
Abstract
The use of external orthoses following surgical cranial vault remodelling in infants with craniosynostosis was first described in the 1980s. While a few preliminary reports have been published on its use, there are no reports outlining specific orthotic considerations. The purpose of this paper is to present the orthotic community with an introduction to the various craniosynostoses, the resultant cranial morphologies, and specific orthotic considerations associated with these morphologies, including trigocephaly, frontal plagiocephly, brachycephaly, scapholocephaly, and occipital plagiocephaly. For each presentation, guidelines are presented as to where the cranial remoulding orthosis should maintain contact, thereby discouraging cranial growth, and where the voids should be established and maintained to allow for corrective cranial growth. Principles are supported by photographs of representative cases.
Introduction
Craniosynostoses are a collection of defined craniofacial deformities resulting from premature closure of one or more cranial sutures. In the 1890s, Lannelongue performed the first attempt at surgical correction of a sagittal synostosis (1890). Since that time, “a myriad of surgical procedures have been developed and used for the treatment of this condition” (Jimenez et al. 2002). As recently as 2000, the technique of choice in many craniofacial centres was identified as calvarial vault remodelling (CVR) (Jimenez and Barone 2000).
In addition to the corrective surgical procedures, a few reports were published in the 1980s describing the post-operative use of “skull moulding caps” (SMC) as an adjunctive treatment modality (Persing et al. 1986; Ham and Meyer 1987; Ham 1989). These devices were fabricated out of low temperature plastics 3 – 10 days following the cranial surgery and worn by the infant, throughout the day for 3 – 6 months post-operatively (Persing et al. 1986; Ham and Meyer 1987). In addition to the provision of post-operative protection of the remodelled skull, SMCs were indicated to encourage further corrective growth in cases where operative procedures failed to provide complete cranial symmetry, to prevent relapse of the skull into its pre-surgical morphology and to prevent the formation of new aberrant head shapes (Persing et al. 1986). This was done through the application of gentle pressure in targeted regions to inhibit bone growth and the inclusion of targeted voids in other areas to promote growth (Ham 1989).
During the same time period, Clarren first described the phenomenon of “positional plagiocephaly” and its successful treatment with remoulding “helmets” (Clarren et al. 1979; Clarren 1981). These helmets rely on the same treatment principles utilized with SMCs. Concurrent with the dramatic increase in the incidence of positional plagiocephaly associated with the SIDS related “back to sleep” campaign, there has been a renewed interest in cranial remoulding orthoses as part of the non-operative treatment of the more benign “positional” or “non-synostotic” plagiocephaly (Kane et al. 1996; Ripley et al. 1994).
Similarly, the use of orthotic moulding techniques as an adjunctive treatment to traditional CVR procedures appears to be gaining in popularity. A survey published in 2004 indicated that at least 12 craniofacial centres in the United States were using post-operative cranial orthoses after surgical cranial vault remodelling (Barringer 2004). Despite this popularity, recent descriptions of post-CVR orthotic intervention are confined to two articles. The first reporting on the effectiveness of post-operative “moulding helmets” as an adjunct to surgery in the treatment of sagittal synostosis (Seymour-Dempsey et al. 2002), and the second reporting on the preliminary use of such helmets as an adjunctive treatment following surgical correction of less commonly encountered fusions, including those of the metopic and coronal sutures (Higuera et al. 2005).
The purpose of this paper is to outline, in the form of a case series, the experiences of a single craniofacial team currently utilizing the adjunctive orthotic remoulding techniques following CVR. The paper will present the various forms of single-suture synstosis, their pre- and post-operative morphologies, the implications of these factors on their orthotic management and post-orthosis outcomes. In the absence of any universally accepted techniques to adequately document craniofacial asymmetries and proportions, this cases series is primarily based on representative photographs of the various craniosynostoses, (a) prior to surgery, (b) after surgery but prior to orthotic intervention, and (c) following the use of remoulding orthoses.
Patient summary and methods
Between 2003 and 2006, 22 patients were treated at Texas Children's Hospital for non-syndromic craniosynostosis with total cranial vault remodelling followed by orthotic moulding. Patients had the following distribution: 5 left coronal, 5 right coronal, 4 bicoronal, 3 metopic, 3 lambdoid, and 2 sagittal. The patients' ages at time of operation ranged from 4.25 – 15.5 months, with an average age of approximately 7.5 months. Cast impressions preparatory to the fabrication of remoulding orthoses were obtained by the same orthotist approximately 10 – 14 days after surgery. The cranial orthoses were fitted an additional 10 – 14 days after the casting. For most patients, these consisted of 5 mm (3/16 inch) co-polymer thermoplastic with an interface of 13 mm (½ inch) polyethylene foam. The trim-lines for each orthosis were patient-specific. However, all had some form of superior opening with a side closure. For patients with sagittal synostosis, orthoses were fabricated of 6 mm (¼ inch) surlyn. These had no superior opening and were bivalved with an anterior and posterior component. Each orthosis was created from a modified plaster template, under the direction of the treating orthotist. Patients were instructed to wear the helmet 23 hours each day.
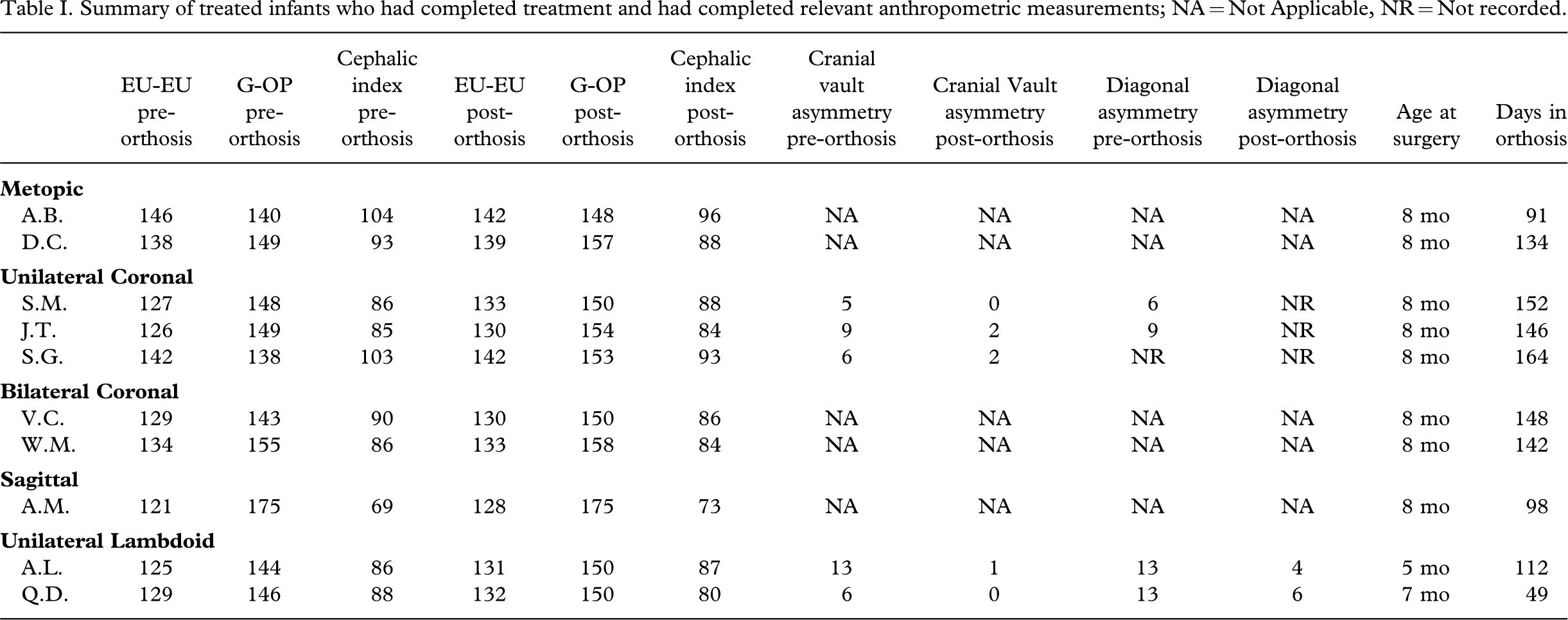
Cranial measurements of each patient were obtained by the orthotist at the time of casting and at follow-up appointments. When possible, similar measurements were also obtained prior to the corrective surgeries. The measurements taken evolved as protocols were established, but generally included the following: Head circumference, measured at the equator at the level of the brow and parallel to the floor; cranial width, from eurion to eurion; cranial depth, from glabella to opisthocranion, and when indicated, cranial vault, from the exocanthion to the contralateral eurion, and the more informative oblique diagonals, taken from the apex of the occipital bossing to the apex of the contralateral frontal bossing, and from the centre of the occipital flatness to the centre of the contralateral frontal flatness. For each set of measurements of cranial width and length, a cephalic index was calculated as the percentage of cranial width to length. Where appropriate, the difference between the cranial vaults was recorded as the cranial vault asymmetry, and the difference between the oblique diagonal measurements was recorded as the oblique diagonal asymmetry. These measurements and successive photographs were used to document improvement in cranial proportion and symmetry prior to surgery, after surgery but before the use of a remoulding orthosis, and at the conclusion of orthotic remoulding. A summary of those patients for whom complete measurements were available before and after the use of the remoulding orthosis is provided in Table I. Of the 15 patients who had completed helmet use and were not lost to follow-up, helmets were worn an average of 134 days before discontinuation.
