
Abstract
Treatment of scoliosis has been under discussion in relation to surgical intervention since the Boston brace was presented by Hall in 1976 (Hall et al. 1976; Watts et al. 1977). The effects of rigid bracing on thoracic skeletal integrity and the possible deformation of ribs due to the high localized pressure due to prolonged wear (Biorthex 1999; Coillard et al. 1999) have been highlighted. The lack of compliance (Houghton et al. 1987) has encouraged clinicians to investigate other options for non-surgical treatment. The Spinecor and Triac bracing systems have been developed as a result of this research; however, both of these orthoses had been designed with idiopathic scoliosis in mind. Little research has been done into the effects of bracing on the neuropathic curve. The use of dynamic Lycra® garments in the treatment of neurological scoliosis offers the advantage of deformity correction without the bulk and discomfort of rigid braces. Recent clinical experience has shown that the Lycra® suits have a positive effect in the treatment of scoliosis. This study discusses the treatment of a child presenting with a spinal tumour and although not truly of neurological presentation indicates that the garment can be used for the different scoliotic presentations.
Introduction
The word “scoliosis” is derived from the ancient Greek word, Skoli-osis, meaning a curve. In the field of medicine it means lateral curvature of the spine (Webster 1983) combined with a rotational aspect. The spinal column, when examined in the sagittal plane, has normal lordosis and kyphosis. In the anteroposterior plane, a lateral curvature of over 10° is considered abnormal (Cassella and Hall 1991) and is defined by the American Scoliosis Research Society as a scoliosis. Following the work of Hall et al. (1976) the Boston brace has become regarded as the “gold Standard” in the treatment of scoliosis. The Boston brace is a modular system made to standard measurements to a prescriptive manufacturing specification. The use of training courses enabled a large number of clinicians from around the world, to be able to produce repeatable and good fitting spinal corrective braces. The results of numerous studies (Emans et al. 1985; Emans 2000; Nachemson 1995) indicated a good result in that the original curve at presentation for bracing had been held in the majority of cases. An outcome was considered to be successful if the curve Cobb angle at the end of brace treatment remained the same as at the start.
The Boston brace protocol involved wearing the brace for up to 23 h a day with an hour out of brace for activity and exercise. Emans (2000) indicates that the use of rigid bracing, when worn for the prescribed time has a positive effect on the natural progression of the idiopathic scoliosis. Compliance studies of clients using the Boston bracing system indicated that in some cases the brace was only worn 20% of the time, and therefore, the treatment was having little effect on the prognosis of the condition (Houghton et al. 1987).
Spinecor relies on elastic bands to apply a dynamic corrective force to the trunk to counter the de-rotational and translation aspect of the typical idiopathic scoliosis, however, the bracing system is contra indicated for use on the neuropathic curve (Coillard et al. 1999). This system uses a continuous pressure to “encourage” the spine to correction. The results have been mixed and the author is aware of issues in relation to abrasion, which have caused management concerns, however, the brace has good compliance and the treatment protocol indicates reduced treatment duration.
Triac® brace also provides a dynamic correction however any curves below T11 are untreatable due to the hinge section of the orthosis. Again, early trials (Veldhuizen et al. 2002) have indicated an improvement in the time the brace is worn and the curve corrections have been encouraging.
The author has been involved with the treatment of children suffering from cerebral palsy and other neurological conditions for eight years, and particular use of dynamic Lycra® orthoses (DLO) used in the treatment of neurological caused scoliosis.
The utilization of simple panels added to DLOs on the convex aspect of the curve has been used to reduce the progression in the early stages of neuropathic scoliosis in patients with cerebral palsy (Matthews 2003). The evolution of these garments has led to the design of the scoliosis corrective Lycra® orthosis.
Patient and method
The case study patient presented with a cystic tumour in her thoracic spine at the age of 5 years, with a three-week history of intermittent backache, which woke her at night. Examination indicated a left convex postural scoliosis without any rib hump. Her neurological signs were deficient from the greater trouchanter down, and she required a shoe raise to counter the left leg length discrepancy. Detailed MRI scans indicated a neurocytoma in the thoracic cord with a syrinx above which was excised. At the age of 7 years a recurrence was observed. The development of scoliosis after this type of surgery is not uncommon. As all neurological signs were intact, spinal corrective brace treatment should be the preferred treatment, however, the use of a rigid bracing system was not an option due to her previous experiences and the scoliosis design dynamic Lycra® orthosis was prescribed.
