
Abstract
Since the start of the new digital impression-taking era which started around 2008 with the introduction of the 3M Lava COS, a slow transformation is gaining momentum and it looks as if this and next year will have a broad impact on the clinicians. From being merely a way of replacing impressions now the total digital workflow enters the industry. This means a whole new way of thinking and a new way to produce prosthetic work where a reproducible constant quality can be achieved. An obvious development of improved ceramic materials that simultaneously can satisfy the mechanical, bio- and aesthetic demands of the prostheses and the corresponding technologies for production that would work for the clinic digital workflow is out of the expertise of the dentists. This calls for a cross-disciplinary collaboration with the experts in the communities of ceramics and digital manufacturing.
Keywords
Introduction
To repair partially damaged teeth or lost teeth has always been an individual practice. Besides the selection of suitable materials, the in vitro preparation and the in vivo fixing of the prostheses were highly case sensitive. This fact turned dentistry as a handcraft-based practice until 1980s when an industrial approach, based on computer-aided design and computer-aided manufacturing (CAD/CAM) principle, was introduced to manufacture the cores of the prostheses [1-7]. Since then, the advanced ceramics, particularly tetragonal zirconia polycrystalline ceramics, known shortly as zirconia in practice, early developed for other industrial sectors have been increasingly used in dentistry [810]. Otherwise, in traditional model-dependent approach, the adaptable materials were limited to the metal alloys or glass-ceramics or In-Ceram type of ceramic composites that were able to be formed by casting or plastic deformation or slip deposition processes [1114]. The superior performances of advanced ceramics on mechanical, bio- and aesthetics thus were hindered to be applied to satisfy the patient's needs.
Yet, a laminated crown structure inherited from porcelain fused on metal (PFM) prostheses, consisting of a load-bearing strong ceramic core and a silicate glass out shell for restoring the occlusion/articulation relationships and the aesthetic behaviours (known as coping and veneering, respectively, in daily practice) has limited this approach to be only partially digitalised [15-17]. To accomplish the still remaining handcraft part of the work, manual operations by technicians in vitro and by dentists in vivo were unavoidable, which determined the current statue of the prosthetic dentistry characterised by the need of huge numbers of dental technicians/laboratories surrounding the dental clinics, providing customised services to dentists. Despite the vast efforts made in this way, perfect fit of the prostheses remains as a dream. Rather, the imperfect matching either in geometries or in aesthetics often yielded the in vivo adjustment and even returning-back of the prostheses to the labs. There are also other fatal drawbacks of this family of laminate structured ceramic prostheses that include high chipping rate, wear to the opposite tooth and the formation of secondary caries due to imperfect margin fitting observed in clinical follow-up studies [16,1820].
Monolithic structure would solve this problem of chipping, but often at the expense of aesthetics. Glass-ceramics, particularly those in the lithium silicate family, demonstrated a very good optical translucency that is crucial for meeting the aesthetic demand, but their mechanical strength is less than half of that of the zirconia ceramics that used to be regarded as strong but aesthetically not attractive enough for monolithic restoration particularly in the anterior region [9,10,21,22]. To meet such challenging demands that often require conflicted functions to be integrated into one single material, new ceramic materials are needed that in addition are able to be produced in a process that would match with a full digital workflow in which digitalised net-shape manufacturing is a vital step.
In implant dentistry, precision is the upmost important issue that must be satisfied in order to achieve perfect fitting between the implant and the abutment customised according to the position, angle, rotation, size and depth of a dental implant. The overall precision is determined not only by the accuracy limited by the software and hardware for digital design and manufacturing, but also by the fact how the material behaves during the manufacturing process. The current wide-spreading technique for making customised ceramic abutments by milling of a partially sintered blank often ends up an abutment having a surface with roughness up to 10 μm besides the frequent edge chipping, both of which would deteriorate the fitting precision. To solve such problems, it appears again essential to find suitable ceramic materials and their processing methods that can be integrated into a full digital workflow.
