
Abstract
The aim of this study was to compare the functionality during daily activities and quality of life of patients with transtibial amputation vs. salvage surgery after severe lower limb trauma. Ten patients with unilateral below knee amputation and nine patients with salvage surgery after severe lower limb trauma were enrolled. Functional Ambulation Scale (FAS), Visual Analogue Scale (VAS), Short Form 36 (SF-36) Energy Expenditure Index (EEI), 6-Minute Walking Test (6MWT) and 10-Meter Walking Test (10MWT) were used for the evaluation of subjects. Patients in the salvage group were also evaluated radiologically with Graves' radiological assessment method and Freiburg ankle scoring system. All patients were classified as grade 5 according to FAS. All SF-36 subgroup values were higher in the amputation group whereas only those of general health and vitality reached statistical significance (p < 0.05). The visual analogue scale (VAS) has been used to assess the efficacy of pain management. Mean VAS scores were found to be statistically higher in the salvage group (p < 0.005). Reoperation rates were one in 10 amputee and six in nine salvage patients. Mean Freiburg ankle scores of the patients in the salvage group were 55.33 ± 15.51 which was consistent with moderate functionality. According to Graves' radiological assessment; four patients had grade 3 degeneration, four had grade 2 and one had grade 1 degeneration in the ankle joints. Mean EEI values, 6-MWT and 10-MWT results were not significantly different between the groups (p values > 0.05). Although amputation still remains as the last resort both for patients and the physicians, our results demonstrated that reoperation rates, quality of life (general health and vitality) and pain scores were better in amputee patients.
Introduction
Currently, it is quite difficult for surgeons to decide clinically whether to perform an amputation or salvage surgery following a complex extremity trauma.1,2 Although many factors including expected functionality, cosmetic image, pain and lack of sensation in the salvaged limb, time period for recovery, treatment cost, emotional and psychological factors, premorbid condition of the foot and ankle, condition of the non-injured contralateral extremity, age, smoking, diabetes and vascular insufficiency are considered for the decision of amputation vs. salvage surgery;3 the decision is mainly substantiated by the experience of the surgeon subjectively.
Amputation may seem to be a treatment alternative that causes an unfavorable eventual image for the patient, the family and the social environment. Therefore, various problems are usually encountered in clinical practice at the time of patient's or the family's acceptance for the amputation decision.4 Either due to such attitudes or the developments in microsurgery, a trend towards salvage surgery – where otherwise amputation would be carried out – emerged recently. Accordingly, the decision for amputation surgery has become even more challenging for severe lower limb trauma. On the other hand, despite all these developments in reconstructive surgery, the main criteria including functional outcome, cosmetic image, treatment duration and cost-effectiveness have not much changed. It is well known that the duration of hospital stay and treatment costs are more in salvage patients and to our best notice, there are only few studies that have evaluated the functionality of salvage patients until now.5-7 Those studies have mainly focused on the gait parameters and quality of life; however energy expenditure has not been assessed before. Therefore, the aim of this study was to compare the functionality – including the energy expenditure which is an objective, reliable and quantitative method – during daily activities and quality of life of patients with transtibial amputation vs. salvage surgery after severe lower extremity trauma.
Materials and methods
Patients
Patients were recruited from the soldiers of the Turkish Armed Forces with severe lower limb trauma and who were under rehabilitation in Turkish Armed Forces Rehabilitation Center between September 2006 and May 2007. The soldiers of the Turkish Army receive basic military training before they start military service. As all patients were young males who were soldiers with military training, we assumed that all of them had similar physical capacity. Those individuals who had the following criteria were included in the study: Being at least on the 3rd month of postoperative period, having completed primary wound healing, having stable medical condition and independent mobilization (grade 5 according to Functional Ambulation Scale). Those who had concomitant other system injuries that would impede gait patterns, traumatic brain injury, spinal cord injury, neurological, vascular, pulmonary and psychological/mental disorders were excluded. Subjects who were immobilized for long periods were also excluded. Overall, 10 patients with unilateral below knee amputation and nine patients with salvage surgery were enrolled.
