
Abstract
An analysis of the take-off technique in transtibial amputee high jump was performed on two athletes (both using intact limb take-off) competing in the high jump finals of the 2004 Paralympic Games. Two digital video cameras were used to film the event with the data later digitized and reconstructed using standard 3D direct linear transformation (DLT) procedures. Some similarities with non-amputee high jump technique were noted in that centre of mass height was low at touch-down (TD), there was a similar magnitude of negative vertical velocity at TD, and most of the vertical velocity generated occurred in the first half of the take-off phase. However, both transtibial amputee athletes exhibited a slower horizontal approach velocity, a lower positive vertical take-off velocity, a more upright position at touch-down and a greater range of motion of the hip throughout the take-off phase compared to what is known about non-amputee high jump technique. These differences may be associated with constraints of taking off from the prosthetic limb on the previous step, resulting in having to adopt a different posture at touch-down compared to non-amputees. Understanding transtibial amputee high jump technique and the differences compared to what is known about non-amputee technique has implications for coaching and improving performance in prosthetic sport.
Introduction
Identifying the biomechanical characteristics associated with successful high jump technique for elite transtibial (TT) amputee athletes performing with a prosthetic limb has not previously been undertaken. To date, transtibial amputees do not take off from their prosthetic limb when performing the high jump. Thus, the effect of the prosthetic limb itself on take-off is not in question, although an attempt does need to be made to understand how transtibial amputees perform high jump in order to improve technique and coaching. While this has been already done for non-amputee athletes, it is a new and necessary area in the development of prosthetic sports, especially when it has been found to be detrimental to performance for amputee athletes to copy an established non-amputee technique (Nolan et al. 2006).
There exists a solid body of evidence for elite non-amputee athletes (Dapena 1987; Dapena and Chung 1988; Conrad and Ritzdorf 1990; Papadopoulos et al. 1995; Greig and Yeadon 2000) providing a description and understanding of the Fosbury flop technique. Studies on non-amputee athletes have divided this high jump technique into three distinct phases: Approach run, touch-down to take-off, and the flight phase including bar clearance. The peak height of the centre of mass (CM) during the flight phase and bar clearance has been found to be dependent on the height and vertical velocity of the CM at take-off (Dapena 1987). This in turn is dependent on approach speed and the position of the body at touch-down.
At touch-down, the foot is planted well ahead of the body which has a backward tilt (Dapena and Chung 1988). This postural configuration allows a low centre of mass position which allows for a better conversion of horizontal to vertical velocity in preparation for take-off. While the foot is still in contact with the ground (the take-off phase), the knee initially flexes then extends (Dapena and Chung 1988; Alexander 1990). The initial flexion has been suggested to cushion the impact (Dyatchkov 1968) as the high jumper touches down with a high horizontal velocity and a small downward vertical velocity. Paradoxically, while the knee is flexing, the centre of mass height is increasing (Dyatchkov 1968; Dapena and Chung 1988), and continues to increase throughout the rest of the take-off phase. Joint angle values and velocities have been documented in several studies, as have the relationships between selected parameters, yet it remains unknown whether TT amputees exhibit a similar technique or whether such relationships between selected parameters also hold for them.
While no studies have previously investigated high jump technique of those with a transtibial amputation, several have reported amputee long jump technique (Nolan and Lees 2000, 2007; Simpson et al. 2001; Nolan et al. 2006). Elite amputee long jumpers exhibit a differing technique to non-amputee athletes at touch-down in terms of a more upright body position, a higher CM and a smaller leg angle due to constraints of taking off from their prosthetic limb on the previous step. Alexander (1990) reported similarities between non-amputee long and high jump techniques in terms of the take-off phase (touch-down to take-off), but with high jumpers having a slower approach run and planting the touch-down leg further in front of their body (a large leg angle). It may be that elite transtibial amputees who perform the high jump using the Fosbury flop technique may display adaptations to the constraints associated with the use of a prosthetic limb. If so, the nature of the adjustments and the purposes they serve has implications for coaching and training. It is known that currently, few amputee athletes compete at elite level in high jump, but the sport is growing. Thus, the aim of this study was to use a case study approach to analyse the high jump technique used by individual elite transtibial amputees (TT) athletes.
Methods
The final of the men's F44-F46 (International Paralympic Committee classification for unilateral transtibial amputees, bilateral transtibial amputees and arm amputees) high jump competition at the 2004 Paralympic Games was filmed using two 50 Hz digital video cameras (Sony, model DCR-TRV33E). The cameras were placed perpendicular to each other so that the last step and take-off were visible in both cameras, regardless of which side the athlete approached the high jump mat. Before competition, a 3-D 18-point calibration frame was placed and filmed in several different locations in front of the high jump mat.
Only two of the 11 competitors in the final were transtibial amputees (TT), both having unilateral amputations. The present analysis thus focuses on these two athletes and their individual techniques. All jumps (successful and unsuccessful) for the two TT athletes were digitized using eHuman digitizing software (HMA Technology, Inc, Ontario, Canada) using a 9 segment model (1 head and trunk, 2 upper arm, 2 lower arm and hand, 2 thigh, and 2 lower leg and foot segments) defined by 18 points (C7, top of the head, bilateral wrist, elbow, shoulder, hip, knee and ankle joint centers, and the toe and heel) (Nolan and Lees 2000, 2007; Nolan et al. 2006). The segmental data used for adult males (Dempster 1955) were modified for each athlete to account for the prosthetic limb (Nolan and Lees 2000). As measurements of the athletes' heights were not available, estimated height for each athlete was calculated as the sum of the length of the individual intact segments (Hay and Nohara 1990; Nolan and Lees 2007; Nolan et al. 2006) from the digitized data. The 3-D coordinates of the digitized points were generated (standard direct linear transformation (DLT) procedure) and filtered using a Butterworth 2nd order filter with a cut-off frequency of 7 Hz using the eHuman software. Kinematics at the key events of touch-down (TD), maximum knee flexion (MKF) and take-off (TO) in the high jump, defined by previous analysis of elite non-amputee athletes, were determined for each jump in the sagittal plane. The eHuman software allowed rotation of the 9 segment model in each of the XY, XZ or YZ planes (Figure 1). Viewing the model in the sagittal plane (YZ), and thus subsequently calculating the chosen parameters in this plane was determined by visual inspection and a repeatability analysis. While there are errors associated with this procedure, to optimize repeatability, the same author digitized all jumps. To report the magnitude of error from this process, one jump was chosen at random and digitized on three separate occasions. Parameters were then calculated for each of the re-digitized trials in the same way as presented above. The variability between these trials (range) was found to be 0 for CM height, 0.15 m · s−1 for vertical velocity, 0.29 m · s−1 horizontal velocity, 1.7° for knee angle and less than 1° for hip and leg angle.