In this article, we will demonstrate the possibilities how the nano- and functionally gradient structure concepts and the wet-chemistry based additive manufacturing (AM) processes developed in the ceramic community can be implemented as new tools to enrich the arsenal in solving these problems through a cross-disciplinary approach. These successes have opened up numerous possibilities for the establishment of a flexible and easy-to-use full digital workflow that integrates the advantages of intraoral scanning, model-free designing and model-free manufacturing into a modern digital dental eco system.
A partial digital workflow
In this article, the term workflow always refers to an entire cyclic procedure including all the steps from patient to patient involved during the prosthodontic treatment. It thus encounters the tooth preparation in patient mouth, the digitalisation of the intraoral geometrical situation either indirectly by scanning the impression/plaster models or directly by intraoral scanning, the documentation of the shade condition, the computer-aided designing and manufacturing of the prostheses, and the manual completion of the prostheses by veneering/staining/glazing/polishing, and finally the setting of the prostheses in patient month. The clinical treatment part of the work is thus integrated together with the technical support part of the works. In early days when the CAD/CAM concepts just were introduced into dentistry in the 1980s, only the core of the ceramic prostheses was able to be produced [3-7]. The lack of mature scanners, CAD/CAD software, net-shape forming technologies, specially developed for the prosthodontic purposes limited the development of CAD/CAM based workflow. Until today, what is available and well accepted is still a partial digital workflow during which too many manual operations are unavoidably involved in determining/selecting of the CAD/CAM parameters besides the commonly known fact of manual veneering/staining/glazing/polishing that involves several lab work steps and increases the complicity of the workflow, see Figure 1(a). Nevertheless, other benefits associated with CAD/CAM generated dental restorations have been recognised that included an increase in quality and reproducibility as well as a standardised chain of production. All these advantages make it possible to re-assemble the technical support part of the works besides improving the planning strategies and improving the precision of the produced parts.
The zirconia core (a) and a ready-to-use bridge (b) produced through a conventional partial digital workflow based on CAD/CAM and through a novel full digital workflow based on CDD/CDM, respectively.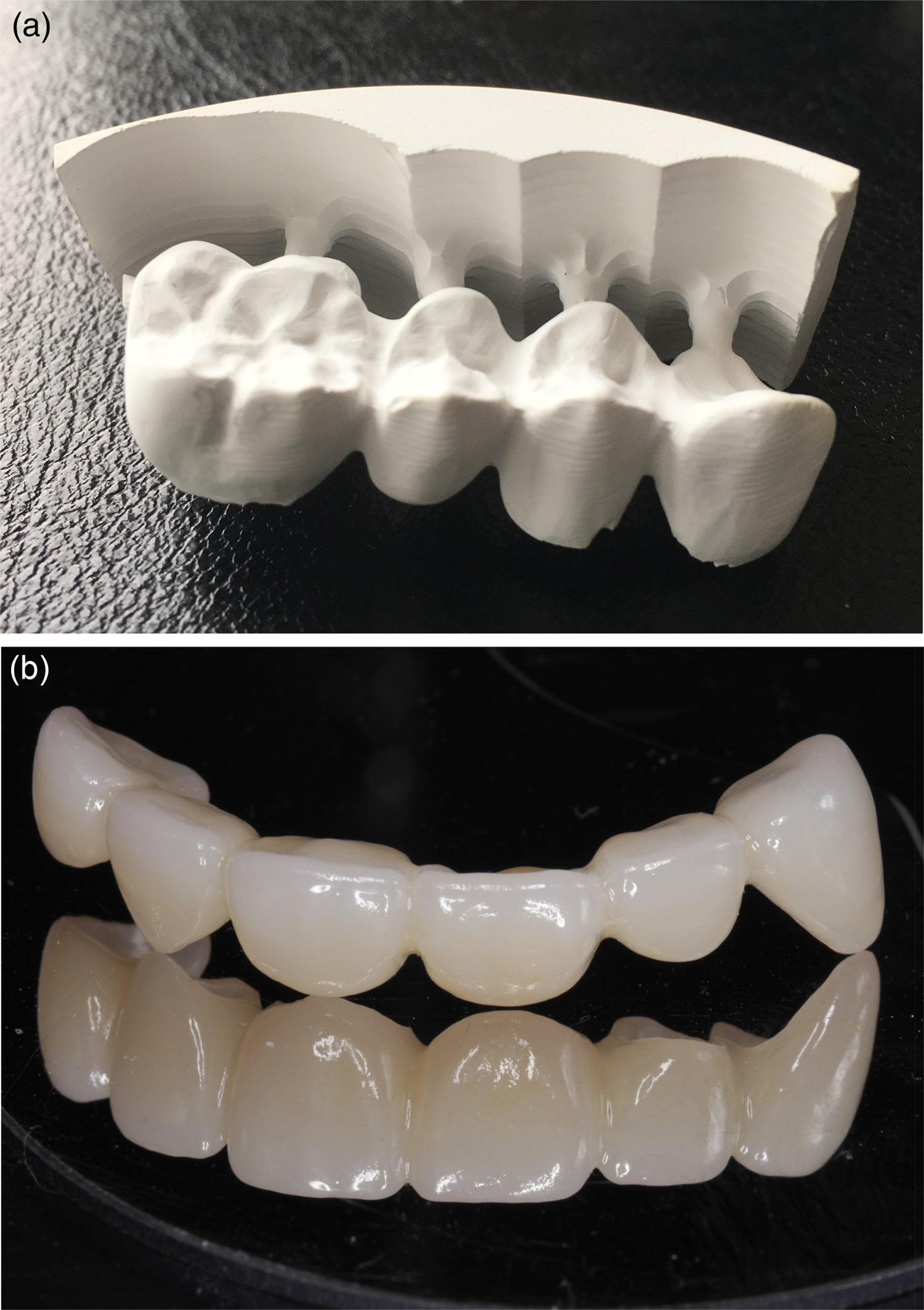
The assembling of CAD/CAM-based workflow