Summary of treated infants who had completed treatment and had completed relevant anthropometric measurements; NA = Not Applicable, NR = Not recorded.
Suture fusion and compensatory growth
Deleshaw et al. (1989) outlined what they described as a “working hypothesis for calvarial growth”. Based on their analyses of the various simple synostoses, the authors found that each of the resultant deformities could be predicted based on four rules. These rules were later condensed and somewhat simplified by Jane et al. (2000) and are summarized below:
With respect to the fused suture, compensatory growth is greatest at adjacent sutures. If the adjacent suture is more or less parallel to the fused suture, the compensatory growth will be symmetrical. If the adjacent suture is more or less perpendicular to the fused sure, the majority of the compensatory growth occurs from the bone distal to the fused suture.
By applying these rules, clinicians can predict and understand the various cranial morphologies that result from the compensatory growth following the fusion of a given suture.
Metopic
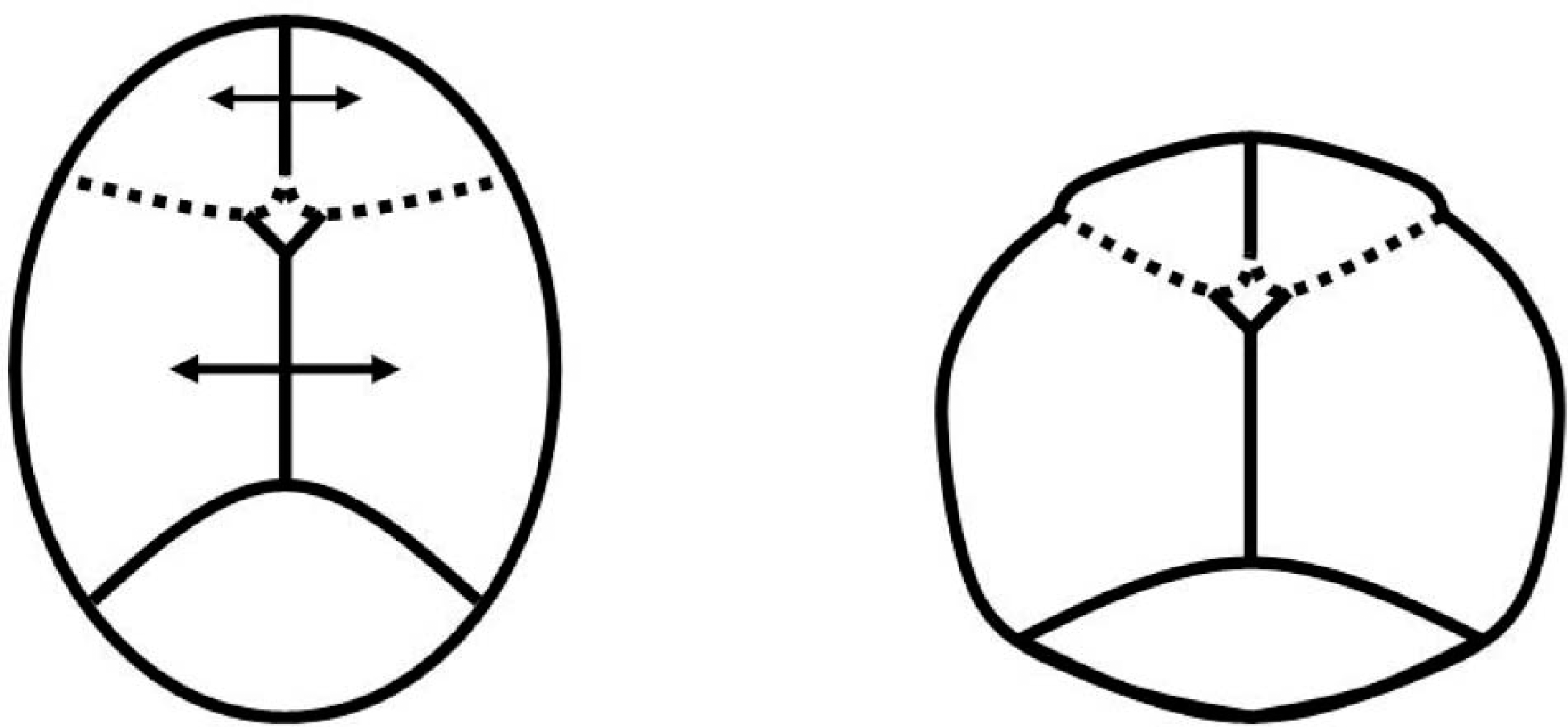
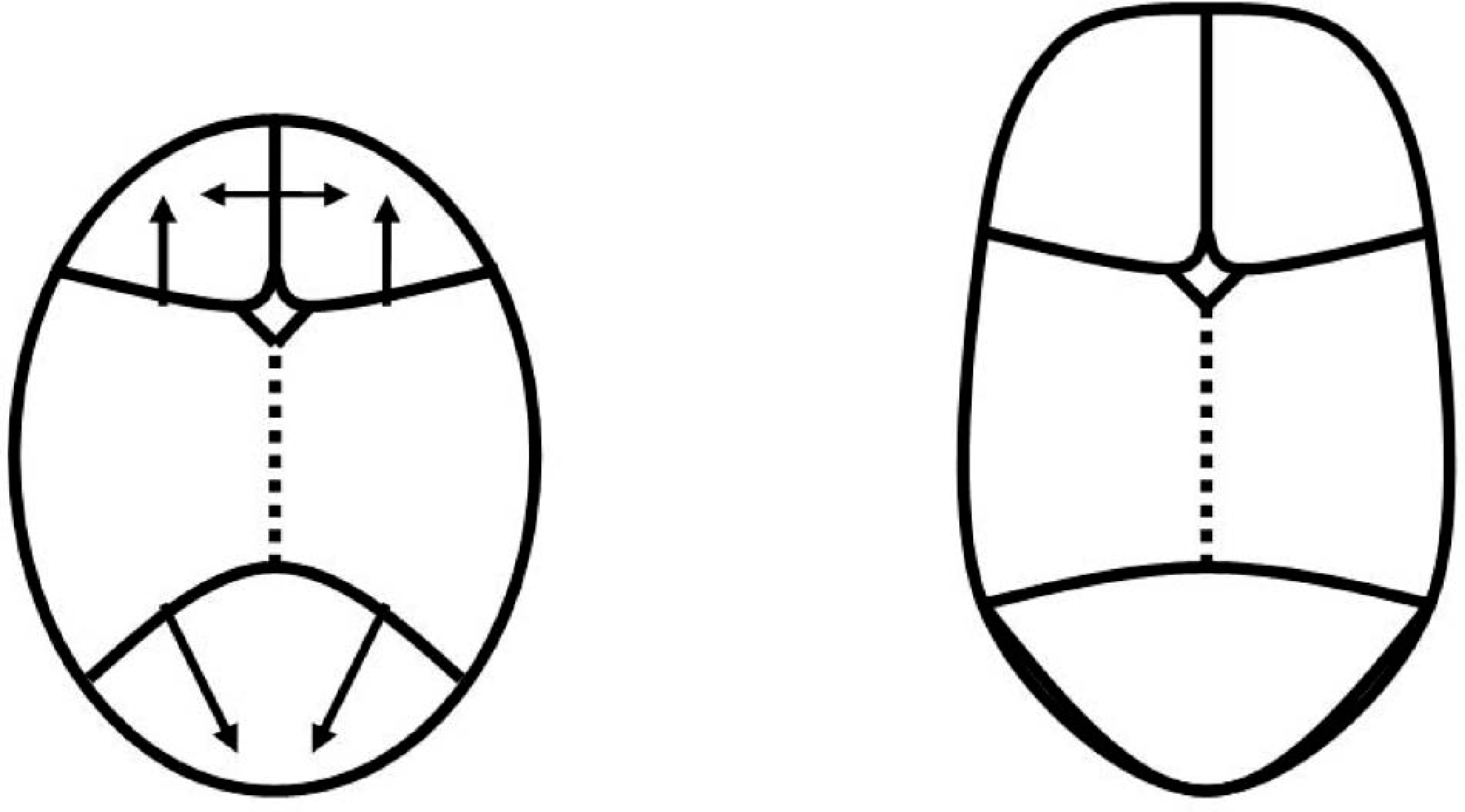
Applying the rules of compensation to a skull with a premature fusion at the metopic suture, compensatory growth is anticipated at the coronal and sagittal sutures more so than the lambdoid sutures. The fusion of the metopic suture prevents any growth of the frontal plates. Growth at the perpendicular coronal sutures will occur distal to the fused metopic suture, into the parietal plates. At the sagittal suture, growth will occur symmetrically into the parietal plates (Persing et al. 1989) (Figure 1).
