
Abstract
This paper reports findings of experiments aiming to (1) compare the load tolerant ability over different regions of stumps of lower limb amputees, (2) study the effect of walking on the load tolerant ability, and (3) examine the distal-end weight-bearing ability supported by different interface materials. The method was to apply increasing load to the stump up to the pain level through a force transducer or a digital scale, considering the effect of regional difference, walking, and interface materials. The results show that the patellar tendon and the distal end of the fibula were the best and worst load-tolerant region, respectively. Walking with prostheses tended to increase the load-tolerant ability, which is thought to be due to the massage-like effect of the socket. Different interface materials did not significantly alter the distal-end weight-bearing ability. However, there was a great difference in the distal-end weight-bearing ability among different subjects.
Introduction
Comfort is one of the most important considerations in designing lower-limb prostheses (Legro et al. 1999; Nielsen 1991). Discomfort may result from high stresses applied onto the limb region, which is not particularly tolerant to loading (Zhang et al. 1998). In an attempt to design a comfortable prosthesis fit, it is important to understand the stress distribution at the stump – socket interface as well as the pain-tolerant ability to externally applied stresses over different stump regions.
The basic philosophy for prosthetic socket design varies from either distributing most of the stress over specific load-bearing areas or more uniformly distributing the stress over the entire limb. The patellar tendon bearing (PTB) socket is one of most popular types of socket for trans-tibial amputees. The main principle of the PTB socket is to load more over the load-tolerant regions and to relieve pressure-sensitive areas (Radcliffe and Foort 1961). Many studies have been conducted to quantify the stress distribution at the interface between the stump and the prosthetic socket by either experimental measurements or finite element analyses, as reviewed by Mak et al. (2001), Silver-Thorn et al. (1996), Zachariah and Sanders (1996), and Zhang et al. (1998). The load-tolerant regions and load-sensitive regions have been identified qualitatively and have been used as guidelines for socket modifications for many years. However, quantitative information on the magnitude of pressure that different regions of the stump can tolerate is still missing. The measured or predicted interface stresses at the stump – prosthetic socket interface are of little clinical significance if the pressure-tolerant ability of different regions of the stump is unknown. In order to achieve a successful prosthetic socket fit so that pain would not be induced, one design criterion is that the stresses produced by the socket should be proportional to the ability of the limb to sustain the stresses, without crossing the thresholds to induce pain (Zhang et al. 1998).
Several investigations were conducted related to the pain responses to stresses applied onto lower-limb stumps. Global pain response of the stump to external pressure has been studied (Kelly et al. 1998; Neumann 2001). The ability of the distal end of the stump to tolerate load was investigated (Katz et al. 1979; Persson and Liedberg 1982). More research is required to obtain quantitative data about the ability of the stump to tolerate stress so that the design parameters of an optimal prosthesis interface can be fully established. In addition, load is repeatedly and intermittently applied to the stump by the socket as the amputee walks. It is useful to understand if the load-tolerant ability is changed with load cycles.
The aim of this paper is to report the findings from several experiments, with three main objectives: (1) to evaluate and compare the load-tolerant ability over different regions of the stump; (2) to study the effect of walking cycles on load-tolerant ability of the stump; and (3) to examine the distal-end weight-bearing ability supported by different interface materials.
Methods
Twelve male trans-tibial amputee subjects participated voluntarily in the experiments. The subject information is shown in Table I. The subjects had no symptoms of peripheral neuropathy. Different amputee subjects were invited in the three experiments conducted at different times. Written consent was obtained from all participants. The experiments were conducted in line with the human subject guidelines of the Research Committee of The Hong Kong Polytechnic University.
Subject information of the participated trans-tibial amputees.
Pain responses of different regions of trans-tibial stump to pressure
Eight male unilateral trans-tibial amputee subjects (subject number 1 – 8) participated voluntarily in this part of the study. They were asked to sit comfortably, resting their stumps with one knee extended on a support. Force was applied to the test regions perpendicularly to the skin surface through a circular flat-ended Pelite indenting material of 12 mm diameter and 4 mm thickness connected to a force transducer (maximum load 200 N). The force was increased gradually until the subjects said ‘stop’ (Figure 1a). The load rate was manually controlled at about 4 N/s. The subjects were instructed to say in Chinese ‘painful’ and ‘stop’, respectively, when they started feeling pain and could not stand the pressure any more. Force magnitudes were recorded from the force transducer when the subjects said ‘painful’ and ‘stop’. Pressures corresponding to the pain threshold and tolerance were calculated by dividing the force magnitudes by the contact surface area of the indenter.