The standing, low dose, standard scoliosis brace treatment protocols were followed with pre- and post-brace X-rays to measure the effectiveness of the brace. Following intervention, the clinical team including the orthopaedic consultant, physiotherapist and senior orthotist reviewed the outcome.
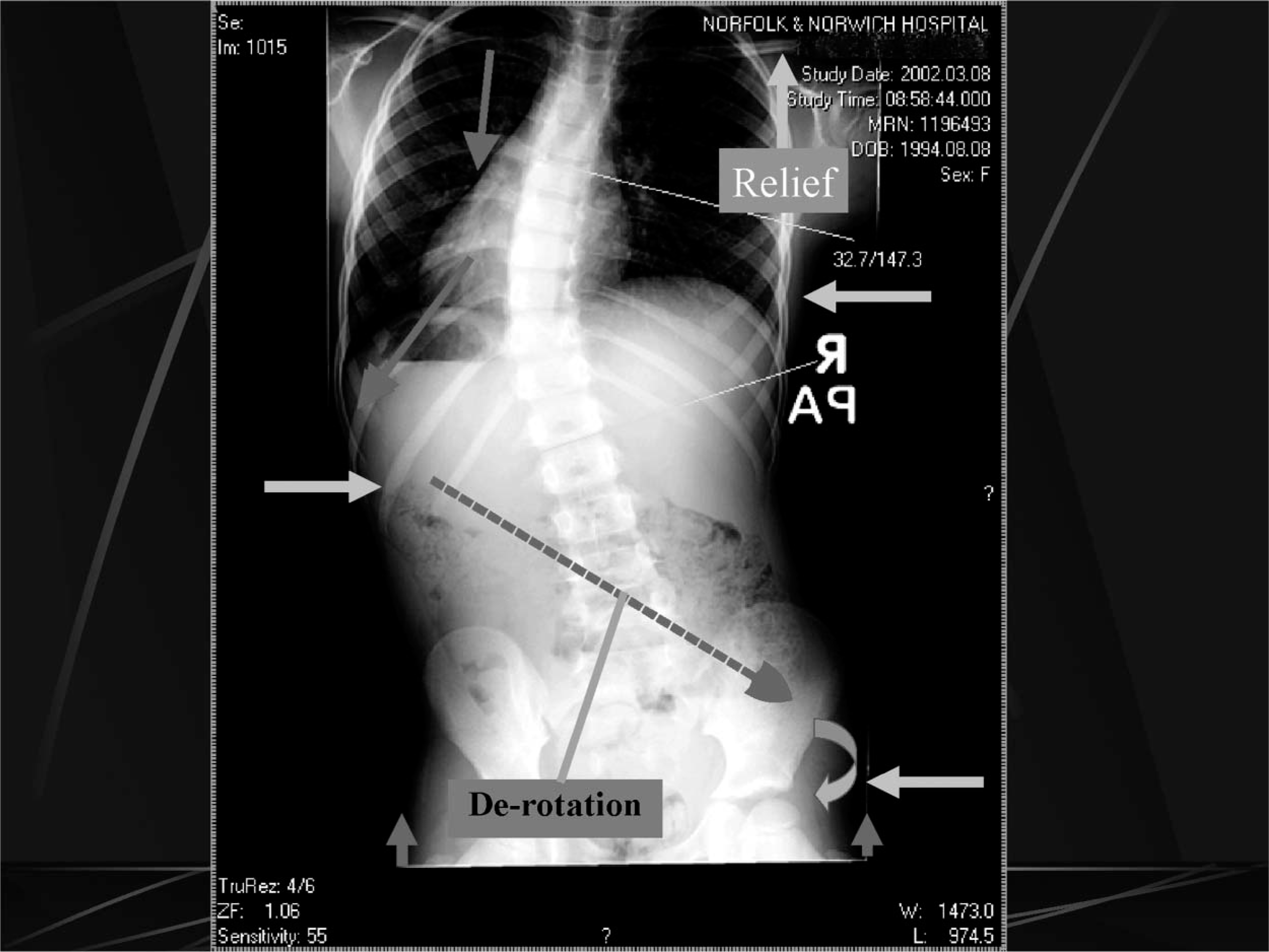
The initial pre-brace X-ray indicated a 33° curve with apex at the tumour site; T9 with a left curve with little or no compensation either in the lumbar or upper thoracic region. Circumferential and length measurements were taken to enable the manufacturers to produce the suit. The basic design was of a vest style extending down both legs to end superior to the knee, with a lateral panel that extended from centre front to centre back on the convex side to provide a resistance to the curve via the thoracic cage. In addition a de-rotatory panel (to counter the thoracic spine rotation) and two translatory panels (to reduce lateral shift often experienced in curve presentation) were added. The de-rotation panel extended down from over the axilla anteriorly and swept down diagonally across the mid back to end over the right anterior superior iliac spine. The aim of this panel is to compress the convex side of the curve and to counter the natural progression of the scoliotic curve rotation (Figure 1). A lay over Velcro® shoulder strap was fitted to the concave side to allow for the upward movement of the shoulder when the opposite side was compressed.