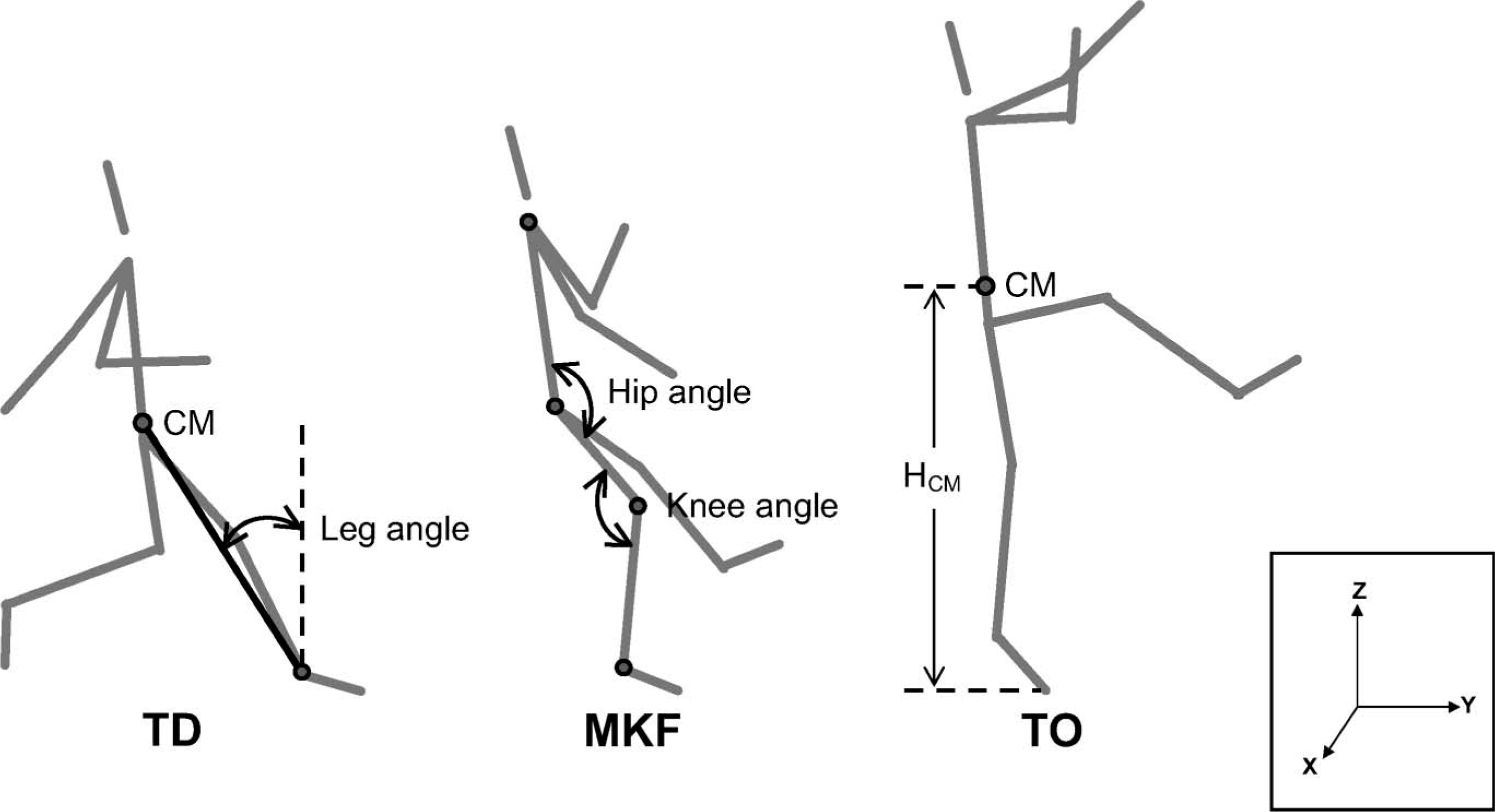
Angle conventions at touch-down (TD), maximum knee flexion (MKF) and take-off (TO).
Whole body centre of mass position was calculated from centre of mass locations of the individual segments using standard procedures. Centre of mass height (CM) was calculated as the vertical distance between the centre of mass position and the vertical coordinate of the toe in contact with the ground. CM was then normalized to individual standing height (%HCM), horizontal (Vhoriz) and vertical velocity (Vvert) of the whole body centre of mass were then calculated. Leg angle, knee angle and hip angle were calculated in the sagittal plane (Figure 1). Changes in the above-mentioned variables in the first half (TD-MKF) and second half (MKF-TO) of the take-off phase were calculated as a percentage of the values over the whole take-off phase (TD-TO). Range of motion of the hip and knee throughout TD-TO was also calculated.
It is assumed that in sport, a sampling frequency of 50 Hz is a little too slow and information at key points such as TD may be missed. To record how much error may be present due to the 50 Hz sampling frequency for transtibial amputee high jumpers, one jump was chosen at random and variables were calculated for the chosen frame of TD and one frame before. The difference in parameters between these two frames represent the maximum error due to the actual point of TD falling between these two points (Nolan et al. 2006). For the CM height and velocity, no difference (when rounding to 1d.p.) was seen between the two frames. For the angles, a maximum difference of 3° was seen. This was within the intra-subject variability for all but Athlete 2's hip angle at TD. Thus for the data presented in thus study it is deemed that 50 Hz is on the limit of acceptability.
As there were only two transtibial amputees in the competition, descriptive data are used to characterize the individual TT high jump techniques from the athletes' successful jumps. In addition, the data will be used to explore the importance of selected kinematic parameters of the technique to successful high jumping for TT athletes, by descriptively comparing unsuccessful jump parameters to successful jump parameters.
Results
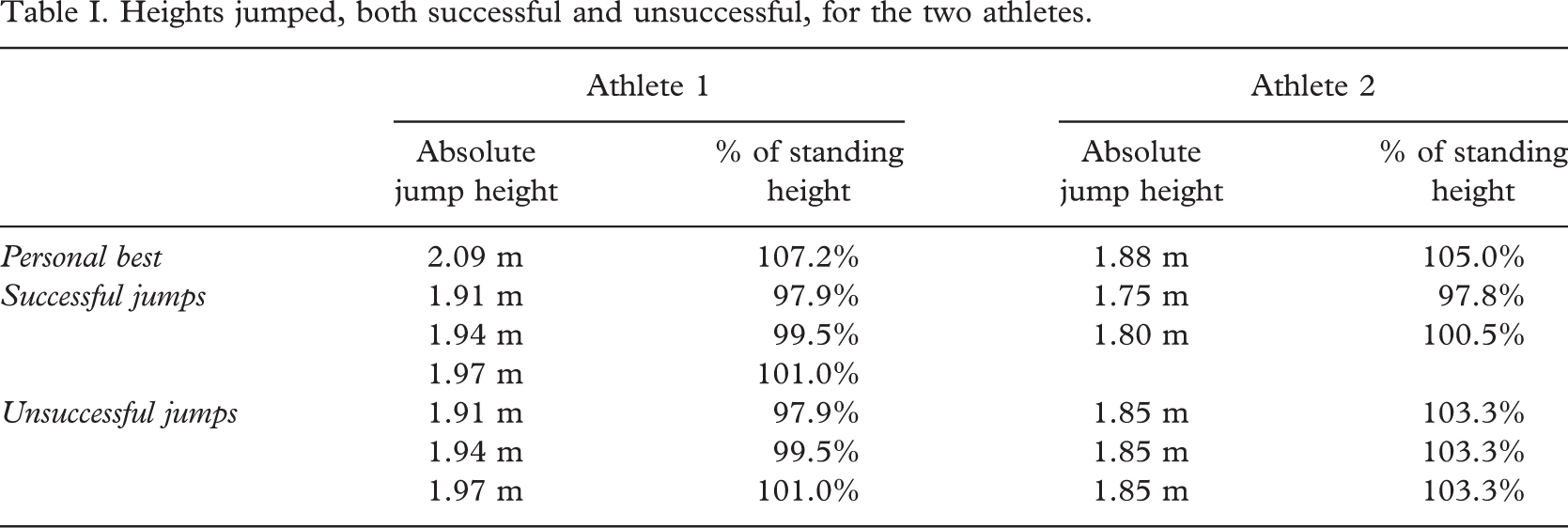
Both athletes used the Fosbury flop technique with a curved approach run, took off from their intact leg and used a flex-foot type prosthesis. Three successful and three unsuccessful jumps for Athlete 1, and two successful and three unsuccessful jumps for Athlete 2 were included in the analysis. Personal bests, successful heights cleared and unsuccessful jumps during the competition are presented in Table I.
