
Abstract
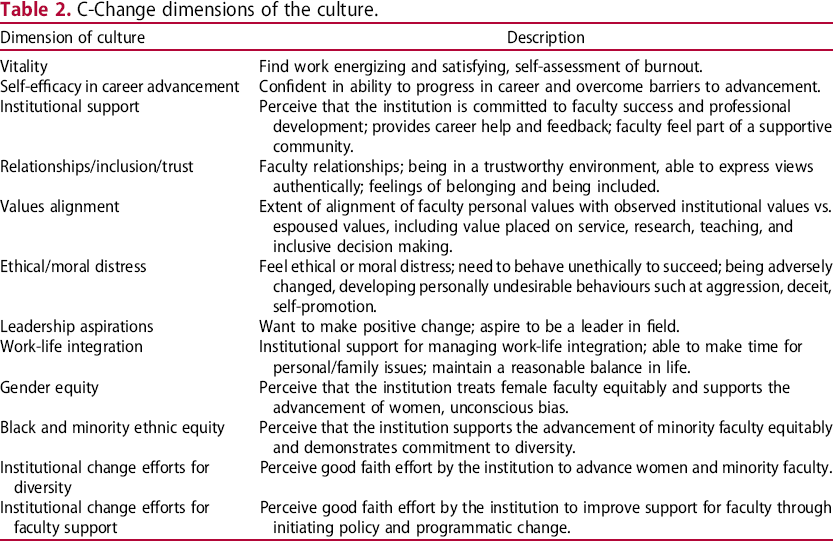
Results of two C-Change surveys of 4997 faculty and staff in medical and social sciences are analysed quantitatively and qualitatively and presented with illustrative quotations giving voice to critical personal perceptions of the culture and efforts to improve it. The C-Change survey included 12 dimensions of the culture: Vitality; Self-Efficacy in Career Advancement; Institutional Support; Relationships/Inclusion/Trust; Values Alignment; Ethical/Moral Distress; Leadership Aspirations; Work-Life Integration; Gender Equity; Black and Minority Ethnic Equity; Institutional Change Efforts for Diversity; Institutional Change Efforts for Faculty Support. Women were less positive than men on six dimensions in medical and ten dimensions in social sciences, suggesting that women's experiences are different to those of men. Both women and men were more positive about the culture in medical than social sciences. A more positive culture in medical sciences is attributed to the wide-spread implementation of Athena SWAN gender equality action plans linked to the NIHR funding incentives.
Introduction
The ground-breaking report by the United States’ National Academies ‘Beyond Biases and Barriers: Fulfilling the Potential of Women in Academic Science and Engineering’ poignantly identified the importance of organizational culture for women's advancement and leadership in academic and research organizations:
In most organizations in which women's advancement and leadership opportunities have been limited, the problem is not old-style, overt sex discrimination, but rather unrecognized features of the organizational culture that affect men and women differently. Those features tend to be so embedded in organizational life as to be invisible. They generally also bear no obvious relationship to gender. The only indication that such issues exist may be an unexplained inability of the organization to attract, retain, or promote women in sufficient numbers despite an apparent willingness to do so. (Committee on Maximizing the Potential of Women in Academic Science and Engineering 2007). Truth Descending on the Arts and Sciences to Expel Ignorance from the University. Ceiling fresco centrepiece, Sheldonian Theatre, University of Oxford, by Robert Streater, 1670. Credit: DeFacto (2017).
In what follows, we report and discuss the results of our interdisciplinary comparative study into the culture of medical and social sciences at the University of Oxford, United Kingdom, with a view to understanding how to accelerate women's advancement and leadership while creating a more supportive and inclusive university culture for all faculty and staff.
Methods
Study setting
Ten key principles of the Athena SWAN Charter (Advance HE).
Athena SWAN was established in the UK in 2005 to advance careers of women in science. In 2015, it was expanded to include arts, humanities, and social sciences, staff in administrative and other professional and support roles, and also to address gender equality more broadly, taking into account considerations of intersectionality (Advance HE). Athena SWAN is also adopted in Ireland (Science Foundation Ireland n.d.), Australia (Science in Australia Gender Equity n.d.), the United States (American Association for the Advancement of Science n.d.), and Canada (Natural Sciences and Engineering Research Council of Canada n.d.). The European Commission is actively promoting gender equality as one of the five pillars of responsible research and innovation (Colizzi et al. 2019) and currently exploring scenarios for the introduction of a gender equality scheme similar to Athena SWAN in the wider European Research Area (European Commission 2018).