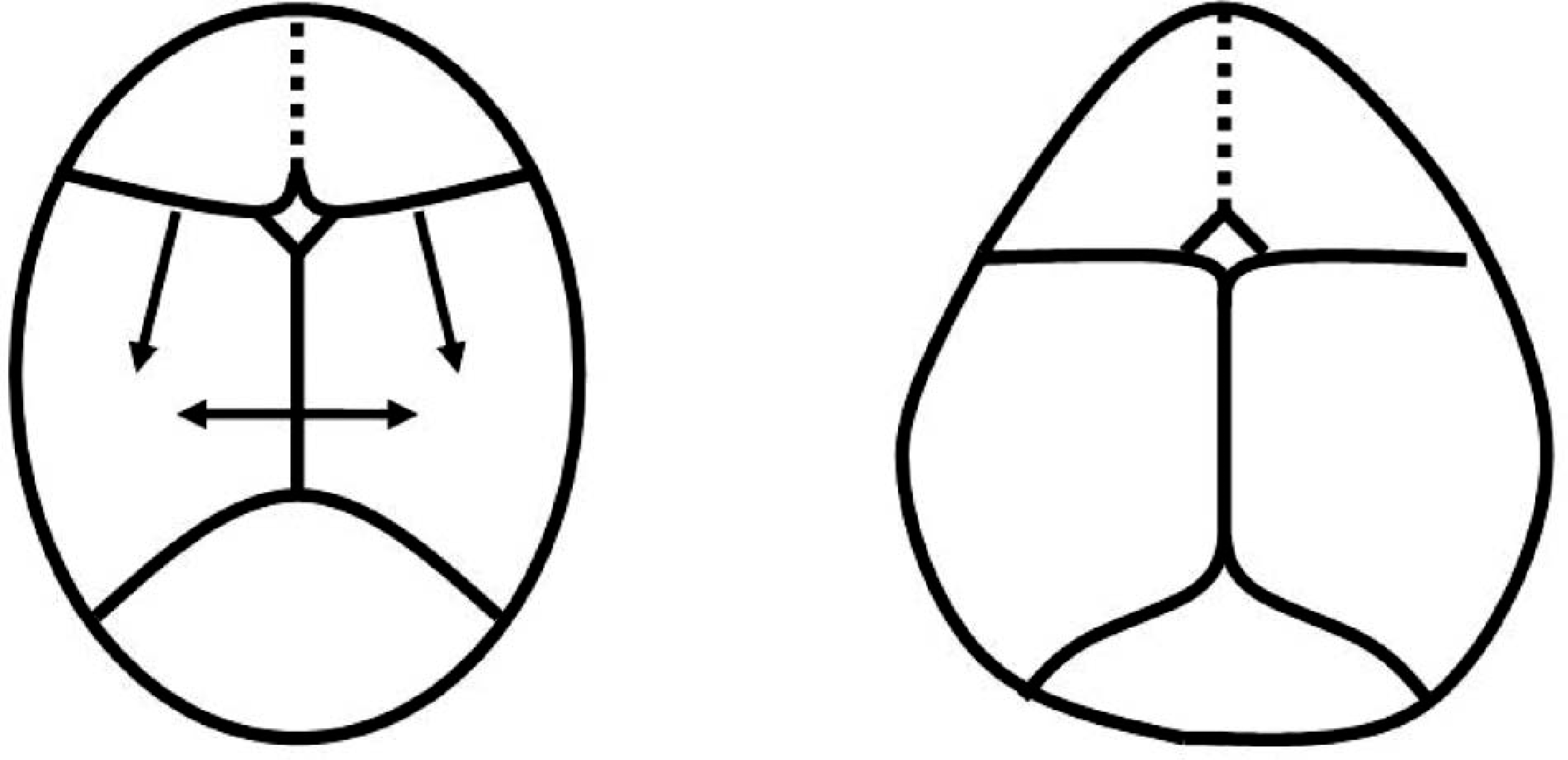
Metopic synostosis and resultant trigocephaly.
The resultant trigocephaly is characterized by extreme frontal narrowing with biparietal flaring, resulting in a “tear drop” appearance (Figure 2).

Patients with metopic synostosis and resultant trigocephaly, pre-operative.
Following surgery, areas of concern are any residual frontal narrowing, general contour of the frontal plates and any residual biparietal flaring. Efforts should be made to maintain intimate contact of the remoulding orthosis against the frontal apex, if present. If necessary, voids can be placed bilaterally off of the apex to allow for corrective growth and an improved frontal contour. The coronal width of the cranium should be contained, to constrain growth in this dimension, while allowing growth in the occipital region to increase the cranial depth. Improvements can be appreciated subjectively and through improvements in the infant's cephalic index as cranial depth improves in proportion to cranial width (Figure 3).

(a) Post-operative presentation of a patient with metopic synostosis. (b) Post-orthosis presentation of the same patient. Note the improved frontal contour and more proportionate cranial depth. Cranial vault reduced from 104 to 92 during 4 months of helmet use.
Unilateral coronal
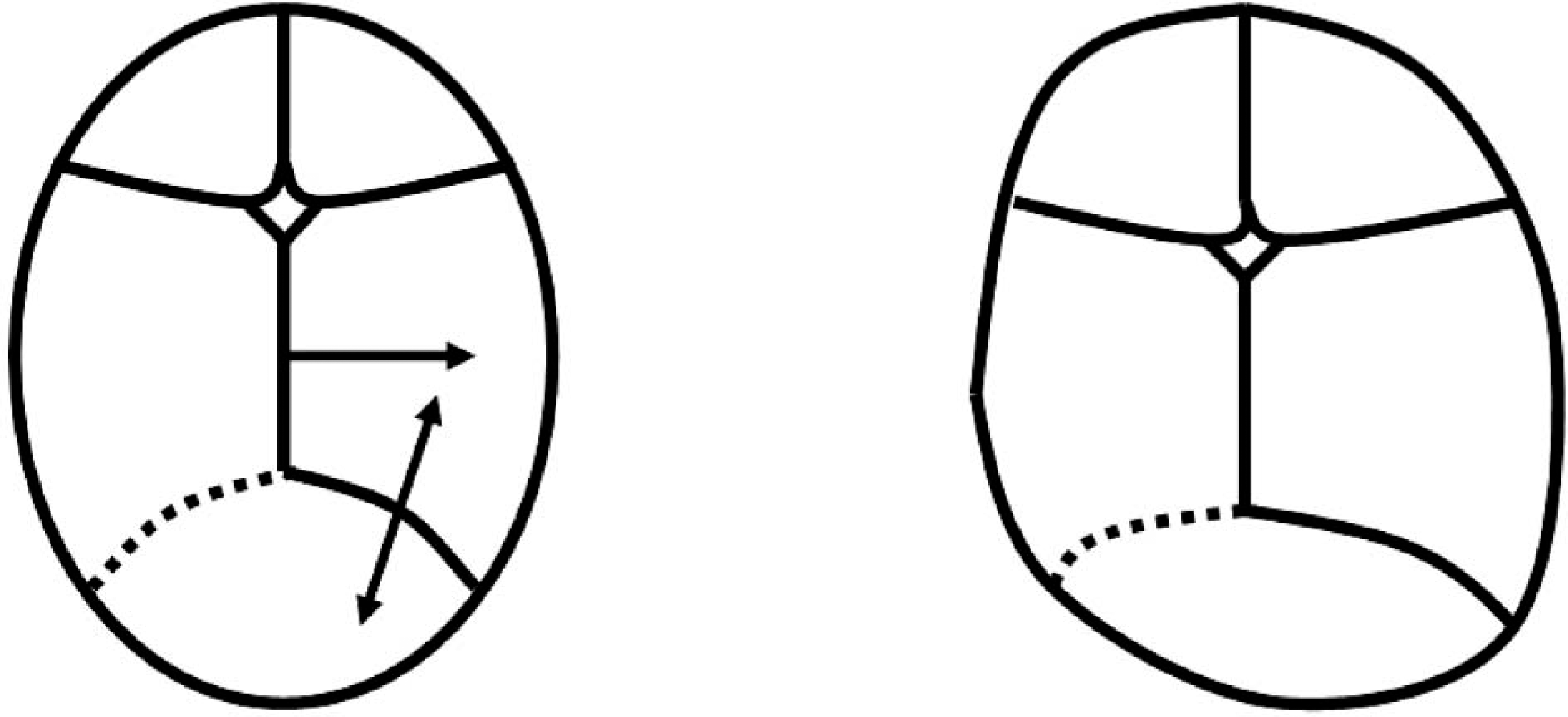
Applying the rules of compensation to a skull with a premature fusion at a single coronal suture, compensatory growth is anticipated at the contralateral coronal suture as well as the metopic and sagittal sutures more so than the lambdoid sutures. The fusion of the coronal suture discourages growth at the ipsalateral frontal and parietal plates. Growth at the perpendicular metopic and sagittal sutures will occur distal to the fused coronal suture, into the contralateral frontal and parietal plates. At the contralateral coronal suture, symmetrical growth will occur into the contralateral frontal and parietal plates (Deleshaw et al. 1989; Persing et al. 1989 (Figure 4).