Almost during the same period of time in 1980s, two concepts, Cerec and Procera, regarding how to assemble the workflow based on CAD/CAM for cost-effective production of ceramic prostheses, were developed and introduced in Switzerland and Sweden, respectively. Cerec, initially the abbreviation of the term ‘Chair-side Economical Restoration of Esthetic Ceramics’ and latterly also referred as the abbreviation of the term ‘CEramic REConstruction’, developed by W. Mörmann and M. Brandestini at the University of Zurich in Switzerland aimed for accomplishing a prosthodontic treatment within one single visit [1,2]. It incorporates a camera/scanner, a computer, and a milling machine into one setup. The camera/scanner digitalises the tooth and the space to be restored into an optical impression that is transferred and displayed on a computer screen where the accredited dentist or trained staff virtually design the restoration using a CAD software. Then the core of the restoration is automatically produced by milling of a pre-sintered ceramic blank in a CNC milling machine based on CAM principle that is further accomplished by manual veneering/staining/glazing/polishing. The last step in this procedure is to bond/cement the newly prepared restoration to the surface of the prepared natural tooth. This workflow is well known by its vision of accomplishing inlay/onlays, single crowns or short bridges chairside in a single appointment with the expense of the deep involvement of dentists in technical support part of the works.
Procera system developed by M. Andersson in Sweden paved another way of accomplishing ceramic restorations in a modern industrial manner. Instead of setting up chairside, it divided the entire prosthodontic procedure into three units by following the step-unit principle for large scale industrial production, i.e. taking impression in clinics, scanning and veneering done in the labs and designing and manufacturing of the customised ceramic copings in production centres [3-5]. It was brave and visionary enough to put forward such a concept before the wide-spreading application of the internet and at the infant stage of the establishment of modern economic fast-delivery systems. A unique character of the Procera workflow is the integration, an intelligent way of integration, of the segments of technologies, expertise and competences that have the potential for further development. It allowed experts in different disciplines to focus their works they are good for and made the system open for sustainable development. This advantage was evidenced by its accommodation capacity. Although initially the application of Procera workflow was limited to the production of single crowns made of alumina, the approach has soon enabled the production of customised multiple unit ceramic anterior and posterior fixed partial dentures made of zirconia though in a different manner by adapting the results of continued development that was out of the initial imagination.