In 2011, the National Institute for Health Research (NIHR) introduced a policy linking its biomedical research funding to the demonstrable commitment of institutions to gender equality through Athena SWAN awards (Ovseiko et al. 2017). The UK government Department of Health stated that in the 2016 competition for the NIHR biomedical research funding it did not expect to shortlist any academic institution that had not achieved at least the Silver award of Athena SWAN (Ovseiko et al. 2017; Kalpazidou Schmidt et al. 2019). When this study was conducted in 2014, all of the medical sciences departments and none of social sciences departments or Oxford colleges had been developing and implementing Athena SWAN gender equality action plans to achieve Athena SWAN awards.
Study population
The study populations were all (N = 4997) academic and research as well as administrative and other professional and support staff at grades 6 and over in the Medical Sciences Division and its 16 constituent departments (N = 3824) and in the Social Sciences Division and its 16 constituent departments (N = 1173).
The medical sciences departments included the following disciplines: Biochemistry; Clinical Medicine; Clinical Neurosciences; Experimental Psychology; Medicine; Obstetrics and Gynaecology; Oncology; Orthopaedics, Rheumatology and Musculoskeletal Sciences; Paediatrics; Pathology; Pharmacology; Physiology, Anatomy and Genetics; Population Health; Primary Care Health Sciences; Psychiatry; and Surgical Sciences.
The social sciences departments included the following disciplines: Anthropology and Museum Ethnography; Archaeology; Business School; Economics; Education; Geography and the Environment; Government; Interdisciplinary Area Studies; International Development; Internet Institute; Law; Martin School; Politics and International Relations; Quantitative Finance; Social Policy and Intervention; and Sociology.
C-Change survey
To facilitate an interdisciplinary comparative approach, we used the internationally validated C-Change Faculty Survey instrument with adaptations to the context of medical and social sciences in the UK. A range of survey instruments was discussed at the expert international workshop ‘Accelerating women's advancement and leadership in academic medicine’ (Wadham College Oxford 2014) to create an evidence base and to formulate an agenda for future research and action (Edmunds et al. 2016; Ovseiko, Edmunds, et al. 2016; Ovseiko, Greenhalgh, et al. 2016; Kuhlmann et al. 2017). The C-Change instrument was chosen by the workshop participants, with input from Professor Dame Sally Davies, Chief Medical Officer and then Chief Scientific Adviser at the Department of Health, by consensus.
The C-Change Faculty Survey was developed and validated in United States medical school faculty members by the National Initiative on Gender, Culture and Leadership in Medicine: C-Change at Brandeis University. The domains and items of the survey questions were derived in large part from themes identified in previous C-Change qualitative studies (Carr et al. 2009; Pololi, Conrad, et al. 2009; Pololi, Kern, et al. 2009; Conrad et al. 2010; Pololi and Jones 2010; Pololi, Cooper, and Carr 2010) in conjunction with a literature search and reviews of relevant instruments (Butler 1991; Pololi and Price 2000; Pololi et al. 2003; Schindler et al. 2006). Detailed descriptions of the C-Change survey study methods have been published elsewhere (Pololi et al. 2012).
C-Change dimensions of the culture.
Data collection and analysis
The study was supported by the University of Oxford Vice-Chancellor's Diversity Fund and received ethics clearance through the Brandeis and Oxford university ethics committees. The surveys were administered anonymously by C-Change online. All individuals in the study population received an e-mail with a link to the electronic survey with a participant information sheet and informed consent form, which the respondent was required to fill in before being able to access the survey. Non-respondents received twice-weekly reminders over the six-week fielding period in medical sciences and a five-week fielding period in social sciences.
Given that the university culture is an organizational-level construct, university members share similar assumptions, beliefs, values, norms, rules, and practices, which nevertheless may vary across different sciences and organizational units. To maximize the generalizability and impact of our research at the university level, quantitative analysis focused on the same dimensions of the culture across sciences, and qualitative analysis focussed on the critical perceptions of the culture that are shared across sciences. Unlike quantitative analysis, identifying variations and differences across sciences was beyond the scope of qualitative analysis.
