
Abstract
The purpose of this study was to clarify the relationship between mechanical stress and tissue response of the contracted knee joint in rats and to propose a new design of contracture correction device for clinical use. Wistar rats were operated on to immobilize their knee joints with a procedure causing periarticular bleeding and were kept in flexed position for 40 days. At day 40, the immobilizing wire was removed, and after day 43, the contracted knee joint had been treated with tunable corrective devices secured by an external fixation method to the rear limb. These devices consisted of four types of motor-driving system which provided several different low-load and continuous stretch torques. Measuring the angle of maximum knee extension, its effectiveness was assessed comparing with a lower load and control group of natural recovery course. The device also had a cyclic joint movement within the acquired range of motion and an oval cam mechanism producing a small distraction force to the joint along its long axis. The results showed that an appropriate range of low-load continuous torque was more effective to correct joint contracture. On the basis of the animal experiment, a new computer-controlled, gas-driven contracture correction device was developed for clinical trial. It was concluded that mechanical application in a condition with low and continuous torque is a useful treatment for fixed joint contracture.
Keywords
Introduction
Joint contracture is a consequence of immobilization or various traumas, and is one of the most prevalent syndromes encountered in rehabilitation medicine (Halar and Bell 1998). In an immobilized condition causing joint contracture, biomechanical characteristics, which reflect the surrounding mechanical environments, respond to adapt to a newer circumstance, and histological and biochemical changes of joint tissue are associated with it. Quantitative studies have been accumulated to clarify the relationship between mechanical stress and tissue response (Brand 1995, Frost 1983, 1988).
In daily practice, changes in size and shape in living tissue are often encountered which reflect the tissue response to a modelling and remodelling process:
abdominal wall of pregnant women; enlargement of the skin and soft tissue by tumour growth; soft-tissue expansion in behaviour and customs of the world; bone-deformity correction (drifts) after fracture union; leg lengthening in orthopaedic surgery and tissue expansion in plastic surgery.
In those conditions, the common aspect is a very small but continuous tissue stretch with or without minimal pain.
The research results reported in the past have already confirmed a possibility that low-load, long-lasting tension is effective to encourage growth of connective tissues and could be a useful treatment for a fixed joint contracture (Bell-Krotoski and Figarola 1995, Flowers and LaStayo 1994). For further improvement of treatment, a new corrective device and therapeutic equipment will be required on the basis of a quantitative understanding about pathological mechanisms of contracture development in relation to mechanical stress (Brand 1995). Trudel et al. (2003) used the term ‘mechanotransduction’ pathways to describe this phenomenon. If one is able to modulate signal detection at the level of cells or tissue, one can manufacture musculoskeletal systems through tissue remodelling.
On the basis of the above hypothesis, the purpose of this study was to test the effect of low-torque and continuous stretch reducing knee flexion contracture quantitatively and to propose a prototype design of a new contracture correction device.
Materials and methods
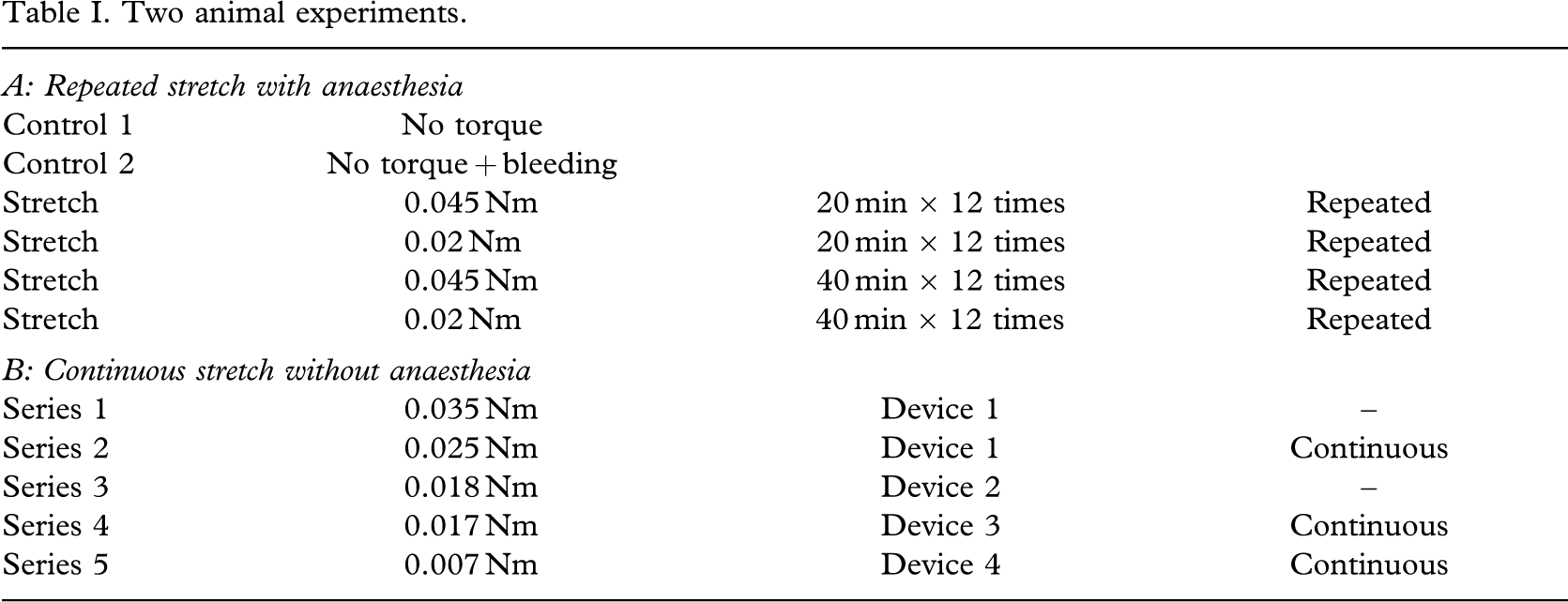
To warrant the validity of the authors' hypothesis, two series of animal experiments were performed (Table I). Based on the results of animal experiments, the authors tried to develop a new device for clinical use.