Heights jumped, both successful and unsuccessful, for the two athletes.
Athlete 1, who successfully jumped higher than Athlete 2 both in absolute terms and when normalized to standing height (Table I), had the greatest horizontal velocity both at TD and TO (Table II). Vertical velocities of the two athletes were similar, with Athlete 1 having a slightly less negative vertical velocity at TD and a slightly greater vertical velocity at TO than Athlete 2. However, there was no visible relationship between either horizontal or vertical velocity at TD, MKF or TO and successful height jumped for either athlete (Figures 2A, 2B). Most of the horizontal velocity lost and vertical velocity gained during the take-off phase (TD-TO) occurred between TD-MKF. These values were similar for both athletes (Table II).
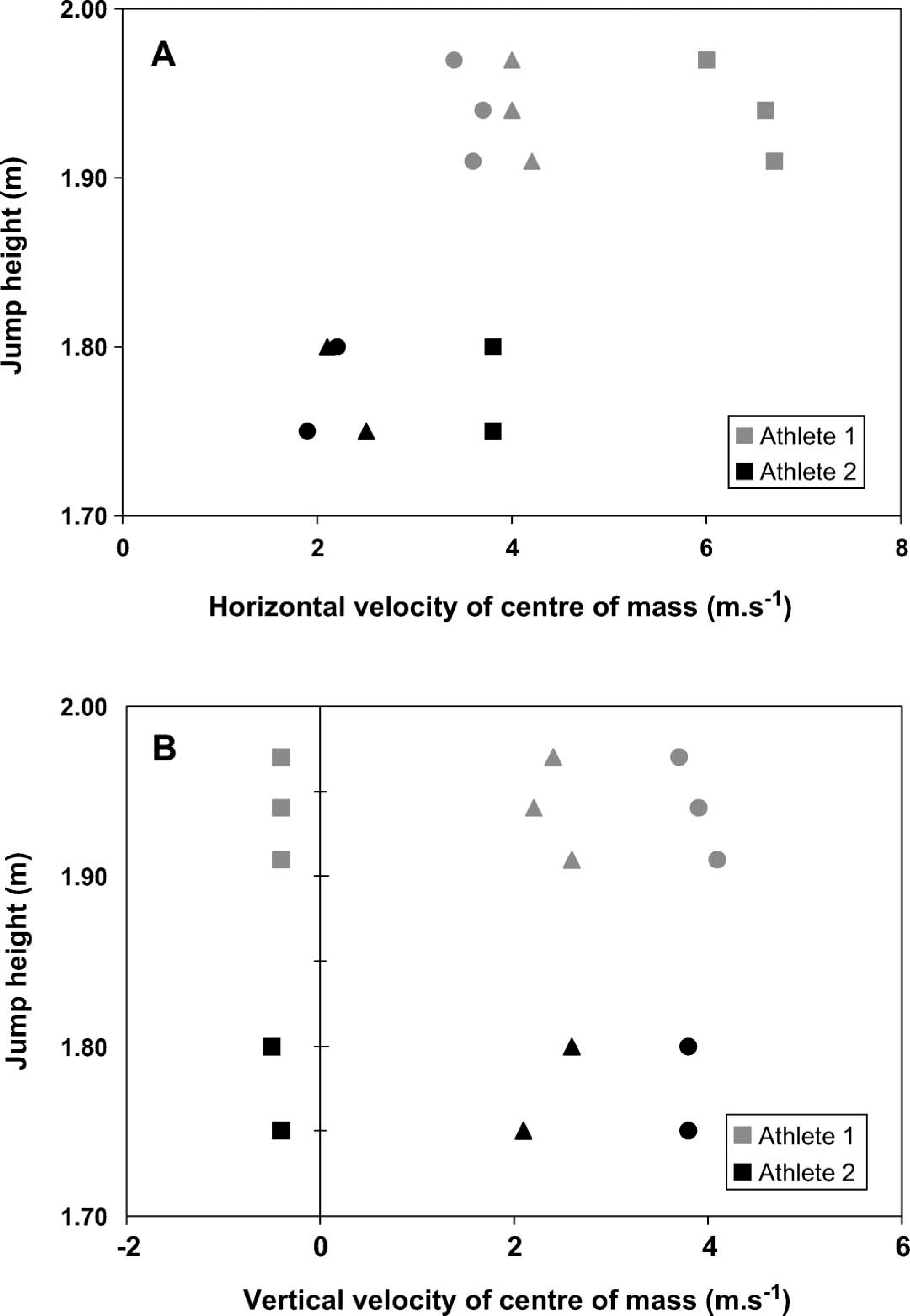
(A) horizontal and (B) vertical velocity of the centre of mass (CM) for each successful height jumped. Indicated are velocities at touch-down (square), maximum knee flexion (triangle) and take-off (circle).
Horizontal and vertical velocity of the centre of mass and relative centre of mass height at touch-down (TD), maximum knee flexion (MKF) and take-off (TO) (mean ± standard error) for the TT athletes' successful jumps.
