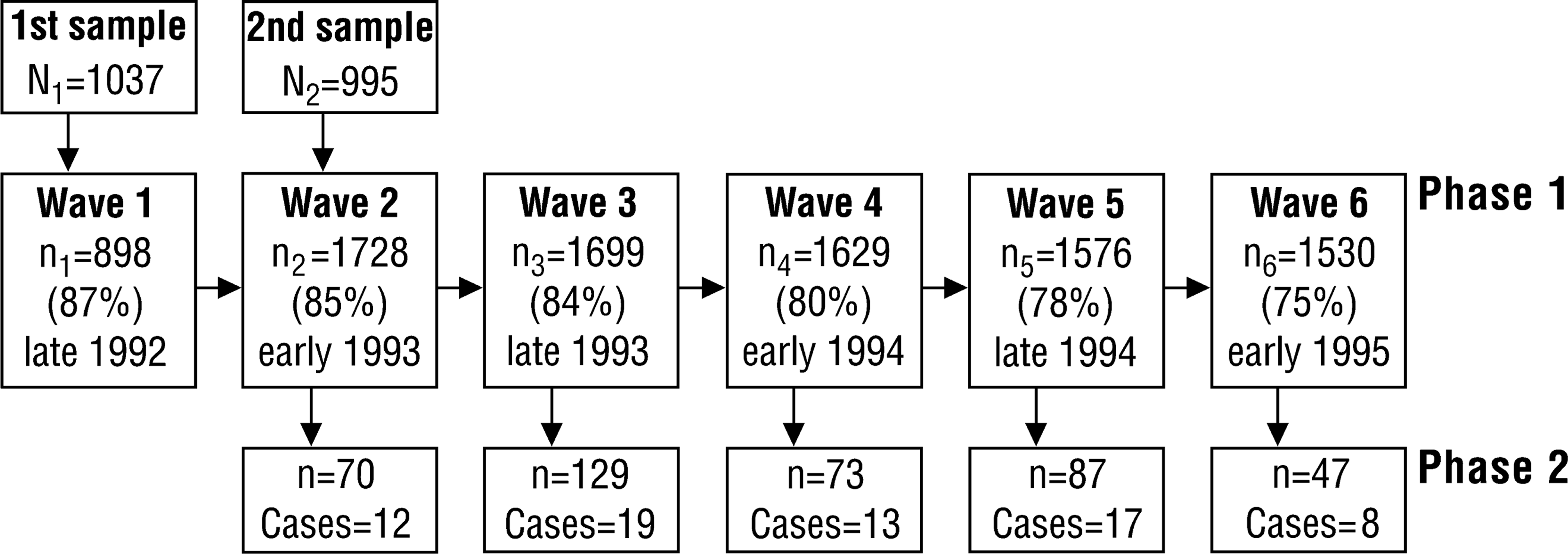
Procedure and measures
Phase one
In the first phase the computerised version of the Revised Clinical Interview Schedule (CIS-R) was used as a measure for depressive disorder [16]. The CIS-R is a branched questionnaire, designed for assessing symptoms of depression and anxiety in non-clinical populations. Fourteen subscales delineate the frequency, severity, persistence and intrusiveness of symptoms commonly found in depression and anxiety. These symptoms were used to generate diagnoses of ICD-10 depressive disorder. Each subject fulfilling criteria for at least a mild depressive episode was selected for phase 2. For each CIS-R case, two subjects not meeting criteria were selected at random at the same time at each school [17].
