
Abstract
Substance misuse is very common among psychiatric patients [1–3]. While dependence on alcohol and nicotine are common [2,4], cannabis, heroin and amphetamines are also often misused [5]. Both substance misuse and mental health specialists have long recognised that neither service provides adequate clinical care for dual diagnosis patients [6,7]. Patients with mental illness, but without a coexisting substance use disorder, are deemed to have better access to treatment services than patients with mental illness and a comorbid substance use disorder [8]. Patients with a comorbid substance use disorder receive less outpatient treatment because they are considered difficult patients by mental health professionals [9]. Also, it is common for psychiatric patients with alcohol problems to feel unwelcome in alcohol treatment agencies [10]. Often the liaison between drug and alcohol and specialist psychiatric settings are inadequate, and many psychiatric patients may not relate well to the demands placed on them by drug and alcohol agencies. Use of alcohol and/or other substances may also exacerbate the course of the psychiatric disorder. These factors often lead to relapses and non-compliance with pharmacological and psychosocial interventions [5].
Although there has recently been a proliferation of different clinical programs and guidelines to treat psychiatric patients who misuse alcohol or other substances [11], reports of randomised controlled trials for this population are scarce [12–14].
Rationale for the development of the present program
Based on the review and recommendations proposed in the current psychiatric literature, it is evident that: (i) psychiatric patients who misuse alcohol or other substances generally do not receive adequate attention; (ii) considerable economic burden is caused by dual diagnosis patients in terms of higher rates of relapse and rehospitalisation, more admissions to emergency rooms, non-compliance with psychosocial and pharmacological interventions and a history of arrests [15]; and (iii) randomised clinical trials evaluating the effectiveness of interventions for this group of patients are seriously lacking.
Our interest was to use existing resources and: (i) develop and implement an integrated opportunistic intervention program for psychiatric patients aimed at reducing their alcohol and other substance use; and (ii) evaluate its impact.
Initiating a partnership between mental health and drug and alcohol services
To address the previously mentioned issues, a collaborative partnership was formed between the Drug and Alcohol Services and the Mental Health Services from the Western Sydney Area Health Services to discuss: (i) the prevalence and clinical implications of alcohol and other substance misuse among psychiatric patients seen by the Mental Health Services; and (ii) investigate the possibility of implementing an intervention program. Regular meetings were held over several months among psychiatric, nursing and allied health staff. Based on these consultations, it was unanimously agreed to implement an opportunistic intervention program, and train staff to detect, assess, and offer standardised treatment.
Selecting brief assessment instruments
The first task was to identify and select brief scales with good psychometric properties to detect alcohol and other substance use. As there is some evidence that psychiatric patients are willing to admit to substance misuse on self-report measures, but deny this in clinical interviews [16], and as our proposed intervention is opportunistic, we preferred to include user-friendly, self-administered scales. The Alcohol Use Disorders Identification Test (AUDIT) [17] and the Drug Abuse Screening Test [18] were selected for this purpose. Both these measures have excellent psychometric properties [19,20].
Provision of manual-based treatment
From the outset, we decided to implement a manual-driven treatment program. Manual-driven treatments are considered to represent an important breakthrough in the development, evaluation, and dissemination of empirically validated therapies [21,22]. A specific treatment manual based on the principles of cognitive-behaviour therapy and adopting a harm-reduction approach [23,24] was developed for this purpose. The clinical procedures described in the treatment manual are validated and considered both method- and cost-effective in the drug and alcohol treatment literature [5,10,12,13,25–38].
Staff training
Rather than recruit ‘specialist dual-diagnosis clinicians’ from either the drug and alcohol or mental health services, we decided that it would be practical to train staff members from the mental health services to opportunistically detect and offer an integrated drug and alcohol intervention. This approach (i.e. enabling staff with the necessary skills to offer brief opportunistic intervention) has been found to be cost- and method-effective in the alcohol and cigarette-smoking literature [4,10,13,26]. Staff from the Mental Health Services who expressed an interest in attending the training programs were offered a series of clinical workshops. To date, over 40 staff members from various disciplines have attended the training programs. Briefly, the training programs focused on the current drug and alcohol and mental health literature regarding the prevalence of comorbidity, and the effectiveness of various interventions. Participants were then introduced to the assessment instruments and trained to administer, score and interpret the scales. In addition, procedures to enhance patient motivation and effective behaviour change methods were discussed, emphasising a harm-reduction approach. The time taken to conduct the training workshops were approximately 4 h. Information about the training workshop can be obtained from the first author.