Two animal experiments.
Animal experiment
Two operative procedures of wire ligation to make a joint contracture
Seventy-eight, 6-week-old male Wistar – Imamichi rats, initially weighing 170 – 190 g were used. Under intraperitoneal anaesthesia with the mixture of 57.6 mg/mL of ketamin hydrochloride and 23.3 mg/mL of xylazine (Ketalar 50 and Celactal for 0.15 mL per body weight of animal), a subcutaneous femorotibial ligature with surgical wire (diameter 0.7 mm, Mizuho Ika Kougyo) on the left rear limb was performed to keep the knee joint in approximately 135° of flexion (Wilson and Dahners 1988). Wire insertion was done by means of two different inserters. This simple ligation group served as the subjects for a repeated stretch procedure and the Control 1 which indicated a natural recovery course.
Another 21 rats were used as the subjects for a continuous stretch experiment, and a further six as another control (Control 2) with the same ligation and periarticular invasive procedure. Under the same anaesthesia, the lateral femoral condyle was approached via parapatellar incision. Sharp dissection of the soft tissue layers exposed the periosteum close to the articular cartilage of the lateral femoral condyle to be perforated with a drill of 1.0 mm in diameter. With this procedure, some bleeding around and into the joint cavity was induced to make a stiffer contracture than with simple ligation. All rats were kept freely after operation in their cages, and then the wire was cut and removed at day 40.
Four conditions receiving a repeated stretch with anaesthesia
The setting of an appropriate correction torque was an essential step of the present experiment. A search for an appropriate torque range for repeated stretch was conducted under anaesthesia as the first stage of the animal experiment. In this experiment (A), the four groups of animals received a total of 12 treatments in 4 weeks, i.e. three treatments a week (every 2 days on weekdays) given by one of the authors (MU). The values of the torque used for stretch and the treatment time were 0.045 Nm × 20 min, 0.02 Nm × 20 min, 0.045 Nm × 40 min, and 0.02 Nm × 40 min. Ten rats from the simple ligation group (Control 1) and the other 6 from the ligation and periarticular invasion group (Control 2) were also used as references without stretch.
Measurement of the angle of maximum knee extension
The measurement of the angle of maximum knee extension in the repeated stretch group and in Controls 1 and 2, were performed under intraperitoneal anaesthesia with ketamin and xylazine. These drugs were selected to decrease the risk of animal death by repeated anaesthetizing. An electric blanket was also used to maintain the body temperature of the animals during angle measurement. After the addition of 0.8 N at the distal end of the lower leg, the angle of maximum knee extension, the external angle from the supposed starting position of the full extension between the long axis of the femur and the tibia, i.e. the greater trochanter of the femur, the centre point of the lateral femoral condyle, and the lateral malleolus, were measured using a plastic goniometer.
Four types of contracture correction devices without anaesthesia
The correction devices were controlled by a personal computer and were able to provide a constant torque. In the series of continuous stretch experiments, four different devices were alternately used to check each specified performance and supported at each step by computer software developed by the authors (Figure 1). In preliminary testing, the first device was checked for functionality under anaesthesia. The contracture angle decreased drastically within 1 h. In the experiment, the devices were activated without anaesthesia.
