
Abstract
Treatment for people with mental illness is becoming increasingly community-orientated, as the accompanying papers describe [1,2]. In Sydney, the location of care for the study patients reported here was changed. This was in accordance with legislation aimed to treat patients in the least restrictive environment possible, and because of the planned closure of a psychiatric hospital caring solely for people with chronic mental illness.
This study has three major components: economic, psychological and anthropological. This paper reports the findings of the economic component of the project. The result of the other components of the study are presented in the accompanying papers [1,2]. The economic results should be considered in conjunction with the other findings, as patients' needs (i.e. satisfaction outcomes) must be adequately met in order for ‘cost of care’ analysis to be relevant. The economic study concentrated on factors including cost collection and analysis, with disaggregation of the hospital costs and prospective collection of costs incurred in the community setting.
Several studies have been conducted in different countries on the cost effectiveness of deinstitutionalisation. A German study found that the average cost of community care was 43 per cent of the cost of hospital care. However, this study also found that with increased ‘later’ discharge to community residences, the costs of care in the community eventually exceeded the hospital [3]. A study from the USA found that not only was deinstitutionalisation less expensive, but that it could also be achieved using financial resources already available and currently being spent in mental hospitals [4]. These studies are of interest but are unable to provide direct comparisons due to their different methods and categories of cost collection, including the treatment of indirect costs.
In England, the Team for Assessment of Psychiatric Services (TAPS) project [5], found that the cost of community care was lower than the cost of hospital care for both the first group of residents to leave the hospital and for the whole hospital population when the analysis was extrapolated. This was based on a 1-year period after discharge and recognised that the long-term costs may increase with higher demands for services for those discharged later. The authors stated three reasons for higher costs for later leavers in the UK. First, the early movers in most hospital run-down programs are less dependent, with fewer symptoms of mental illness, than those who remain behind to move in later cohorts. Second, it is commonly the case that new capital projects are not needed for the first leavers because existing day and residential facilities are as yet not operating at full capacity. Third, although often overlooked, it is possible that the supply price of certain types or grades of staff may rise with the growth of demand for them in the community [5].
Despite considerable deinstitutionalisation in the past 10 years in Australia, there has been no published outcome research. This study reports on the economics of the deinstitutionalisation of a cohort of psychiatric patients who had been hospitalised for many years.
Methods
The hypothesis of the study was that the cost of care for these long-term psychiatric patients would be less in the community than in the hospital. The study was designed to collect only direct costs of care in order that the two care settings could be directly compared. As a comparative study, there was no analysis of loss of productivity due to the illness, nor the cost of transfer of pension benefits to the residents, as these costs were being incurred at a similar rate in both care settings. It concentrates on a comparison of the costs of appropriate service provision in two different locations. While some cost shifting may have occurred, both between the two levels of government and within the health and welfare sector, this has not been analysed in this paper.
Collection of expenditure data from the hospital was undertaken from the period 1989–1990 to 1995–1996. This involved analysis of the financial end-of-year working papers of the hospital in the earlier period and cost centre reports for the later period. The cost data was not collected and generated in such a way to allow for measurement of variation of cost estimates. Data from minutes of committee meetings and associated reports provided supplementary information. Forty patients were transferred from the hospital between May and August 1994 to four community residential facilities, each of 10 people, which were specifically established for them. Some patients moved to more independent accommodation and some returned to hospital, resulting in a total study population of 47 patients who lived in the community residences. Patients were costed either as a community patient or a hospital patient and not individually followed. Expenditure information was collected for the first 2 years of establishment of these community residences. These data consisted of cost centre reports, residence accounts and a survey of all staff who contributed to the operation of the residence in any way, even if the contributions did not appear on the cost centre report. This information provided cost categories of goods and services, repairs, maintenance and renewals, and staff salaries and wages. Funding was provided for the transfer of patients, although this information is not analysed here, as it was a one-off expense. The data were collected retrospectively and currently for both the hospital and the community.