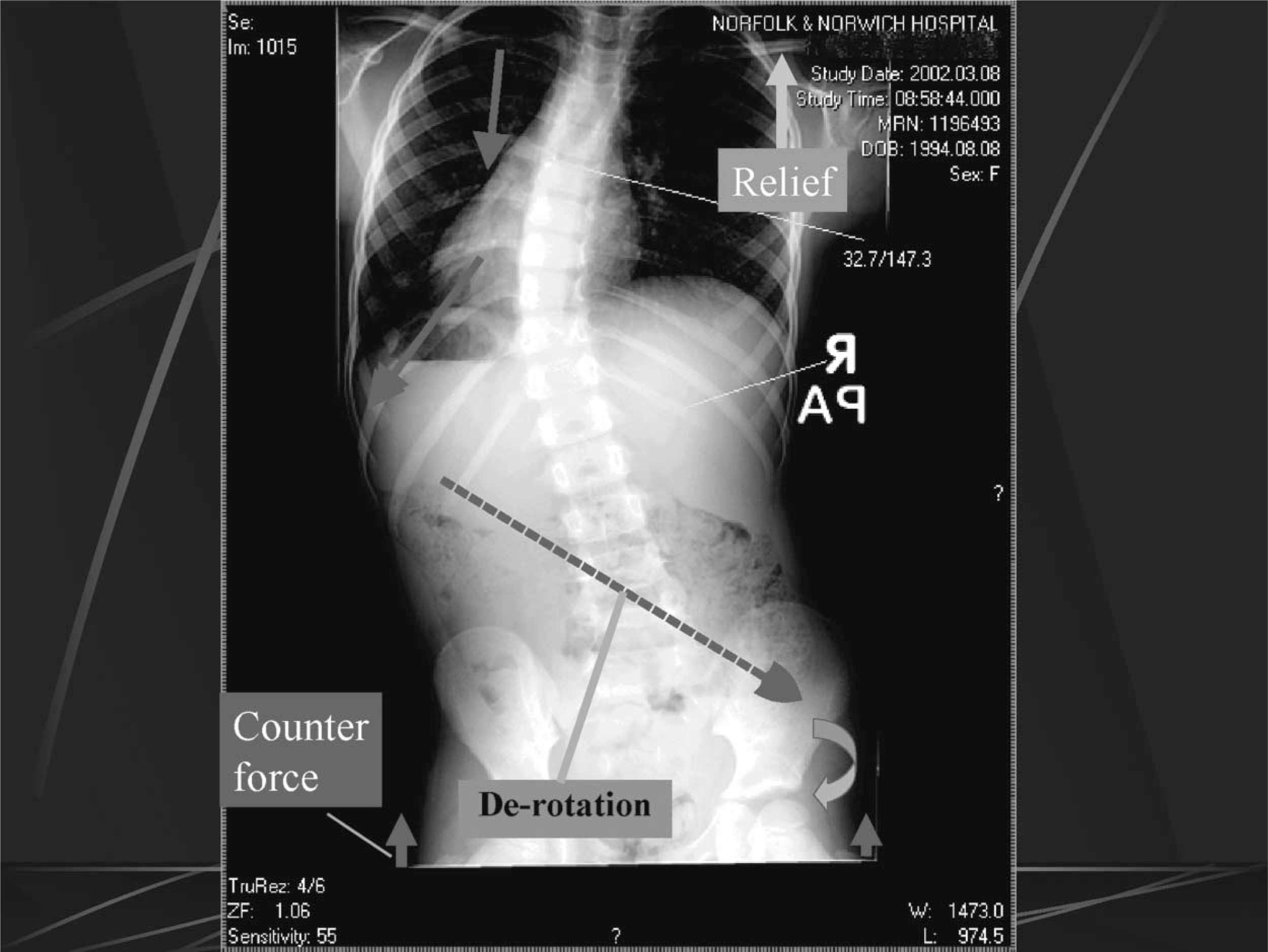
A vector diagram indicating the de-rotational moments built into the suit.