The quantitative responses were summed and scores divided by the number of items in each scale. Cronbach's α reliability coefficients were estimated to assess the reliability of each scale. Independent-sample t-tests were calculated to determine whether differences in responses between sciences and subgroups of respondents were statistically significant with the significance level set at p < .001. The open-ended responses were analysed using a three-stage thematic framework approach (Ritchie and Lewis 2003). Researchers were sensitized by the C-Change dimensions of the culture and reflected on their own prior views and experiences, which might have influenced the analysis. The most informative quotations were selected to highlight the critical perceptions of the culture across sciences.
Results
Quantitative results
Respondent profile
Professional and socio-demographic characteristics of the study population and respondents to the C-Change surveys in medical and social sciences.
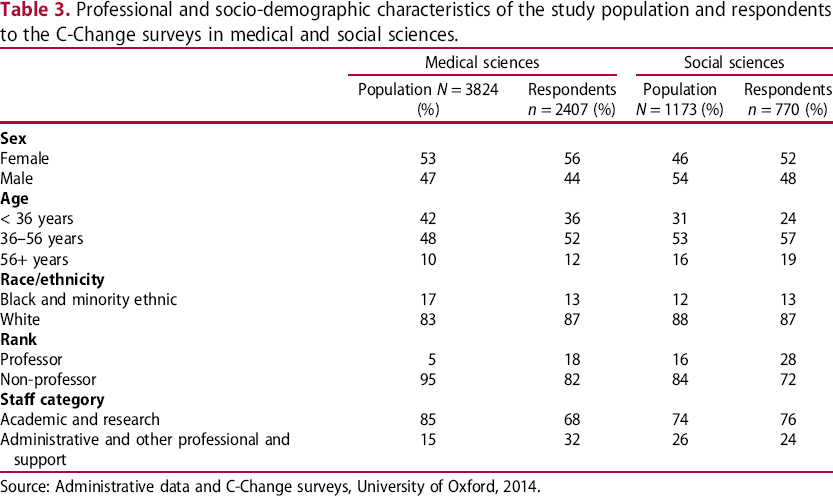
Source: Administrative data and C-Change surveys, University of Oxford, 2014.
Despite the sufficient response rates, a possibility of non-response bias cannot be ruled out due to notable socio-demographic differences between respondents and non-respondents. In medical sciences, the survey sample was characterized by a lower proportion of younger respondents, a higher proportion of senior faculty with professorial titles, and a higher proportion of administrative staff than the study population. In social sciences, the survey sample had a lower proportion of younger respondents, a higher proportion of women, and a higher proportion of senior faculty with professorial titles than the study population.
There were also other important differences between respondents in medical and social sciences with regard to three self-reported employment-related characteristics, for which we could not account in the study population. A greater percentage of respondents, including both women and men, in social than medical sciences had a permanent contract of employment associated with job security, a formal leadership role associated with a higher status, and an Oxford college affiliation associated with in-kind privileges and monetary benefits; compared to their male counterparts, women were disadvantaged in all of these three employment-related characteristics consistently across sciences (Figure 2).