The study design was a pre–post design. For ethical reasons it was necessary that the study group be non-randomised and, furthermore, due to the establishment of these special community houses, there was no appropriate community control group for comparison. From currently available data, these patients were largely representative of a chronically hospitalised sample of patients with intractable psychoses.
As the four residences were in different sectors within the area health service (each with a different service structure) the economic operation of each house was unique. There were some similarities, however, including the availability of local services such as general practitioners, retail shops and hairdressers that were formerly provided in the hospital. The residences were similar in resident numbers and severity of illness of residents, and therefore decision was made to combine these data for economic analysis.
The cost information was analysed by conversion to costs per occupied bed-day, to enable comparison between the hospital and community residences. The hospital information was collected for a longer period (including retrospectively), which enabled a comparison to be made with the community residences, both before the patients were transferred and after their relocation. It was not considered necessary to convert the costs to a base-year price, as the analysis was undertaken within a fairly short time period during which the Consumer Price Index increased only slightly. While it is recognised that these costs could be converted to a base-year price, the major cost comparison between hospital and community has only 2 years of community costs.
The analysis was divided into three periods:
Pre-transition (1989–1990 to 1992–1993): considered only the hospital accounts as the community residences were not yet established. During this period there was planning in the community and consultation with the hospital regarding the process of transfer of people to the community residences.
Transition (1993–1994 to 1995–1996): with the transfer of patients there was a one-off transfer of funds from the hospital to the community of $40 000 per patient. This was used to help the residents establish, settle into the community and provide staff salaries for the first year. While the costs incurred during this period were recorded for verification purposes, the cost comparisons which can be used to inform future policy are those which compare periods one and three. The transition costs, although they present a significant opportunity cost, were not included in the cost comparison as it was considered that such an inclusion would not assist in a comparison of the costs of care in alternative locations.
Current (1995–1996): the community residences were now fully incorporated into the community services in the area.
