
Abstract
Over the last decade, schools have increasingly been the target of strategies and interventions designed to improve young people's mental health. Greater school retention rates mean that more young people are in school for longer. In school settings, they are seen as being more accessible than in their family settings or in their community or leisure environments. Hence, in the development of strategies to address the mental health and wellbeing of young people, the role of workplaces, sporting organisations and leisure industries (for example) in promoting practices and attitudes that enhance young people's mental health is often overlooked. Despite some recent positive contributions of the media to young people's attitudes regarding mental illness (e.g. in the Australian television series ‘Home and Away'), schools bear the weight of the youth mental health promotion agenda. This weight does not necessarily reflect the reality of schools' impact on young people's lives.
Conceptualising the role of schools in mental health promotion
The tendency to focus solely on schools as a site for mental health promotion is reinforced by an approach that conceptualises school programs as ‘interventions’ occurring within contained systems. The focus on proving the ‘effects’ of mental health programs (for example, through attempting to develop evidence based on the model of randomised, clinical control trials), inevitably obscures the significance of the broader life patterns of young people. These patterns include the interactions that occur between part-time work, family relationships, leisure interests and activities and school factors which enhance or inhibit wellbeing.
Hence, the question what role does school have in the promotion of mental health in young people? MindMatters has been developed with the understanding that it is indeed part of the ‘core business’ of schools to promote the mental health and wellbeing of their students (and personnel). There is increasing recognition that psychiatric problems are not uncommon in young people. Early intervention offers an opportunity to improve mental health outcomes, including the shaping of more positive attitudes to mental health. It is recognised that schools are only one of many places where the environment affects young people's wellbeing. Hence, the program has been developed to work in an organic way with schools and school communities. It builds on the multitude of practices that are already in place to promote young people's wellbeing and to strengthen schools' roles in the building of social capital, to build a sense of community for all involved with the school and to foster of a sense of belonging (for young people, their families and school personnel). This concept is articulated in the concept of ‘Health Promoting Schools’: ‘Strengthening life-skills and resilience, fostering a supportive school environment and a school culture which encourages partnerships between school and community within a comprehensive program is one pathway to promoting mental health and wellbeing among young people’ [1].
Strengthening the school's role in promoting mental health involves supporting teachers to feel confident of their own areas of professional practice and assisting them to identify the specific areas where specialised professional support from health professionals is needed. Understanding the outcomes of mental health promotion through schools involves recognition that schools are only one part of young people's lives. Although schools provide an attractive setting for health promotion and for health interventions, it is simplistic to ignore the role of other areas of life in which young people's mental health and wellbeing is shaped.
For these reasons, the MindMatters project is influenced by the model of school change developed by the World Health Organization. The triangle describes four levels at work in a whole-school approach (Fig. 1). The widest part of the triangle represents the emphasis which the whole-school approach places on creating an environment which is ‘health promoting’ for all participants. This level involves the entire school community; the quality of the relationships with parents, students and with community agencies; the school ethos and the nature of school policies. The MindMatters project places a strong emphasis on this level of practice. It provides a framework within which schools can identify their strengths and adapt and improve on current practices.