Unilateral coronal synostosis and resultant synostotic frontal plagiocephaly.
The resultant synostotic frontal plagiocephaly is characterized by a flattened forehead ipsilateral to the fused coronal suture, with bossing of the contralateral forehead and parietal region. Also observed is a relatively anterior projection of the malar eminence ipsilateral to the fused coronal suture and an ipsilateral ear that is positioned relatively anterior and superior to the contralateral ear (Deleshaw et al. 1989; Bruneteau and Mulliken 1992) (Figure 5).
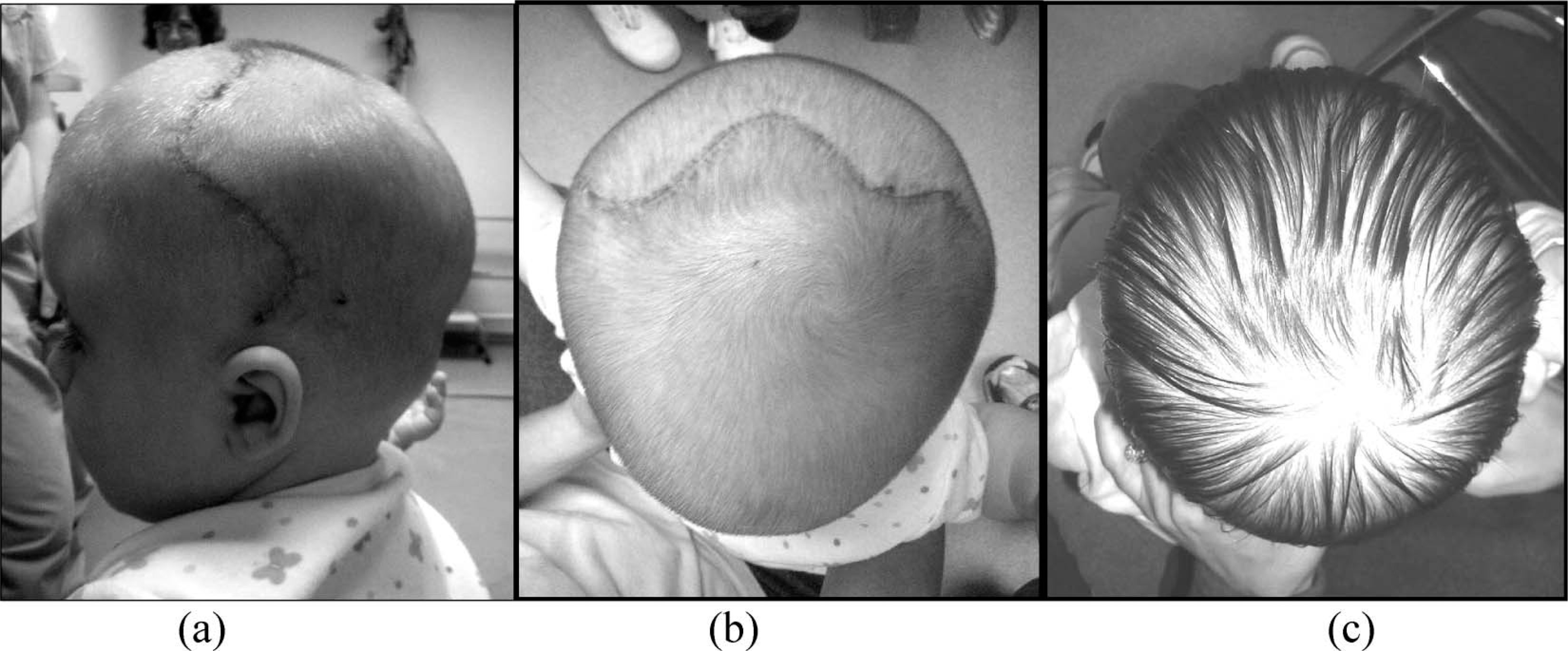
Patient with right coronal synostosis and resultant synostotic frontal plagiocephaly (a) pre-surgery, (b) immediately post-surgery, pre-orthosis.
Following surgery, there are several areas of concern that should be evaluated on a patient specific basis. Most intuitively, the contour of the frontal plates should be assessed. Intimate contact should be maintained over the forehead, contralateral to the involved suture, to contain this bossed area. A void should be ensured over the forehead ipsilateral to the involved suture to encourage corrective growth. These efforts act to encourage symmetry and to prevent recurrence of the pre-surgical morphology. Improvements can be subjectively appreciated and monitored through measurements of the infant's cranial vault asymmetry and oblique diagonal asymmetry (Figure 6). However, these indices should be interpreted cautiously as, to the extent present flatness of the contralateral occiput will offset some of the frontal bossing, resulting in measurements that fail to adequately represent the asymmetries of the forehead.
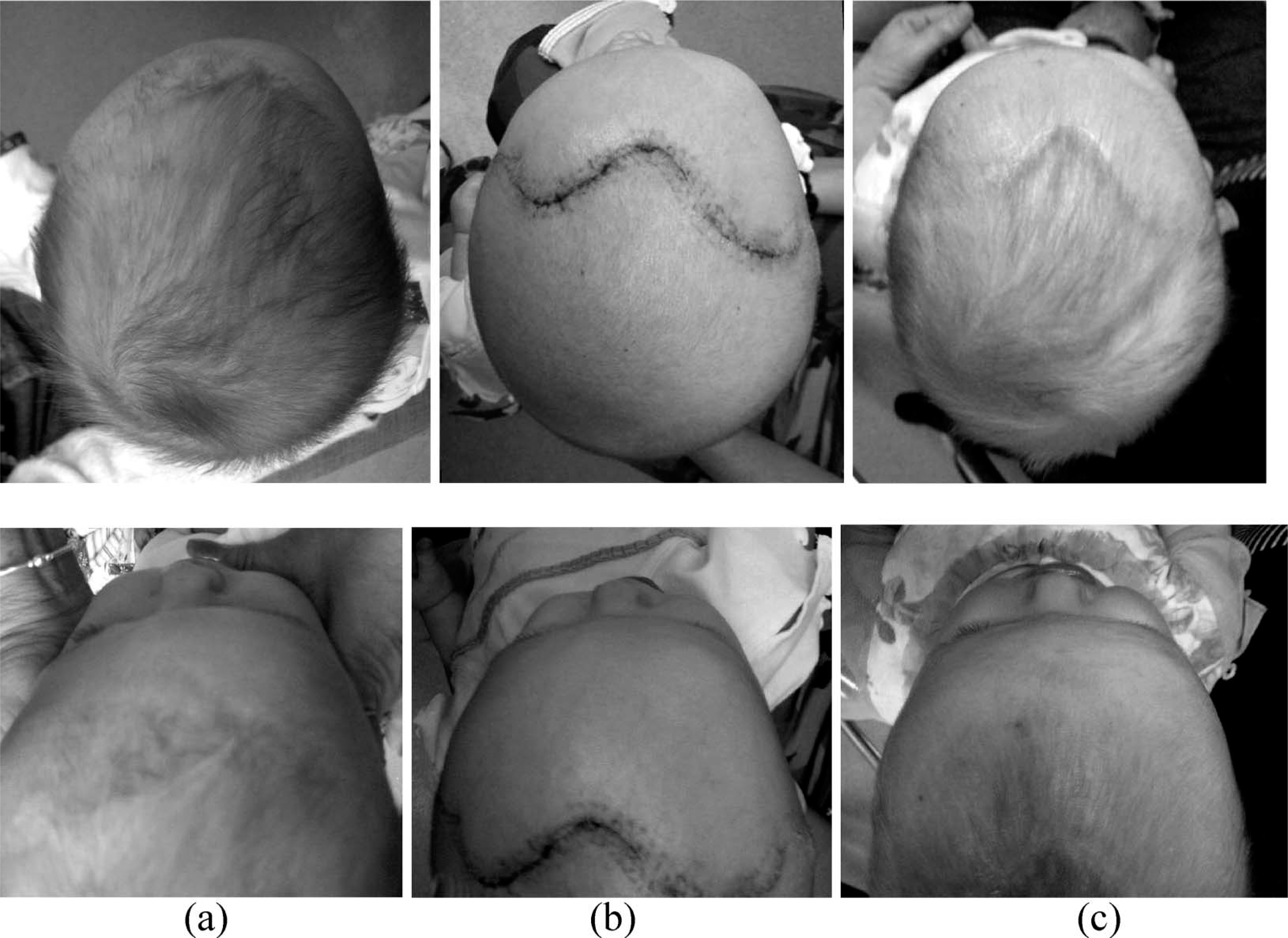
Patient with left coronal synostosis shown from two views (a) pre-surgically, (b) post-surgically, pre-orthosis, (c) post-orthosis. Note the improved frontal contours at each stage. The patient's oblique diagonal asymmetry reduced from 11 – 2 mm following 8 weeks in a cranial remoulding orthosis.