The transfer of residents to the community enabled the consolidation of remaining patients into fewer wards and some empty buildings were leased out, which meant the hospital recouped some of the revenue they lost by having fewer patients. As in the hospital, the patients in the community contributed to their care by paying board, which was generally 75 per cent of their government-provided disability pension and 80 per cent of their rental assistance. This represented only a small proportion of the cost of care, although it was a large proportion of the personal income of the resident (see Table 1).
Costs per occupied bed day in the hospital and community
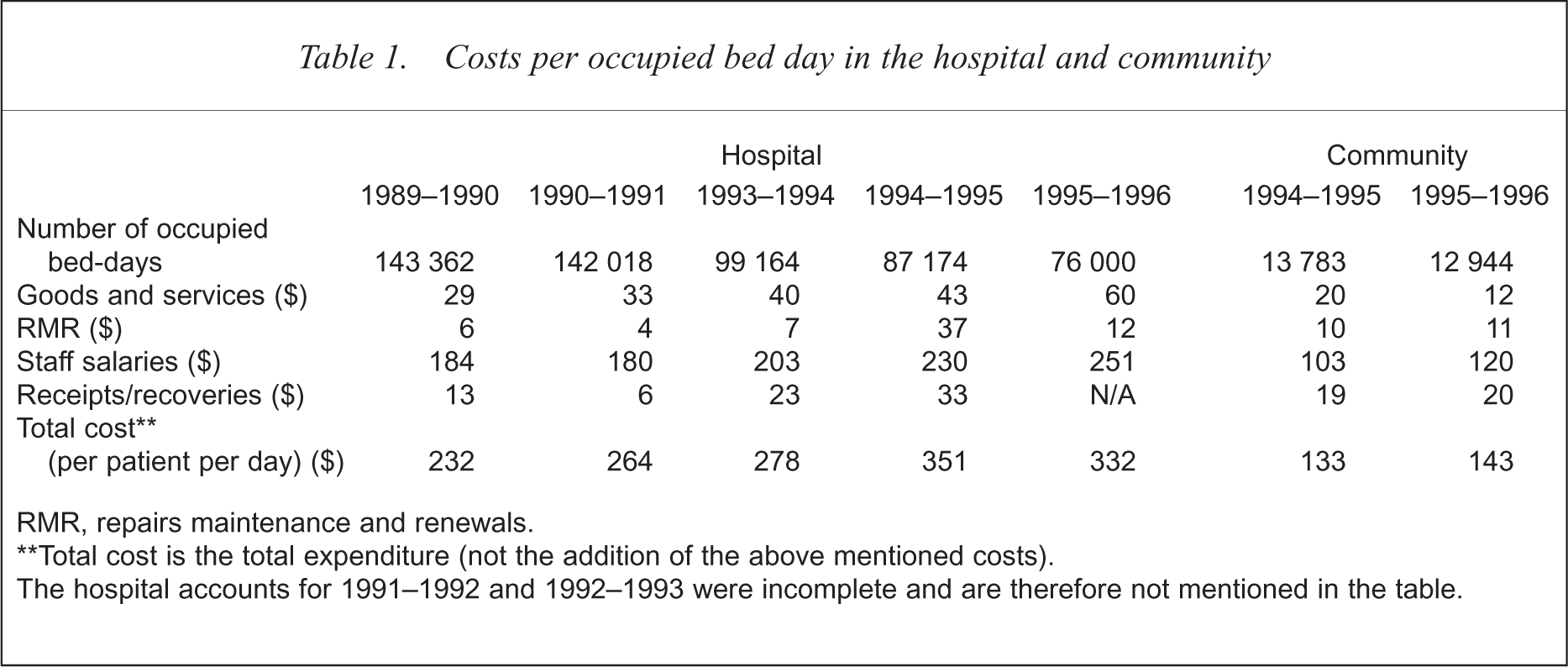
RMR, repairs maintenance and renewals.
Total cost is the total expenditure (not the addition of the above mentioned costs).
The hospital accounts for 1991–1992 and 1992–1993 were incomplete and are therefore not mentioned in the table.
Results
Table 1 sets out the detailed cost components in each setting. The four community residences were found to be $190 less expensive per occupied bed-day than the hospital in the year 1995–1996. The cost for a patient in the hospital for 1 year was approximately $121 000 while the cost for a patient in the community for 1 year was approximately $52,000, that is 43 per cent of the cost of care for a hospital patient. Even when considering all the limitations of the research, the difference in expenditure between the two settings is so great that intensive care in the community for such patients provides cost savings. It also should be remembered that these residents were cared for in an intensive (24 h supervised), community setting for 2 years, and are therefore more costly than other community residents who are able to live in supported residences. Furthermore some of the residents in this study were able later to move to other (less expensive) accommodation. These analyses do not address these diminishing community costs.
The hospital goods and services costs increased over the period from $28.71 to $59.83 per occupied bed-day. This increase in hospital goods and services expenditure in 1995–1996 can be explained by the reduction in hospital inpatient numbers, which occurred without a corresponding decline in good and services expenditure. The total expenditure on goods and services in 1995–1996 was actually less than in 1990–1991 (by 4%), however, the patient occupied bed-days approximately halved in the same time period. Within the community, goods and services expenditure declined substantially during the 2 years of the study.
The difference between the hospital and community expenditure on goods and services was mostly due to medical and surgical supplies, which were $10.18 per occupied bed-day in the hospital, while only $0.27 in the community residences. Also, domestic charges were $13.80 in the hospital per occupied bed-day and $1.13 in the community.
There was a significant increase in repairs, maintenance and renewals expenditure at the hospital in 1994–1995, which was due to refurbishment of many of the wards. Expenditure in the community increased slightly.