Employment-related characteristics of respondents by gender.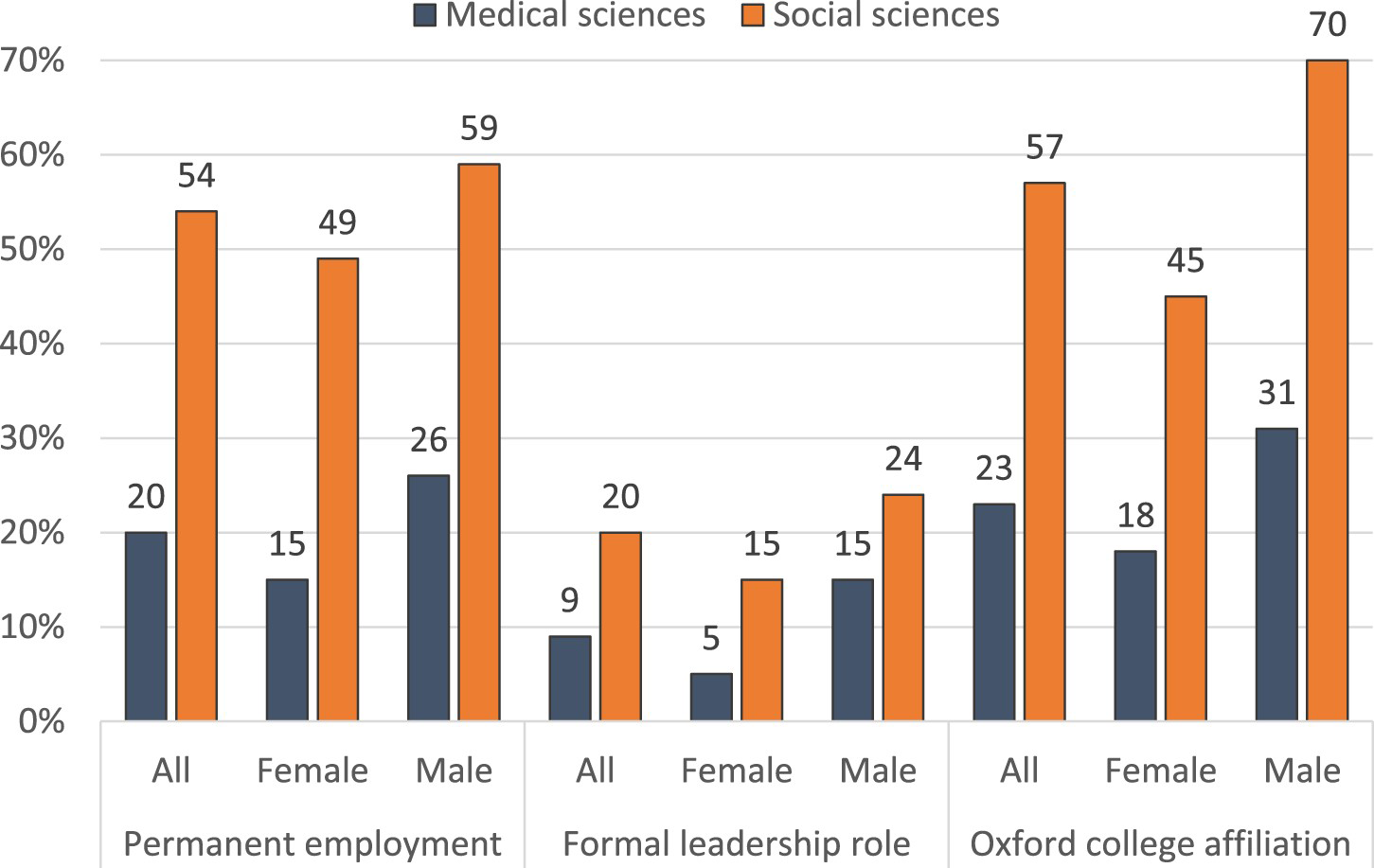
Reliability of the C-Change dimensions of the culture
C-Change dimensions of the culture with the means for male (M), female (F), and aggregated male and female respondents (M + F), Cronbach's α reliability coefficients, and the independent-sample t-test results for statistically significant differences with p-values <.001 in medical and social sciences, University of Oxford, 2014.
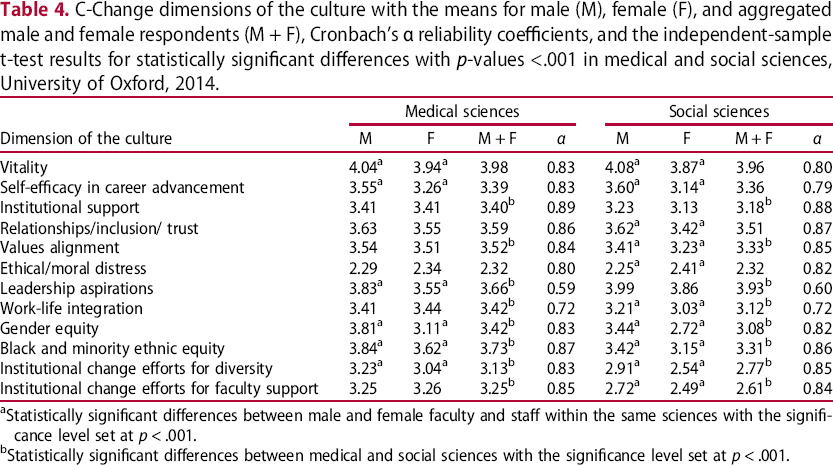
aStatistically significant differences between male and female faculty and staff within the same sciences with the significance level set at p < .001.
bStatistically significant differences between medical and social sciences with the significance level set at p < .001.