Additionally, the parietal region contralateral to the affected suture should be examined. A degree of bossing is often evident post-surgically, and may be observed from above, or behind the child. Efforts should be made to maintain contact over this region to prevent further bossing. Likewise, a void should be ensured over the contralateral parietal region to encourage corrective growth. Improvements can be subjectively appreciated from posterior view of the infant's skull (Figure 7).
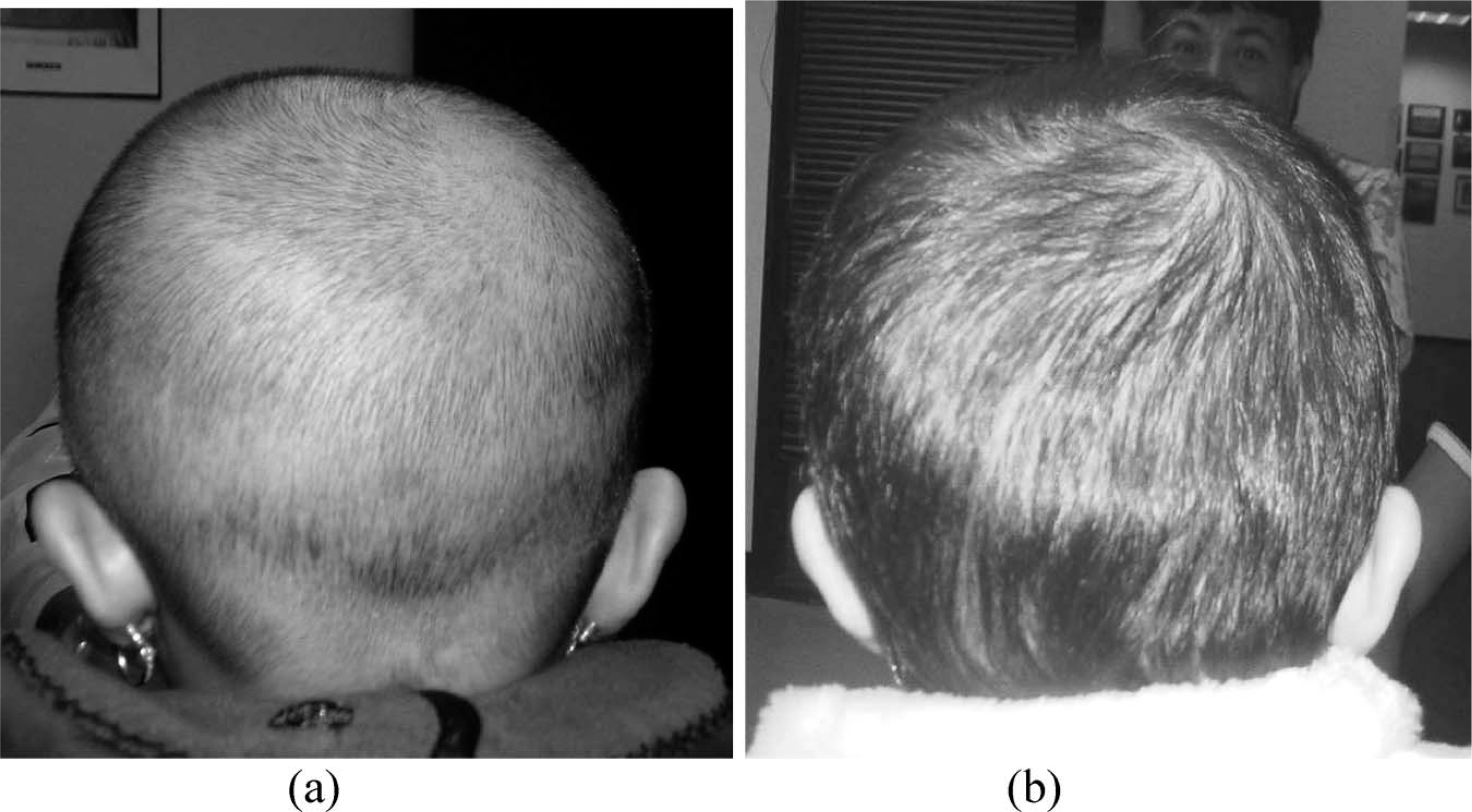
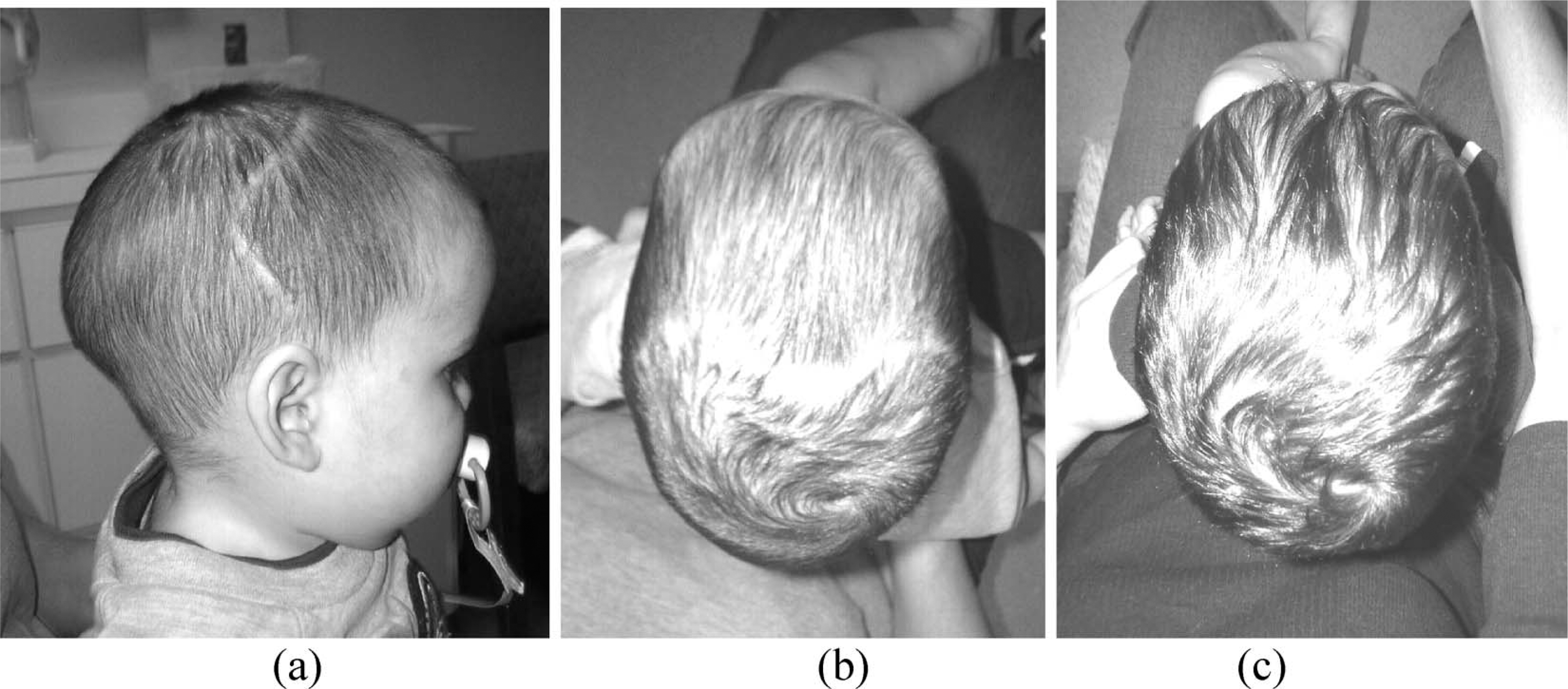
Infant with right coronal synostosis, (a) post-operative, pre-orthosis, (b) post-operative, post-orthosis. Note the corrective growth in the right posterior-parietal region and improved parietal height symmetry.