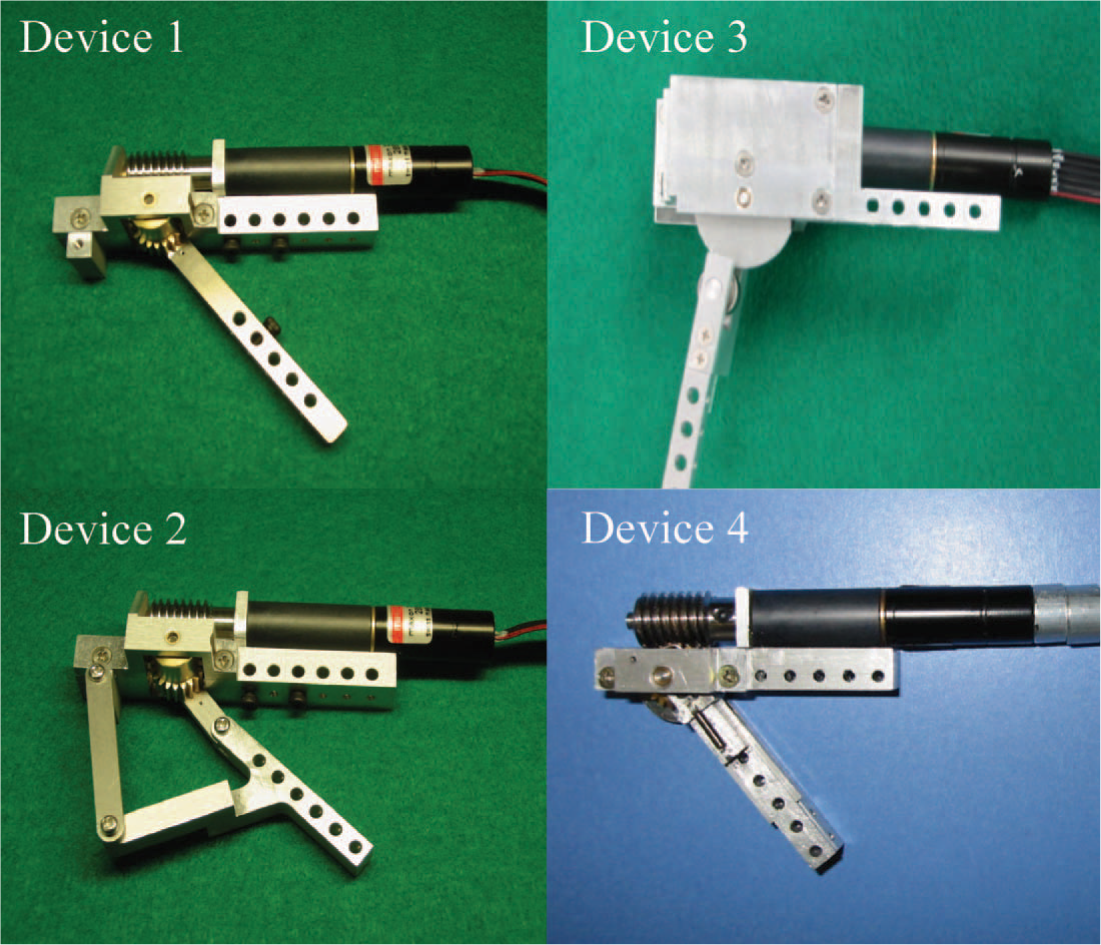
Four types of contracture correction device. The first weighed 68 g and provided 0.035 Nm or 0.025 Nm extension torque. The second weighed 57 g and provided 0.018 Nm with a cam mechanism. The third weighed 60 g and provided 0.017 Nm. The fourth weighed 52 g and provided 0.007 Nm.
The first device provided 0.035 Nm or 0.025 Nm of torque and was used in the first two series, in which regular recording of joint angle every hour and every 15 min, respectively, and cyclic joint motion within the range achieved were confirmed. The second device provided 0.018 Nm of torque and used another joint-movement system. The third device provided 0.017 Nm to investigate the minimal effective torque value at the early phase of its application and was applied to check a cam mechanism working as protection of articular cartilage to avoid overstress against articular surface. The fourth device had a different cam system and produced only 0.007 Nm of extension torque.
Fitting of the correction device and other equipment
Under intraperitoneal anaesthesia with pentobarbital sodium (4 mg/100 g body weight), the motor-driving device was secured on the lateral aspect of the left rear limb with the help of special threaded fixation pins (diameter 1.2 mm, Ito Ika, Japan) (Figure 2a). Once fitted, the device produced a constant extension torque against knee contracture to achieve correction and had to be hung up by a string. The animal body was also suspended using a body sling to lift the rear limbs. The body sling and the device were tied to the moving blocks of a rail on the ceiling. With the aid of these moving blocks, the animals were able to move around their cage. The upper front limbs were kept on the floor to allow feeding (Figure 2b). A goal of 5 – 7 days was set in keeping the animal under these conditions.