Program plan
Who is eligible to participate?
All patients aged between 16 and 65, who can speak and understand English, admitted to Paringa Ward of the Cumberland Psychiatric Hospital and the associated community mental health centres are routinely screened for alcohol and other substance use. Although it is necessary to include patients from a non-English-speaking background, we decided to trial this pilot program with patients who can speak and understand English. We also decided to exclude patients with organic brain disease and intellectual impairment (as judged by their clinical records). As our primary interest is to ascertain the impact of the intervention at follow-up, we decided to exclude patients with no fixed abode (as determined on admission), and those who discharge themselves within 3 days of admission (against the advice of the medical and nursing staff).
Recruiting patients
Cumberland Psychiatric Hospital
All patients identified as using alcohol or other substances by (i) the admitting medical officer, (ii) their clinical notes, and (iii) the daily clinical case discussion meetings, were earmarked to complete the assessment scales at a later date. Obtaining information about substance use from such multiple sources is viewed as an optimal method of information gathering [14]. When the medical and nursing staff are convinced that these patients are capable of completing the brief assessment scales, a specific time is set aside to administer the same. A staff member is present while the patient completes these measures, to ensure that all items of the scales are completed and to answer any queries. Patients are informed that the information they provide is confidential and that it may assist in a better understanding and management of their clinical conditions. The scales are scored immediately and the patient is allocated to a case manager specifically trained to deliver the intervention.
Community mental health services
Outpatients presenting directly to the community mental health centres (i.e. patients who are not referred by the psychiatric hospital) are also routinely screened for alcohol or other substance use, and those identified with a drug or alcohol problem are referred to the appropriate case manager.
Assessment
Based on the clinical information obtained about the patient during the recruitment process, patients are required to complete either the 10-item Alcohol Use Disorders Identification Test (AUDIT), or the 20-item Drug Abuse Screening Test (DAST), or both. In addition, patients who predominantly misuse alcohol are administered a Drinking Self-efficacy Scale [32,33,37]. Similarly, patients who predominantly use other substances are administered a Self-efficacy Scale (Drug version) based on the ‘Drug Use Precipitant Inventory’ [Sitharthan T, McGrath D, Cairns D, Saunders JB: unpublished data, 1991]. Assessment of self-efficacy judgements can be used during treatment sessions to prepare the patients to cope effectively in future high-risk situations [39]. The nursing unit manager and the team leader from the community oversee the assessment process. All other relevant clinical and demographic information are obtained from the admission records and case notes.
Randomisation
Patients who score eight or more on the AUDIT and those who score six or more on the DAST are deemed eligible to participate, as these cutoffs warrant clinical attention [17–20]. All eligible patients are randomly assigned to receive either the integrated drug and alcohol intervention (IDAI) based on cognitive-behavioural principles or a simple minimal invervention (MI) that discusses health issues.
Patients who score seven or less on the AUDIT and those who score five or less on the DAST are provided with a simple pamphlet about how drug use interacts with health and behaviour, but are not assigned to any intervention condition.
Ethical considerations
As it was neither ethical nor practical to have a control group, we decided to include a minimal comparative condition, which will receive full IDAI after 3 months (Fig. 1). This ensures that all patients are offered some basic health information about drug use, yet the design allows us to validate the effectiveness of the intervention being tested. Also, the proposed IDAI intervention will be in addition to existing treatments the patients receive either in the hospital or in the community. We also decided to monitor all patients (through regular staff meetings and clinical supervision) to ensure that they are not experiencing any negative effects from participation. To comply with confidentiality issues, we decided to include all patient data on a separate computer coded only by number.