The World Health Organization's four-level, whole-school approach to school change.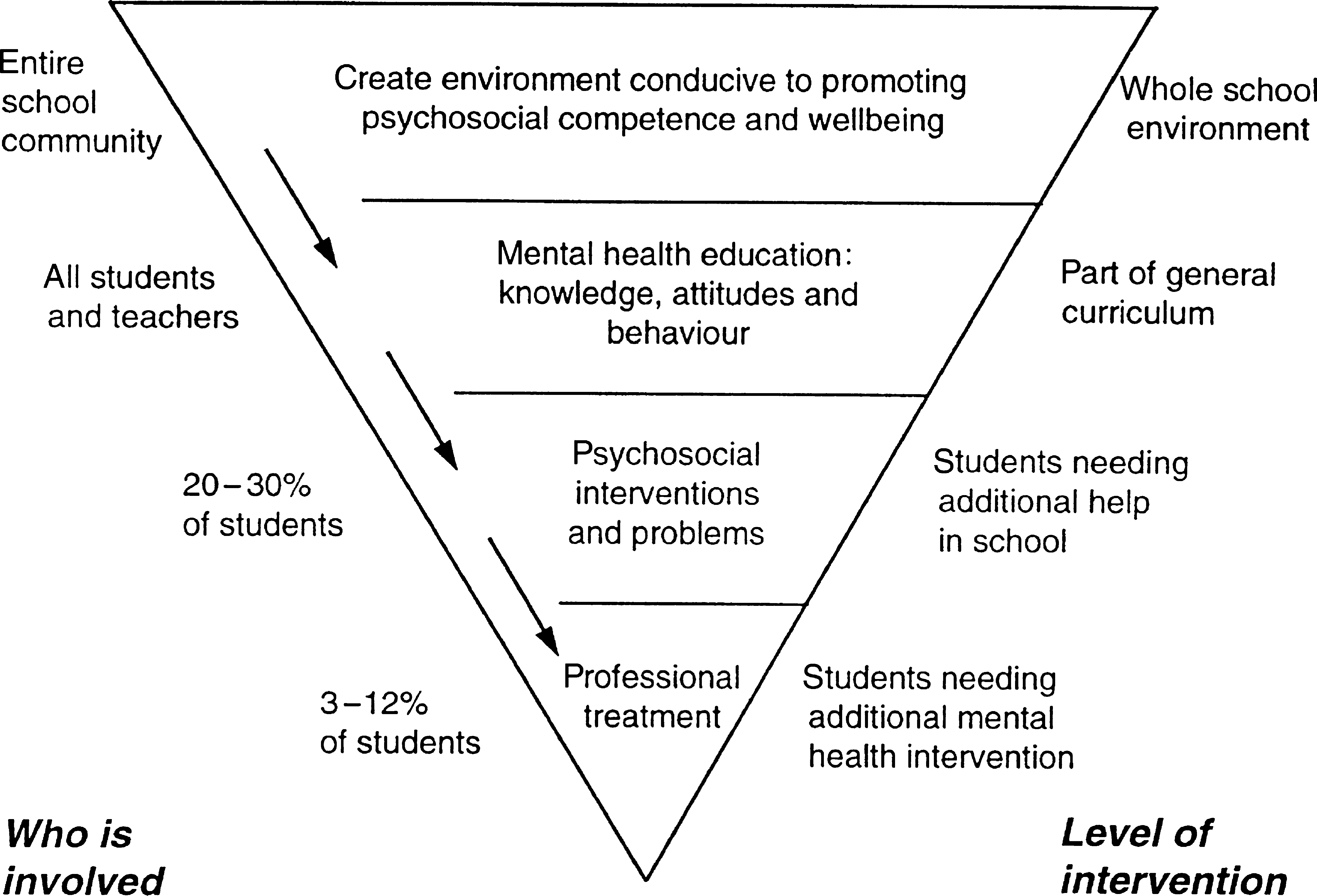
MindMatters draws on the framework of a comprehensive approach to health in schools, developed by the Health Promoting Schools movement. MindMatters involves schools in a structured process leading to an understanding of their particular strengths, gaps and needs in three areas or ‘spheres’ of practice: curriculum, teaching and learning; school organisation, ethos and environment; and partnerships and services. All spheres interact to create ‘health-promoting’ school environments (see Fig. 2). Collaboration between teachers, parents, students and the wider school community is a key process in developing a healthpromoting school.