Introduction of advanced structural ceramics
Before the introduction of CAD/CAM principles, the production of prosthodontic prostheses had to rely on the geometric dimensions defined by the impressions and models. The plaster model is the holy grail of dental technicians. No dimensional change was allowed during the production, so only casting, plastic deformation and In-Ceram type of processes were compatible with the prosthodontic procedure. This fact determined that the technical support part of the prosthodontic work was based on handcraft, which can hardly be recognised as being industrialised. Within a conventional workflow even after CAD/CAM based technologies were involved, the final geometries of the prostheses have to be accomplished on the plaster model. The digitalisation made it possible to remove the dimensional restriction and to involve other near net-shape forming technologies like the Computer Numerical Control (CNC) milling of the pre-sintered blanks fully or partially densified into the workflow. As long as the dimensional change can be controlled, prostheses made of advanced rigid ceramics can be prepared in an enlarged form that can reach the demanded dimensions after sintering by compensating the sintering shrinkage.
In the early stage of development of Cerac systems, lithium disilicate based glass-ceramics was introduced as a suitable restoration material because of its similarity to the tooth substance in colour and physical properties [21]. The prostheses with the desired shape made of this type of glass-ceramics were prepared by CNC milling of the fully dense blanks while they were still in glass state. A subsequent heat-treatment process turned the glass to glass-ceramics by controlled crystallisation that substantially increased the strength and changed the optical translucency of the prostheses. The stains and glaze applied before the crystallisation process further enhanced the aesthetic properties.
Initially, Procera system embraced the CAD/CAM concept to fabricate an all-ceramic crown composed of a densely sintered high-purity alumina coping combined with a compatible veneering porcelain. During the process, an enlarged model was prepared first by CNC milling according to the virtual CAD file, a layer of alumina powder was then pressed on this model by cold isostatic pressing (CIP) that was then CNC-milled again to generate the out contour of the coping. The green body of a coping was thereafter removed from the model and sintered to full density to gain strength and optical translucency [4]. This robust process was industrialised as a typical example of volume production of customised components, but can be applied only for the production of single units.
Such a fatal drawback was complemented by the later invention of F. Filser, P. Kocher and L. J. Gauckler at ETH Zurich in Switzerland [6,7]. Through Direct Ceramic Machining (DCM) of a pre-fabricated ceramic blank made of zirconia ceramics with a nano-crystalline porous structure in the pre-sintered state based on CAD/CAM principle, it became possible to fabricate multi-unit all-ceramic dental bridges made of zirconia. With this process, also known as CERCON, substantially improved mechanical properties were obtained when the components were fully sintered after the machining step in comparison with the components made of lithium disilicate based glass-ceramics and alumina. The afterwards veneering of the high strength ceramic framework added the required aesthetic and wear characteristics as in other cases of ceramic copings.
The limitations of an inherent laminate structure and a dry process
The current version of ceramic restorations is bi-layer structured, consists of a strong inner coping made of zirconia or lithium disilicate-based glass-ceramics and an outer porcelain shell for adjusting the anatomy contour and for achieving the demanded aesthetics of the individual teeth. The out shell porcelain/veneer is in fact a silicate-based oxide glass with flexibly adjustable optical properties but with thermal mechanical properties that often do not match well with that of the rigid ceramic coping. Thus, the failure of the restorations frequently takes place within the weaker porcelain layer [16]. Cone cracks originate from defects at the porcelain surface caused by high cyclic compressive stresses at the occlusal contacts due to bite force. These cyclic loads initiate local tensile stresses and initiate micro-cracks and slow crack propagation by fatigue that would result in porcelain chipping at the end. Sometimes the chipping is small and does not affect the proximal contact area with the adjacent teeth or change the contour of the teeth. In this case, the restoration could still perform as normal and did not fail. In another instance, however, the restoration can ultimately fail and need to be replaced, especially when the chipping damage of the proximal margin ridge results in the loss of the normal contact area with adjacent teeth. It should be aware that the local chipping also deteriorates the surface by increasing its roughness that would increase the wear to the opposite tooth.
