
Abstract
The wellbeing of adolescents has long been of interest in the fields of psychiatry and developmental psychology, with a recognition that the biological, psychological and social transitions of the teen years are commonly accompanied by emotional difficulties. Until recently, however, adolescent emotional wellbeing has received little attention from policymakers in government and the broader health community [1]. In the past decade much has changed and adolescent mental health is now high on the health agenda. There are several reasons for the change. First, community surveys have documented that mental health problems in adolescents are common, with around one in five experiencing some form of emotional disorder. Major disorders are also common, with the prevalence rates of depressive disorder highest in the late teens and early twenties [2–4]. Second, time-trend data suggest that adolescent mental health has not improved. Upward secular trends are most apparent for suicide in young males, alcohol and drug abuse, but are also apparent for depressive disorder. As yet poorly understood, but potentially reversible, socioeconomic influences are presumed to underlie these trends. This line of speculation has brought consideration of the modifiability of social influences through preventive and health promotional work [5–7]. Third, the overall importance of mental disorder in the public health agenda has grown with a recognition of the substantial burden of disease associated with depression and other common mental disorders [8]. By the year 2020 depression is predicted to lie second only to ischaemic heart disease as a cause of disease burden in the developed world [8]. The scale of the problem has driven a search for innovative public health responses, including exploration of the scope for early prevention. Given the extent to which these problems have their first manifestations early in life, mental health promotion in children and adolescents has been at the forefront of considerations.
Attachment theory as a conceptual framework for mental health promotion in adolescence
John Bowlby's work on attachment theory has continued to influence clinical and developmental perspectives on the relationship of the social environment to emotional wellbeing [9]. Bowlby hypothesised that anxiety and depressive symptoms were most likely to arise at times when social and interpersonal bonds were threatened, or in individuals where patterns of interpersonal attachment were poorly developed or insecure. Recent work on the effects of life events, social support and disruption of social relationships has to a large extent affirmed Bowlby's views. It has also illustrated the complexity of links between social attachments and emotional wellbeing. Undoubtedly, experiences of