The interacting spheres of a healthpromoting whole-school environment.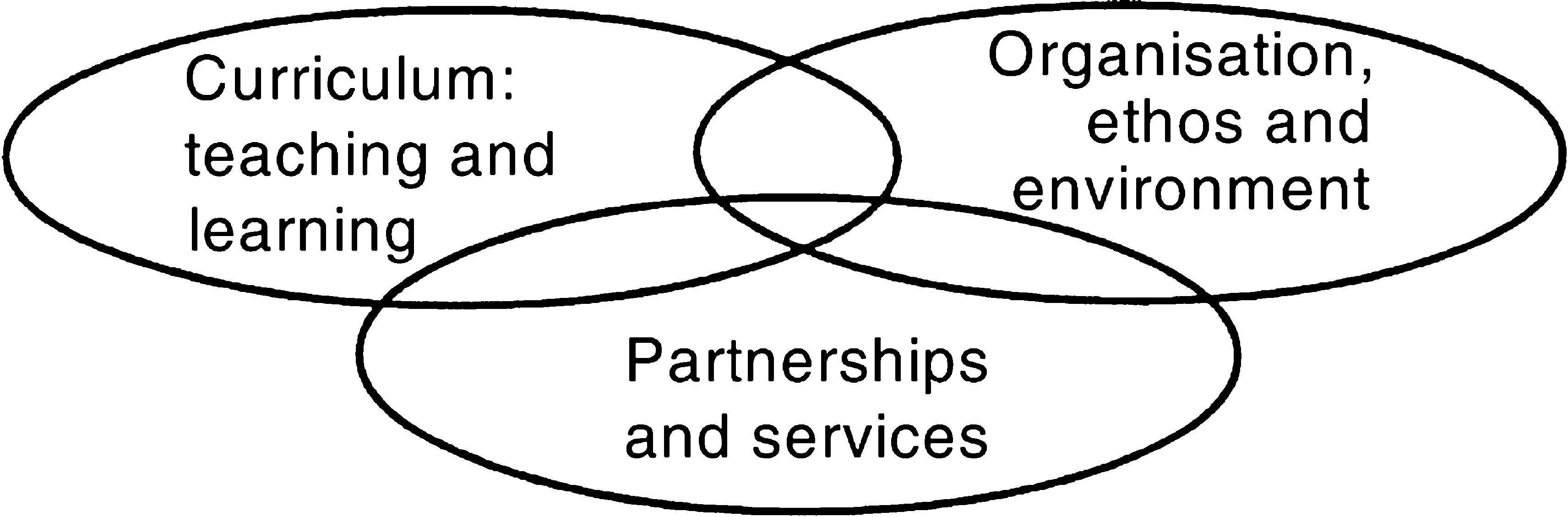
Thus mental health promotion is much more than simply inserting curriculum materials into health, English or other curriculum areas. Schools committed to the welfare and learning of their students are addressing the following questions in all areas of the school's performance:
How can we provide a safe and supportive environment in which all students can maximise their learning? How can we remain accessible and responsive to their needs? How can we assist our students to develop their ability to cope with challenge and stress?
There are many ways in which schools can address these questions. The almost infinite variety of school settings and contexts means that there is no blueprint for exemplary practice. The MindMatters project team found that even schools in similar circumstances chose to focus on different dimensions of mental health promotion. For example, two schools in relatively similar metropolitan areas chose to approach the implementation of MindMatters in very different ways. One identified bullying and harassment and, in addition to addressing this issue in the classroom, developed and performed a play on the issue using the arts as a vehicle for health promotion. The other school focused on enhancing resilience, connected with parent groups and involved the whole school and local service providers in a forum promoting awareness of mental health.
The key issue was that these schools were able to establish mental health promotion as a focal point for their endeavours. It reflected an ethos within which schools were able to draw together many activities.
School personnel also ask ‘How can we identify those students in particular need of assistance or support?’