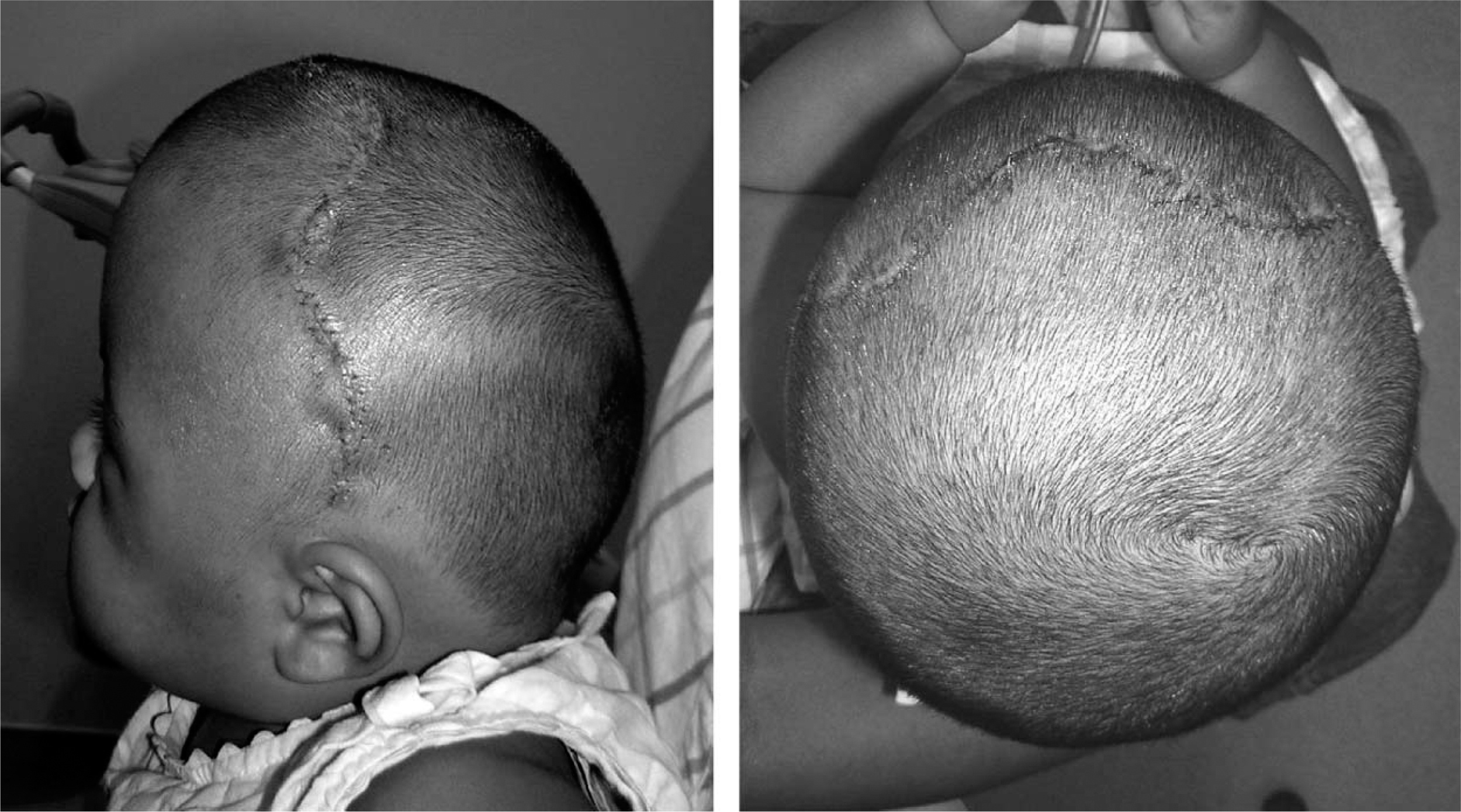
Finally, the infant's occipital contour should be examined. For many infants, any asymmetries may be subtle. For other infants, a degree of flatness may be seen ipsilateral to the involved coronal suture. In such cases, the contralateral bossed area should be well contained by the orthosis, while ensuring a void over the ipsilateral flatness. Improvements may be subjectively appreciated, or monitored through measurements of the infant's cranial vault asymmetry (Figure 8).

Infant with right coronal synostosis, and ipsalateral occipital flatness, (a) post-operative, pre-orthosis, (b) post-operative, post-orthosis. Note the improved occipital contour gained through corrective growth in the right occipital area. The patient's oblique diagonal asymmetry improved from 16 – 4 mm following 10 weeks in a cranial remoulding orthosis.
Bilateral coronal synostosis
Applying the rules of compensation to a skull with a premature fusion at both coronal sutures, compensatory growth is anticipated at the metopic and sagittal sutures more so than the lambdoid sutures. The fusion of the coronal sutures discourages growth at the frontoparietal plates. Symmetrical growth occurs at the perpendicular metopic and sagittal sutures (Deleshaw et al. 1989; Persing et al. 1989) (Figure 9).
Bilateral cronal synostosis and resultant synostotic brachycephaly.
The resultant synostotic brachycephaly is characterized by a symmetrical, but abnormally tall, shallow head shape (Figure 10).
Patient with bilateral coronal synostosis and resultant synostotic brachycephaly. Note the flattened, wide, forehead contours.
As with unilateral coronal synostosis, variation exists between individual cases. For some patients, in addition to the exaggerated skull height, there may be a degree of occipital narrowing when viewed from above. In contrast, the contour of the forehead is quite full. Thus, efforts should be made to contain the frontal bones with the orthosis, to prevent further bossing. This containment should extend into the parietal region bilaterally to contain the cranial growth in the coronal plane. In cases where the head is simply shallow, and no occipital narrowing is evident, an adequate void should be ensured in the occipital region to allow for corrective growth in cranial depth. In these cases, improvements can be appreciated in a reduction in the infant's cephalic index, as cranial depth improves in proportion to cranial width. In cases where occipital narrowing is observed, the apex should be contained within the orthosis, with voids ensured bilaterally to allow corrective growth and improve the contour of the occipital region (Figure 11).
Infant with bilateral coronal synostosis with evident occipital narrowing, (a) and (b) post-surgical, pre-orthosis, (c) post-orthosis. Note the improved occipital and frontal contours.
Sagittal
Applying the rules of compensation to a skull with a premature fusion at the sagittal suture, compensatory growth is anticipated at the metopic, coronal and lamboid sutures. Fusion of the sagittal suture discourages growth in both parietal plates. Growth at the perpendicular coronal and lambdoid sutures will occur distal to the fused sagittal suture, into the frontal and occipital plates respectively. At the metopic suture, there will be symmetrical, compensatory growth into the frontal planes (Deleshaw et al. 1989; Persing et al. 1989) (Figure 12).
Sagittal synostosis and resultant scaphocephaly.
The resultant scaphocephalic deformity is characterized by a narrow head shape, with exaggerated length (Figure 13). Prominences of the frontal bones or occiput may be present, depending on the location and extent of the fusion along the sagittal suture (Jane et al. 2000).

Patient with sagittal synostosis and resultant scaphalocephaly.
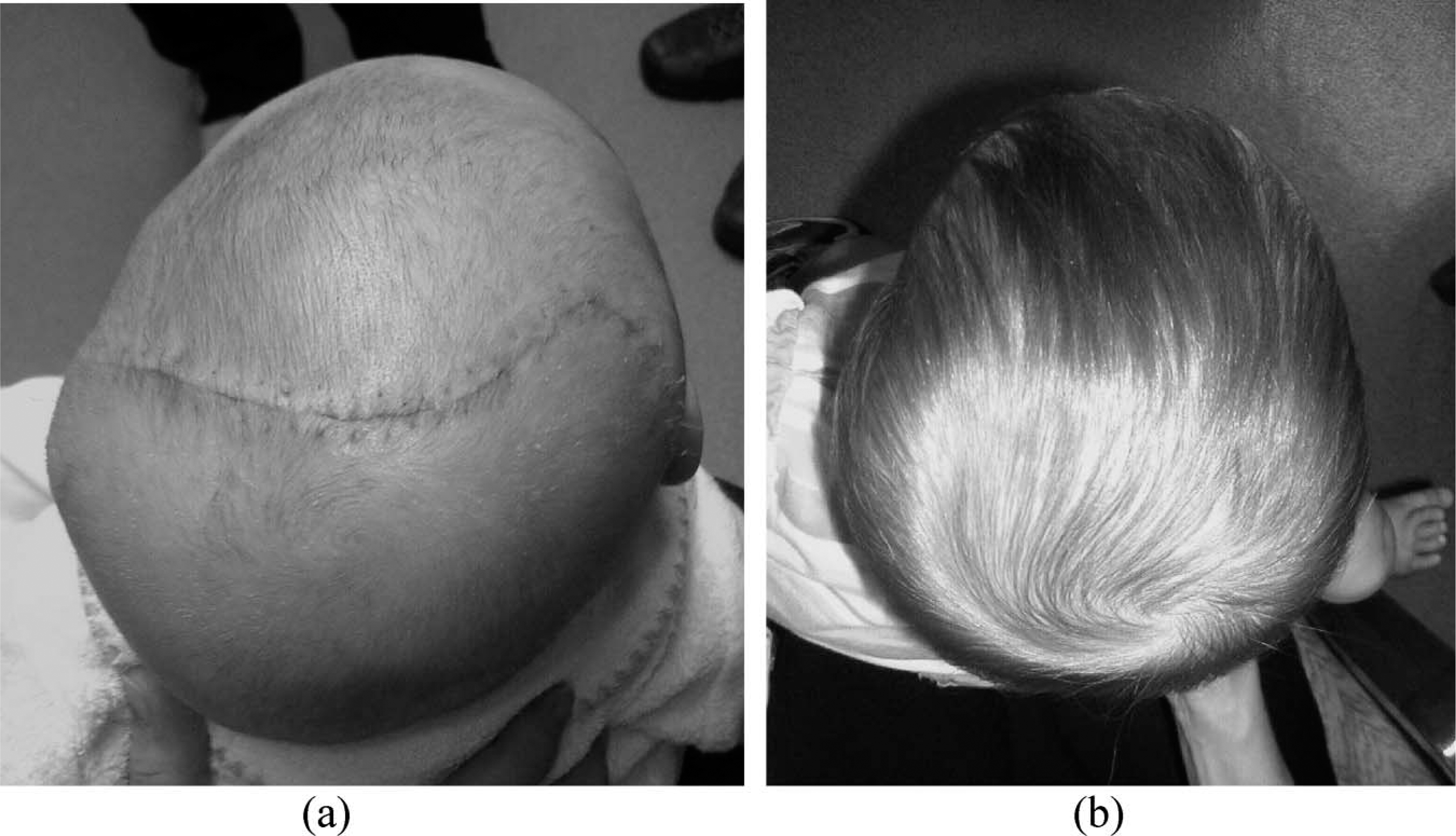
Following surgery, the orthosis should attempt to constrain any growth in the sagittal plane, preventing any recurrence of the pre-operative cranial morphology. Additionally, voids should be ensured over both parietal plates to allow for corrective growth in the coronal plane. Improvements can be appreciated through an increase in the infant's cephalic index as the cranial width increases in proportion to the cranial depth (Figure 14).