All subjects had previously completed a rehabilitation program that comprised range of motion, strengthening exercises, balance and gait education, occupational and psychosocial rehabilitation. They were recruited in the study during their readmissions for other reasons. All patients were informed about the study and they gave consent to participate. The study was approved by Gülhane Medical Academy Ethics Committee.
Assessment instruments
Functional Ambulation Scale (FAS) is a simple and sensitive evaluation method of ambulation which is often used during active rehabilitation. It especially shows the external support needs of a patient during ambulation, so It was applied for the evaluation of independent mobility.8,9 The visual analogue scale (VAS) has been used to assess the efficacy of pain management regimens in patients during daily activity. Pain measured by SF-36 does not specifically evaluate local pain but VAS can be used to quantify such painful conditions. Therefore we used VAS (to assess stump pain in amputees and local limb pain in salvage patients) especially after the walking tests (6-MWT, 10-MWT, EEI). The VAS frame measures exactly 10 cm.10 Turkish validated version of Short form 36 (SF-36)11 was used for the assessment of quality of life scores (on all subscales scores range from 0 to 100, with higher scores indicating better health status).12
Postoperative ankle movement limitations, degeneration and consequently functional loss are common after limb (foot) salvage operations. Accordingly, patients in the salvage group were also evaluated with Graves' radiological assessment method (graded between 0 and 3 where higher grades indicate worse degeneration)13 – which has been used to evaluate ankle joint degeneration in previous studies.14 Functionally with Freiburg ankle scoring system which evaluates the ankle function with a total of 100 points where higher scores indicate a better ankle function.15
Energy expenditure index (EEI), 6-minute walking test (6MWT) and 10-meter walking test (10MWT) were performed for the evaluation of the energy expenditure and the functional capacity of the patients. The 6 MWT and 10 MWT were performed consecutively with a sufficient resting time interval. EEI was performed on a subsequent day. All tests were performed after the completion of the rehabilitation program during the current hospitalization.
The EEI was measured by using Vmax 29C Sensor Medics, California, USA. In order to make the subjects familiar with the testing procedure, detailed explanation was given and they were asked to exercise 5 minutes before the testing. Before each walking test, the patients had a resting time of 5 min. For EEI, the patients were tested four times in accordance with our department's protocol as follows: Walking 5 min on the treadmill (plain) with 1.5 km/h velocity and 5 min with 3 km/h velocity, walking 5 min on the treadmill (with 5° inclination) with 1.5 km/h velocity and 5 min with 3 km/h velocity. During the testing procedure, patients' oxygen consumption, ventilation parameters and heart rates were monitored. Patients were allowed to rest before each walking test. Mean oxygen consumption (ml/kg/min) within the last two minutes of every test was taken into analysis.
The subjects were asked to walk for 6 min in their regular walking rhythm without any encouragement in the corridor of the ward (30 m). At the end of the test, the total distance was recorded in meters.16
In order to determine the walking speed of the patients, we used 10 MWT17,18 which is safe and convenient. The subjects were asked to walk 10 m on a straight line at a speed similar to their daily activities. The time elapsed was determined by a chronometer and the speed was calculated in m/sec. After two consecutive speed measurements, the average speed of the subject was calculated.
Three patients in the salvage group were using silicon orthoses and as we asked the patients to perform the tests in their most comfortable condition. Those three subjects preferred to carry out all the tests with their orthoses.
All of the functional tests were performed by an experienced physiotherapist, VAS and SF-36 were self administered by the patients.
Statistical analysis
All data were analyzed by Statistical Package for Social Sciences version 15.0 for Windows. Mann-Whitney U, Chi-square and Spearman correlation tests were used. Statistical significance was set at p < 0.05.