Second phase assessment
All individuals selected for phase 2 were invited to attend for a further diagnostic assessment and more detailed measurement of putative risk factors for early onset depression. The depression and hypomania modules of the Composite International Diagnostic Interview (CIDI, Core Version 1.1) were used to generate ICD-10 diagnoses for affective disorder [2]. The CIDI is a structured diagnostic interview devised for use by non-medical professionals after a standardised training [18]. A ‘somatic syndrome’, equivalent to the melancholic, biological or endogenous subtypes in other classifications, was defined on the presence of four out of eight symptoms. A research psychologist, trained in the use of the CIDI and blind to first phase CIS-R scores or diagnostic status conducted the second phase interviews. These took place at a subject's school within 3 weeks of completion of at least 70% of first-phase assessments in that school. Subjects confirmed as cases of depressive disorder on the CIDI at second phase interview were excluded from the selection procedure for phase 2 at subsequent study waves. Participants who fulfilled CIS-R criteria, but not the CIDI were returned to the sampling frame in subsequent waves.
Analysis
Data analysis was carried out using the Stata program (Stata, College Station, TX, USA) [19]. Stata's survey estimation commands (svymean, svylc) were used in the estimation and comparison of prevalence rates. Inverse probability weights, designed to approximate the inverse of the sampling fraction at the second phase assessment, were used in all analyses. For CIS-R cases, weights were the inverse of participation rates at phase 2. For CIS-R non-cases, probabilities of selection were estimated for each school across all study waves. These were then used to group the 44 schools into tertiles corresponding to high, intermediate and low probabilities of screen-negative selection. The probability weight for all subjects within each fertile was obtained as the inverse of the ratio of the number of screened subjects to the total number eligible within the tertile. This specific approach was used to smooth the estimated weights as numbers within each school were too small to calculate meaningful weights. The weighting procedure adjusted first for the fact that the control group consisted of disproportionate numbers of screen-positives, and second for the potential bias arising from first phase non-cases being more likely to be drawn from schools with high numbers of cases.
Results
Phase 1 responses (the cohort study)
From a total sample of 2032 students on class registers, 1947 (95.8%) completed the first phase (cohort) questionnaire at least once in the course of the study. Based on the total selected sample, response rates across waves were as follows across waves 1–6: 87%; 85%; 84%; 80%; 78%; 75%. The gender ratio of the cohort (males 47.0%) was similar to that in Victorian schools at the time of sampling [20]. The mean age at wave 1 was 14.5 (SD = 0.5) years and at wave 6, 17.4 years (SD = 0.4). Two hundred and thirty-three subjects (12% of participants) completed only one or two waves of the study and were designated ‘low completers’. Low completers were compared with other participants in a multiple logistic regression analysis. Males were overrepresented in comparison to females (odds ratio (OR) = 2.1, 95% CI = 1.6–2.7), as were Australian-born subjects (OR = 2.6, 95% CI = 1.5–4.5), and those who had experienced parental divorce (OR = 2.5, 95% CI = 1.5–4.2). Depressive symptoms at entry (OR = 1.6, 95% CI = 0.8–3.2) and school location (metropolitan vs non-metropolitan) (OR = 1.0, 95% CI = 0.6–1.7) did not appear to differ greatly in high and low completers.
Phase two responses
One hundred and forty-five subjects across waves 2–6 fulfilled CIS-R criteria for depression and were selected for second phase interview. One hundred and thirty (90%) of the first phase cases completed second phase assessment. Two hundred and ninety subjects were selected from the CIS-R non-case stratum, of whom 276 (95%) participated at the second phase. Reasons for second phase non-participation were absenteeism or persistent interview non-attendance (n = 22), parental refusal (n = 5) and premature termination of interview (n = 2).
Of the 130 first phase cases, 69 (53%) also fulfilled criteria on the CIDI and were designated ‘confirmed’ cases. Of these cases, 59 (86%) were female and 10 (14%) male, corresponding to period prevalence rates in the main cohort sample of 5.9% in females and 1.1% of males. Of the 276 subjects drawn from the first phase non-cases, 24 (9%) also fulfilled the lifetime diagnostic criteria on the CIDI and were not included in the analysis. Twenty-five (36%) of the 69 confirmed cases reported one or more previous episodes. Ninety-four per cent reported their first episode at the age of 12 or later. The maximal episode severity according to ICD-10 rating was severe in 16 (23%), moderate in 32 (46%) and mild in 21 (31%). Seven of the confirmed cases also fulfilled criteria for the somatic syndrome (at least four of eight somatic symptoms). The somatic syndrome was uncommon in mild and moderate episodes, but was present in close to one in three of those who described severe episodes. The following analyses do not include the 24 subjects who were cases on the CIDI, but not on the CIS-R. The CIS-R cases not confirmed on the CIDI were incorporated into the control category.