The flaws/defects/irregularities that act as the fracture origins of the ceramic restorations are introduced and accumulated during the entire fabrication process of the prostheses. It was noticed that voids, agglomerates and impurity inclusions form randomly in outer shell porcelain layer [23,24]. This type of defects is unavoidable and hard to control as long as the porcelain layer has to be made by a manual layering process. On the other hand, the type of detrimental defects in zirconia copings made by the current process of CNC milling of a partially sintered blank can all be traced back to the dry process applied for consolidation of ceramic particles to form a green body and CNC milling in the dry state. These defects present either as bulk defects originated from the particle packing during the consolidation of the green body, or as surface defects originated from the interaction between materials and the pressing or machining tools. The defects of later type dominate in prostheses made of lithium disilicate-based glass-ceramics CNC-milled from an already fully dense blank.
Hard agglomerates and packing voids introduced in the raw powder and during the dry pressing process, respectively, are responsible for the largest defect population in the blank, while the surface local chipping of hardly aggregated grains is found to be the largest defects introduced during the CNC milling or grinding. This fact indicates that, in real practice, the performance of a ceramic prosthesis would be strongly dependent on the process history of the materials, and properties such as strength and translucency will not necessarily be the same when the ceramics are prepared through different processes or by different producers, even if the same raw materials are used. Optimising the process could minimise these processing-related defects with only limited success. The inherent drawbacks of the dry process can hardly be removed if a new process enabling more homogeneous packing of individual nanoparticles and the formation of the smoother surface is not developed and introduced.
A full digital workflow
With the introduction of smaller, faster, more precise and more cost-affordable intraoral scanners and the maturing of the AM family of processes all required segments of technologies become accessible for building a full digital workflow consisting of three major steps: digitalisation, digital design and materialisation. This type of more flexible workflow reflects the future trend. It would improve the component reliability, treatment efficiency and patient satisfaction by further simplifying the restorative procedure. The resulting challenge to ceramics developers is to develop ceramics and corresponding processes in such a way so that ready-to-use products customised for patient cases can be produced with high precision, reliable quality and satisficed aesthetics with a digital approach without or with very limited involvement of any manual operation.
Model-free by net-shape manufacturing
The use of intraoral scanners makes it possible to abandon impression and plaster models. Under these conditions, a virtual design can be achieved with high precision, the net-shape manufacturing becomes the only bottleneck in bringing model-free manufacturing approach into real practice. The current manufacturing process based on CNC milling of the pre-sintered blanks fully or partially densified can only achieve near net-shape. As long as the final geometries of the prostheses need to be accomplished on the plaster models, the advantages of the model-free approach and their contribution to the establishment of a full digital workflow are partially masked. To achieve the goal of net-shape manufacturing of customised prostheses, the current hard-to-avoid manual operations, like cutting the connecting bars and polishing/glazing the surface to gain required aesthetics and dimensional tolerance, have to be omitted or replaced by digital operations.
An attractive solution for this is the implementation of AM family processes, commonly known as 3D printing, into the production workflow. For AM of ceramic prostheses, it is usually recommended that the most suitable process is the stereolithographic additive manufacturing (SLA) that uses a stable hybrid gel containing a high concentration of ceramic nanoparticles mixed with a UV curable resin monomer as a precursor. This process allows nearly unlimited geometry design and production of multiple customised components at a time with little material waste [25,26]. By adding and UV curing of hybrid gel layer-by-layer with controlled layer thickness complicated structures, especially those with a hierarchical inner section that is inaccessible for milling tools in subtractive approaches, could be easily processed. To obtain full dense ceramics components de-binding for removing polymerised resin by burning and sintering are necessarily needed. Any inhomogeneous distribution of polymers in the printed body would yield corresponding inhomogeneous distribution of porosity after de-binding thus influence the density homogeneity of the final sintered products. Despite intensive efforts made worldwide during the recent years, the performances of the ceramic components made by this way of AM can still not compete with those made by CNC milling of pre-sintered blank prepared by CIP, especially the optical translucency that is more sensitive to the residual porosity even with very low concentration. Further development of this process relays on the improvement of packing/sintering homogeneity/density.
