
Abstract
The aim of this study was to investigate associations between post-amputation phantom and residual limb pain and prosthesis satisfaction, activity restriction and psychosocial adjustment to amputation among lower limb prosthesis users. Eighty-nine people with a lower limb amputation completed a postal survey. Characteristics of phantom and residual limb pain, prosthesis satisfaction, activity restriction and psychosocial adjustment to amputation were assessed using the Trinity Amputation and Prosthesis Experience Scales (TAPES). Comparisons of those who experienced residual and/or phantom limb pain in the preceding assessment with those who did not revealed significant differences in prosthesis satisfaction, psychosocial adjustment but not in activity restriction. Overall, it is important for clinicians to ascertain the type and level of pain that the person is experiencing and to separate the experiences of the pain from the experiences of the prosthetic limb.
Introduction
Clinicians working with amputees acknowledge that there are many factors other than the severity of the amputation that are likely to affect the clinical outcome. The Trinity Amputation and Prosthesis Experience Scales (TAPES; Gallagher and MacLachlan 2000) were developed to assist clinicians in assessing the patient's status. In this study, we describe the associations between pain, activity levels, prosthesis satisfaction and psychosocial adjustment in lower limb amputees.
Many individuals with amputations experience significant amputation-related pain both in the early post-amputation period and longer term (Gallagher et al. 2001; Ehde et al. 2003; Ephraim et al. 2005). Although prevalence estimates vary considerably (see Borsje et al. 2004, for commentary), amongst individuals with lower limb amputations phantom limb pain (i.e., pain in the missing portion of the amputated limb) prevalence of up to 85% has been reported (Sherman and Sherman 1983; Sherman et al. 1984), while prevalence of residual limb pain, pain in the remaining part of the limb (sometimes referred to as stump pain), as high as 76% has been documented (Smith et al. 1999; Ehde et al. 2000). In addition, significant associations between occurrence, frequency, and intensity of residual limb pain and phantom limb pain have been documented (Kooijman et al. 2000; Gallagher et al. 2001).
Chronic pain has been highlighted as a significant risk factor for affective distress in a variety of clinical populations (Von Korff and Simon 1996; Geerlings et al. 2002). However, evidence for an association between chronic post-amputation pain and affective distress is limited and inconclusive. Investigations to date have largely focused on associations between phantom limb pain and emotional distress (Fisher and Hanspal 1998; Katz and Melzack 1990; Datta et al. 2004). Fisher and Hanspal (1998) found no association between phantom pain experience and emotional distress. Similarly, Katz and Melzack (1990) reported that individuals with phantom pain, painless phantom sensations or no phantom sensations could not be distinguished in terms of their scores on depression or anxiety inventories. In contrast, considering both phantom and residual limb pain, Desmond and MacLachlan (2006) found that phantom, residual limb pain and the combination of these pain experiences were differentially associated with emotional distress indicators. While anxiety scores were higher among all pain groups when compared to those who did not experience either phantom or residual limb pain, only those who experienced both phantom and residual limb pain reported significantly elevated trauma symptoms. In addition, both the residual limb pain alone and combined phantom limb and residual limb pain groups (but not the phantom limb pain alone group) could be distinguished from those who did not experience either phantom or residual limb pain with respect to intrusion (a core phenomena of traumatic stress) and depressive symptomatology. Similarly, Darnall et al. (2005) found that being bothered by either phantom limb pain or residual limb pain was a significant risk factor for depressive symptoms.
In the wider literature on chronic pain, there have been few studies on everyday activity levels (van den Berg-Emons et al. 2007). In lower limb amputees, greater attention has been paid to the relationship between phantom limb pain and activity levels than residual limb pain and activity. Some recent work has suggested that those experiencing phantom pain do not perceive it as significantly disabling (Ehde et al. 2000; Gallagher et al. 2001). For example, Ehde et al. (2000) found that 75% of respondents in their sample who experienced phantom limb pain fell into the two low pain-related disability categories as assessed using the Chronic Pain Grade (Von Korff et al. 1992) whereas approximately 8% (n = 14) were categorized as grade IV (i.e., high disability, severely limiting). Limited investigation of functional limitations and activity restriction as a consequence of residual limb pain has also been conducted. For example, Gallagher et al. (2001) report that a third of respondents experienced ‘moderate’ to ‘a lot’ of interference with their normal lifestyle activities as a result of residual limb pain. Similarly, Ehde et al. (2000) reported an average ‘bothersomeness’ rating of 5.2 (on a 10-point VAS scale; SD = 2.9) with 60% of participants describing their residual limb pain as ‘moderately’ or ‘very bothersome’. Ehde et al. (2000) suggest that for many residual limb pain results in greater distress and restriction of activities than phantom limb pain.