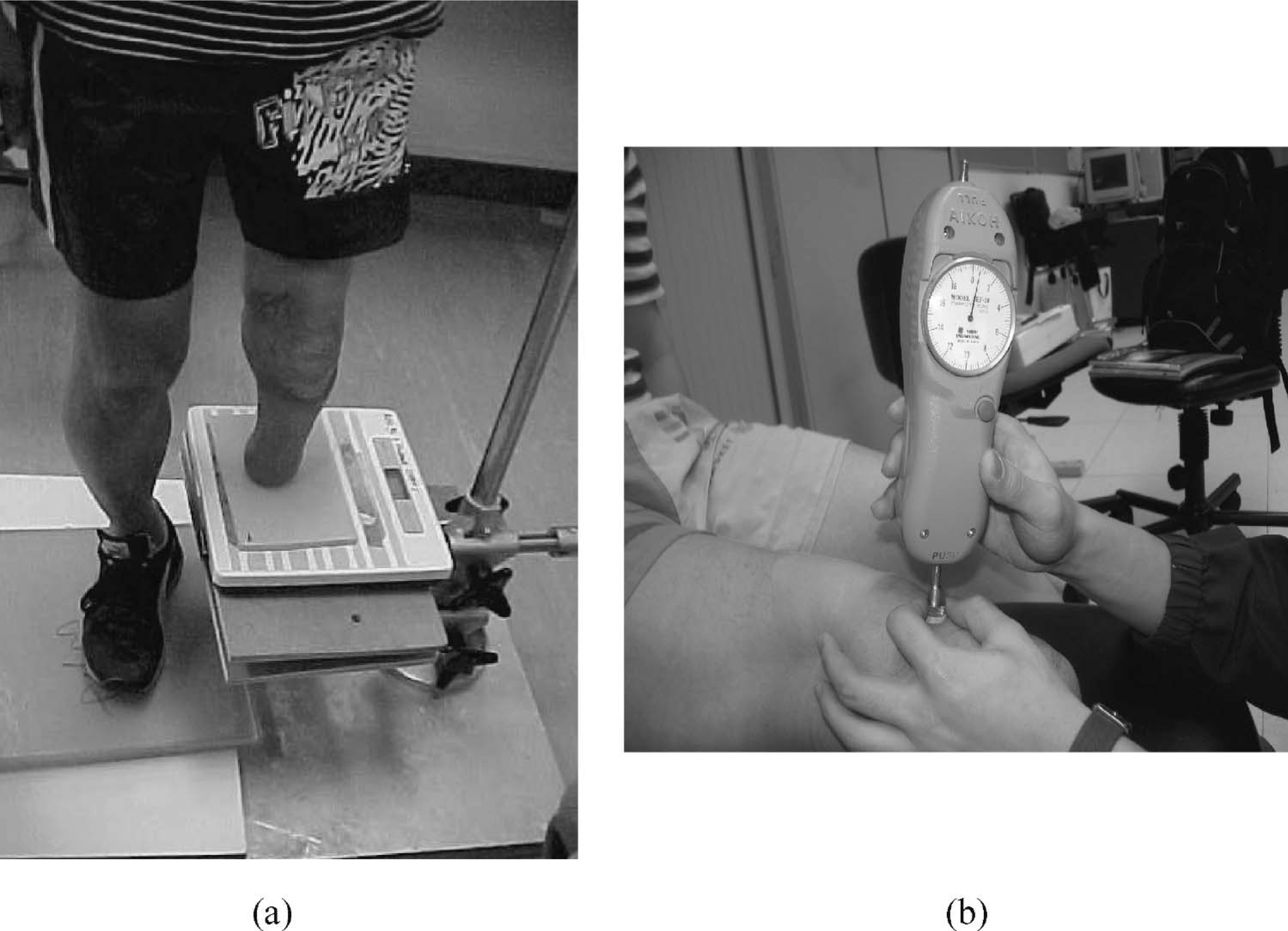
Experimental setup: (a) distal-end loading test; (b) indentation test.