Infant with sagittal synostosis, (a) post-operative, (b) pre-helmet, and (c) post-helmet. Note the augmented cranial width in proportion to the sustained cranial depth and improved occipital contour. The patient's cephalic index improved from 69 to 73 following 14 weeks in a remoulding orthosis.
Unilateral lambdoid
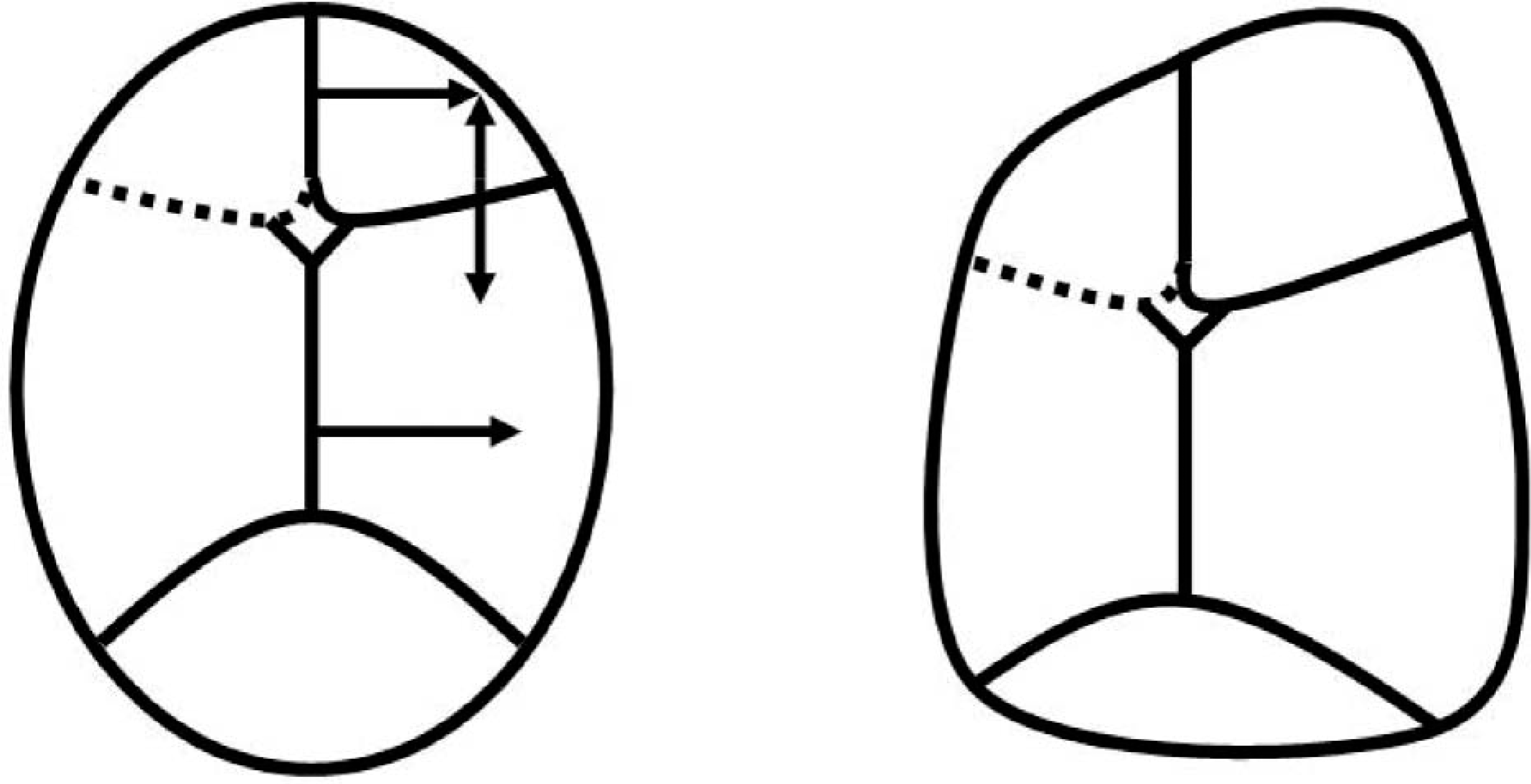
Applying the rules of compensation to a skull with a premature fusion at a single lambdoid suture, compensatory growth is anticipated at the sagittal and contralateral lambdoid sutures more so than the coronal or metopic sutures. Growth at the contralateral lambdoid suture occurs along the parietal border into the contralateral parietal plate, while growth at the sagittal suture is directed distal to the involved suture, also into the contralateral parietal plate (Deleshaw et al. 1989; Persing et al. 1989) (Figure 15).
Lambdoid synostosis and resultant synostotic occipital plagiocephaly.
The resultant synostotic occipital plagiocephaly is characterized by flatness of the occiput ipsilateral to the prematurely fused suture, and an ipsilateral ear that is relatively posterior and inferior. A characteristic mastoid bulge is evident ipsilateral to the involved suture, with a posterior parietal-bossing occurring contralateral to the involved suture. The two later events give the head a parallelogram shape when viewed posteriorly (Huang et al. 1996) (Figure 16).

Patient with right lamboid synostosis and resultant synostotic occipital plagiocephaly.