In light of the wide variation in psychosocial adjustment to amputation and the potential for post-amputation pain to mediate such outcomes, our research investigates associations between post-amputation phantom and residual limb pain and prosthesis satisfaction, psychosocial adjustment to amputation and activity restriction. While a number of studies have considered adjustment in the context of either phantom or residual limb pain, to date few studies have addressed the potential cumulative effect of these conditions. It is also important to review this within the context of the clinical setting.
Method
Participants and procedure
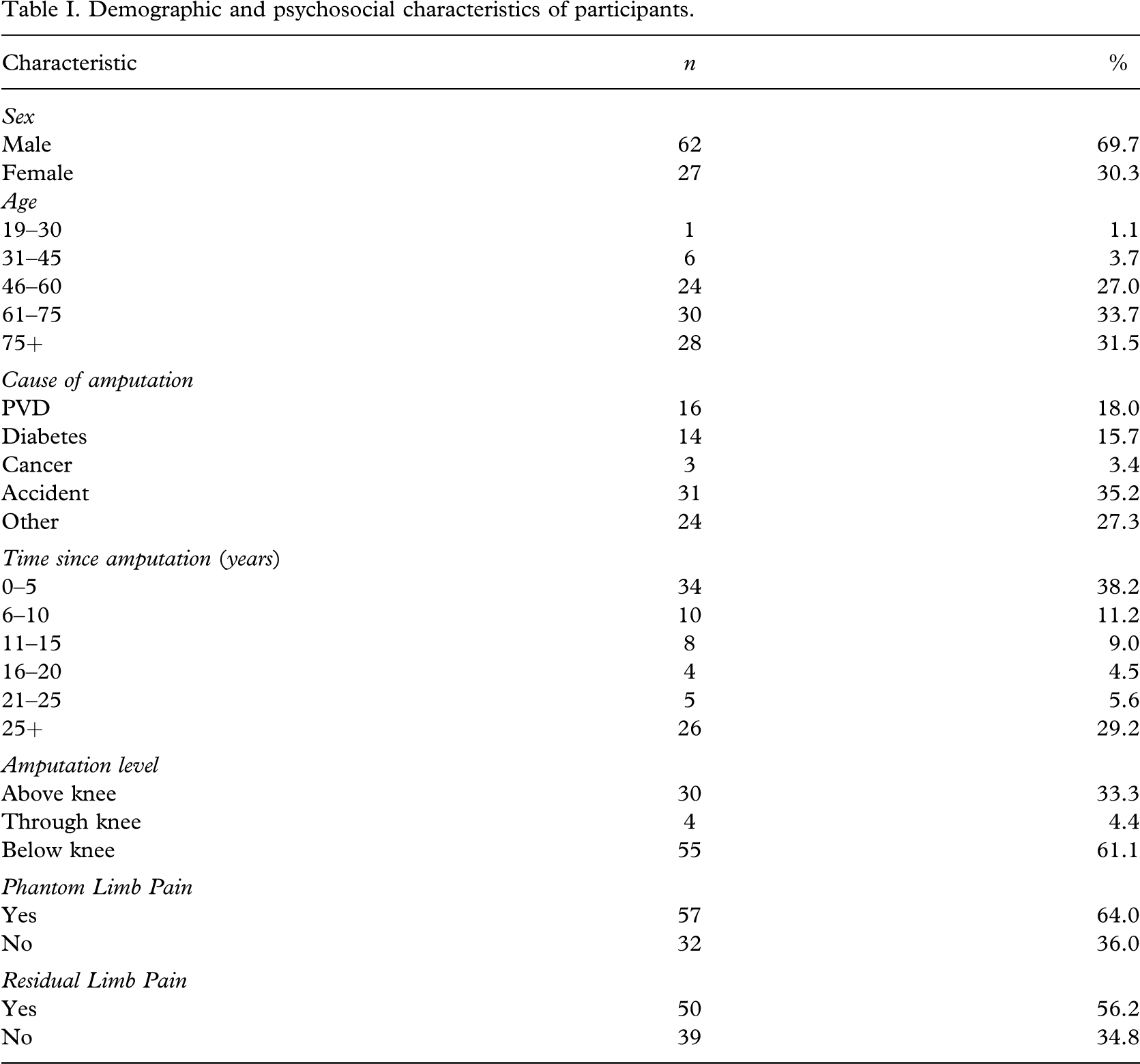
Eighty-nine people who were at least 18 years of age and attending a rehabilitation/limb fitting centre completed a postal questionnaire. The characteristics of the sample are detailed in Table I. The majority of participants were male (69.7%), had transtibial amputation (61.1%) and were older than 60 years of age (65.2%).