In this section, the test regions were mid-patellar tendon, medial tibial flare, mid-shank of fibula, popliteal muscle, anterolateral and anteromedial tibia, which are believed to be load-tolerant regions in PTB socket design, and tibial tuberosity, mid-shaft of tibia, fibula head, distal ends of fibula and tibia, where commonly load relief is needed in socket modifications. The whole test was performed twice, and the pressure values at each test site were averaged.
Effect of walking cycles on the pain-tolerant capability of weight-bearing regions of the trans-tibial stump
Six subjects (subject numbers 1 – 6) participated in this part of the study. The self-selected comfortable walking speeds of the subjects were measured by timing the subjects walking through a 10 m walkway. The subjects were requested to walk for four trials on a treadmill operated at the recorded comfortable walking speeds. At each trial, they walked for an assigned number of walking steps: 500, 1000, 1500, and 2000 steps. To reduce the carryover effect, the order of the trials was randomized, and at least 30 min rest was given to the subjects between trials. Immediately after each walking trial, pain threshold and pain tolerance over six different regions of the stumps were measured. The pain-measurement method was the same as that used in the previous section. The six test sites studied in this section were mid-patellar tendon, medial tibial flare, medial tibia, lateral tibia, mid-shaft of fibula and popliteal muscle. They are believed to be the load-tolerant areas where a relatively high magnitude of pressure is produced by a prosthetic socket during walking. Before the walking trial, pain threshold and tolerance were measured twice with a 30 min rest interval. The repeatability of the measured pain threshold and tolerance on the repeated indentation tests was assessed by the intraclass correlation coefficient (ICC). ICC model (3, 1) was used for a single measurement at each trial taken by one experimenter.
Stump distal-end weight-bearing ability of trans-tibial amputees with various soft interface materials
Five male unilateral trans-tibial subjects (subject number 8 – 12) were involved in this study. Digital bathroom scales with a maximum load of 136 kg were used to measure the load applied over the distal end. The scale was mounted on a height-adjustable stand (Figure 1b). The subject was in standing position and asked to shift his body weight to the amputated side onto the scale gradually until pain was felt. During the weight shift, the stump was kept vertical to the scale. The subject was requested to report immediately the onset of pain, and the reading displayed on the scale when pain was just felt was recorded. The distal-end load-tolerant ability was presented as the percentage of the recorded load to the body weight of the subjects.
Each subject has to load the stump against five different interface materials of 6 mm thickness on the digital scale. The order of the use of interface materials was randomized. The five interface materials often used at body – support interfaces are Pelite, Multiform, Plastazote, Nora Lunalastik, and Poron. The test was performed four times, and the means and standard deviations were calculated.
Results and discussion
Table II shows the difference in pressure-tolerant ability among different test regions. The mid-patellar tendon was shown to have the best pressure-tolerant region among the 11 test sites. Statistical analysis using SPSS 11.0 reveals that the mid-patellar tendon region tolerated a significantly higher pressure than the distal end of the fibula under both pain threshold and tolerance conditions (P < 0.05). As far as other test regions are concerned, the tibial tuberosity, fibular head, medial tibial flare, and mid-tibial crest on average had a higher ability to tolerate pressure than medial and lateral regions tibial, mid-shank of fibula, and popliteal muscles. However, no statistically significant difference was found with these test sites. The relationship of the pain-tolerant ability (subjects 1 – 8) to their body mass index (BMI) was studied using the Pearson product-moment coefficient of correlation. The results showed that there was no close correlation between the pain-tolerant and their BMI (r < 0.5). The indentation test method was similar to that used in previous studies focusing on other parts of the human body (Fischer 1986; Neumann et al. 1997; Pickering et al. 2001).
Mean and standard deviation of pain threshold and tolerance at the stumps (eight subjects).

MPT: mid-patellar tendon; MSF: mid-shaft of fibula; TT: tibial tuberosity; PM: popliteal muscle; FH: fibular head; ALT: anterolateral tibia; MTC: mid-tibial crest; DT: distal end of tibia; MTF: medial tibial flare; DF: distal end of fibula; AMT: anteromedial tibia.