The lower parts of the triangle presented in Figure 1 pertain to this question. Educators in a healthpromoting school face the difficult task of enhancing the wellbeing of all students, and at the same time, being able to identify those students with special needs, and those ‘at risk’, who would benefit from targeted interventions. Here, the relationship between the school and outside agencies is important. A range of programs and interventions are available which address the needs of students with special needs, such as those with eating disorders, depression and bipolar disorder students suffering loss and many others. MindMatters provides schools with a structured process through which educators make choices about using available interventions or programs.
MindMatters: an innovative approach
The MindMatters program represents a significant shift in thinking about mental health promotion. Rather than providing yet another ‘intervention’, MindMatters is designed to provide a framework that integrates existing mental health education and health promotion interventions and initiatives. It provides the first comprehensive approach to the promotion of mental health for young Australians, through school programs.
The development of the program involved the collaboration of health and education experts, with the support of a reference group of recognised mental health education and prevention professionals. Mind-Matter was developed during 1997, drawing on current knowledge about exemplary practice in education [2]. It is grounded in the understanding that the professional development of teachers is fundamental to the success of any innovation. This means developing supportive structures within schools and between schools and their communities, as well as providing teachers with up-to-date knowledge about practice. The curriculum materials are based on the understanding that young people need to engage actively with ideas and concepts in order to learn. The classroom materials frequently place the student at the centre of activities, positioning the teachers as a facilitator.
For this reason, the curriculum units and teaching processes are designed to assist in teaching for as well as about mental health. Many of the sessions use experiential and interactive teaching strategies to promote learning and skills development. These activities can introduce a level of fun and vitality into the classroom and at the same time require students to cooperate and communicate in order to address the challenges inherent in the task. Guided discussion is used to assist students to move from an experiential to a reflective mode. Discussion and processing of the activity assists students to develop concepts and language with which to further examine and share their experience and to move to a level of conceptualisation and awareness which would be difficult without a concrete or experiential base.
The MindMatters program consists of a professional development program, and materials for use in schools. The materials consist of a booklet that provides the basis for establishing a whole-school approach, suicide prevention guidelines and an annotated bibliography. They include an audiovisual resource on understanding mental illness and a resource entitled Mapping and Managing MindMatters, which provides information on the process for establishing a whole-school approach. For the classroom, the materials include resources to support programs in four areas: enhancing resilience, dealing with bullying and harassment, grief and loss and understanding mental illness. In addition, the draft suicide prevention guidelines were trialled.
The program is also innovative because it is conceived and implemented on a national scale. MindMatters has been tested extensively, in a range of schools in all systems and all States and Territories. Twenty-four pilot schools were selected, through a process of consultation with school systems, to provide a balance of schools from government, independent and Catholic schools and to ensure a representation from rural and remote areas of Australia, as well as from metropolitan and regional areas. An important criterion for inclusion was the commitment of the school to addressing mental health education and promotion, through the identification of a team of staff who would take responsibility for the project, including the school principal.
Pilot schools trialled the program during 1998, supported by members of the MindMatters project team. Initial visits provided support for the first step in the process: an audit of the school's policies, practices, programs and partnerships in the broader mental health area. Schools identified their areas of concern and priority for attention as part of this audit. In this way, the program is able to provide a framework for the school to address its own needs. This feature of the program means that all schools will shape the program in their own way. From the point of view of evaluation, this means that there were effectively twenty-four programs in operation. Here, we provide a brief description of the way in which the program was trialled in schools.
The model for piloting the program placed strong emphasis on teacher professional development, and, at the same time, on the provision of a minimum level of support for teachers in their schools. The trial provided important information about the sustain-ability of the program under normal conditions.
Teachers reported that the process of conducting this audit was a good introduction to the Health Promoting Schools framework and assisted them to conceptualise the importance of taking a holistic approach to mental health promotion in schools, as these two examples from the pilot schools illustrate:
It helped us to realise we were already doing a lot of things we hadn't regarded particularly as being about mental health promotion and focused us on just how everything interconnects to make a whole. (Western Australia, rural)
The audit got us to look at all of the areas of the school and we were able to pick out the gaps in our approach – at the same time as telling us we were already doing some things – and doing them very well. (Western Australia, urban)
During the first visit to their schools, MindMatters team members provided 2 days of professional development activity, introducing the Health Promoting Schools concept, and assisting with understanding the Managing and Mapping MindMatters portfolio.