Demographic and psychosocial characteristics of participants
Outcome Measures
The Trinity Amputation and Prosthesis Experience Scales (TAPES; Gallagher and MacLachlan 2000) is a multidimensional assessment of adaptation to amputation and prosthesis use developed specifically for use with individuals with lower limb amputations. The TAPES comprises three Psychosocial Adjustment subscales, three Activity Restriction subscales and three Prosthesis Satisfaction subscales. The final section of the TAPES includes an assessment of other medical problems and phantom and residual limb pain experience. Details of the psychometric characteristics and validity and reliability data can be found in the following (Gallagher and MacLachlan 2000, 2004). (The TAPES is freely available and can be downloaded at www.tcd.ie/psychoprosthetics).
Psychosocial adjustment
The General Adjustment subscale reflects the extent of adjustment to and acceptance of an artificial limb. Social Adjustment pertains to the influence of the artificial limb in social situations, encompassing ease of talking about the limb and dealing with others' reactions to it. The Adjustment to Limitation dimension reflects restriction ensuing from having an artificial limb. The five items on each of these subscales are rated on a 5-point Likert scale and are summed to give a score ranging from 5–25, with higher scores indicating more favourable adjustment.
Activity Restriction
The three Activity Restriction subscales reflect different arenas where limitation of pursuits or interests may be manifest. The Functional Restriction subscale covers rudimentary functional tasks such as ‘walking 100 yards'. Athletic Restriction refers to limitation of activities that involve more dynamic physical effort, for instance ‘sport and recreation’ and ‘running for a bus'. The final Activity Restriction dimension, Social Restriction, addresses limitation of social activities such as ‘visiting friends' and ‘working on hobbies'. The four items on the Activity Restriction subscales are scored on a three-point scale ranging from ‘limited a lot’ (2) to ‘not limited at all’ (0) and are summed to give a score from 0–8. Higher scores indicate greater limitation.
Prosthesis Satisfaction
The Functional Satisfaction subscale assesses extent of satisfaction associated with the following functional characteristics of the artificial limb: ‘reliability’, ‘comfort’, ‘fit’, and ‘overall satisfaction’. Aesthetic Satisfaction reflects contentment with cosmetic characteristics such as ‘shape’, ‘colour’ and ‘noise’, while the final subscale Weight Satisfaction is a single item measure assessing satisfaction with the weight of the prosthesis. Items are rated on a 5-point scale ranging from ‘very dissatisfied’ (1) to ‘very satisfied’ (5). Higher scores indicate greater Prosthesis Satisfaction.