The fact that the mid-patellar tendon and the medial tibial flare had a better ability to tolerate pressure, while the distal end of the fibula had the least ability, is consistent with the qualitative description of Radcliffe and Foort (1961). The design of the PTB socket has undercuts at the mid-patellar tendon and medial tibial flare regions and relief at the distal end. Results also showed that some bony portions of the stump such as the tibial tuberosity, fibular head, and mid-tibial crest on average tolerated a higher pressure than some areas with softer tissues, such as the anteromedial and anterolateral tibia, mid-shank of fibula and popliteal muscle. It appears contrary to common belief that skin-thin regions and soft-tissue regions are pressure-sensitive and pressure-tolerant regions, respectively (Bowker and Michael 1992; Radcliffe and Foort 1961). However, it does not contradict the conceptual design of the PTB prosthetic socket. Socket rectification is described in terms of displacement; for example, 25 mm is usually suggested for the undercut at the patellar tendon region. Since the mechanical properties of the bony regions with a thin layer of soft tissue are much stiffer than the fleshy regions covered with thicker soft tissue (Silver-Thorn 1999), for a given magnitude of displacement, the stress produced in skin-thin regions would be greater than the fleshy regions. In other words, fleshy regions could tolerate displacement more than skin-thin regions without pressure significantly shooting up. It is the principle of the PTB socket to allow more deformation applied at regions with softer tissues.
Figure 2 shows the average pain threshold and tolerance of the six weight-bearing regions under different walking steps. There was a trend of an increasing pain threshold and tolerance as the number of walking steps increased. Pain threshold and tolerance at 2000 steps reached on average 13.4% higher than the values recorded before the walking trials. Statistical analysis reveals significant differences in pain threshold and tolerance between the ‘before walking trial’ and the ‘2000 steps’ (P < 0.05). Reliability test results demonstrated a good repeatability of the pain measurement method as, on repeated measurements of pain threshold and tolerance, the ICC reached 0.94 and 0.84 for pain threshold and tolerance level, respectively.
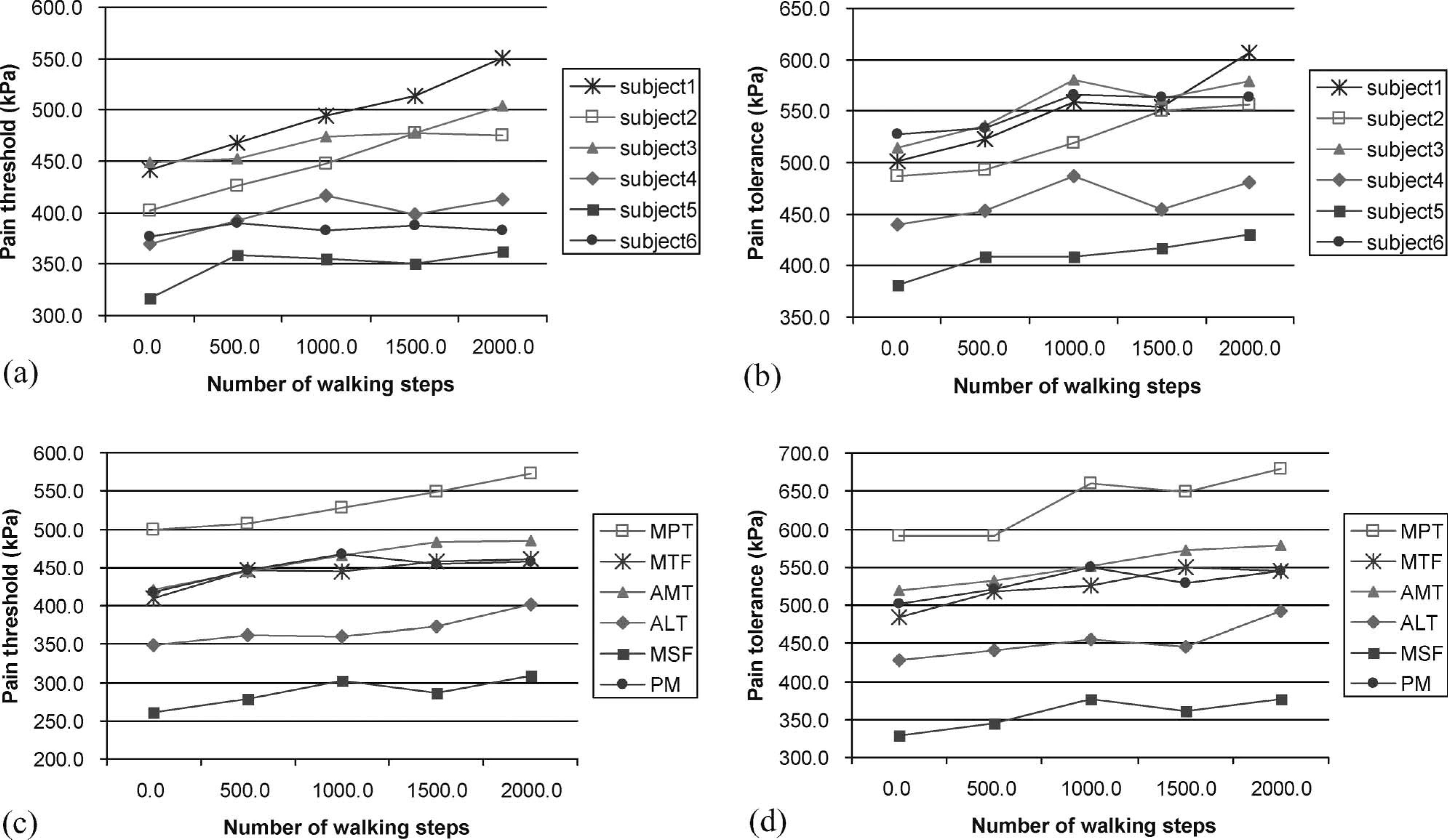
Relationship between the number of walking steps and pain threshold/tolerance, with (a, b) the average of the six subjects for the six test sites (c, d) the average of the six test sites for the six subjects.
The increase in pressure-tolerant ability can be explained by the massage-like effect when the prosthetic socket repeatedly applies pressure onto the stump during walking. Previous studies showed that massage aids venous return, relaxes musculature and relieves tension throughout the body, which helps relieve pain (Kingdon et al. 1998). The potential pain-relief ability, gentle tapping to the distal end, and massage over the stump have been therapeutic interventions in amputees with stump pain. A recent finding also shows that exercise causes secretion of endorphins, which may reduce pain (Koseoglu et al. 2003).