Results
Demographic features of the patients
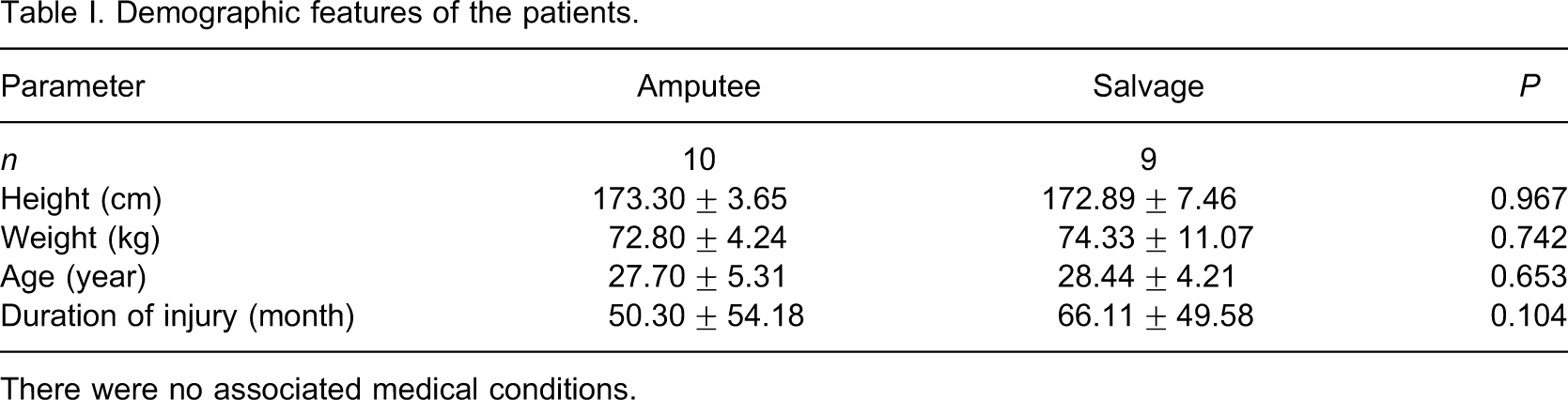
There were no associated medical conditions.
While all of the amputee patients were injured by high-energy land mine explosions, six patients in the salvage group had land mine injuries and three patients had close gun shot injuries.
Comparison of data pertaining to patients in each group
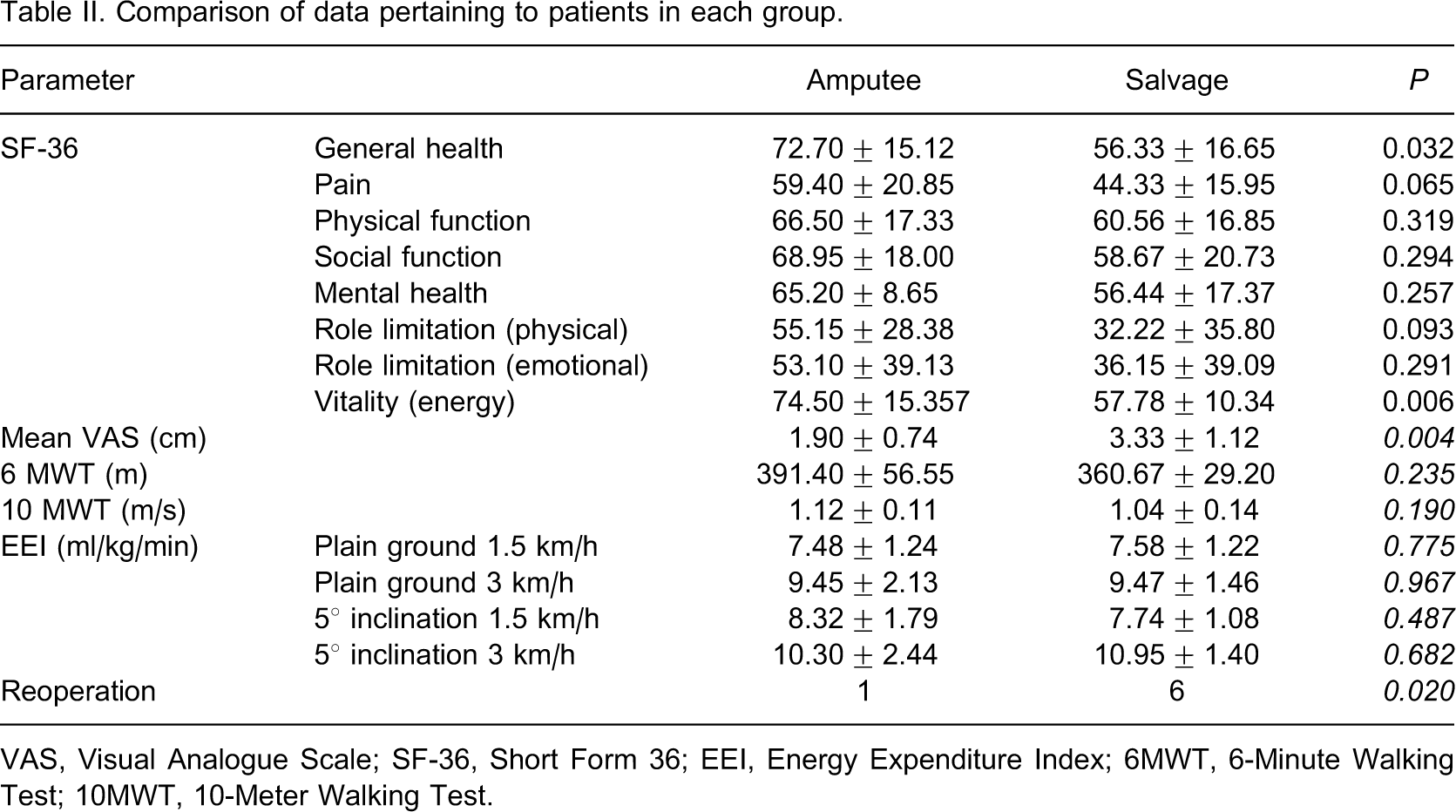
VAS, Visual Analogue Scale; SF-36, Short Form 36; EEI, Energy Expenditure Index; 6MWT, 6-Minute Walking Test; 10MWT, 10-Meter Walking Test.
Mean Freiburg ankle scores of the patients in the salvage group were 55.33 ± 15.51 which was consistent with moderate functionality. According to Graves' radiological assessment; four patients had grade 3 degeneration, four had grade 2 and one had grade 1 degeneration in the ankle joints. Mean EEI values, 6-MWT and 10-MWT results were not significantly different between the groups (all p values >0.05).
Discussion
In this study, functionality and life quality of patients with transtibial amputation and salvage surgery were compared; although gait parameters were found to be similar between the groups, quality of life (general health and vitality) and pain scores were different.
Subjects with lower limb sequelae after traumatic injuries are exposed to several physical, psychological and social problems. In our study, we have used SF-36 for the assessment of quality of life. This practical and widespread tool19,20 has been previously used and validated in amputee patients.5,21-24 Dagum et al.24 found a significant difference in SF-36 physical function scores – but not in mental summary scores – in favor of limb salvage over amputation. On the other hand, when amputee and non-amputee patients were compared, SF-36 scores were reported to be worse in the amputee group.22,23,25 In our study, we found significantly better vitality and general health scores in the amputation group (Table II). Amputee patients are usually encouraged by physicians and the social milieu towards sportive activities. However, as lower limb salvage patients are categorized in between healthy and handicapped, and as they are usually instructed by the physicians to protect their limbs, eventually these subjects are prone to inactivity. Therefore, we believe that the difference in vitality scores is due to the fact that amputee patients are much more active and motivated in their lives.