Another alternative is to integrate the additive and subtractive manufacturing principles into a workflow. To facilitate this, the current process characterised by handling everything in the dry state is not feasible but has to be turned to a wet process involving colloids/hybrid gels as the precursors instead of dry powders, which can be easily added in droplet-by-droplet or layer-by-layer manner. After consolidation/ photo-polymerisation, the additively produced green bodies can then be subjected to a follow-up subtractive process to gain the required dimensional tolerance with high precision. One effort made in this direction is the establishment of a process named as precise additive 3D gel deposition invented by one of the current authors of this article. This hybrid net-shape manufacturing process has enabled the production, in industrial scale, of a new grade of customised full-contour zirconia prostheses known as Self-Glazed Zirconia [27] (Figure 2).
A feasible full digital workflow for industrial production and clinical implementation of customised zirconia prostheses.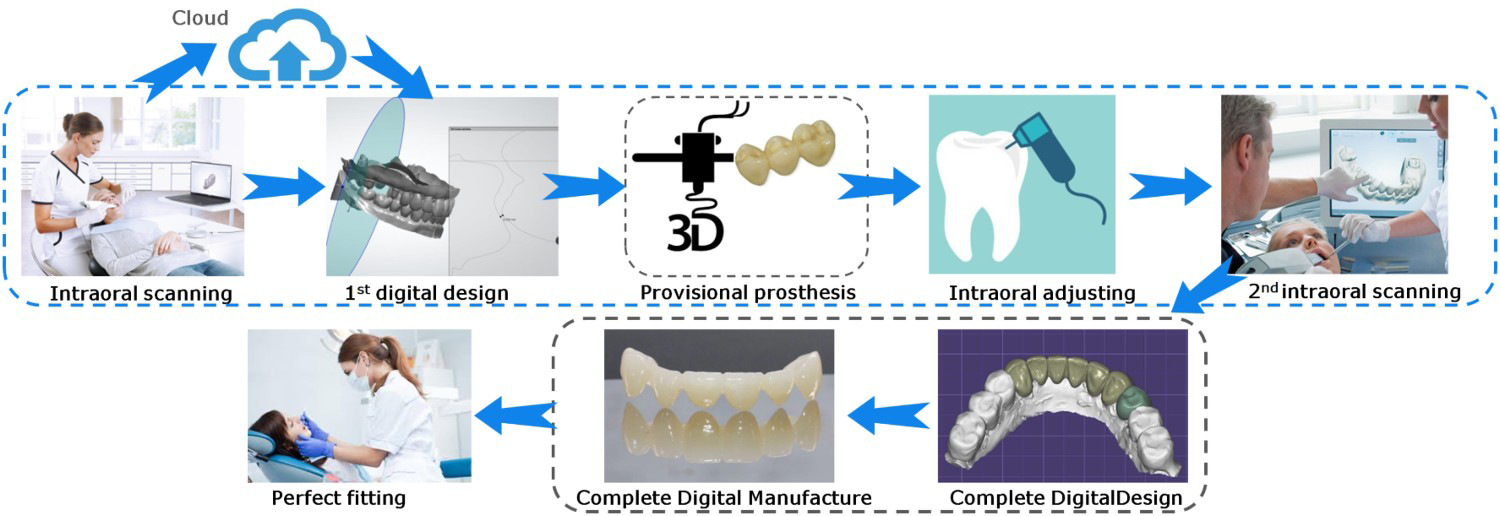
Full-contour monolithic prostheses with improved aesthetics
Full-contour monolithic prosthesis structure is demanded due to its obvious advantages in simplifying the manufacturing process and in preventing undesirable chipping of porcelain and other complications associated with the bilayered ceramic structure. Two crucial issues have to be considered in order to improve its harmonious and aesthetic appearance with the adjacent natural dentition to a level that would satisfy all indications. These are (1) to generate a smooth surface that imitates the appearance of natural enamel directly during the manufacturing process; and (2) to generate a 3D gradient of both shade and optical translucency. For the former, in current strategy of CNC milling of a pre-sintered blank there is no technical solution besides manual polishing and/or glazing; For the latter, a common technical solution currently implemented is to increase overall optical translucency by introducing more cubic phase in the expanse of mechanical strength and to generate a 1D shade gradient by forming a pre-shaded multilayered-blank with high optical translucency and shade gradient in the thickness direction. In this way, in order to get the right shade gradient, the prosthesis has to be well-aligned in the blank. Never the less, manual operations are still necessary to achieve steric shade and translucency gradient.