Phantom limb pain and residual limb pain
The residual and phantom limb pain sections of the questionnaire comprise questions relating to (a) whether pain is experienced; (b) frequency of pain episodes in the previous week; (c) average duration of typical pain episodes; (d) average intensity (mild, discomforting, distressing, horrible, excruciating); and (e) extent to which pain interferes with normal lifestyle activities (not at all, a little bit, moderately, quite a bit, a lot). Phantom pain was defined as ‘pain in the part of your limb that was amputated’. Residual limb (i.e., stump) pain was defined as ‘pain in the remaining part of your amputated limb’. The initial cut-off points applied were ‘yes’ and ‘no’, where ‘no’ represents never experiencing phantom or residual limb pain and ‘yes’ represents a wide range of pain experience from pain once a year to constant pain. For both types of pain, frequency and average duration of pain episodes in the week prior to assessment were recorded; thus a point prevalence estimate for ‘active’ phantom and residual limb pain is also provided. Among those reporting active phantom limb and residual limb pain, the average intensity of pain (mild, discomforting, distressing, horrible, excruciating) in the previous week, and the extent of interference with normal lifestyle activities (not at all, a little bit, moderately, quite a bit, a lot) were evaluated separately.
Data analysis
Continuous variables are presented in terms of mean value, median, standard deviation and range. Initially respondents were divided according to their pain experience (i.e., no phantom or residual limb pain, phantom pain alone, residual limb pain alone, or both phantom and residual limb pain). Differences in the demographic and clinical characteristics of the groups were assessed using chi-square. Differences in Prosthesis Satisfaction, Psychosocial Adjustment and Activity Restriction were investigated using a series of multivariate analyses of variance (MANOVA's) with Bonferonni post-hoc comparisons where appropriate.
Respondents were then classified according to type of pain experienced in the week preceding assessment (i.e., active pain) and a second series of MANOVA's was conducted to determine whether those with active phantom and/or residual limb pain differed from those without active pain in terms of the TAPES dimensions. A p < 0.05 level was chosen for statistical significance.
Results
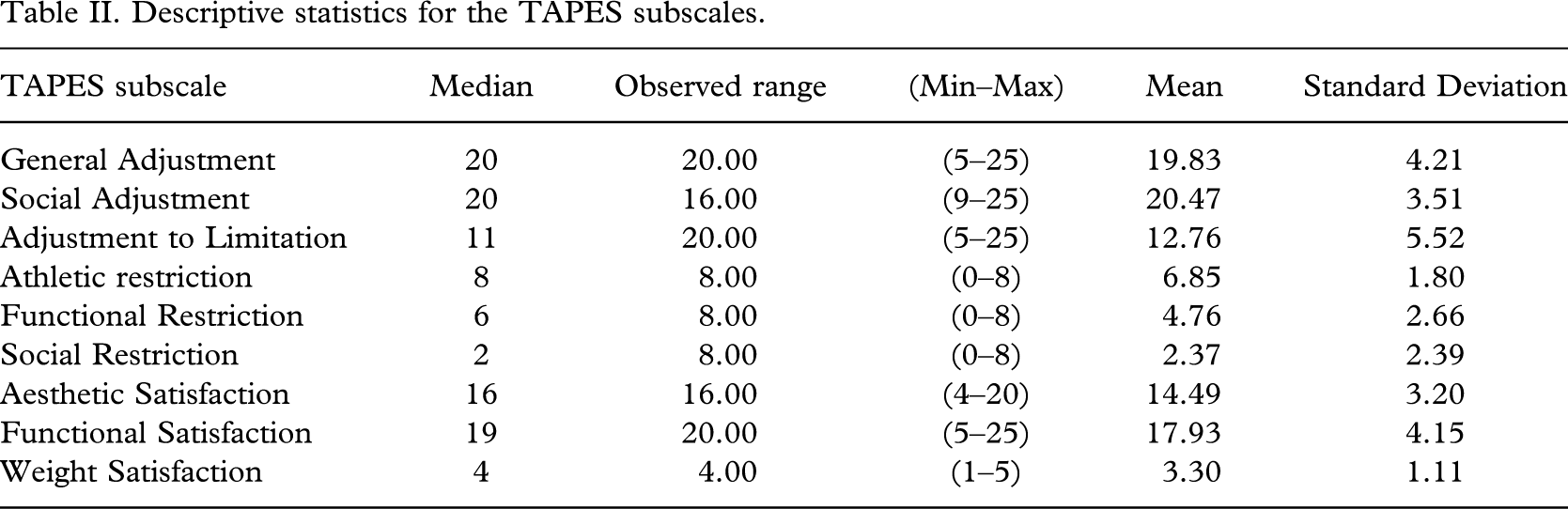
Descriptive statistics for the outcome measures are displayed in Table II. Seventeen people (19.1%) did not experience either phantom or residual limb pain, 22 people (24.7%) experienced phantom pain only, whereas 15 people (16.9%) experienced residual limb pain only and 35 people (39.3%) experienced both phantom and residual limb pain. The four pain groups did not differ with respect to sex (χ2 (3) = 1.312, p = 0.726) or level of amputation (the small number of individuals with through knee amputations were excluded from this analysis; χ2 (3) = 5.082, p = 0.166).