It is well known in the literature that salvage patients may encounter many complications like prolonged hospital stay, numerous operations and sometimes amputation of the nonfunctional extremity.1,26-28 Likewise, in our study six of nine salvage patients and one of 10 amputee patients were hospitalized for a revision surgery. Thus, patients may suffer physically, psychologically, socially and financially and we believe that the group differences in the general health subscale scores of the SF 36 also stem from this fact. The majority of the amputee patients in our study were hospitalized for routine follow-up concerning rehabilitation or prosthesis care; whereas many of the salvage patients were hospitalized for complications (infection, bone growth etc.). Pain control in amputee patients may therefore be easier than salvage patients. The difference between the groups regarding VAS scores could be due to these issues. Nevertheless, the difference in SF 36 pain domain was not significant. We attributed this difference to the fact that some patients would score (general) pain in SF-36 less precisely due to their intellectual differences (i.e., educational background); however VAS pain scoring is more specific and the patient can quantify it. Therefore, VAS scores were mainly taken into account.
EEI is an objective, reliable and quantitative method determining the energetic penalty of gait disability and a patient's functional performance ability. The O2 cost per meter is directly related to the extent of the patient's gait disability.29 Interruptions in the normal gait cycle and the energy conserving characteristics of trunk and limb motions result in increased energy expenditure.30,31 Nevertheless, in response to a gait disability, a patient will adapt by performing compensatory gait substitutions to minimize the additional energy expenditure30 and such changes are usually paralleled with decreased gait speed.32 Accordingly, to avoid any misinterpretation, we had the subjects walk at two different speeds and on both flat and inclined treadmill. Our results did not show any difference between the groups; but further studies are awaited to confirm our preliminary findings. Yet, in the literature, there are studies that have compared the EEI among individuals with different amputation levels33,34; but there are no studies measuring the EEI between individuals with different surgical approaches.
Functional ambulation requires the individual to traverse a certain distance to perform various daily living activities.35 This has been reported to be 300 m walking distance with an average walking speed of 1.33m/sec (range: 1.0–1.67 m/sec)36,37 which indicates that majority of the daily living activities can be done with an average of 5-min-walking. Our patients were tested at their comfortable speeds for six minutes. There was no significant difference between the groups and every individual in each group could finish the testing. In other words, independent from the surgical technique they had functional ambulation. Further, walking speeds between the groups were not significantly different and the patients' preferred speeds were within the aforementioned normal range. Majority of our patients were previously healthy young military personnel; therefore, we believe that age had a favorable effect on the functional outcome of our patients in either group.
Although all salvage patients had various degrees of degeneration in the ankle joints and had moderate functionality with respect to the Graves' radiological assessment method and Freiburg ankle scoring system respectively, their performance test results (Table II) were similar to normal values.35-37 Therefore we imply that ankle degeneration did not seem to affect the eventual functions of these patients.
The first and perhaps the most important drawback of this study is the limited number of subjects and secondly the fact that majority of the amputee patients were hospitalized for routine follow-up during their rehabilitation. On the contrary, the salvage patients were mainly hospitalized for various medical complications. Moreover, since our amputee group comprised war veterans that were treated with the most suitable prosthesis, the results may not correctly reflect the general population where social security systems may assert financial limitations, which may have an impact on the functionality. The current sample was comprised of young soldiers. This is clearly a specialized sample thus the results may not be generalizable to the wider community.
Conclusion
In closing, although amputation still remains as the last resort both for patients and the physicians, our results demonstrated that reoperation rates, general health and vitality – two domains associated with the measure of health-related quality of life and pain scores – were perceived better by amputee patients when compared to non-amputees. Further studies with larger samples that also represent the general population are awaited. Last but not least, no matter which type of surgical procedure is applied, we advocate that early rehabilitation, thus close cooperation of surgeons and rehabilitation physicians is paramount in this regard.