loss, adversity and disruptive life events are associated with emotional distress and mental disorder. However, the quality of the social environment also has the capacity to influence mental health in a variety of ways. The extent to which an individual has robust social ties is likely to have a direct influence on self-concept and sense of belonging, and, in turn, reactions to social stressors [10]. Conversely, the experience of ongoing insecurity and threat has a detrimental effect on emotional wellbeing. An individual's capacity to deal with adversity is in part dependent on the availability of support in the immediate social environment, as well as the skills he or she has for making appropriate connections at times of stress. Lastly, the quality of an individual's engagement and participation with supportive others may in part determine the likelihood of experiencing emotionally hazardous events with their subsequent effects on mental health.
Similar themes are found in studies of social influences on mental health problems in young people. A sense of security and trust in others appears fundamental. Social and familial settings in which abuse and victimisation occur are associated with high levels of mental disorder [11]. A sense of connectedness, good communication and perceptions of adult caring have emerged in studies of schools and families as being related to a wide range of behavioural and mental health outcomes [12]. Last, a sense of active engagement and broader participation in a range of contexts has emerged as an important characteristic of more positive social environments with benefits in terms of self-regard [13]. The relationship of these three constructs to an individual's perception of a sense of belonging underpins the Gatehouse Project's conceptual framework and is illustrated in Fig. 1
Theoretical framework for the Gatehouse Project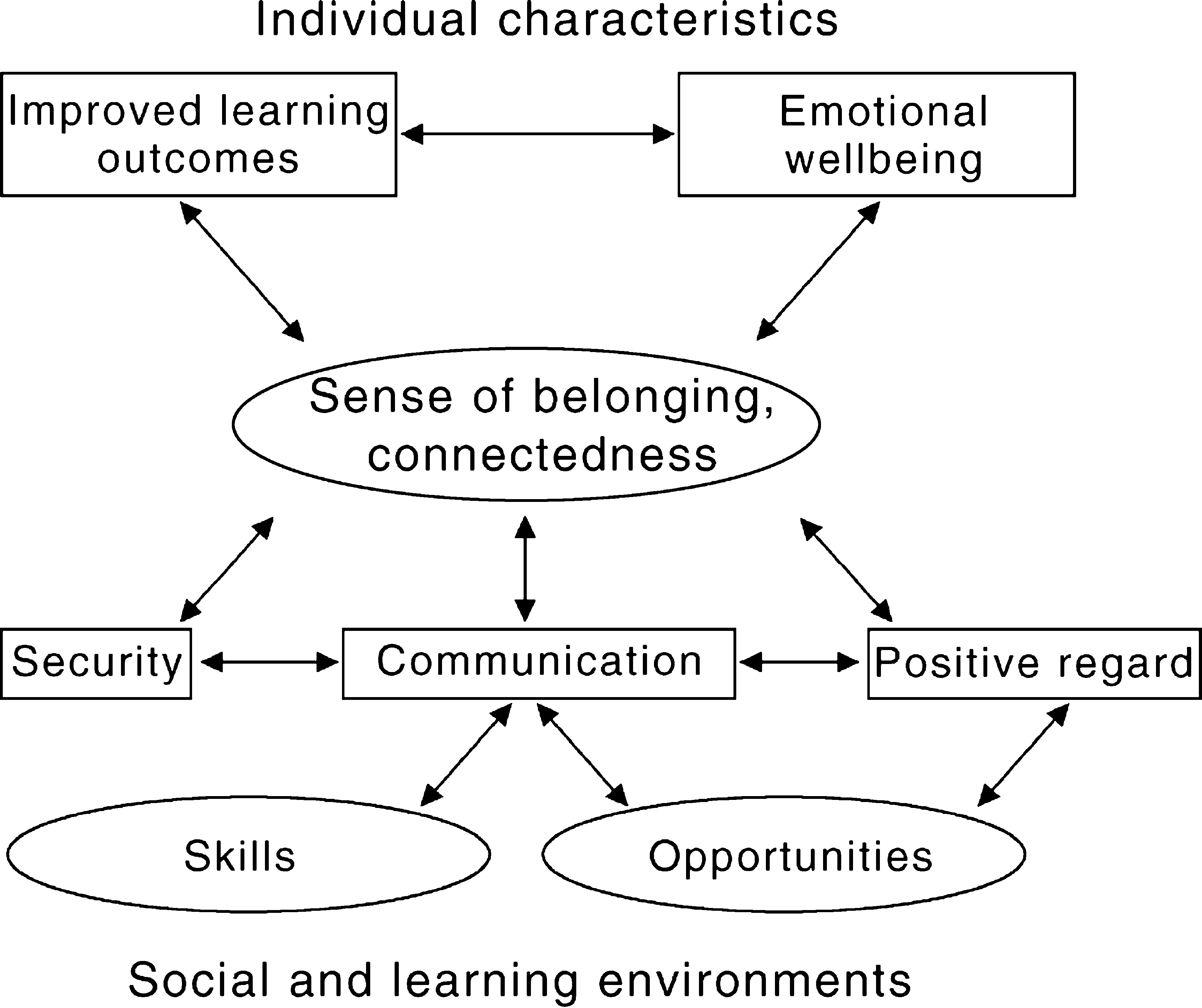
Schools as a setting for adolescent mental health promotion
There are sound reasons to consider schools as a setting for mental health promotion. They are arguably the only point of close-to-universal access to young people at a time during which emotional problems and behaviours with long-lasting, harmful effects on health commonly emerge [14]. More importantly young people spend close to half their waking hours in school and inevitably the quality of experiences with teachers and peers in that setting will affect emotional wellbeing [15]. Finally, transitions in education are among the most significant events in the lives of younger adolescents. The transition from primary school to secondary school brings a loss of continuity in relationships (teachers and friends), changes in curriculum and teaching styles as well as adaptation to a different secondary school culture [16].