Descriptive statistics for the TAPES subscales
Multivariate analysis of variance showed that the four pain groups did not differ significantly in terms of Prosthesis Satisfaction (F = 1.835, p = 0.063) or Activity Restriction (F = 1.686, p = 0.093) but differed significantly in Psychosocial Adjustment (F = 2.081, p = 0.033). Univariate analyses indicated that this effect was attributable to differences in both the General Adjustment (F (3,81) = 3.186, p < 0.05; partial eta2 = 0.028) and Adjustment to Limitation scales (F (3,81) = 2.831, p < 0.05; partial eta2 = 0.095). Post hoc Bonferonni comparisons indicated that the no pain group had significantly better General Adjustment than those with both phantom limb pain and residual limb pain. The no pain group had significantly better Adjustment to Limitation than those with both PLP and RLP (see Table III).
Results of the univariate tests for all pain groups on Psychosocial Adjustment. Mean and standard deviation on the Psychosocial Adjustment subscales according to pain group
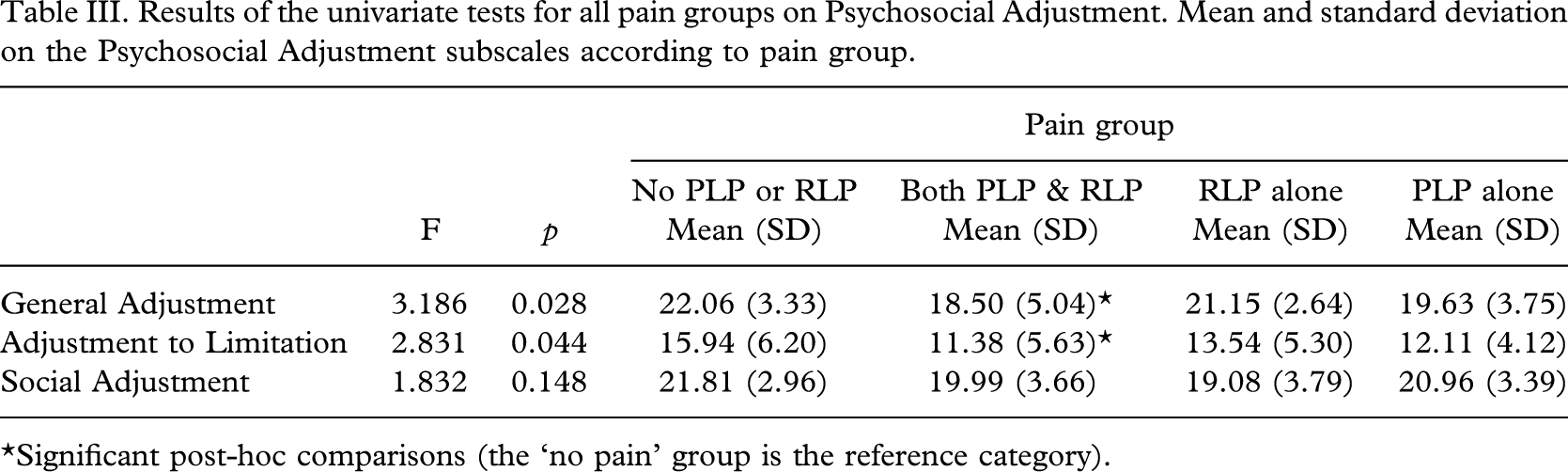
∗Significant post-hoc comparisons (the ‘no pain’ group is the reference category).