Gender disparities in the experiences of the culture
There were statistically significant (p < .001) differences in the perceptions of the culture by women and men (Table 4). Women reported experiencing a less positive culture on six dimensions in medical sciences and ten dimensions in social sciences. Across both sciences, more women than men found work less energizing and personally satisfying; felt less confident in their ability to progress in career and overcome barriers; were less convinced that the university treats women equitably and supports the advancement of black and minority ethnic faculty and staff equitably. The highest levels of disparity in the perceptions of the university culture between women and men across both sciences were with regard to gender equity and self-efficacy in career advancement. In medical sciences, women reported lower leadership aspirations than men, however this unusual finding may be explained by the heterogeneous respondent pool. Women and men in medical sciences reported similar perceptions of institutional support for work-life integration and institutional change efforts for faculty support. Notably, these were the only two dimensions of the culture where women reported slightly more positive (but not statistically significant at p < .001) perceptions than men. In social sciences, women as compared with men experienced less positive relationships and feelings of belonging, inclusion, and trust; they felt a lesser degree of alignment between personal and institutional values; felt more ethical or moral distress; and were particularly less convinced about institutional change efforts to advance women and minority faculty and staff.
Experiences of the culture across sciences
The interdisciplinary comparative analysis of the C-Change dimensions of the culture in medical and social sciences is visually represented on the radar plot in Figure 3. It reveals a number of important points of convergence and divergence in how faculty and staff experience organizational culture in medical and social sciences. The perceptions of organizational culture converge on four dimensions. On the whole, faculty and staff in medical and social sciences find work energizing and personally satisfying; experience relationships and feelings of belonging, inclusion, and trust; feel confident in their ability to progress in career and overcome barriers; and do not feel ethical or moral distress to a similarly high level.