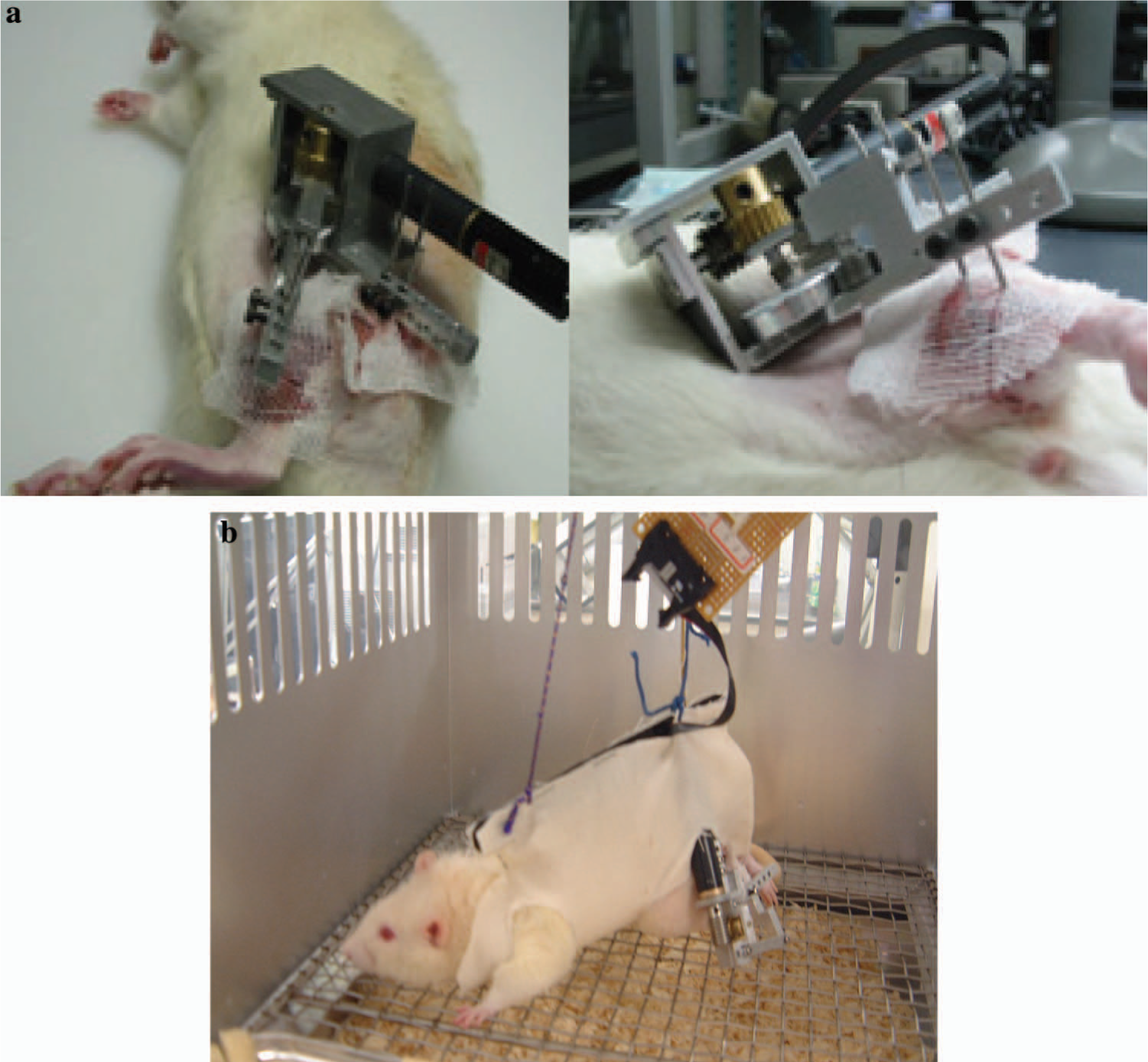
(a) Pin fixation of the third type of correction device. (b) Rat with a contracture correction device (first type) under suspension. The device, secured on the lateral aspect of the rear limb with external fixation and suspended sling, provides continuous extension torque.
The animals lost approximately 35 – 40 g of body weight in a week of preliminary tests as a direct result of body suspension.
X-ray check
The device automatically recorded the angle between the main part secured along the femoral shaft and the moving arm on the middle of the tibia during the experimental period (Figure 3). As the tibia of the rat was anteriorly bowed, however, an adjustment was needed to obtain an accurate knee angle. An X-ray check was done to detect the discrepancy between the moving axis and the anatomical axis of the lower leg (the centre point of the lateral femoral condyle and the lateral malleolus).