The translation force is provided by a ‘V’-shaped panel to both back and front sections, with the apex of the ‘V’ on the rib below the vertebral angle “null” point (Figure 2). The combination of both force corrections can be seen in the combined force X-ray (Figure 5) and are used to produce the dynamic orthosis issued to the patient (Figure 6). The ‘V’ section allows for a lateral shift within the spine to be initiated, and can lead to the patient experiencing a loss of balance as the midline is shifted temporarily off centre. The patient adapted to the new position within a short period of time.
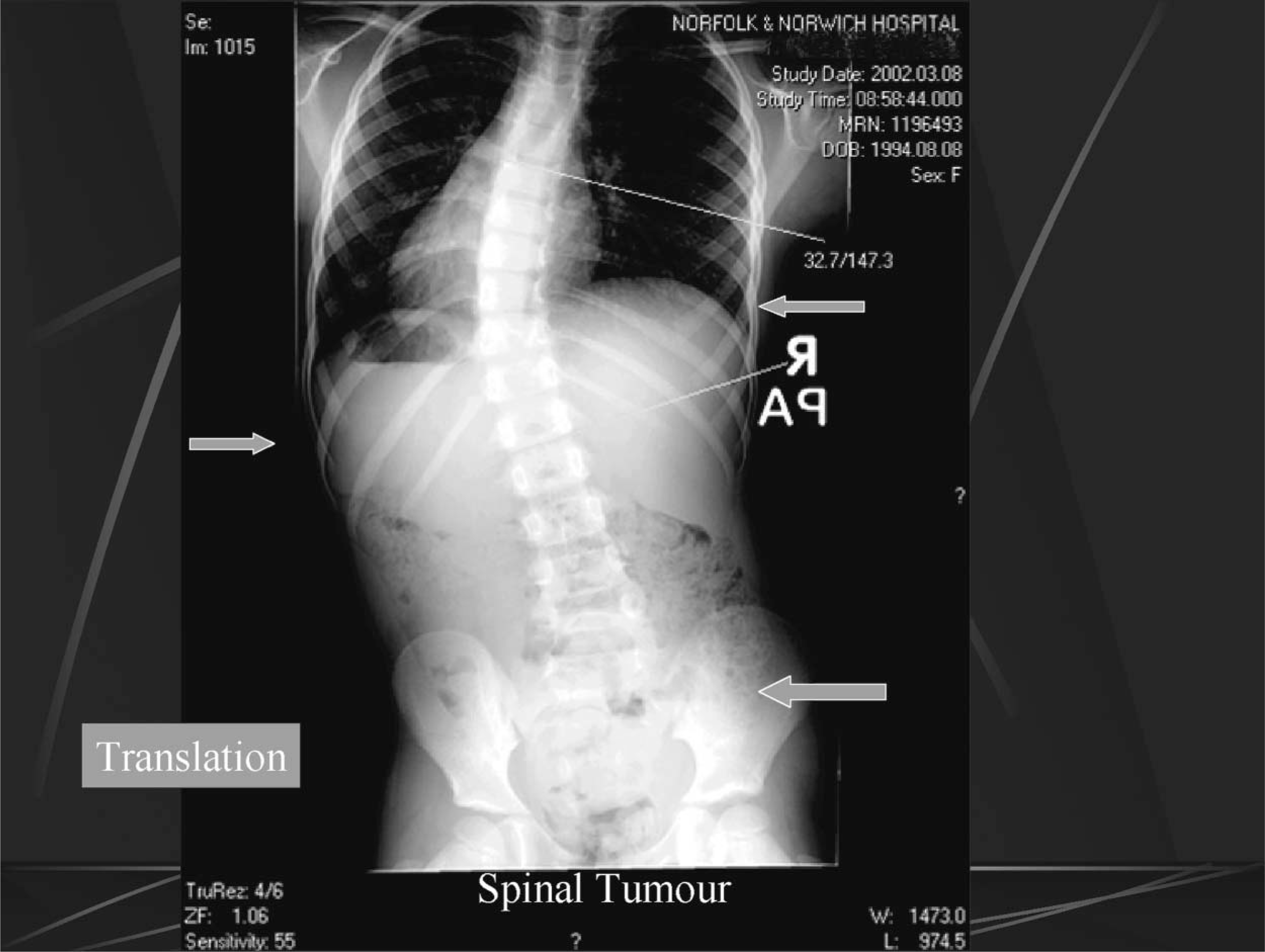
The lateral translation panel locations indicating the use of the X-ray to identify the exact positioning.
Results
X-rays of the patient wearing the orthosis have indicated a halving of the Cobb angle from 33° (Figure 3) to 15° (Figure 4). The tumour site can be clearly