Schools are settings where there has been much controversy about their purposes, responsibilities and effects on young people. Some early research raised doubts about whether education even made a difference, given social class, family and other social conditions. Rutter and his colleagues, in the landmark Fifteen Thousand Hours Study [15], identified substantial differences between secondary schools in a range of student academic and behavioural outcomes. Most importantly, they concluded that these differences were largely a result of schools' characteristics, their organisation and climate, not differences in the intake of students. They stressed the importance of the quality of the social relationships and the school as a social institution. Subsequent work on school effectiveness and school improvement has explored the impact of more specific school and classroom characteristics which influence student engagement in learning and social development [16–18]. Relationships between teachers and students in classrooms, opportunities for student participation and responsibility, and support structures for teachers consistently emerge as associated with student progress.
There are signs that health and educational agendas are converging. There has, for example, been an increasing interest in the forms of schooling that might best meet the educational needs of early adolescents [16,19]. The call for reform and restructure in the middle years of schooling (10–15 years of age), has been driven by the identification of alienation or disengagement of young people as the major barrier to educational success in the younger teens [16,20]. The extreme consequences of alienation are seen in young people who ‘drop out’ of school or have high levels of truancy or absenteeism. This same group are those that commonly have the worst mental health outcomes. The proposed solutions on the education side have been the promotion of a school environment or culture which enhances a sense of belonging, including more supportive relationships with teachers, opportunities and skills to make a valued contribution to school life, a sense of security and the availability of close and positive relationships [16].
The understandings from such research into school education reform and improvement have guided the strategies for promoting mental health in the Gatehouse Project. The aim has been to avoid piecemeal ‘add-ons', but rather to support those practices that are sustainable and institutionalised. We have drawn on three key areas emerging from this literature, which point to aspects of a school's functions, structures and culture. These are: (i) school social and learning environments; (ii) content and implementation of school curriculum; and (iii) linkage between the school and its community.
More specifically, in each of these areas the focus is to enhance young people's sense of security and trust, sense of social connectedness with teachers and peers and opportunities for meaningful and valued participation in school life.
These aspects of schooling are modifiable and under the school's influence, but to initiate change, schools need to be convinced of the relevance of and need for change, consider the readiness of the staff to become involved and be prepared to allocate school resources, including time [21,22].
The Gatehouse Project: enhancing the quality of social and learning environments
The Gatehouse Project brings together a team at the Centre for Adolescent Health with backgrounds in education, psychiatry, welfare, psychology and public health, in partnership with school-based teams in 12 secondary school communities in metropolitan and regional Victoria. The primary aim of the project was to prevent or delay the onset of depressive symptoms through the promotion of a more positive school social environment. The project has developed a whole-school strategy, to build the capacity of school communities to promote a sense of wellbeing and address the common emotional needs of young people. Importantly, the strategy seeks to make changes in the schools' social and learning environments, introduce relevant and important skills through the curriculum and strengthen the structures within the each school which promote links between the school and its community.
Three interrelated strategies underpin the whole school intervention: (i) the development of a school profile; (ii) the establishment and support of a school-based adolescent health team; and (iii) the identification and implementation of feasible and effective intervention strategies.
Development of a school social climate profile: assisting school communities to develop priorities
Much health promotional work already takes place in schools to address the wellbeing of students. Little of this work is coordinated or sustained. Such initiatives may arise as a result of changes in government or educational policies, the interest of a particular member of staff, or because a local health agency has an interest in a particular approach. Most take a single-issue focus with short-lived support. They are frequently perceived as extras and remain in fragmented pockets in the school. One result has been a perception that such health initiatives increase the workload and stress of teachers.
There are other reasons to be sceptical about piecemeal approaches. Research in schooling points out that each school's context is unique and therefore there can be no blueprint proposed for all schools. Such single-focus initiatives may or may not address the major areas of importance in a particular school. These considerations led to the development of a more comprehensive needs analysis for schools. The Gatehouse Project has done this by providing each participating school with its own social climate profile. These social climate profiles of schools were developed using questionnaire data from students, extending a strategy pioneered in earlier work [23]. The questionnaire addressed the three targeted areas of social interaction: security, social connectedness, and gaining positive regard through valued participation. The school climate profile was initially derived from year 8 students (13–14-year-olds) prior to commencement of the program. The derived profile was compared with comparison schools not participating in the study intervention. Each intervention school was provided with a profile of their students' responses to the key areas.