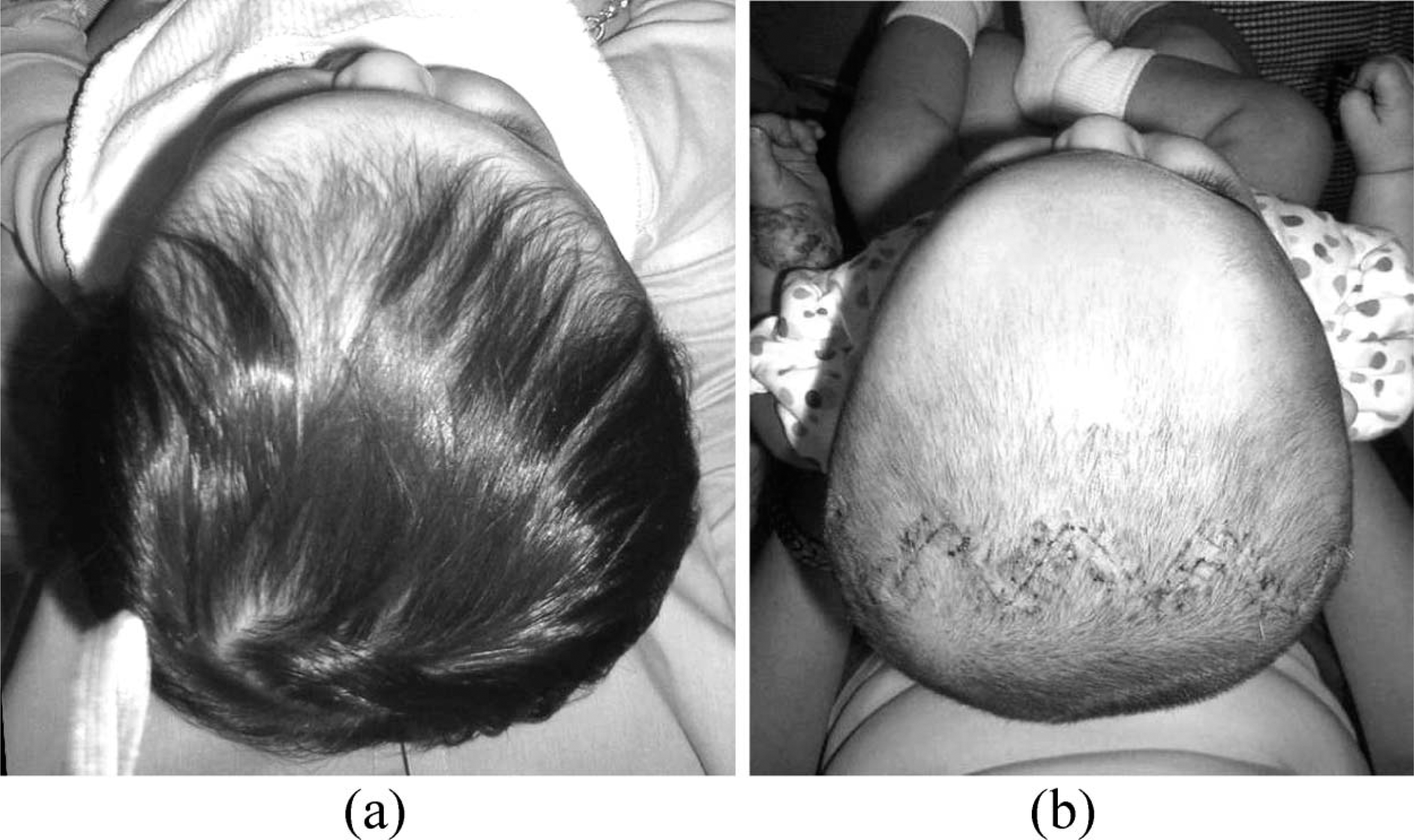
Following surgery, there are several areas of concern that should be evaluated on a patient-specific basis. The most intuitive is the residual contour of the infant's occiput. An intimate fit should be obtained over the mastoid bossing, ipsilateral to the involved suture, and over the contralateral occipital bossing. A void should be verified over the occipital flatness located ipsilateral to the involved lambdoid suture. Improvements can be appreciated subjectively, and verified with measurements in the infant's cranial vault asymmetry and oblique diagonal assymetry (Figure 17).
Infant with right lambdoid synostosis, (a) post-operative, pre-orthosis, (b) post-orthosis. Note the improved contours, both of the occipital region and biparietally. The patient's cranial vault asymmetry decreased from 15 – 1 mm, and their oblique diagonal asymmetry reduced from 17 – 4 mm following 16 weeks in a remoulding orthosis.
Additionally, the extent of the parietal bossing, contralateral to the involved suture should be considered. Care should be taken to contain this area, while ensuring a void in the contralateral posterior-parietal region. Such efforts discourage the return of the pre-surgical head shape, and encourage corrective growth contralateral to the involved suture to offset the residual posterior parietal bossing (Figure 18).
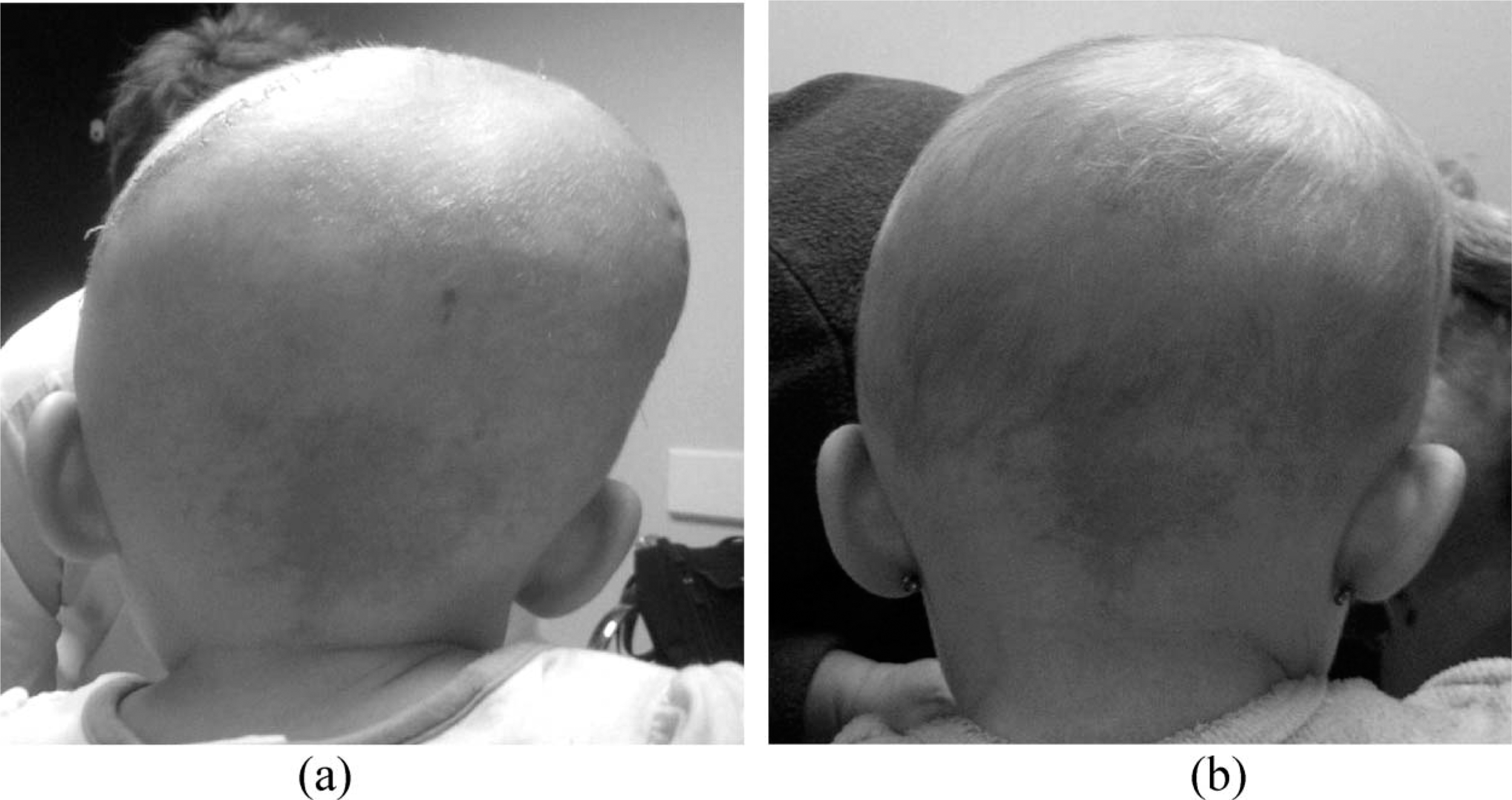
Infant with left lambdoid synostosis, (a) post-operative, pre-orthosis, b) post-operative, post-orthosis. Note the improved parietal contours.
Discussion
There are multiple limitations to the current cases series. It represents an attempt to elucidate the recent experiences of a single craniofacial team which has adopted the use of post-operative remoulding orthoses as the standard practice following CVR. Significant variation exists from patient to patient, based not only on the location of the fused suture, but also on the extent and duration of the fusion and the surgical methods used during CVR. Therefore the presented guidelines should serve only as an introduction to the principles of orthotic remoulding following CVR. The actual post-operative morphology must be evaluated for each infant encountered, and an individual treatment plan formulated. Anticipated orthotic outcomes will vary according to the presentation of the individual infant, the surgical approaches utilized and the infant's age at the time of surgery and subsequent remoulding.
Further difficulty is encountered in the current lack of established methods of documenting changes in cranial symmetry, shape and proportion. As presented in the case series, outcomes are currently assessed subjectively and through inadequate two-dimensional anthropometric measurements. Before critical assessment of post-operative remoulding techniques can be undertaken, more accurate and reproducible means of documenting and quantifying changes are required.
Additionally, with the lack of any controls, the relevance of the post-operative orthotic moulding to final outcomes can not be determined. Without comparison studies between centres with differing philosophies, it is not possible to ascertain the degree to which the orthotic intervention augments any changes that might occur following surgery in the absence of such intervention. Thus, better methods of quantifying changes in cranial morphology and comparison studies using those methods will be necessary before more definitive conclusions can be drawn about the validity of post-operative moulding following CVR.
However, as the subjective improvements observed with post-surgical orthotic remoulding have encouraged its increasing use among craniofacial centres, there is value in reviewing those principles used in the management of this unique patient population.
Conclusion
Orthotic moulding of the infant skull following CVR has been utilized, in various forms, for several decades. Children affected with single-suture synostosis present with characteristic head shapes according to the identity of the fused suture. While considerable individual variation exists between infants, the similarities are such that basic treatment principles exist for each type of simple craniosynostosis. An awareness of the various cranial morphologies that can result from a premature fusion allows the clinician to better plan a patient-specific treatment plan in which cranial growth is optimized for enhanced cranial symmetry and proportion.