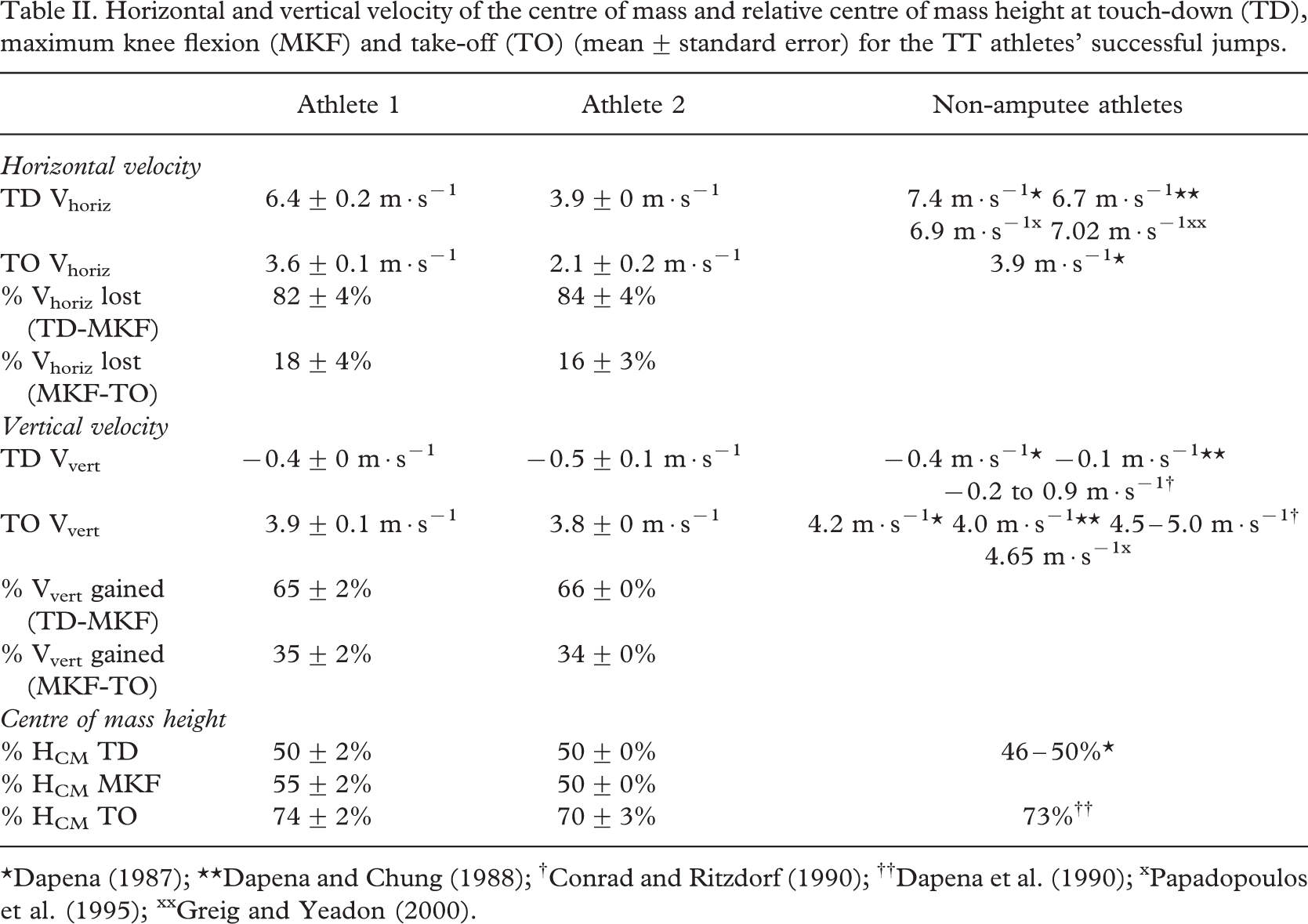
Both athletes had a similar %HCM (centre of mass normalized to standing height) at TD (Table II), but Athlete 1, who jumped higher, had a greater %HCM than Athlete 2 at both MKF and TO. As these athletes did not clear comparable heights it may be that in the need to clear a higher bar, Athlete 1's %HCM needed to be higher than Athlete 2 at TO. However, there was no visible relationship between %HCM at TD, MKF or TO and successful height jumped for either athlete (Figure 3).
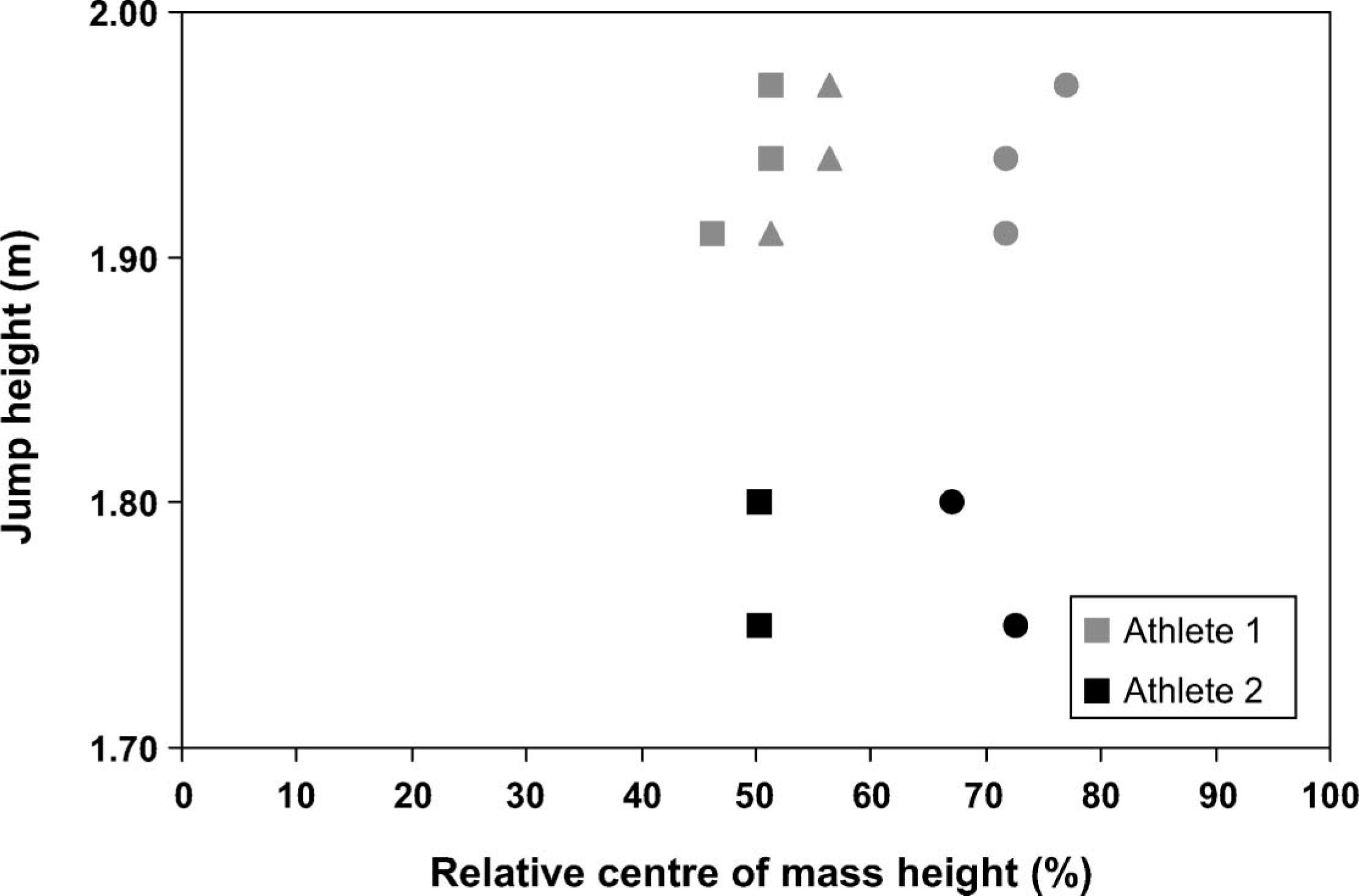
Relative CM height (%) at touch-down (square), maximum knee flexion (triangle) and take-off (circle) for each successful height jumped.