Brief description of the treatment conditions
Integrated drug and alcohol intervention
Patients assigned to this condition are treated individually. The IDAI has four clinical components. Those recruited through the hospital receive at least the first component while they are still in the hospital, with later sessions scheduled after discharge. This was deemed essential to foster an ongoing link between the hospital and the community mental health centres.
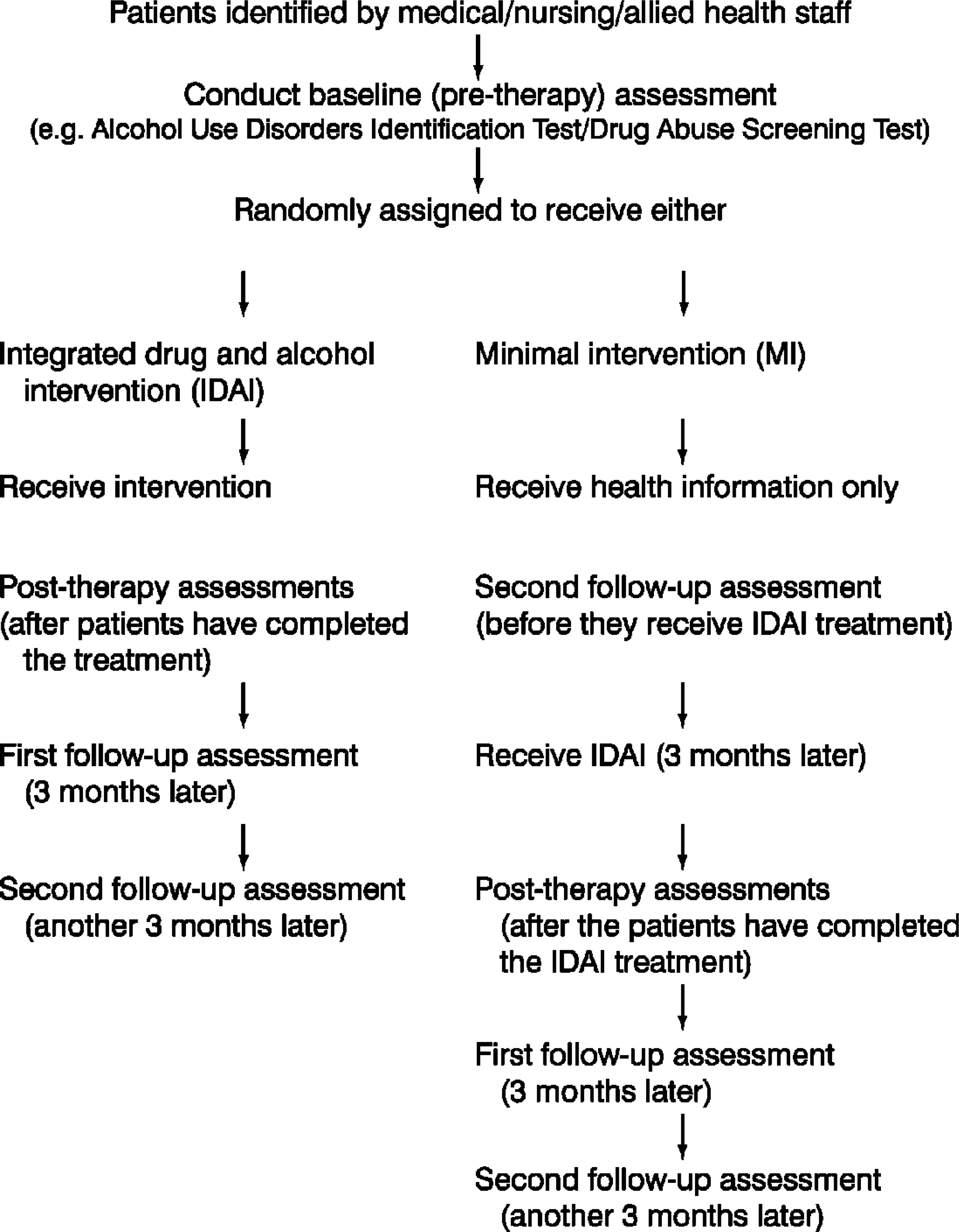
A schematic flow chart of the intervention program
Although the IDAI is a structured manual-driven intervention, we decided to keep the number of treatment sessions flexible. That is, rather than impose the clinician to deliver the treatment in a set number of pre-determined sessions, we have allowed the case managers and their patients to jointly decide as to how often they choose to meet (once a week, twice a week, etc.). Hence, we are concentrating on delivering the entire set of clinical components, rather than delivering the program in a set number of sessions.