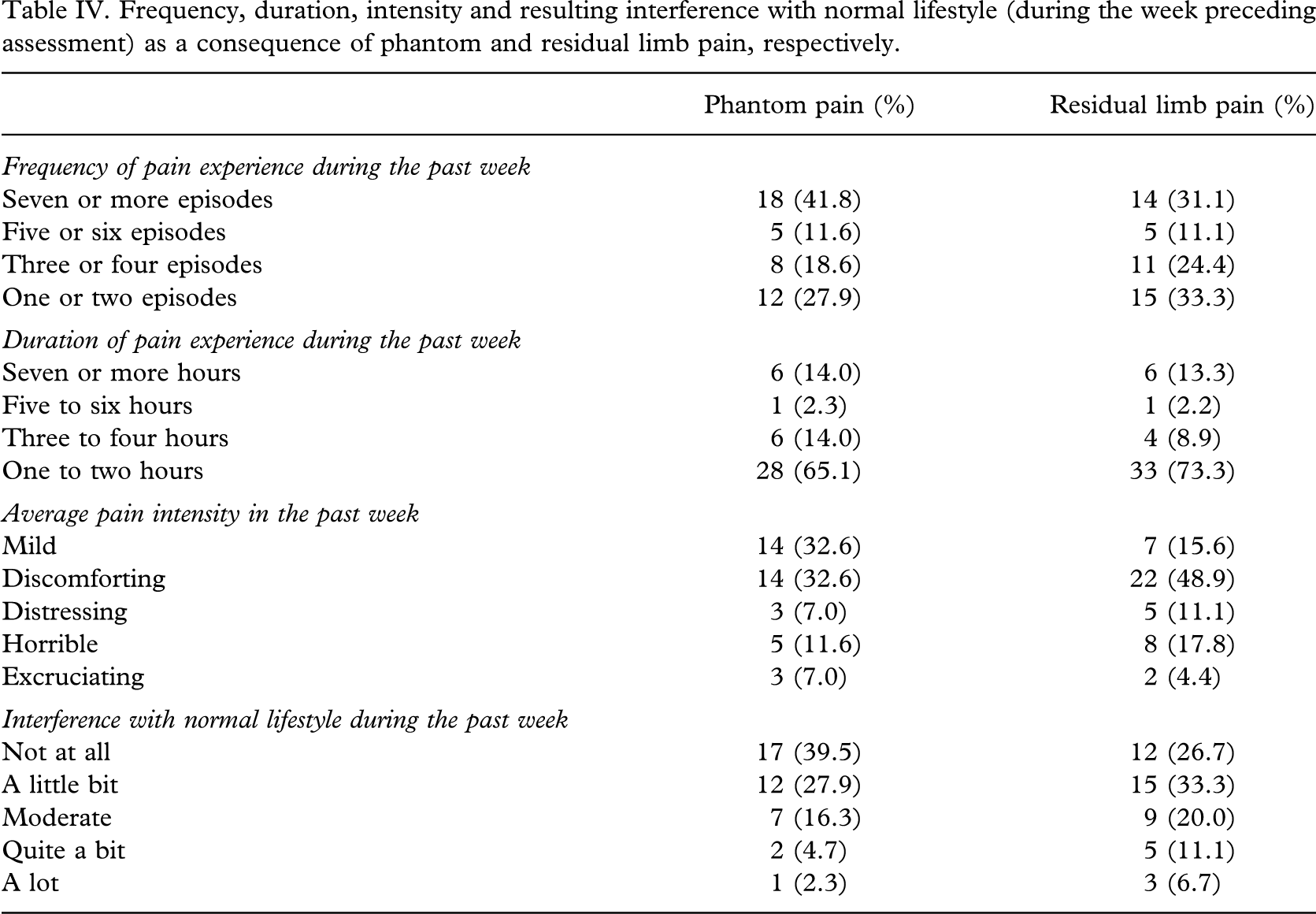
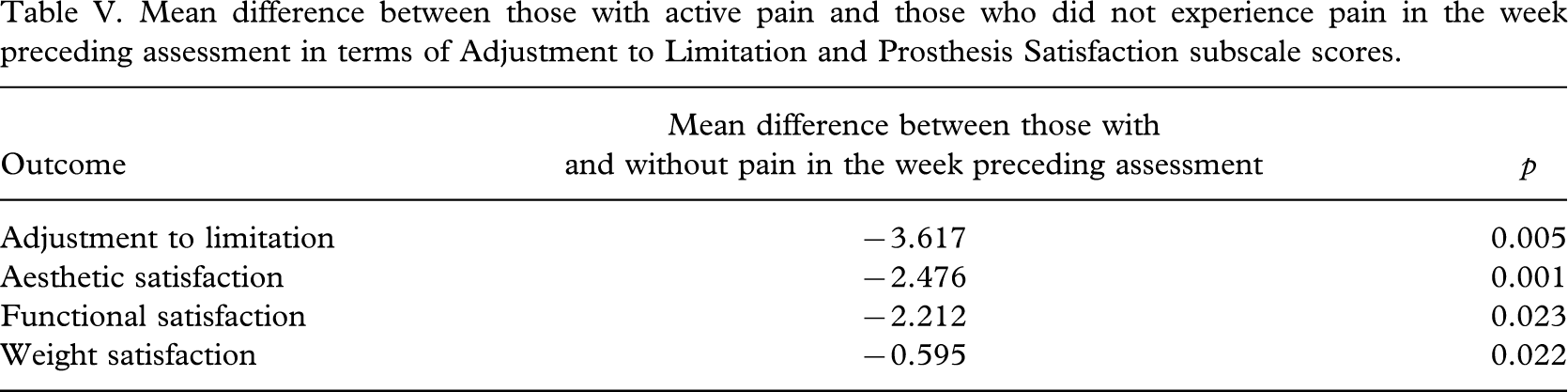
Frequency, average duration, intensity and associated lifestyle interference of pain episodes in the week preceding assessment are detailed in Table IV. Sixty-two people reported pain in the week preceding the assessment. As illustrated in Table IV, 45 individuals (50.6%) reported at least one episode of residual limb pain and 43 respondents reported (48%) at least one episode of phantom limb pain in the week preceding the assessment. Twenty six individuals (29.2%) experienced both phantom and residual limb pain during this period. For a large majority the duration of typical pain episodes was 1–2 hours. The majority of participants rated the average intensity of their pain as mild or discomforting (65.2% and 64.5% for phantom limb pain and residual limb pain, respectively) and their lifestyle interference as minimal (not at all or a little). Comparisons of those who experienced residual and/or phantom limb pain in the week preceding assessment with those who did not revealed significant differences in Prosthesis Satisfaction (F = 4.223, p = 0.008; partial eta2 = 0.135) and Psychosocial Adjustment (F = 3.405, p = 0.022; partial eta2 = 0.112) but not in Activity Restriction (F = 0.825, p > 0.05). Univariate analyses indicated these effects were attributable to significant differences in the Adjustment to Limitation (F(1,83) = 8.422, p = 0.005; partial eta2 = 0.092), Aesthetic Satisfaction (F(1,83) = 12.24, p = 0.001; partial eta2 = 0.128), Functional Satisfaction (F(1,83) = 5.355, p = 0.023; partial eta2 = 0.061) and Weight Satisfaction scales (F(1,83) = 5.413, p = 0.022; partial eta2 = 0.061). Individuals who experienced pain in the week prior to assessment reported significantly lower scores on all three Prosthesis Satisfaction subscales, as well as on Adjustment to Limitation than those who did not (Table V).