The full-contour prostheses made of self-glazed zirconia offer both exceptional aesthetics and strength. It forms inherently an enamel-like surface, being very smooth in micrometer scale, yet with a nanoscale roughness that has been approved to have almost the same friction and wear performance against tooth enamel as a well-polished zirconia surface [28], see Figure 1(b). Owing to the possibilities opened up by the implementation of nano-, functional gradient- and AM principles, structural and functional gradients both in radial and in height direction of the prostheses can be formed. This makes it possible to achieve the demanded aesthetics under the condition of no need of any polishing/glazing on the surface of the prostheses, implying a net-shape manufacturing process for ceramic prostheses ready-to-use.
Separating designing from manufacturing in a new era
Because all the step-units involved in this full digital workflow share a common source of digital data that can be communicated through long distance and across the disciplines, the skills and expertise among dentists, dental engineers/technicians, software developers and materials manufactures would be possibly exchanged and integrated into a modern system in a level that has never been achieved earlier. The production of ceramic prostheses thus can be accomplished through a Completely Digital Design & Completely Digital Manufacture (CDD/CDM) approach instead of the previous partial digital approach CAD/CAM that only aided to increase the accuracy and reliability of the produced prostheses but not change its manual operations-dominated character. The outcome of this new workflow is then the evading of the physical impression, the veneering porcelain layer and any clinical adjustment. Through strengthening the collaboration among clinics, labs, design and manufacture centres, this new workflow would also gain improved efficiency/accuracy/reliability, as well as the predictable and visualised results for meeting the patient satisfaction (Figure 3).
A cyber physical system representing the novel cloud connected dental eco system, a full digital platform worldwide characterised by the separation of design work to form independent design centres from the convention production centres.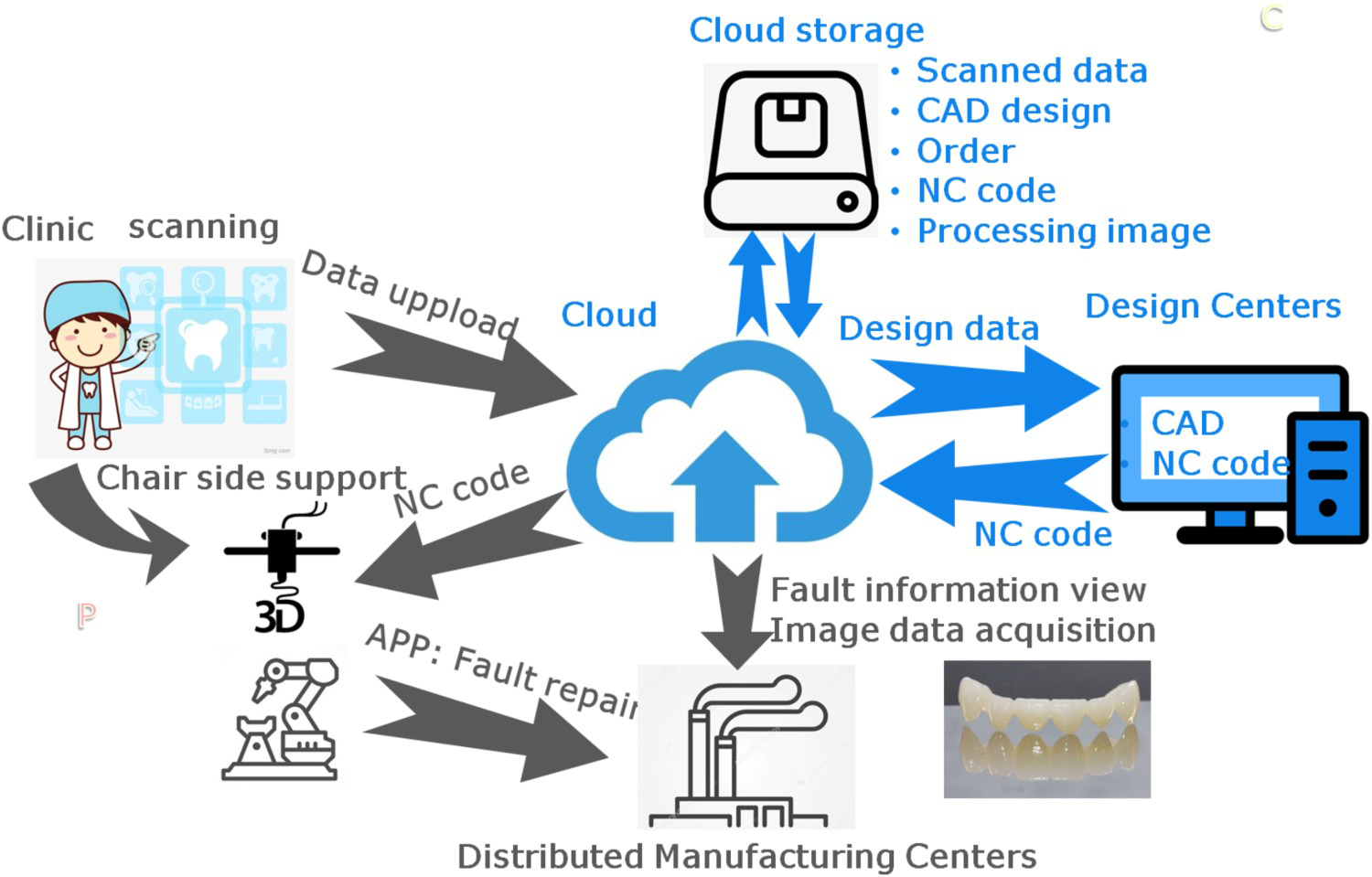
When the geometry and aesthetic characters of the prostheses were accomplished by manual operations, CAD/CAM technology aided only to adopt advanced materials and to improve the accuracy and reliability of the produced prostheses, the shape and quality of the restorations are determined mainly by the skills and experiences of the technicians. After the realisation of a CDD/CDM approach, the geometry and aesthetics of the prostheses can both be achieved through digitalised net-shape manufacturing processes based on the digital designs that in turn can be pre-viewed by the dentists in charge. With the deep involvement of dentists, the role of technicians in the