Treatment is tailored to suit the individual needs of the patient. Rather than employ confrontational methods, the case manager/therapist is trained to provide choices, empathetically assist the patient to set achievable goals, focus on realistic perspectives on recovery, provide feedback, and promote self-motivational statements; as recommended by Miller and Rollnick [36]. In addition, printed handouts on the materials discussed are provided to the patients to enhance comprehension and memory for information, and to increase compliance [40].
The details of the four clinical components and the treatment handouts are presented in the IDAI treatment manual, and can be obtained from the first author. A brief description of the four clinical components is presented in Appendix I and II.
Minimal intervention condition
Patients assigned to this condition are also seen individually. They are provided a single 60 min session of ‘drug information’. The assigned case manager discusses the harmful effects of drug use (e.g. physical and mental), and provides a simple pamphlet consisting of the same material (a generic pamphlet developed by the Department of Health, New South Wales Government, and available in most treatment agencies). No information construed as cognitive-behavioural is provided to these patients.
Patients assigned to this condition are informed that they will receive additional treatment in 3 months time, and an appointment is made to deliver the same. However, any patient who expresses a need for additional treatment immediately (i.e. those who do not want to wait for 3 months), will be seen earlier and provided IDAI. These patients will be identified separately for data analysis.
Treatment integrity
Treatment integrity is maintained through regular, periodic discussions with the project team and the case managers. Furthermore, specific clinical checklists have been developed and employed to ensure that: (i) all patients are routinely questioned about substance use and screened for the same; (ii) screening instruments are correctly scored; (iii) patients are randomly assigned; and (iv) intervention is delivered as per the treatment manual. The verification of these clinical checklists are undertaken by four program coordinators, two of whom are from the hospital and two from the community. We also plan to randomly tape-record 20 sessions (from each condition), for further verification of treatment integrity. In addition, clinicians have also been encouraged to write up individual case studies, with a view towards publication.
Expected benefits
To our knowledge, this is the only randomised opportunistic intervention that is currently being implemented and investigated from a psychiatric teaching hospital and associated community mental health centres. If the IDAI is demonstrated to be efficacious, it will have a wide clinical application, with the potential to be readily incorporated in regular psychiatric settings. This process could be less expensive and clinically achievable [7,41], and enable a wide range of health professionals to be trained to deliver intervention after a very brief training period. Additional benefits that may be gained include the identification of favourable treatment predictors.
Conclusion
Many psychiatric patients who abuse alcohol or other substances rarely attend a traditional drug and alcohol treatment agency. Training psychiatric staff to routinely screen and offer a relatively brief integrated intervention may be a useful alternative. The current clinical program is designed with this in mind. There are several attractive features of this program: staff can be trained in a relatively short period of time, patients can be treated within the same setting without placing any additional demands on them, the integrated intervention is relatively brief and can be offered in conjunction with the standard psychiatric care they receive, and the impact of the intervention can be ascertained objectively.
Notes
This program was approved by the Cumberland Hospital Human Ethics Committee.
Footnotes
Acknowledgements
We wish to thank A. Bongon, K. Bowen, G. Butler, A. Christopher, R. Elliot, L. Gaunt, R. von Gneisanou, C. Kwok, S. McMahon, L. Parkes, K. Schadel, N. Sharma, J. Snars, R. Stuart, I. Wells, G. Whatmough and A. York for their assistance in implementing this program.