School were asked to form a core team of at least four members (one of whom was a member of the executive) to manage the project and were allocated a small budget from the project funds. The core teams had an initial task of forming a support group of potential partners and advisers such as local health or youth services, parents, student representatives and indigenous or ethnic advisers.
Some schools had these teams in place for the initial 2-day workshop. Others were not able to form such teams due to difficulty in generating local support and/or inaccessibility or overload of local health services. The issue of ‘overload’ was a continuing theme in several schools, either because the distance between schools and services was too great or because lack of funding made existing services too busy to add another commitment.
Each school established its own priorities for whole-school action, with most schools using staff briefings to promote awareness of the project and to enrol support. A number of schools provided professional development for all the staff on a specific mental health issue using the MindMatters team as trainers. In addition, each school agreed to trial at least one of the curriculum units and identified their areas of interest from the four themes of enhancing resilience, dealing with bullying and harassment, grief and loss and understanding mental illness.
Subsequent to the initial visit, funding was provided to schools in order to send two teachers to professional development workshop. Some used their own resources to send extra teachers, indicating a level of investment in the program. They received 2 days and two evenings of intensive training in the research and theories underpinning the practice, use of the curriculum materials, and issues contained in the suicide guidelines. Time was also allocated to help develop a school-based action plan.
Over the ensuing terms the school piloted the curriculum units of their choice and continued to work at their school-wide activities. The majority of schools piloted a number of units. Although the units were developed for use in health, English, drama, study of society or psychology classes, many schools opted to use components of the health units in pastoral care programs or in religious education.
Schools engaged in a range of activities as part of their whole-school strategies. These included activities as varied as running youth forums; mental health days; making dramas and videos around the theme of bullying; conducting school-wide team building games; addressing staff mental health needs via the conduct of staff surveys; drafting policy and practice guidelines regarding incidents of bullying or harassment; organising parent forums; revising referral protocols and enhancing transition and peer support programs.
At the end of the first year, when schools had already trialled the program, an evaluation workshop was held, attended by members of teams from each of the 24 schools. The purpose of this workshop was to provide a formative evaluation data for revision of the program. Here, teachers identified the support of the executive as the single most critical factor in the success of the program. Significant involvement of the school leadership personnel was required to address the school-wide focus called into play by the Health Promoting Schools framework. The professional development and curriculum materials provided by MindMatters was also identified as very important to the efficacy of the program, as was the use of a core team structure to drive and manage the project, the development of a critical mass of staff support and the guidance of a member of the consortium.
Those schools that were able to engage the support of community or health agencies found these links contributed significantly to their efforts. Many schools, due to their remote or rural placement, were not able to build these partnerships and identified the lack of access to services as an area of concern, particularly in regard to referral of at-risk students or staff. Contact with other schools engaged in similar work, use of existing school structures such as student councils, peer support or pastoral care programs, and provision of a budget were also identified as factors contributing to the efficacy of their work.
The workshop revealed that the curriculum units were very favourably received and widely used, a finding confirmed subsequently by the external evaluation [3]. Teachers reported that students responded well to the interactive techniques and issues offered for exploration. For some staff, teaching in this way was a departure from regular practice; professional development was identified as most important in encouraging teachers to extend their repertoire. Teachers reported varying degrees of success in sharing materials or providing in-house professional development for fellow staff. A number of teachers commented that their own knowledge and awareness of mental health was augmented as a result of their participation in the project, in particular their knowledge about mental illnesses and their awareness of what their students perceived as the more stressful or challenging components of their lives. After receiving training in the use of the curriculum materials, many teachers commented that they had been ‘least familiar’ with mental illness, and ‘I feel a lot more comfortable with the whole notion now’. In particular, teachers appreciated ‘getting some precise information about the different types of illnesses and some new teaching methods’. Working with one issue enabled schools to start the process of whole-school change. For example, one school reported that the use of the ‘Bullying Survey’ provided a focus for changing ‘the way we do things in the school’.