C-Change dimensions of the culture with the means for aggregated male and female respondents, and the independent-sample t-test results for statistically significant differences with p-values < .001 in medical and social sciences.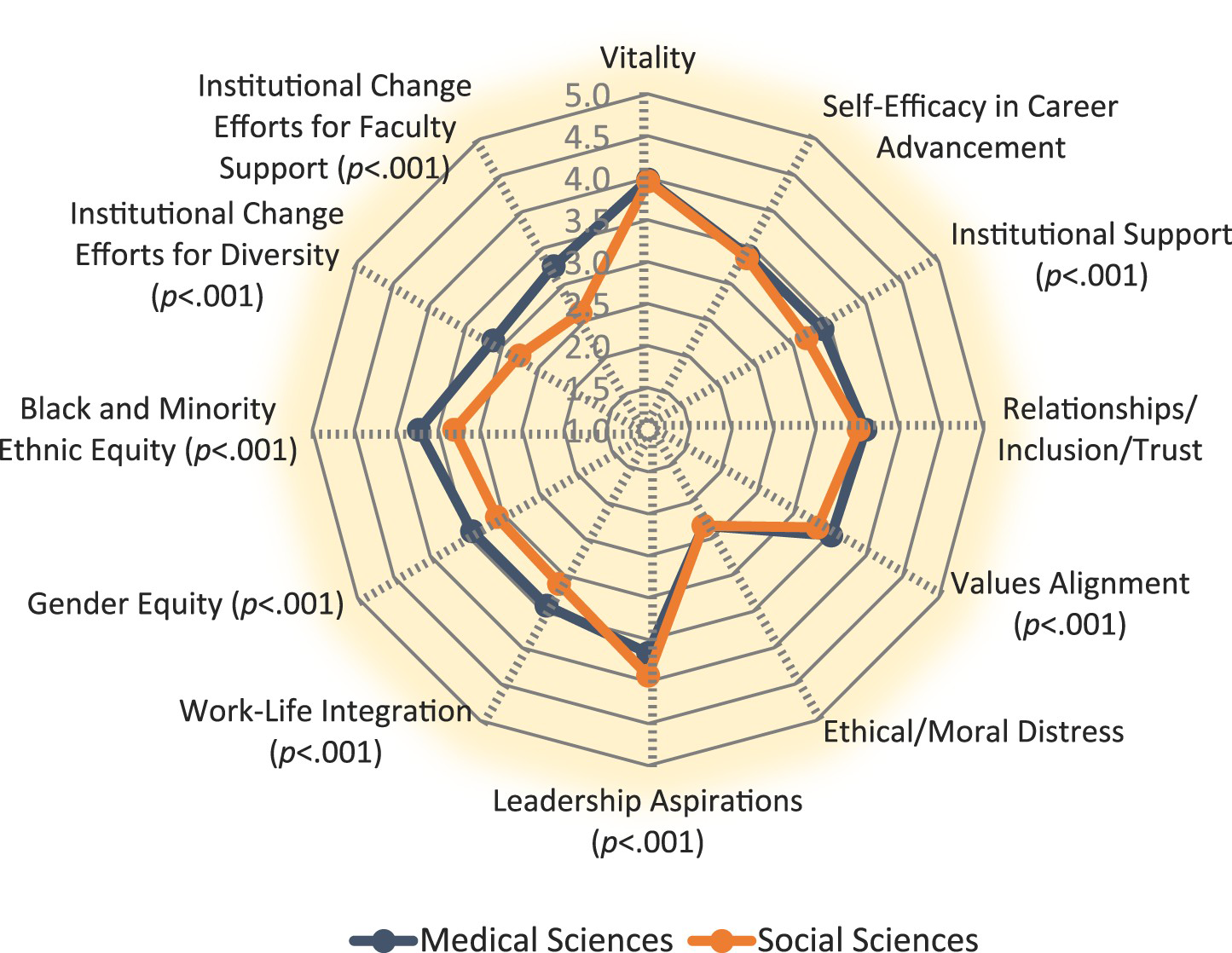
Respondents’ perceptions of organizational culture diverged on eight dimensions of the culture, with medical sciences scoring higher on seven dimensions and social sciences on one dimension. The greatest areas of divergence between medical and social sciences were in the perception of the institutional change efforts for faculty support and diversity; black and minority ethnic equity; and gender equity. Respondents in medical sciences perceived good faith institutional effort to improve support for all faculty and staff and to advance women and minorities to a significantly higher degree than respondents in social sciences. Respondents in medical sciences also felt institutional commitment to faculty and staff success as well as alignment between personal and institutional values to a higher degree than respondents in social sciences. Yet, respondents in social sciences had higher leadership aspirations than respondents in medical sciences.
Mentoring received by faculty and staff
The interdisciplinary comparative analysis of the adequacy of mentoring received by faculty and staff in medical and social sciences is visually represented on the stacked bar chart in Figure 4. It reveals that only 26% of faculty and staff in medical sciences reported positive experiences of mentoring associated with receiving both high quality and a satisfactory amount of mentoring, but it was significantly (p < .001) higher than in social sciences (22%). There were important subgroup differences and similarities within and across sciences. While there was no statistically significant gender difference (p < .001) in positive experiences of mentoring received in medical sciences, a significantly lower proportion of women reported positive experiences of mentoring received in social sciences. A significantly (p < .001) higher proportion of black and minority ethnic than white faculty and staff reported positive experiences of mentoring received across both sciences. Likewise, a significantly (p < .001) higher proportion of academic and research staff reported positive experiences of mentoring received than administrative and other professional and support staff across both sciences.