Rates of individual depressive symptoms
Symptom frequencies in confirmed cases using the CIDI ratings are shown in Table 1.
Frequency∗ (as percentage with 95% confidence intervals) of ICD-10 depressive symptoms in 69 adolescents with confirmed depressive disorder defined by the CIS-R and CIDI and 313 adolescent controls
Cases
The commonest ICD-10 symptoms were depressed mood and fatigue. All other ICD-10 symptoms were reported by the majority of cases with the exceptions of psychomotor retardation or agitation (42%). The mean number of somatic symptoms reported by cases was 2.3 (95% CI = 1.9–2.6) with the commonest being lack of emotional reactivity, diurnal variation in mood and reports of objective psychomotor change.
Non-cases
Depressed mood was reported by almost one in five non-cases. None of the remaining symptoms were commonly reported in the non-cases. Loss of confidence or low self-esteem was the next most common in 6%. Fatigue was reported by only 1% of non-cases suggesting that in the majority of instances severe fatigue is associated with depression. Somatic symptoms were very uncommon in non-cases.
Individual depressive symptoms and episode severity
Symptom frequencies were calculated for confirmed cases classified according to severity (Table 2). The symptoms of self-reproach and guilt and psychomotor agitation and/or retardation increased in frequency from rates of less than one in four in mild depression to over two in three of those with severe depression. Appetite disturbance with weight change also showed a steep rise in frequency with increasing severity. Loss of pleasure, loss of confidence, diminished concentration, sleep disturbance and suicidal ideation increased with severity, but were also found commonly in those with mild depression. In contrast, early morning wakening and diurnal variation in mood were similar across all levels of severity. The number of somatic symptoms increased with severity of depression, from a mean of 1.3 symptoms (95% CI = 1.0–1.5) with mild depressive episodes to 2.3 (95% CI = 1.8–2.7) with moderate episodes and 3.2 (95% CI = 2.3–4.1) in subjects with severe episodes.
Frequency∗ (%) of individual depressive symptoms in 69 subjects with confirmed depressive disorder classified according to maximal episode severity
Discussion
Good descriptive information on the phenomenology of adolescent depression is sparse [21]. Of young people in this study, 3.5% had had a confirmed episode of depression over the 30 month time frame of the study, with the rate in females over five times that of males. All ICD-10 symptoms of depression were common in cases and, with the exception of depressed mood, all symptoms were uncommon in non-cases. Depressed mood was reported by one in five adolescents without a current depressive episode. Symptoms of particular value in distinguishing cases were loss of pleasure, decreased energy and fatigue, sleep disturbance, suicidal ideation and diminished concentration. It is of particular note that decreased energy and fatigue sufficient to reach the CIDI criterion threshold appeared, in the great majority of instances, to be associated with depressive disorder.
Episodes ranged from mild to severe. Three symptoms; self-reproach and guilt, psychomotor agitation and/or retardation, and appetite disturbance with weight change, showed a very clear rise from low to high frequency with increasing severity of episode and appeared useful markers of severity. A somatic syndrome of depression was relatively uncommon, but strongly associated with a higher severity of episode, consistent with a view of an endogenous (somatic) symptom pattern as reflecting disorder severity [22].