The school-based adolescent health teams were able to use their school profiles to determine priorities for action. There have been multiple starting points, and, indeed, there are no quick fixes but rather planned processes of change with each school choosing and adapting strategies which are appropriate to its own context.
Identification and support of a school-based adolescent health team
An over-arching challenge for the project has been to integrate mental health promotion into core areas of school life. This entailed the development and implementation of relevant school policies, coordination of pre-existing programs, professional development of teachers and bringing about changes in school structures and time-tabling to facilitate the involvement and commitment of all staff.
To this end, schools were invited to identify and establish an adolescent health team or equivalent, drawing on staff from the school administration, curriculum, welfare and year level coordinators, as well as personnel from outside agencies linked with the school. In some cases, parents have also been involved. This team draws together staff with expertise and interest to work on issues relating to the health and wellbeing of young people at the school. It takes a formal place within the school's organisational structure, acknowledged and supported by the school principal and leadership team. It provides a focus for linkage both within the school and with the school's local community.
An adolescent health team provides a school with a flexible and responsive structure to address the specific social context in each school. The team can make links between the potentially conflicting initiatives and coordinate appropriate responses in the school. It can define common elements and plan responses that involve systematic professional development and strategic implementation of priorities. This shifts the focus of schools from single issues, teaching and delivering fragmented ‘projects’ and interventions to an approach that allows for a more coordinated response to identified priorities. Furthermore, the school-based health team allows for a clearer point of contact to strengthen the connections with relevant community agencies and use community resources for health promotion.
The Gatehouse Project staff from the Centre for Adolescent Health supported the work of the adolescent health teams in schools. The Centre staff consisted of educators with experience of secondary school teaching, student welfare, professional development and curriculum design. They acted as ‘critical friends’ and professional development resources in each of the project schools [24]. The role of ‘critical friend’ has both a formal and informal dimension. The formal dimension has been one of providing feedback of data, making sense of the data, providing support in the planning of priorities, and training and support in the implementation of strategies with the potential to address specific aspects of the social climate. The informal dimension has involved mobilising practical support, building trust between staff, discussing and raising questions, reflecting on actions taken and helping maintain the momentum.
Promoting school social and learning environments
The development of a collaborative culture between curriculum, student welfare and administration areas, facilitated by the adolescent health teams, provides a powerful means for enhancing the quality of social and learning environments [16,25–27]. The two main areas that the teams focused on were the social climate of the school as a whole and the promotion of positive classroom climates.
Whole school social climate
The actions taken by schools in response to their school profiles have varied. Examples have included the adaptation of guidelines for responding to and preventing bullying, introduction of mentoring programs for students with specific needs, the use of peer support and peer leadership strategies and increasing the opportunities and skills for students to participate in decision-making at all levels of the school.
Schools have taken a pro-active stance on preventing bullying by developing policies and procedures and training all staff and students in those procedures. Much of this focus has been on the more subtle forms of bullying that take place, such as being deliberately left out, having rumours spread and being teased. Young victims may be distressed and teachers are often unsure about how to deal with the situation and avoid making things worse. Pikas' [28] method of shared concern has been an important element of the professional training of teachers, and has proven useful for teachers approaching and discussing conflicts with a young person, not just incidents of bullying.
Schools provide many and diverse opportunities for student engagement beyond the standard curriculum. Schools have examined which students have opportunities for participation to ensure that individual students are not excluded, and participation potentially involves the majority of students [11]. They have undertaken a systematic development of school-wide strategies of ensuring age-appropriate means for rewarding and recognising achievements academically, in sport, socially and in other relevant areas [29]. For students, this has offered greater opportunities for developing positive attachments to individual teachers and allows for experiences of success in the school environment.