Leg angle at TD was similar for both athletes (27 – 28°) (Table III). Qualitatively there appeared to be a relationship between leg angle at TD and height jumped for both athletes (Figure 4), i.e., the smaller the leg angle (the less far in front of the body the TD leg was placed), the greater height jumped.
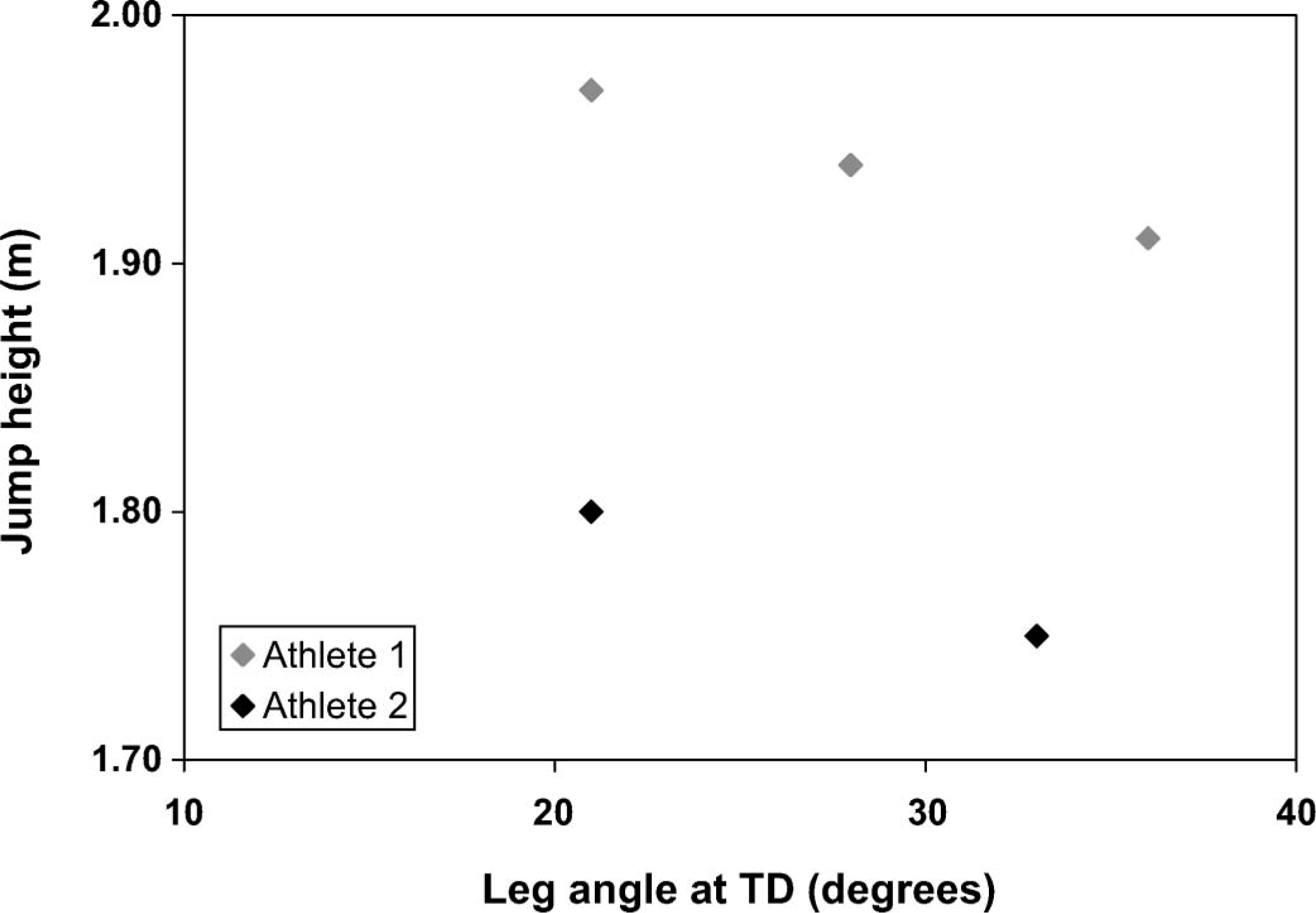
Leg angle at touch-down (TD) for each successful height jumped.
Joint angles at touch-down (TD), maximum knee flexion (MKF) and take-off (TO) (mean ± standard error) for the TT athletes' successful jumps.
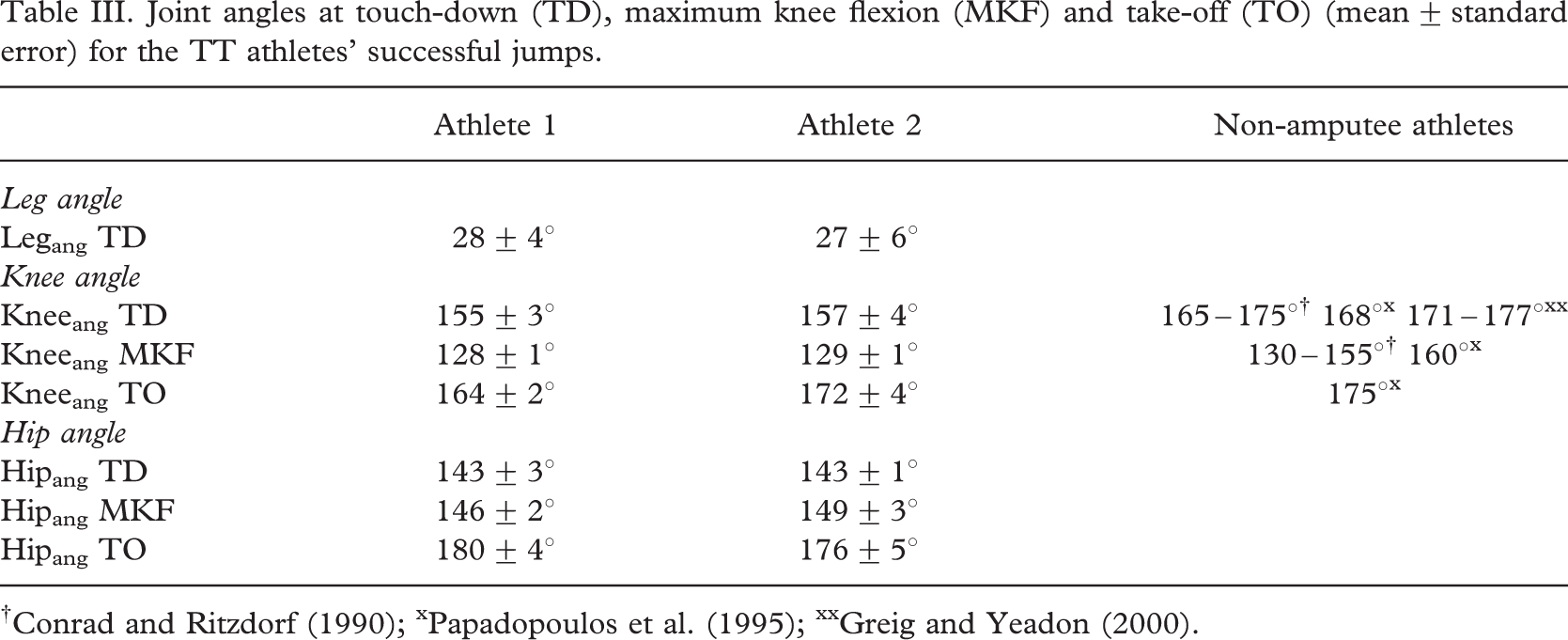
Both TT athletes showed similar knee flexion angles at TD, being flexed more than that reported for non-amputee athletes (Table III). Knee flexion increased to a similar value at MKF for both athletes, again, more flexed than that previously reported for non-athletes (Table III) followed by Athlete 2 having a greater extended knee than Athlete 1 at TO. Thus, Athlete 2 had a greater knee range of motion throughout the take-off phase than Athlete 1 (Figure 5). There appeared to be no relationship between knee angle at TD and successful height jumped for either athlete (Figure 5), nor was there any relationship between knee range of motion and height jumped.