Some previous investigations (Neumann 2001; Persson and Liedberg 1982; Renstrom 1981) suggested that the weight-bearing ability of the stump increases with years of experience of prosthetic use. In this case, the increase in pain-tolerant capability with years of experience can be explained by the increased toughness of soft tissue and strengthening of the muscle (Hornby and Harris 1975; Persson and Liedberg 1982) at the stump. As in the present experiment, the walking duration was short, on average less than 30 min to finish the 2000 steps, this was unlikely to change stiffness significantly in the stump during the experiment. It is believed that the massage-like effect plays a role in raising the pain threshold and tolerance.
Table III summarizes the results of the percentage of the distal-end load tolerance to the body weight. The average of all measurement value was 48.6 ± 29.0%. There are some differences in the distal-end weight-bearing ability among the interface materials; the statistical analysis did not show any significant differences among the materials used. There was a great difference in distal-end weight-bearing ability among the subjects as the mean weight-bearing ability ranged from 7.2 ± 2.3% to 106.9 ± 9.6%, as shown in Table III. The great variations in distal-end weight-bearing ability among subjects was consistent with previous findings (Persson and Liedberg 1982) using a similar method with bathroom scales.
Distal end weight bearing ability (maximum tolerable force divided by the body weight) with the different interface materials (five subjects).

Conclusion
Understanding the pain – pressure relationship of the stump is an important step to achieve non-pain prosthetic socket fit. Experiments carried out in this study revealed that the load-tolerant ability varies significantly with regions and subjects, and walking steps influence the ability. The difference in distal-end load bearing ability was small among the different interface materials. Although the number of subjects involved in the three studies is small, these provide a great insight into the pressure-tolerant ability of different regions of the stump under different conditions. Further studies with a larger number of subjects of different characteristics such as amputation reason, soft-tissue stiffness, gender, and age, are suggested to generate a database of stump pressure-tolerant ability. Accumulated knowledge on load-tolerant ability associated with computational modelling of interface pressure distribution can one day be a powerful tool for optimized socket design.
Footnotes
Acknowledgements
The work described in this paper was supported by The Hong Kong Polytechnic University Research Studentship and a grant from the Research Grant Council of Hong Kong (Project No. PolyU 5200/02E).