Classroom climate
The Gatehouse Project has incorporated two broad approaches to promoting a positive classroom climate: clear classroom management and the development of more interactive teaching styles. Classroom rules have been negotiated between teachers and students and are displayed in each classroom. Examples of common rules which emerged were ‘no put downs', listening to others' points of view, and treating others' belongings with care.
Positive teacher-student relationships, and student-student relationships have been enhanced through the use of small group work, class discussion and interactive teaching strategies. The value of using questions to open up discussions and facilitate looking at ideas from different perspectives has been emphasised. Teachers were encouraged to maintain a ‘not knowing’ or inquisitive stance and to listen to and facilitate an exchange of differing points of view and opportunities to challenge and debate ideas. Where appropriate, acknowledgement of the value of all student contributions was promoted. This included authentic displays and presentation of student work to ‘real’ audiences such as parents, other students and teachers, and members of the community. However, change in instructional practices takes time and, as Fullan [30] has noted, the change in the culture of teaching toward greater collaborative relationships among students and teachers is the ‘hardest core to crack'.
As the focus of schooling has broadened, so too has the breadth of innovation and change. More and more is being expected of schools while, at the same time, schools themselves are undergoing changes in management arrangements, accountability processes, curriculum standards and work practices. In turn, teachers' work has intensified [16]. Not only are they working with young people whose needs are complex and diverse, but also the demands, expectations and workloads of teachers have increased.
An important factor emerging in the Gatehouse Project is the significance of the school climate for teachers. We have found that, in our strategy for promoting mental health and wellbeing of young people, there has been a need to pay attention to the wellbeing of those professionals who work with them. Similar concerns have emerged in the educational literature where the conditions that surround teaching affect the roles a teacher may adopt in the classroom. Without attention to the support for teachers, the scope for change in the school climate and improvement in classroom practices will be limited [30].
Using the school curriculum in mental health promotion
School curricula have been widely used in preventive programs targeting substance abuse and cardiovascular risk factors. Curriculum ‘packages’ for mental health promotion also appear attractive and, indeed, have been the cornerstone of most mental health educational and health promotional work in schools. However, curriculum-based health promotion strategies alone have a history of limited success in changing individual behaviour, largely because such programs are frequently of short duration, fragmented and focused on the provision of information [14,31]. Programs which extend over a longer period and which address a broader range of cognitive and life skills may, however, bring substantial behavioural gains which persist beyond the school years [32].
The scope for siting curricula for promoting mental health in schools has grown as schools have come to play a broader role in equipping young people for adult life; schools have a greater readiness to promote and foster critical and reflective skills, problem-solving abilities and to encourage collaborative work. These skills have relevance not only for academic and workplace learning, but also for social and emotional development. This broader conception of the role of schools provides the scope for introducing curriculum modules focusing on the cognitive and interpersonal skills underlying emotional wellbeing.
A number of factors were considered in the development of the Gatehouse Project curriculum materials:
Relevance of materials. The perceived relevance of materials to adolescents was a prime consideration in the curriculum design. The materials were designed to address universal rather than exceptional adolescent experiences. The curriculum modules for year 8 students, therefore, dealt with communication in the classroom, dealing with feelings of anxiety or low mood, recognising and re-framing common adverse social experiences (for example, with friends or parents), developing a sense of trust in others and coping with internal and external expectations. Integration within mainstream teaching. The Gatehouse Project curriculum materials were designed to be used by subject teachers, both within English classes and in classes more traditionally concerned with student health and wellbeing (health and physical education, personal development and pastoral are programs). The materials were designed to meet not only health objectives, but also to allow teachers to use the Gatehouse Project curriculum to meet essential educational objectives. Professional development of teachers. A 6-hour intensive program of professional development for teachers was followed by weekly, school-based professional development concerned both with curriculum implementation and development of a positive classroom climate. The professional development of teachers also included a focus on specific teaching strategies relevant to implementation, including the use of small group work, personal journals, and improvisation and role play to promote communication within classrooms. Integration of materials into multiple year levels. The materials were designed for initial use at the year 8 level (13–14-year-olds), corresponding to a time when common symptoms of depression and anxiety are emerging with greater frequency. Shorter programs were developed for use at years 9 and 10.