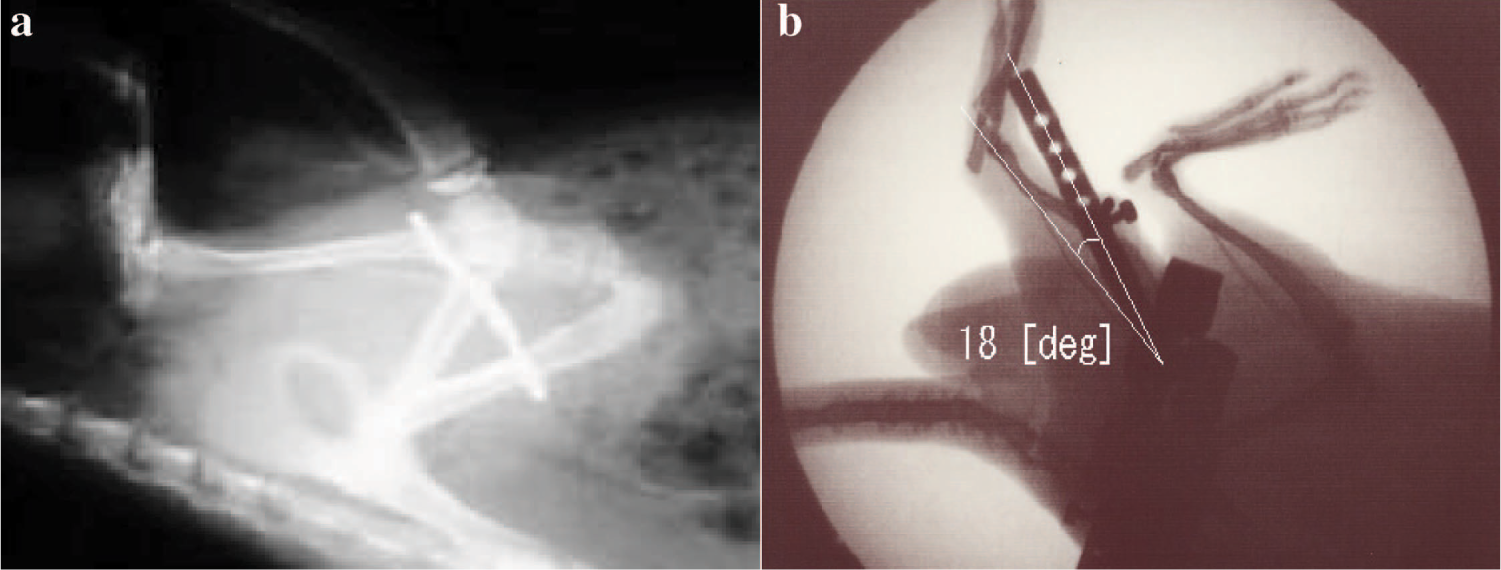
(a) X-ray of wire ligation against the rear limb. (b) Soft X-ray of the rear limbs fitted with a contracture correction device. Adjustment for −18° was needed to gain an accurate knee angle because the tibia of rat was anteriorly bowed.
Statistical analysis
Statistical calculations according to analysis of variance (ANOVA) were applied to test for differences among the groups for body weight gain and the angle of maximum knee extension in the first week. The analysis was carried out using a commercially available computer software program (Statview, Berkely, CA, USA).
Developing a new device for clinical use
Two innovative features added to the device
When external stress is applied to the joint, protection of articular cartilage must be considered with caution. In the process of designing a contracture correction device, two innovative features were incorporated in the torque application structure. The first was to keep the nutrition of the synovial (joint) fluid through as much cyclic joint motion as possible. With the aid of computer software, prolonged stretch activity had an intermittent break period every 15 min when the achieved range of motion was traced as well as measured. The second feature was to avoid overstress against the articular surface. Considering the fact that the majority of joints do not have a fixed rotational centre but an instantaneous centre and joint ‘play’, avoidance of overstress was achieved by applying a small distraction force to the joint along its long axis by means of a cam mechanism.
A new prototype design for clinical use
The use of gas pressure as a power source has been reported in the mechanisms of contracture correction devices (Bentham et al. 1987, Karachalios et al. 1994, Keeping and Major 1999). By fine-tuning the control by means of a computer, the applied torque was constantly adjusted, and a soft tissue reaction followed in a viscoelastic nature (Akai et al. 1993) in the short term and in tissue growth in the long term (Thompson 1995). The correction device (made by Hitachi Medico) had both a cyclic movement produced and an oval cam mechanism.
Results
Status of the animals
Of the original 78 rats in Experiment A, 51 were used this study, and 27 were excluded: nine due to death before day 40, four due to death after day 43, 12 due to wire loosening by infection or fracture, and two due to insufficient weight gain. Among the 51 available rats, body-weight gain at the time of day 40 was as follows: 355.5 ± 29.7 g (N = 9) for 0.045 Nm × 20 min, 381.5 ± 44.7 g (N = 10) for 0.02 Nm × 20 min, 363.6 ± 32.3 g (N = 8) for 0.045 Nm × 40 min, and 391.8 ± 25.9 g (N = 8) for 0.02 Nm × 40 min. The 10 rats from the simple ligation group (Control 1) were 369.1 ± 27.9 g, and the six from the ligation and periarticular invasion group (Control 2) were 367.6 ± 32.2 g.
In Experiment B, 21 rats were used, and four were eliminated secondary to little weight gain with or without an infectious abscess after removing the wire. When the surgical wire was removed, the animals were already 12 weeks old with an average body weight of 384.6 ± 12.2 g. No significant difference was found in body-weight gain during the 6 weeks, i.e. among the 17 available rats for the continuous stretch with external fixation device and the two control groups.
Time course of the angle of maximum knee extension
The knee joint angles of the two control groups were measured under a fixed extension torque of 0.04 Nm (0.8 N × 5 cm of lever arm between the centre of the lateral femoral condyle and the lateral malleolus) and under anaesthesia. The results of the two control groups are shown up to day 28 (Figure 4a).