Earlier descriptions of symptoms in adolescent depression have derived largely from small clinical samples, with variable definitions of symptoms and covering a broader age range than the group reported here [10,11,21]. Ryan et al. [23] described 92 adolescent outpatients with depression and, in contrast to earlier studies, found half the subjects had an endogenous subtype. However, as symptoms are related to severity, these studies do not provide an unbiased picture of symptoms in adolescent depression. Robert et al.'s [13] study of a community sample of 44 subjects with major depression is more easily compared to the current study. It is consistent with the current study in reporting that depressed mood, loss of pleasure, diminished concentration and sleep disturbance were common.
The methods used in case identification and definition are strengths of this study. Two different standardised instruments were used to delineate a group with clear-cut depressive disorder. The CIS-R with its focus on recent symptoms is suitable for case identification of current episodes, where lifetime diagnostic instruments may be less satisfactory [24]. The CIDI has been the focus of much psychometric work and is arguably the best-standardised of the available diagnostic instruments. Used together they have defined a core group with depressive disorder that is likely to have clinical relevance [25,26].
The cohort sample was derived from a representative group of Victorian secondary schools, but some limitations should be noted. Early school-leavers, not included in the sampling frame, probably do have higher levels of psychiatric morbidity [27]. However, school retention rates of 98% to year nine for Victoria in the year of initial sampling should have minimised this bias [20]. Non-participation of the targeted sample is a further consideration. Average response rates of over 80% at the first phase were high and comparison of high and low responders revealed no differences on baseline depressive symptoms. Similarly, response rates of 93% at the second phase were high. The inverse weighting procedures partially adjusted for non-participation biases by taking into account second phase participation rates under the relatively strong assumption that non-participants were similar to participants.
The putative influences of age and cognitive development have continued to provoke questions about the applicability of adult concepts and definitions of depression to children and adolescents [21,28]. In this context, our findings provide support for the use of the ICD-10 concept of depressive episode in adolescents. All diagnostic symptoms were commonly endorsed by cases and with the exception of depressed mood uncommon in non-cases. However, this study is unable to comment on the value of symptoms not covered by ICD-10 and the CIDI that may also be of use in defining the syndrome of depression or predicting outcome and treatment responses. Such symptoms may include commonly co-occurring anxiety and behavioural problems [29]. Because the three B Group symptoms (depressed mood, loss of pleasure/interest and fatigue) are required for fulfilling the criteria for severe disorder, they are necessarily of limited value in discriminating disorder severity within the ICD-10 classification. However, the somatic syndrome together with other symptoms typically associated with an endogenous picture (self-reproach and guilt, psychomotor change and appetite disturbance with weight change) were useful indicators of episode severity. Indeed, the symptom profiles were not inconsistent with the view that the somatic syndrome is an indicator of episode severity rather than a qualitatively different disorder [30]. If so, the low prevalence of the somatic syndrome in this adolescent population may reflect assessment at early and less severe phase of a recurrent disorder. It is also possible that the somatic syndrome predicts a higher likelihood of relapse and this underlies a higher proportion of adult depressives with this symptom profile [31].
This paper illustrates the potential for population-based epidemiological studies to inform clinical practice. Most depressive episodes in adolescents are unrecognised and untreated [32,33]. For the primary care practitioner the presence of fatigue, loss of interest and pleasure, sleep disturbance, suicidal ideation and impairment in concentration seem likely to be particularly useful in identifying an adolescent with depressive disorder. Syndromes of fatigue in adolescents have received little systematic study with the current understandings derived largely from case reports, small case series and studies in adults [34–36]. This present study suggests that severe fatigue syndromes in adolescents in the absence of other symptoms of depression are uncommon. Suicidal ideation is a further important symptom. It was also present in a majority of those with depressive disorder, reinforcing a message from previous studies in adults and adolescents about the extent to which it is linked to depression and requires adequate assessment in those presenting with depressive disorder [37,38].
Footnotes
Acknowledgements
The authors acknowledge the support of the Victorian Health Promotion Foundation and the Australian Rotary Health Research Fund.