Linkage between the school and its community
School effectiveness research has focused largely on classroom and school level practices. More recently, the influence of government educational policies, the organisational systems within which schools sit and the linkages to local communities have become much clearer [33]. Consideration of the community context in which schools sit has arguably become more important as adolescents adopt lifestyles, relationships and behaviours that in the past have been more associated with young adults. Various models of linkage have been proposed to meet the health and social needs of adolescents, most focusing on the special educational, social or health needs of students. These approaches offer different advantages in terms of access and coordination of services, comprehensiveness of service provision and linkage between agencies [34].
Unfortunately, schools are not able to meet the needs of all young people, particularly those with backgrounds of disadvantage or other special needs. For a small but important group of students, schools will be unable to provide for their needs despite the provision of a positive social environment and promotion of life skills. The adolescent health team has therefore played an important role in strengthening the linkage between a school and relevant community agencies by providing a coordinating point at the school. The team has the potential to identify particular student needs and locate appropriate resources in the local community to respond. These might include the creation of links with other education and training settings for young people with special educational needs. Such training linkages are particularly relevant for schools with high rates of early school leaving.
Summary and overview
Educational environments are complex systems undergoing continuous and simultaneous changes. Understanding the context in which innovations will take place is crucial in ensuring that the processes that are used to initiate, sustain and institutionalise practices are relevant, feasible and effective.
Much health promotion in schools continues a tradition of short ‘add-on’ programs or ‘projectitis’ [30]. These programs are generally not sustained in schools and contribute, in the long term, to a patchwork of health promotion projects where the latest interesting innovation is taken on without careful or critical assessment. Rather, we need to consider how processes and strategies can be integrated with what is already going on and make long-term changes to the school environment. For mental health promotion, these limitations are compounded by a perception that the focus should be on identification and referral, rather than primary prevention. A problem with such a focus is that, although many young people experience emotional difficulties, most will fall short of meeting criteria for mental disorder. The limitations of many mental health activities indicate the need for primary prevention programs which are long-term and sustainable in school environments. The Gatehouse Project was developed to address these issues.
The complexities of mental health promotion in schools are apparent in this description of the Gatehouse Project. The project continues a tradition of collaborative work between health and education that dates back over three decades. In doing so, it has drawn together elements associated with school improvement and aimed to promote these at different levels of school functioning. It has integrated a range of specific strategies previously shown to be effective in promoting educational and health outcomes. Central facets of the project include its development of comprehensive measures of the school social environment and use of these to focus school responses. The creation of an adolescent health team structure within schools has allowed better coordination of responses within the school and a means of linkage with local communities. At a curriculum level, the development of modules integrated into English and health and physical education streams, with scope for achieving both educational and health outcomes simultaneously, is a further strength which should bring benefits in the integration of the work into the school culture and ultimately, its sustainability.
The research on change in schools and school improvement provides important understandings for conceptualising and operationalising school-based mental health promotion. This understanding of change at the level of practice, and the development of relevant and appropriate strategies, has underpinned the work of the school-based teams in partnership with the project team.
The Gatehouse Project stands to provide unique information on the relationships between the social environment and the emotional wellbeing of young people. More importantly, it outlines a process for building the capacity of schools to promote the social and emotional development of young people. Effective change takes time and will rarely involve only a single strategy. Ultimately, the aim is to promote a school culture that ensures the development of all students across all relevant areas rather than implementing single innovations. Whatever the elements of health promotion adopted, they need to be seen as complementary and bringing benefits in educational achievement as well as promoting well-being for all members of the school community.
Footnotes
Acknowledgements
The Gatehouse Project is funded by Queen's Trust, Victorian Health Promotion Foundation, Department of Human Services, Sydney Myer Fund, Catholic Education Office and the NHMRC. The authors would like to acknowledge the valuable contribution made by the school communities participating in the Gatehouse Project as well as all members of the project team.