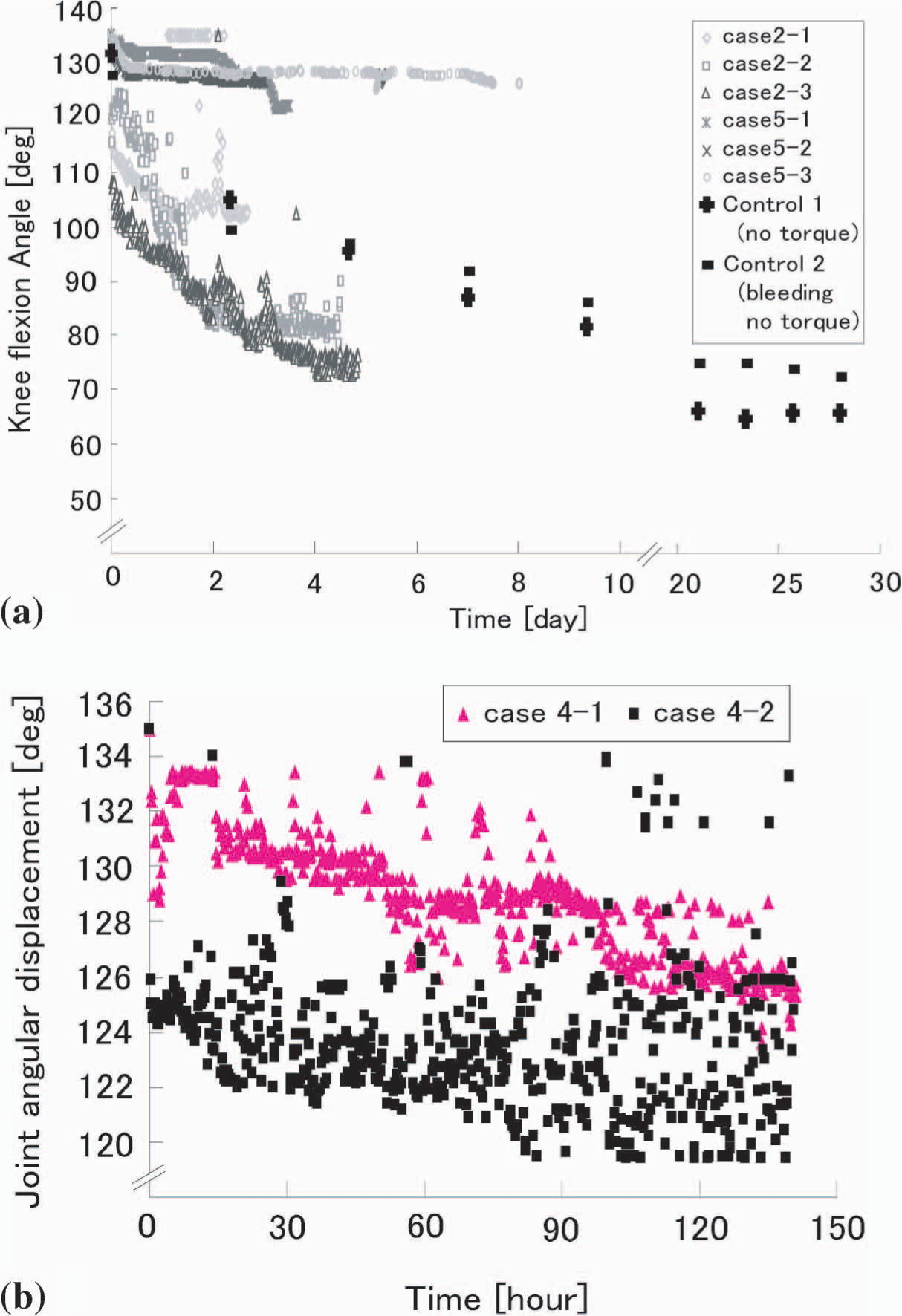
(a) Time course of the angle of maximum knee extension in two representative series. The results of the second series with 0.025 Nm and the fifth series with 0.007 Nm as constant torque are shown in comparison with the Control 1 (no torque) and Control 2 (no torque, periarticular invasion). The time course of the 0.025 Nm series is running under the control groups, and that of the 0.007 Nm series is running over the control groups. (b) Time course of the angle with the third type of device, i.e. the fourth series with 0.017 Nm, which showed the wide distribution of plot to indicate the minimal effective torque in each case.
In Experiment B, the first series with 0.35 Nm and the third series with 0.18 Nm, the authors failed to record the knee angle regularly because of problems in computer control.
In the second, fourth, and fifth series of the experimental group, the computer automatically recorded the angle of maximum knee extension every 15 min, which was compensated by −18°. Figure 4a shows the results of the second series with 0.025 Nm and the fifth series with 0.007 Nm making comparisons with Control 1 (no torque) and Control 2 (no torque, periarticular bleeding). On the contrary, the results with the fourth type of device with 0.007 Nm did not show any improvement in maximum knee extension, even after 8 days (Figure 4a).