Teachers identified that the greatest challenge they met in dealing with the MindMatters project was in addressing a whole-school approach. Adopting a classroom program need only involve engaging the commitment and skill of the teacher. Addressing school ethos and environment, policy and practices and developing or extending partnerships with parents, community groups or health agencies requires direction of time and energy to work with others. This big picture approach entails large-scale change, which takes time and commitment to drive. Previously, it was often seen as activity above and beyond the prime duty of teaching class or contributing to student or faculty management, however, the MindMatters project found that the provision of a safe and supportive environment was seen to be important and part of the core business of a school. Despite this, core team members encountered many comments which indicated barriers to the implementation of mental health education. For example, some teachers felt that too much is expected of schools and teachers and that resourcing for welfare staff is not sufficient. It was common for teachers to say that health education is often marginalised by the competing concerns and limited time available within schools.
Two national organisations, the Australian Principals Association Professional Development Council and the Curriculum Corporation, have been contracted by the Commonwealth Department of Health and Aged Care to manage a national dissemination of the MindMatters resource and the associated professional development over a period of 2 years. The MindMatters resource and a 2-day professional development program will be available to all schools with secondary students who opt to participate in the project.
Discussion: the contribution of MindMatters to mental health promotion for young people in schools
The project has highlighted the tension between the educator's core work of providing the most productive environment for all students, and the health professional's interest in providing treatment for selected young people who are defined as ‘at risk’.
The need for mental health support in schools is so great that there is a temptation (seldom resisted) to ‘do’ mental health by bringing in an ‘expert’ for a session or two, or by including mental health in a part of the curriculum in English or health education, with no relationship to whole-school processes. Health professionals are as much implicated in this process as educators are. The effect of this limited, intervention approach is that the school environment does not shift towards the prevention of ill health or the promotion of wellbeing.
Recently, Syme [4] and Marmot [5] have raised this issue in relation to the conceptualisation of epidemiology more generally. Their arguments are relevant to the promotion of young people's mental health and wellbeing because they suggest that the treatment of ill health and disease is missing the most important point if the social causes of ill health are not addressed. As Syme argues [4, p.463]:
…every time we helped a man in the Multiple Risk Factor Intervention Trial to stop smoking, on that day, probably one or two children in a schoolyard somewhere are taking their first tentative puffs on a cigarette for the first time. So, even when we do help high-risk people to lower their risk, we do nothing to change the distribution of disease in the population because, in one-to-one programs such as MRFIT, we do nothing to influence the forces in society that caused the problem in the first place.
Marmot [5] refers to this dilemma as the ‘prevention paradox reversed’. The ‘prevention paradox’ is the observation that a prevention measure that brings large benefits to the community (for example, comprehensive professional development in mental health education for teachers in rural schools) offers little to each participating individual (many students may not notice the incremental differences in the school climate). The prevention paradox reversed is the observation by Rose that ‘when many people each receive a little benefit, the total benefit may be large’ [6].
The whole-school approach used in MindMatters operates primarily at this level. It aims to bring ‘large benefits’ to school communities, enhancing the development of school environments where young people feel safe, where they belong and where they develop the skills needed to participate fully.
The focus on the social environment in promoting mental health parallels the work of Durkheim, one hundred years ago in which he explored the relationship between alienation and suicide [7]. Durkheim put forward the argument that suicide is directly related to the social conditions pertaining in a society and that different milieu will produce different suicide rates. Contemporary researchers refer to the need to address the alienation of young people from school and from society also drawing attention to the public or social dimensions of individual wellbeing [8]. As Hassan points out, it is important to understand both the social and the psychological factors which contribute to mental health, mental illness and suicide [7].