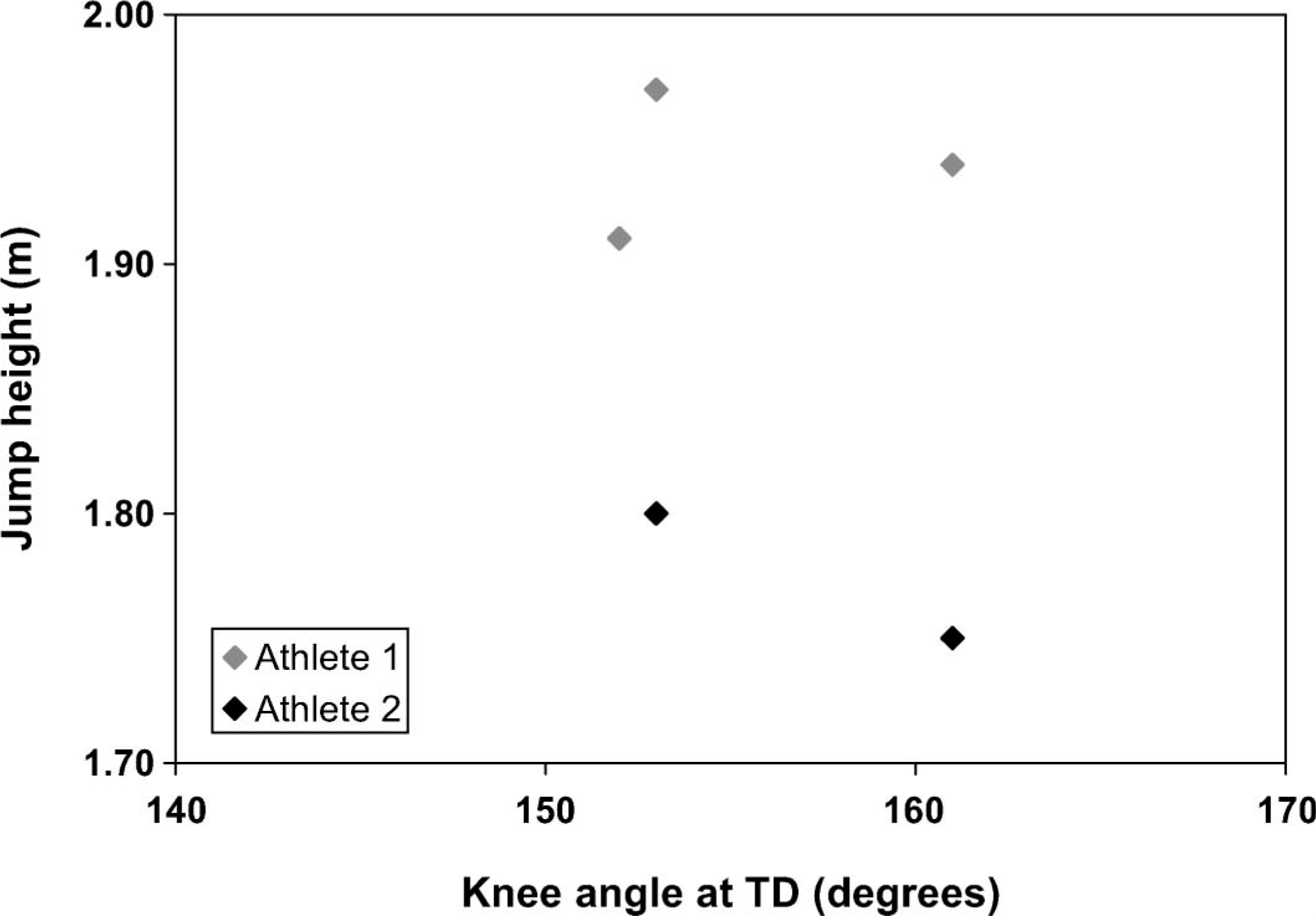
Knee angle at touch-down (TD) for each successful height jumped.
Both TT athletes touched-down with a similarly flexed hip (143°) (Table III). In this postural position at TD, considering the knee and leg angle, the trunk would have to be in an upright position, rather than leaning backwards. After TD, the hip began to extend through MKF and was at approximately 180° extension at TO for both athletes (Table III). Hip ROM during the take-off phase was greater for Athlete 1 compared to Athlete 2 (Figure 6).