manufacturing process is no longer so critical, but the importance of design work emerges. The design engineers or design technicians must have new knowledge and skills for designing the geometry and aesthetic characters of the prostheses in digital forms. Such creative designers are scarce resources. Their skills and experience ought to be cherished, maximally explored and shared in a new eco system, probably by separating the designing part of the work to form design centres from the conventional production centres. The design centre will not only ensure that the designers involved can provide more professional and state-of-the-art designs, but also can explore the potentials of the big data collected, can continuously improve the design and can renew the form of dental engineering supports. A full digital platform would enable much more design works than designing prosthetic components merely. So, components like orthodontic splints, nightguards and implant surgical guides all can be designed in the design centre using the exact same platform of dental digital data. With the help of cloud computing, the worldwide distributed design centres and manufacture centres together will provide efficient engineering supports and customised tools and components in a more flexible and sustainable manner.
Conclusions
In dentistry, digitalisation is no longer a choice but rather a general tendency. There are no any other ways for all the players in dental clinics and dental industry than to adapt it in their daily practice. To meet this challenge, new ceramic materials are demanded that in addition must be produced to a ready-to-use form in a process that would match with a full digital workflow in which digitalised net-shape manufacturing is a vital step. When nano-, functionally gradient structure, and AM concepts developed early in ceramic community are implemented as new tools to enrich the arsenal in solving these problems, the newly developed self-glazed zirconia ceramic restorations are, for example, able to integrate favourable and often conflicted functions on bio-compatibility, mechanical durability and aesthetics into one single material. Through strengthening the cross-disciplinary collaboration among clinics, design and manufacture centres, the full digital workflow would simplify the entire workflow and help improve the communication between the players involved. Radical improvement in efficiency, accuracy, and reliability, and visualised predictable results for meeting the patient satisfaction will be demonstrated by avoiding those manual operation steps that otherwise must be involved in the conventional partial digital workflow. Separating the designing part of the work to form design centres from the conventional production centres will ensure dentists and design engineers to make more influence in dental care on a full digital platform worldwide.
Footnotes
Disclosure statement
No potential conflict of interest was reported by the authors.