Minimal effective value of continuous torque
In the fourth series with the third type of device, there was a wide distribution of the plot of knee angle within every 15 min period (Figure 4b). The line produced by joining the lowest plots on the recording chart was close to the knee-joint angle plot with the second series. This finding indicated an improvement in flexion contracture by continuous stretching with 0.017 Nm, even without anaesthesia, and reflected the resistive power of each animal against the applied extension torque. The animals with the third type of device seemed to behave more calmly and quietly than those with the first device in the cage.
New design of contracture correction device for clinical use
The device developed provided a wide range of torque value, angle recording function, and two variable systems, i.e. (1) the oval cam mechanism (1 mm/120°) and (2) a cyclic motion system (Figures 5a and b). Considering the similar size of the joints, this device could be applied to the proximal interphalangeal joint of human fingers. In addition, a piston-cylinder mechanism (stroke length: 9.1 mm at 120° flexion) was designed with a double lever action to execute a low load and continuous torque for the full range of motion of the joint. Figure 5a shows a design to gain further flexion; however, the device could be used to provide extension after reversal of the piston-cylinder and cam mechanism.
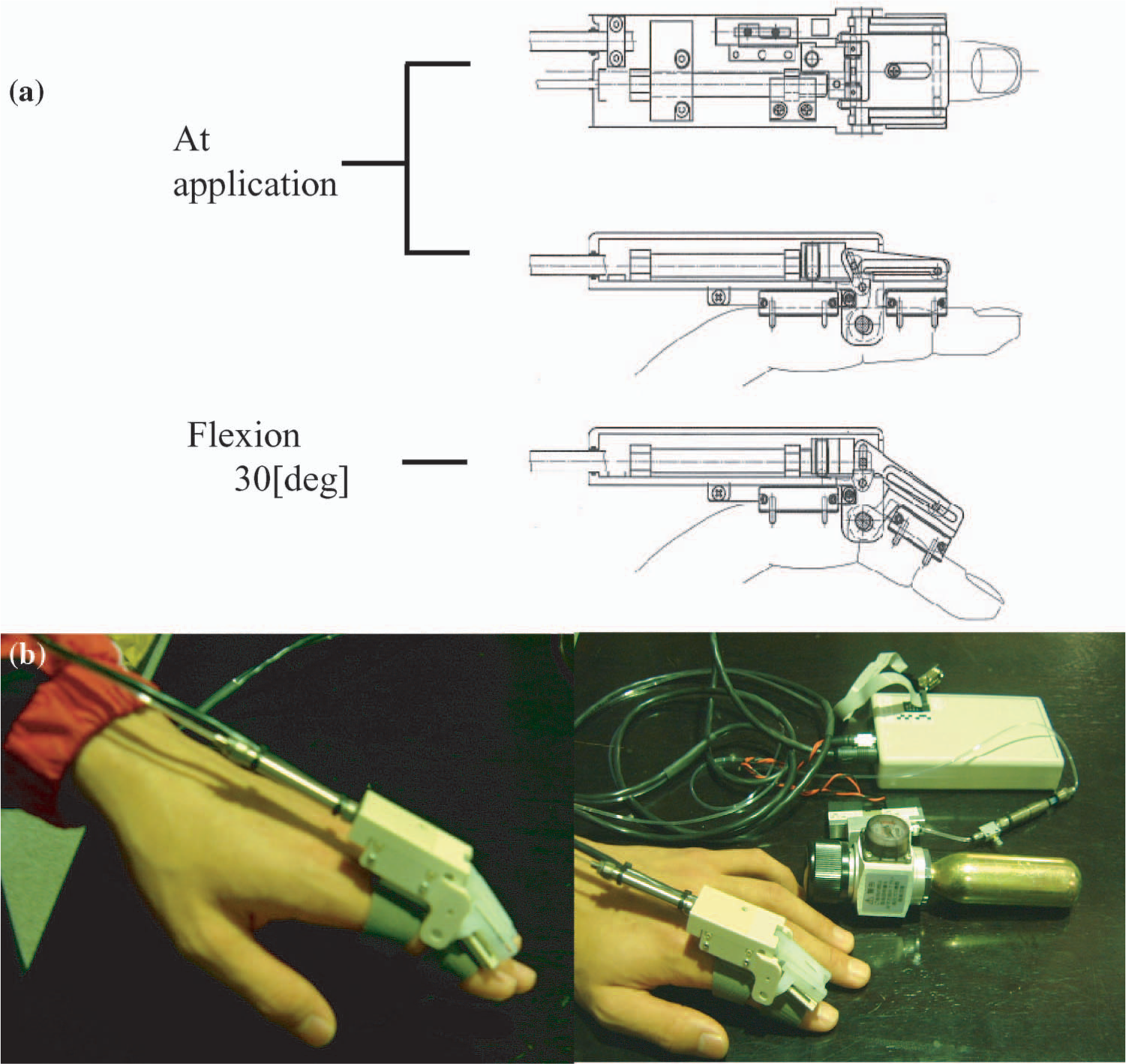
(a) Design of a new contracture correction device for clinical use. The device, fixed in the dorsal aspect of the proximal and middle phalanx, is able to provide a wide range of torque values, angle recording functions, and two additional systems with cam and cyclic motion. The rotational centre of the device corresponds with that of the proximal interphalangeal joint. (b) Gas-driven, computer-controlled, new contracture correction device.