identified at T9/10. The patient also wore a small heel raise of 18 mm in the second X-ray. The raise reduced the pelvic tilt but not the scoliosis as the vertebral angle takes off at the L5 level. If using a Boston brace a troucanter extension would have been prescribed to control this aspect.
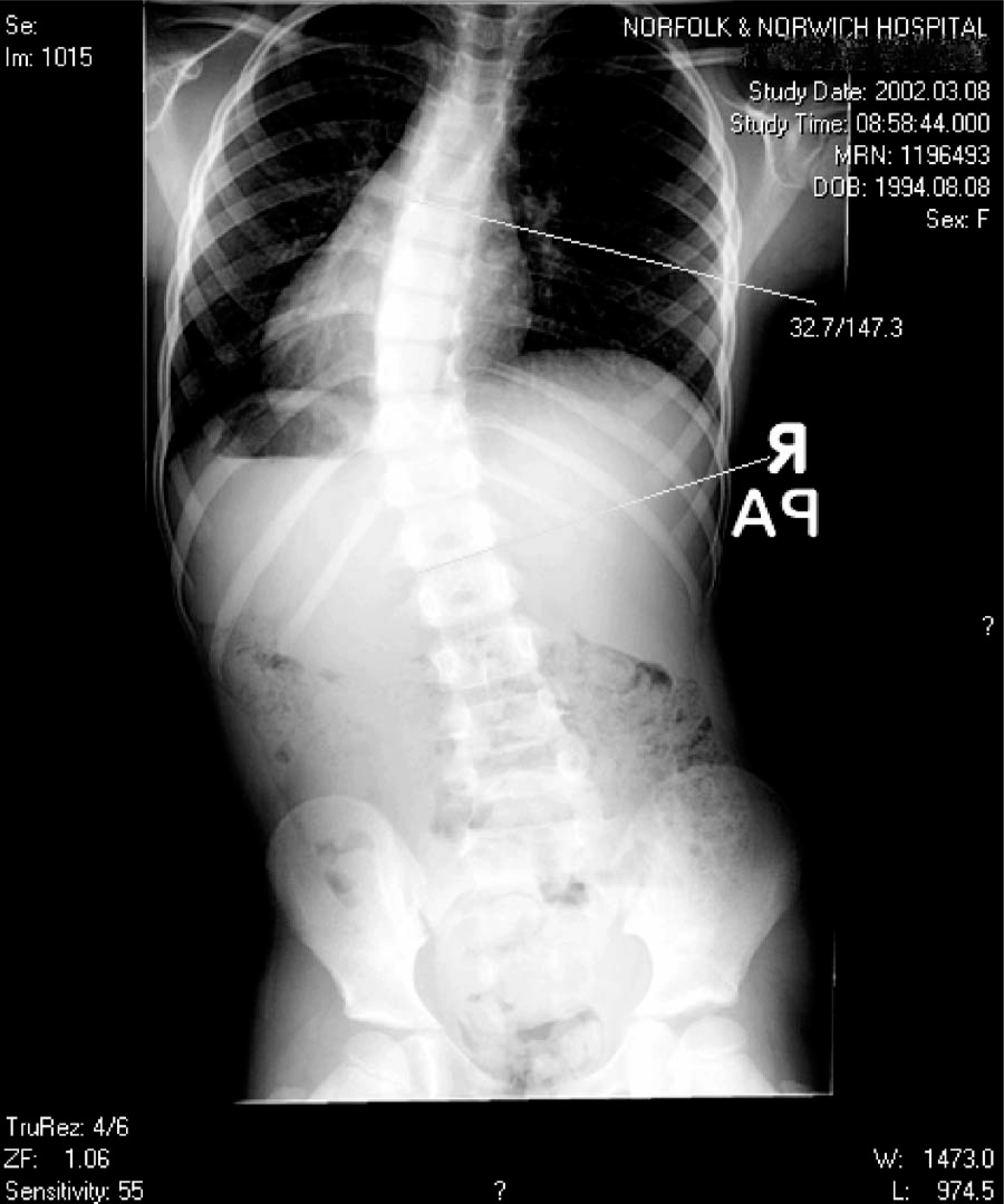
X-ray before dynamic Lycra orthosis.
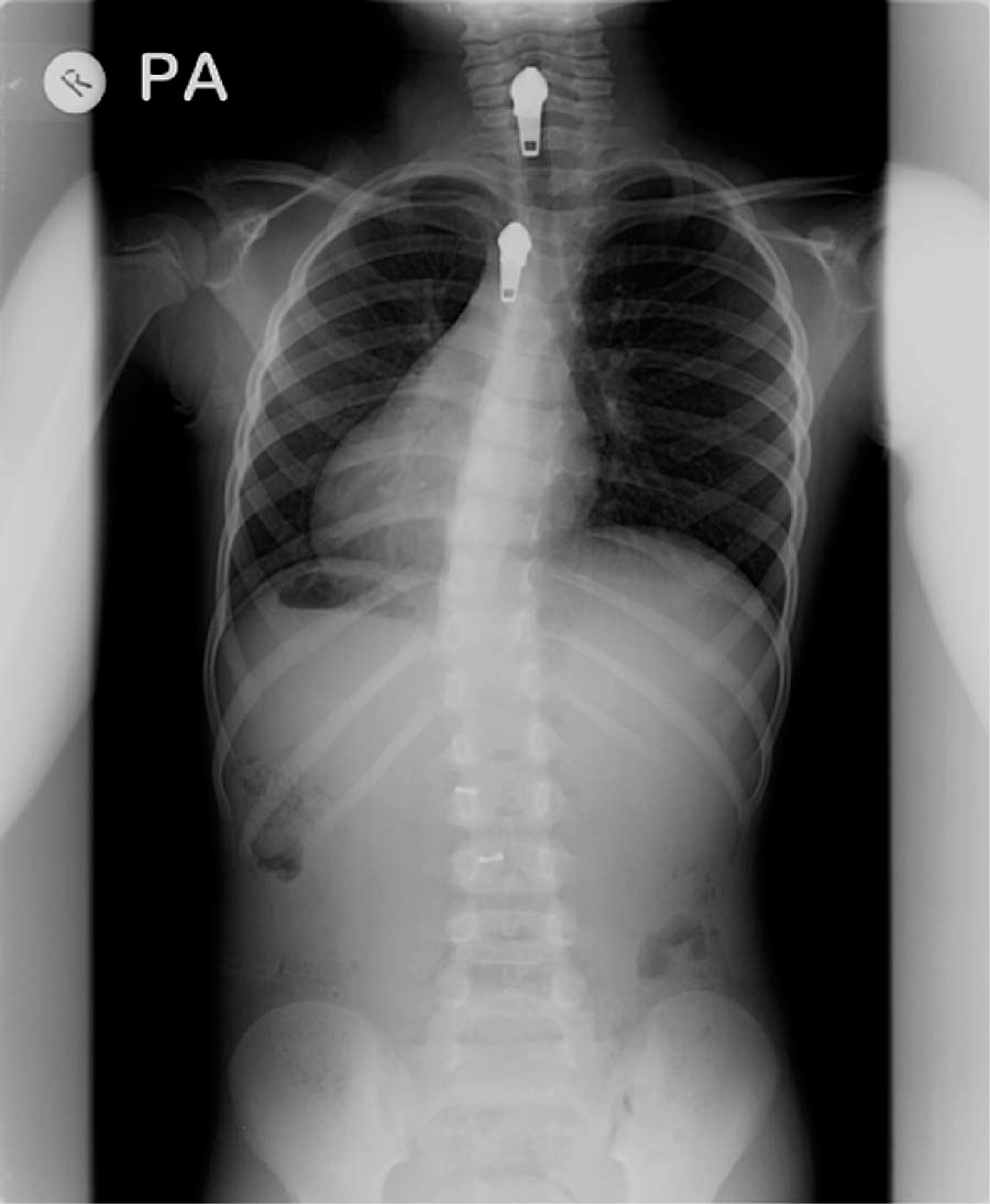
X-ray in dynamic Lycra orthosis (note the zips).