Frequency, duration, intensity and resulting interference with normal lifestyle (during the week preceding assessment) as a consequence of phantom and residual limb pain, respectively
Mean difference between those with active pain and those who did not experience pain in the week preceding assessment in terms of Adjustment to Limitation and Prosthesis Satisfaction subscale scores
Discussion
In this study, there was no association between pain occurrence and extent of activity restriction, i.e., although activity restriction was evident, particularly in the athletic activity domain, average levels of activity restriction were comparable across each of the pain groups. This lack of association may be attributable to the small numbers of people experiencing chronic high intensity pain. Jensen and colleagues (2001) demonstrated a non-linear association between pain intensity and its impact on functioning such that higher pain intensities have a proportionally larger negative impact on functioning than lower pain intensities. Furthermore, in our initial analysis the criteria used to define the ‘pain group’ aggregated a diverse array of pain experience. Using a simple ‘yes or no’ cut-off point meant that the ‘pain groups’ potentially comprised a wide range of pain experiences ranging from constant high intensity pain to infrequent low level pain. As the subsequent analyses indicate, however, most respondents who experienced phantom and/or residual limb pain in the week preceding the assessment, i.e., active pain, reported low pain intensity and duration; a patterning consistent with reports elsewhere (Ehde et al. 2000; Gallagher et al. 2001).
Using the ‘yes/no’ classification the current analyses indicate that people who had both phantom limb pain and residual limb pain reported poorer adjustment to limitation and general adjustment than those who did not experience any pain. The combination of these pain experiences has previously been associated with elevated post-traumatic stress disorder symptoms (Desmond and MacLachlan 2006). Thus it appears that the subgroup of people who experience both phantom limb and residual limb pain are vulnerable in terms of psychosocial adjustment and the combination of these pain types warrants particular clinical attention. Comparing those with active pain to those who did not experience pain in the week preceding assessment also revealed differences in terms of adjustment to limitation. It can be postulated that adjustment to limitation relates to participation in life activities as characterised in the International Classification of Functioning Disability and Health (World Health Organization, 2001). Individuals' personal perceptions about their ability to participate in life activities are an important consideration as they provide an indication of the impact of having a prosthesis on the person's life. Consequently, the relationship between the experience of pain and adjustment to limitation highlights the compounding nature of pain on disability and functioning.
The findings of the current study highlight that ‘active pain’, that is, the experience of residual limb pain and/or phantom limb pain in the last week is associated with the dissatisfaction with the prosthesis. Although it is reasonable to expect a relationship between pain and weight and functional satisfaction, it is not immediately obvious why there would be an association between pain and aesthetic satisfaction. Nonetheless, this relationship between pain and satisfaction with the prosthesis gives rise to a number of potential hypotheses that warrant further research where the specific direction of causality can be teased out. For example, it can be hypothesized that pain experience is expressed as dissatisfaction with the prosthesis, that is, pain precedes the expression of dissatisfaction and that the experience of pain is translated into dissatisfaction with all aspects of the prosthesis. This has important implications for clinicians working with lower limb amputees with regard to ascertaining the source of dissatisfaction with the prosthesis. Alternatively, dissatisfaction with the prosthesis may arise with the belief that the prosthesis is directly affecting or bringing about the experience of pain. It is important for clinicians to ascertain the type and level of pain that the person is experiencing and to separate the experiences of the pain from the experiences of the prosthetic limb.
Some caution is warranted with respect to interpretation of these results. The cross-sectional design of this study precludes inferences about the causal link between pain and adjustment variables. Additionally, the survey response rate and self-report nature of the design may be a source of bias. Furthermore, self-reports may be affected by respondents' self-awareness or cognitive functioning. Additional research with larger samples could investigate whether severe phantom limb pain or severe residual limb pain supersedes the experience of residual limb pain and phantom limb pain together. Furthermore, with a sufficiently large sample of people experiencing severe levels of phantom limb pain and/or residual limb pain, more detailed analyses of the relationship between activity levels and pain would be possible.
The need to measure practice and outcomes has gathered increasing attention in recent times. The TAPES is useful in foregrounding the person in the amputation and limb fitting experience alongside the social content, physical demands, stump characteristics and prosthetic characteristics. From a clinical perspective it is a brief self-administered inventory with a simple scoring system. It can be used by any member of the multidisciplinary team to promote client involvement and is a way to standardise existing client interaction. It contributes to the provision of an evidence base for practice. For example, it provides a medium through which psycho-social issues involved in adjustment and the specific challenges of wearing a prosthesis can be examined. It also facilitates the assessment and planning of care programmes for the individual and groups.