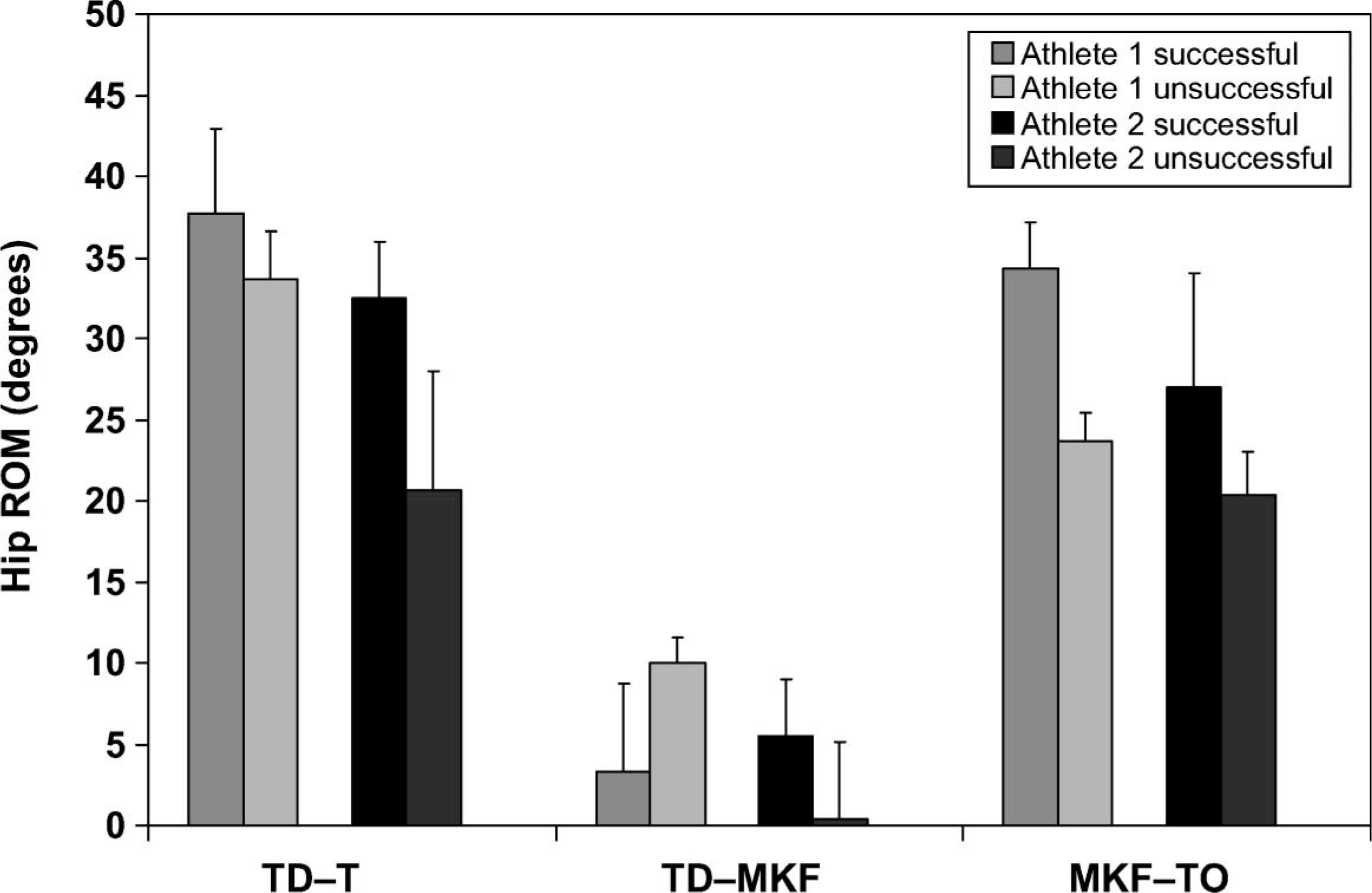
Hip ROM (degrees) from (i) touch-down to take-off (TD-TO), (ii) touch-down to maximum knee flexion (TD-MKF) and (iii) maximum knee flexion to take-off (MKF-TO) for all successful and unsuccessful jumps.
A difference in terms of loss in horizontal and gain in vertical velocity between successful and unsuccessful jumps was seen for one athlete (Athlete 1) but not to the same extent for the other athlete. More horizontal velocity was lost TD-MKF, during successful jumps (82% and 84%) compared to unsuccessful jumps (76% and 80%) for Athletes 1 and 2, respectively (Table II). Consequently less horizontal velocity was lost MKF-TO for the successful jumps. More vertical velocity was gained MKF-TO for successful (35%) compared to unsuccessful jumps (26%) for Athlete 1. Vertical velocity gain was the same for Athlete 2 (34%) regardless of whether the jump was successful or unsuccessful. However, again, Athlete 2 consistently jumped a lower height than Athlete 1.
On looking at the key kinematic parameters from TD to TO of the successful jumps compared to the unsuccessful jumps, only the hip ROM values showed any clear differences for both athletes. For TD-TO and MKF-TO, both athletes had a greater hip ROM during the successful jumps compared to their unsuccessful jumps (Figure 6). While there are many other factors involved in a successful bar clearance – not least, the position of the foot plant from the bar and the body configuration during flight, both of which were not measured in this study – the results qualitatively suggest that hip ROM may be one of the factors in successful high jump technique in TT athletes.
Discussion
Observed differences in reported key kinematic parameters between the two athletes may be due to many factors: Ability, approach speed, personal best, stature, strength, Athlete 1 jumping consistently higher than Athlete 2 etc. However, for many of the key parameters reported, both athletes exhibited similar results to each other regardless of successful jump height; these results also differed to that reported for non-amputee high jumpers. While one cannot generalize these findings to all amputee high jumpers due to having too few athletes, and too few trials in this study, these two athletes were vastly different in approach speed, height jumped and personal best, and thus it is possible that any descriptive similarities between the two could be due more to the fact that they are amputated rather than individual technique. Thus these similarities can be used as a starting point to begin to describe transtibial amputee high jump technique.
While Athlete 1 consistently jumped higher than Athlete 2, he was also taller. On normalizing jump height to the athlete's standing height, it was seen for the successful jumps that Athlete 1 only jumped slightly higher than Athlete 2 (0.1 – 0.5% higher). %HCM, however was higher for Athlete 1 than Athlete 2 both at MKF (%5) and TO (4%) which may indicate that either Athlete 1 was jumping far higher than he needed to clear the bar at that height, or Athlete 2 did not have an optimal technique TD-TO. While it is interesting to look at jump height as a percentage of standing height when two athletes are of different stature, it is not how tall an athlete is per se that determines height jumped. Absolute successful height cleared determines the competition result and thus this parameter is used further in the present study to help provide an explanation of technique for these two transtibial amputee athletes.
Both TT athletes exhibited slower horizontal velocity than previously reported for non-amputee high jumpers (Dapena 1987; Dapena and Chung 1988; Greig and Yeadon 2000). This was expected due to constraints associated with a prosthesis, i.e., lack of ankle musculature that reduces propulsive force and compromises ability to control foot placement location and timing at TD.