Subsequent X-rays have indicated that the curve has been held for 30 months at 20°. Unlike rigid bracing this angle has been held, even when not wearing the suit, suggesting that the patient has developed the muscle control to counter the natural curve progression.Figure 5
Vector description to indicate the combined de-rotation and lateral translation forces built into the scoliosis suit.
Initially the patient felt off-balance but quickly adapted to the new position.
The patient has found that wearing the orthosis has not hindered her activities and allows her to go swimming when on holiday (onlookers comparing her suit to the current vogue for ultra violet light spectrum blocking garments available to protect children from the sun). The garment only required simple laundering after swimming. Compliance was good with 23 h of continual wear every day. No skin deformation or discoloration was experiencedFigure 6.

The dynamic Lycra orthosis used to obtain the results in the X-ray above.
Discussion
There are different possibilities for discussion as to why orthosis appears to be effective:
The suit gives a total “body awareness” through proprioceptive feedback (Laskowski et al. 2000) and therefore allows for an improved alignment of the spinal segment.
The extra panels give a corrective and directory force. (The rigid braces push the spine up until the resistance is felt at which point the brace requires further modification that can become uncomfortable over the long-term). The Lycra suit is truly dynamic and continues to influence the correction by a long, continuous pressure even when the body segment is at rest.
The suit guides rather than pushes the spinal segment into an improved postural position.
The suit appears to counter the natural rotation of the scoliosis by countering the natural progression of the curve and applying a pressure to the convex side whilst allowing for movement in the concave aspect.
A de-rotational aspect is initiated by the diagonal and rotational elements of the reinforcement panels.
Muscle tone does not appear to be diminished. In rigid bracing reduced muscle strength has been noted. All exercise, including swimming, is possible in the suit, the only orthotic spinal treatment to allow this.
The suit is cosmetic and is similar to a vest in fit and cosmesis.
Conclusion
The dynamic Lycra® spinal corrective orthosis when combined with an appropriate heel raise has been found to reduce thoracic scoliosis with improved compliance and comfort. To date, it does not appear to have a detrimental effect on muscle tone and is capable of controlling the curves in mobile presentations.
As this treatment has only been used for 2½ years, it is too early to comment on the prognosis of the condition, but to date the garments have proven to be very effective with the orthotic treatment of mobile, idiopathic and neuropathic scoliotic presentations.
Following the successful result obtained in this trial, the scoliosis Lycra orthosis has subsequently been used in 6 other cases. The results are proving to be similar to this case study, but have still to be evaluated in the longer term.
Further research is required to further develop this treatment modality and to investigate whether continued use of this treatment could have an effect on the vertebral development in other presentations.
Footnotes
Acknowledgements
The authors acknowledge the help and encouragement of the Directorate of Orthopaedics and Mrs S. Morgan, The Jenny Lind Paediatric Physiotherapy Department, Norfolk, and Norwich University NHS Trust as well as the manufacturer of the orthosis: Trulife, 41 Amos Road, Meadowhall, Sheffield S9 1BX, UK.