Salaries and wages expenditure increased over the period in the hospital. This increase was mostly after 1993–1994 resulting from the decrease in occupied bed-days without a sufficient corresponding reduction in staff numbers. In 1993–1994 the total staff salaries and wages expenditure was $20 171 013 whereas in 1995–1996 it was $19 049 674 (a decrease of 5.56%), while occupied bed-days declined by 23 per cent. Community residence expenditure on staff salaries and wages increased during the study period both on an occupied bed basis and on total costs. This was due to an approximate doubling in the occupied bed-day and actual costs for one of the residences; the other residences in fact reduced this expenditure over the period. The difference in staff salaries and wages expenditure between the community residences occurred because one residence employed more staff per shift, while the other three residences reduced staff numbers per shift during the period without any adverse effect on patient care.
There were no detailed data for the hospital in the period (1992–1993) when the community residences were being planned. Assuming the trends in employment-related expenditure in the hospital was similar to previous years, the differences between hospital and community staff expenditures were largely due to the greater employment of ‘hotel service’ staff in the hospital. Both the hospital and the community employed more nurses than other, non-clinical staff, and nurses represented slightly more than one-half the total staff cost in each setting.
Discussion
This study has several limitations. The patients who were transferred do not necessarily accurately reflect the total population of this hospital's patients, as the most chronic patients were less likely to be discharged. Notwithstanding this, those patients who were discharged had spent most of their adult lives (65%) in hospital. The remaining patients may inevitably be more expensive to relocate due to their greater symptomatology. There was also a problem of availability of data in the hospital accounts, due to, for example, incomplete working papers for the hospital (for some years), inaccurate figures between different print-outs and a change in accounting software resulting in categorically dissimilar data. A further limitation related to the organisational structure of the hospital and community residences. When the patients were in hospital, they were part of a ‘closed’ financial structure, in that all the services they required were provided within the hospital (including hairdressers, social activities and physical health services). However, when these patients moved to the community residences, they became part of the community in which they lived. This meant that some of the costs of care were more difficult to collect as these clients had become but one component of an integrated community mental health service. However, the time and involvement of all community staff (up to the Area Director of Mental Health) with these patients was costed; it included estimates of the time of all clinical, administrative and other activities, involving all our staff with these patients.
Furthermore, as a relatively small number of residents moved to each sub-area in the community, there was no need for the specialised services provided (apart from housing) to be expanded to accommodate them. If there had been a larger number of discharges, some expansion of services would have been required. As previously discussed, one study noted that the later (more disabled) transfers, can lead to the community care costs increasing [3]. For this study of 40 residents, cost of care was much lower in the community. Whether this was a cost-effective form of treatment greatly depends on the health improvement of the patients: it was found in this study that both the mental state of the residents and their quality of life improved considerably in the community, as detailed in the clinical evaluation [1].
An American study noted several reasons why community settings were less expensive than hospital settings. These included hospitals having a high number of funded vacancies, while the high staff turnover rate in the community means that cost savings could be made by not funding involuntary layoffs or transfers [4]. Finally these special houses were constantly under close economic scrutiny. Staff salaries and wages are an important consideration, as in this study they are approximately three-quarters of the cost of care for residents both in the hospital and in the community.
The TAPS project found that there were large cost variations between and within the multiple facility types studied [6]. This study only analysed one type of high-staffed hostel, and therefore costs could be less with less-intensively supervised accommodation.
The successful transfer of patients from a hospital for the chronically mentally ill to a community setting may enable the hospital to specialise its services, and, in the process, become more cost-effective. For those patients discharged, their quality of life improves, their clinical illness can improve and they significantly reduce the financial burden on an already strained mental health budget.
Acknowledgements
We are grateful to the staff who participated in the study to provide valuable time and information. This project was funded by Research and Development Grants Advisory Committee, Commonwealth Department of Health, administered by Sydney University, and by a grant from the Northern Sydney Area Health Service.