MindMatters has demonstrated that a whole-school approach provides a framework for enhancing young people's mental health in the school setting. It provides a framework within which educators can provide curricula to develop skills and educate young people about mental health. This framework is designed to identify targeted interventions which provide support and referral for the small group of young people who have serious mental health conditions. For school communities, the key issue is to ensure that the balance between whole school and targeted elements of mental health promotion is right.
The balance is difficult to attain in practice, and it is reflected in a tension within the mental health education literature. In particular, discussions of evidence reveal a tension between targeting of specific mental health problems and the provision of a health-promoting, whole-school environment. For example, Whitehead asks ‘How effective is health education?’ [9]. She concludes that most health education takes place in situations where people or communities ‘can't be randomised, where “controls” cannot be prevented from acquiring health information intended exclusively for the experimental group, and where external factors may act differently on subgroups within the population’. Whitehead argues that, because there is a priority given to measures of effectiveness that involve an experimental design, of necessity, relatively smallscale interventions are most likely to be measured. She points out that while these targeted interventions are of value, they do not shed light on the cumulative effects of interventions and broader policy changes over extended periods of time. Nor do they provide crucial evidence of the sustainabil-ity of programs in the longer term.
The top layers of the health-promoting schools triangle (Fig. 1) consist of just such broad, communitybased and long-term strategies. They are difficult to measure according to traditional health research criteria because they draw on processes that have more in common with community development than medical science. Measurement techniques common in epidemiology (measuring health outcomes over large populations) may be useful in assessing the evidence of outcomes from whole-school approaches, but they need to be used in conjunction with those more common to other fields, such as policy analysis, organisational change and youth studies. Because of these complexities, a recent review of research on school health promotion programs found that while there was ample evidence of the effects of narrow intervention programs which focus on specific health issues (such as alcohol, drugs or smoking) there has been little research on the effects of the Health Promoting Schools program [10].
For these reasons, the lower two levels of the triangle presented in Figure 1 are those more commonly referred to in the literature on health education. An example is the review of ‘effective mental health promotion’ by Hodgson, Abbasi and Clarkson [11]. Their review limits the notion of ‘effective’ to limited interventions that target particular groups and that have been measured through the classic method of intervention and control groups, with no consideration of whole-school approaches.
The MindMatters program places the emphasis on the promotion of the mental health of all young people within the school community. The promotion of mental health in young people through schoolbased programs should be seen as a significant component of a wider mental health promotion strategy that addresses young people's full life patterns and that will have sustainable outcomes.
Whole-school approaches, such as the Health Promoting Schools framework, are a key to youth health promotion because they offer the potential to develop more integrated community responses to the needs of young people. There is a steady shift towards the establishment of sustainable links between schools and local agencies, through youth focused services, full-service schools and many other initiatives. MindMatters is conceived as a program that provides support for this shift. To return to an earlier theme, it is through creating whole-school environments that are conducive to wellbeing and connecting with communities that schools will become the key to addressing the mental health of all young people, across all dimensions of their lives.
Footnotes
Acknowledgements
MindMatters is funded by the Commonwealth Department of Health and Aged Care, Mental Health Branch, under the Community Awareness Program and the National Suicide Prevention Project. Mind-Matters was developed by a consortium consisting of the University of Melbourne Youth Research Centre (Helen Cahill, Roger Holdsworth and Johanna Wyn), Sydney University Faculty of Education (Louise Rowling), Deakin University Faculty of Health Sciences (Bernie Marshall, Margaret Sheehan and Lawrie St Leger) and the Australian Council for Health, Physical Education and Recreation (Jeff Emmel). Shirley Carson is the project coordinator, based at the Youth Research Centre. The consortium thanks the support and enthusiasm of teachers in each of our twenty-four schools.