Discussion
Joint contracture and its treatment
Joint contracture resulting from prolonged bed rest or immobilization leads to a greater degree of disability and jeopardizes the rehabilitation process. The so-called ‘heat and stretch’ technique combining physical modality (heat) and mechanical stress (Warren et al. 1976) is a widely used therapeutic method. The treatment programme for joint contracture consists of positioning, ROM exercise by a therapist and functional splinting, which include exoskeletal fixation, static progressive splinting (Barquet et al. 1993, Bonutti et al. 1994, Schultz-Johnson 2002) and other devices (Kasabian et al. 1998, Charlton et al. 1999, Gelinas et al. 2000). External fixation systems, such as the Ilizarov method, have been used for joint contracture as well as leg lengthening (Damsin and Ghanem 1995, Huang 1996, van Roermund et al. 1998). In more specific conditions such as the postburn contracture, a dynamic system (Joshi External Stabilizing System) that allows the lengthening of contracted tissues by slow distraction has been used for over 20 years (Gulati et al. 2004). To measure joint contracture more precisely, a device controlled by fine-tuning has been developed in an experiment on rabbits (Hildebrand et al. 2003).
Working hypothesis (low-load and continuous stretch)
When the authors started the present study, their working hypotheses were as follows:
Physical modalities such as mechanical stress play an important role to maintain and reveal various cell functions. External mechanical stress compensates for the necessary signals of under-loaded tissue to minimize or prevent changes due to disuse that are caused by rest or immobilization of the musculoskeletal systems. An appropriate stimulus is essential to maintain the metabolic processes of the cell, and low-load and continuous mechanical stress stimulates tissue growth.
When a mechanical stress is applied to living tissue, its response depends upon time factors. After a short period of time, the response of the tissue is based on its viscoelastic properties. Over a long period of time, a biological response is observed with tissue growth evoked by the mechanical stimulus.
Ligament and periarticular tissue have several specific characteristics related to mechanical stress; unlike muscle, there is no voluntary movement, and they are not influenced by energy metabolism over a short time period but are influenced by their viscoelastic properties.
The basic concept of the present study is stimulation of tissue reaction by a prolonged stretch. From a quantitative point of view, Bell-Krotoski and Figarola (1995) stated that a force in the range of 100 – 200 g applied at a point several centimetres from the joint should be sufficient to start that process. Although several clinical studies have demonstrated a significant clinical effect with a low-load prolonged stretch (Light et al. 1984, Nuismer et al. 1997, Steffen and Mollinger 1995), few experimental studies showed the so-called ‘tissue stimulation’ effect quantitatively through cellular function and collagen synthesis change (Nuismer et al. 1997). The authors would like to conduct a precise experiment to investigate this.
New contracture correction device for clinical use
The device that was developed provided a wide range of torque in order to relate data from animal experiment to clinical cases. In the present animal study, one of the main concerns was the possible effect of the different conditions with or without anaesthesia. The authors could not confirm whether or not the animals felt pain during application of extension torque. In addition, the authors were also unable to assess the amount of physical burden caused by the application of the correction device, external fixation, weight of the device, and body suspension, though the lower torque appeared to be less invasive for the animals. This is an unavoidable problem when using an animal model to mimic the clinical situation.
Determination of torque value and its application form
If the range of torque used in this experiment could be regarded as remaining within the elastic range, the low-level torque may affect soft-tissue remodelling. This finding is partly compatible with the previous study by Dent (1993) and O'Driscoll and Giori (2000), who indicated a more effective recovery process in the low-torque and long-period stretching condition. Dent (1993) described an ‘intelligent’ continuous passive motion machine for fingers controlled by a microprocessor.
The pattern of the extension torque in this experiment was constant throughout the whole range. The computer provided a constant torque among the serial angular positions. It is questionable whether a constant torque will provide a better result or not. If a constant gain of joint angle is needed, it might be necessary to adjust this by applying torque corresponding to a torque – angle curve.
Future problems
For clinical use with the present contracture-correction device, there was an obvious advantage in using a gas-driven system over an electrical motor-driven system because the former is more robust and easier to keep watertight during normal daily activity.
A new corrective device and therapeutic equipment will require further improvements on the basis of understanding the pathomechanisms of contracture development. It is hoped that this study could be expanded to other larger joints in a further clinical trial. A comparison of the outcomes using such experimental devices compared with those using conventional physical therapy will be needed before establishing definite conclusions.
Conclusion
Based on the results of animal experiments using the computer-controlled joint-contracture correction device, an appropriate range of low-load and continuous torque was found to be effective in correcting joint contracture.
Footnotes
Acknowledgements
This study is supported by a grant from the Ministry of Health, Labor and Welfare of Japan. (Health and Labor Sciences Research Grants 2001 – 2003) The correction devices used in this study were customized by Daiichi Sokuhan.