Vertical velocity at TD was of similar magnitude to that reported for non-amputee high jumpers (Dapena 1987; Conrad and Ritzdorf 1990). The negative vertical velocity at TD is due to the athlete exerting a large downward force on the ground in order to obtain a large upward vertical reaction force at the end of the take-off phase (Dapena 1987). The positive vertical velocity at TO, however, was slightly lower for the amputee athletes than that reported for non-amputee athletes (Dapena 1987; Dapena and Chung 1988; Conrad and Ritzdorf 1990; Papadopoulos et al. 1995), suggesting that the lack of a relationship between vertical velocity at TO and height jumped by these amputee athletes may stem from problems developing a high vertical impulse during the take-off phase. Vertical take-off velocity is dependent on the horizontal velocity developed in the approach and the effectiveness in which it is converted to vertical velocity during the take-off phase (Dursenev 1991). Non-amputee athletes increase vertical velocity during the first half of the take-off phase (TD-MKF) as a result of the large forces at TD associated with eccentric muscle conditions (Dapena and Chung 1988), but at the expense of a loss in horizontal velocity. Hence, most of the vertical velocity is generated, and consequently, most of the horizontal velocity is lost, in the first half of the take-off phase (TD-MKF). This was also exhibited by the TT athletes. On looking at the individual TT athletes' data to try to determine whether any difference in parameters exist between successful and unsuccessful jumps, the results showed that for the more successful of the two TT athletes (Athlete 1), more horizontal velocity was lost and more vertical velocity was gained TD-MKF during his successful compared to his unsuccessful jumps. The fact that this was not seen in Athlete 2 who did not jump as high may be due to poor technique rather than inability due to the constraints of the prosthetic limb.
Greig and Yeadon (2000) and Dapena (1987) noted a positive relationship between approach velocity and jump height for non-amputee athletes. The lack of a relationship between horizontal or vertical velocity at TD, MKF or TO and successful height jumped for the TT athletes is in contrast with that reported for non-amputee athletes. This may suggest that these two athletes are unable to fully convert their horizontal approach velocity to vertical velocity and thus maximise height jumped, possibly due to a non-optimal touch-down/take-off technique. This has previously been reported for amputee long jumpers where the relationship between approach speed and distance jumped was not as optimal as that reported for non-amputee long jumpers, and was less optimal with increasing level of amputation (Nolan and Lees 2000, 2007; Nolan et al. 2006).
The mechanism in which horizontal velocity is converted to vertical velocity requires a low centre of mass position at TD (Dapena 1987). If the horizontal approach velocity is too fast or the CM position is too low for the amount of eccentric leg strength the athlete has, the leg will ‘buckle’ resulting in an unsuccessful jump (Dapena 1987). Thus there is an optimum relationship between approach velocity and CM height for non-amputee athletes. The two amputee athletes exhibited a similarly low centre of mass position at TD (Dapena 1987), and a similarly high %HCM at TO (Dapena et al. 1990), as is reported for elite non-amputee high jumpers. In addition, no ‘buckling’ of the leg was qualitatively observed during the take-off phase. Thus the reason for not generating as much vertical velocity at TO as non-amputee high jumpers is possibly not due to inadequate eccentric leg strength.
In order to have a low CM at TD, an athlete can either increase knee flexion at TD or increase step length by placing the touch-down leg far in front of the body. In the present study, even though the two TT athletes had a much more flexed knee at TD than that reported for non-amputee athletes (Conrad and Ritzdorf 1990; Papadopoulos et al. 1995; Greig and Yeadon 2000), no relationship between knee angle at TD and height jumped was observed. This is in contrast to such a relationship reported for an elite non-amputee athlete (Greig and Yeadon 2000). However, Greig and Yeadon (2000) reported a case study and thus the knee angle and jump height relationship could have been due to individual technique, strength or ability. In the present study, the qualitative relationship between the touch-down leg angle and height jumped illustrated that for both the TT athletes included in this study, the smaller the leg angle (the less far in front of the body the TD leg was placed), the greater the successful height jumped. This contrasts with that reported for non-amputee high jumpers (Dapena 1987; Greig and Yeadon, 2000), in that the further in front of the body the leg was planted, the higher the jump. If the take-off leg is planted well ahead of the body at TD, a large vertical impulse is provided, maximizing vertical velocity at TO (Dapena 1987), thus such a position is advantageous for a non-amputee high jumper. However, this more upright position at TD for the transtibial amputee high jumpers is similar to that reported for amputee long jumpers (Nolan and Lees 2000, 2007). Hence this might explain why less vertical velocity at TO was generated by the amputee athletes compared to non-amputee high jumpers, and why the conversion from horizontal to vertical velocity, ultimately seen as a relationship between approach speed and height jumped, was not as favourable for amputee compared to non-amputee jumpers.
The amputee athletes touched-down with a flexed hip, i.e., the amputee athletes were slightly upright, not leaning backwards at TD. A backward lean of the trunk at TD has been suggested to be advantageous as it evokes a stretch reflex which may increase the force that the muscles can exert in the second half of the take-off phase (Dapena and Chung 1988). Thus the TT athletes are unable to utilize this advantage. Instead, the amputee athletes, because they land with a less extended touch-down leg compared to non-amputee athletes, may be compensating with a greater range of hip motion during the take-off phase (TD-TO) in order to generate more vertical velocity and height at TO. A similar strategy has previously been seen in elite amputee long jumpers (Nolan and Lees 2000, 2007; Nolan et al. 2006) as a compensatory mechanism for being unable to use sufficient knee ROM due to problems taking off from the prosthetic limb on the previous step. It is interesting to note that Athlete 1 who jumped the highest had a greater hip ROM and a smaller knee ROM than Athlete 2. This could be due to differences in individual technique, but is similar to that reported as a compensatory mechanism by elite lower limb amputee long jumpers.
On looking at joint kinematics for successful versus unsuccessful jumps, both TT athletes clearly demonstrated greater hip ROM from TD-TO and MKF-TO during their successful jumps compared to their unsuccessful jumps. Thus, it may be that in high jump, although further studies are needed, as well as in long jump, amputee athletes compensate for the limitations of the prosthetic limb and loss of lower limb musculature by using their hip musculature much more than non-amputee athletes. This, if true, has implications for strength training and coaching, particularly in that TT should be taught a high jump technique that allows them to utilise their hip more, and not to place their touch-down leg too far in front of their body which may limit their high jump performance.
This study is limited in terms of the number of athletes included, and the number of jumps they performed. Thus, it is not possible to generalize these findings to all TT athletes, even though both exhibited a common technique in terms of several key parameters. However, these data were collected during competition at the highest level in disabled sport, and thus the techniques reflect those used currently by elite performers. As the data were collected during competition, it was not possible to overcome the limitations of number of competitors and number of jumps. Presently, there are few elite TT high jumpers but a better understanding of technique may lead to better coaching and thus more TT athletes participating in the event.
While it is not possible to generalize these findings to a single specific technique used by TT high jumpers, this study has provided some insight to the individual techniques displayed by a population not previously studied. The technique of any TT jumper, as in non-amputee jumpers, is individual due to differing levels of amputation, strength, ability and prostheses used. However, the technique used by the two athletes included here exhibited similar kinematic characteristics in terms of touch-down/take-off parameters, but differed from what is known about non-amputee high jump. These observations not only provide a first insight to understanding the mechanisms underlying TT high jump technique, but also have implications for training and coaching, in an area that currently little is known about.
Footnotes
Acknowledgements
This study was funded by CIF (Centre for Sport Research, Stockholm, Sweden) and The Swedish School of Sport and Health Sciences, GIH, Stockholm, and approved and supported by the International Paralympic Committee. The authors would like to thank Kathy Simpson and Morgan Nolan for help with data collection.