Adequacy of mentoring received by gender, race/ethnicity, and staff category subgroups of faculty and staff in medical and social sciences. Source: C-Change surveys, University of Oxford, 2014. Positive experience of mentoring includes faculty who reported receiving both high quality and a satisfactory amount of mentoring; neutral includes faculty and staff who did not desire a mentor and those who received mentoring but of unsatisfactory amount or quality; inadequate includes faculty and staff who wanted a mentor but none was available and those who received mentoring but of unsatisfactory amount and quality.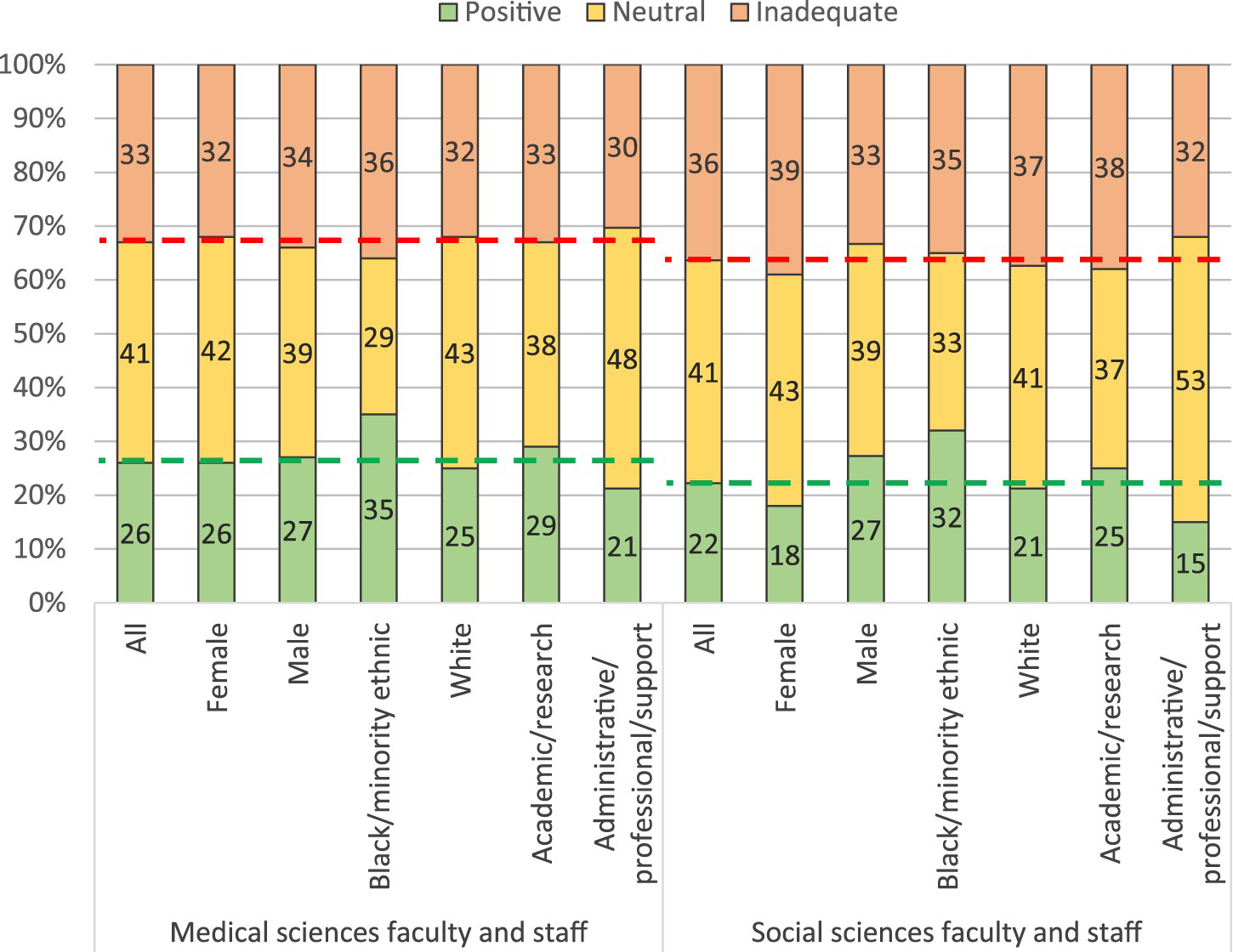
Intention to leave the university by faculty and staff
The interdisciplinary comparative analysis of the reasons associated with the intention to leave the university by faculty and staff in medical and social sciences is visually represented on the stacked bar chart in Figure 5. Faculty and staff who responded ‘agree’ or ‘strongly agree’ to the question, ‘In the last 12 months I have seriously considered leaving my current university’, were asked to indicate whether they were considering leaving the university due to dissatisfaction, personal/family reasons, or other reasons. A high proportion of faculty and staff in medical sciences (23%) reported the intention to leave the university due to dissatisfaction, but it was significantly (p < .001) lower than in social sciences (27%). There were also important differences within subgroups. A significantly (p < .001) higher proportion of women than men in both medical and social sciences, administrative and other professional and support staff than academic and research faculty and staff in medical sciences, and black and minority ethic faculty and staff than white faculty and staff in social sciences reported the intention to leave the university due to dissatisfaction.
Reasons associated with the intention to leave the university by gender, race/ethnicity, and staff category subgroups of faculty and staff in medical and social sciences.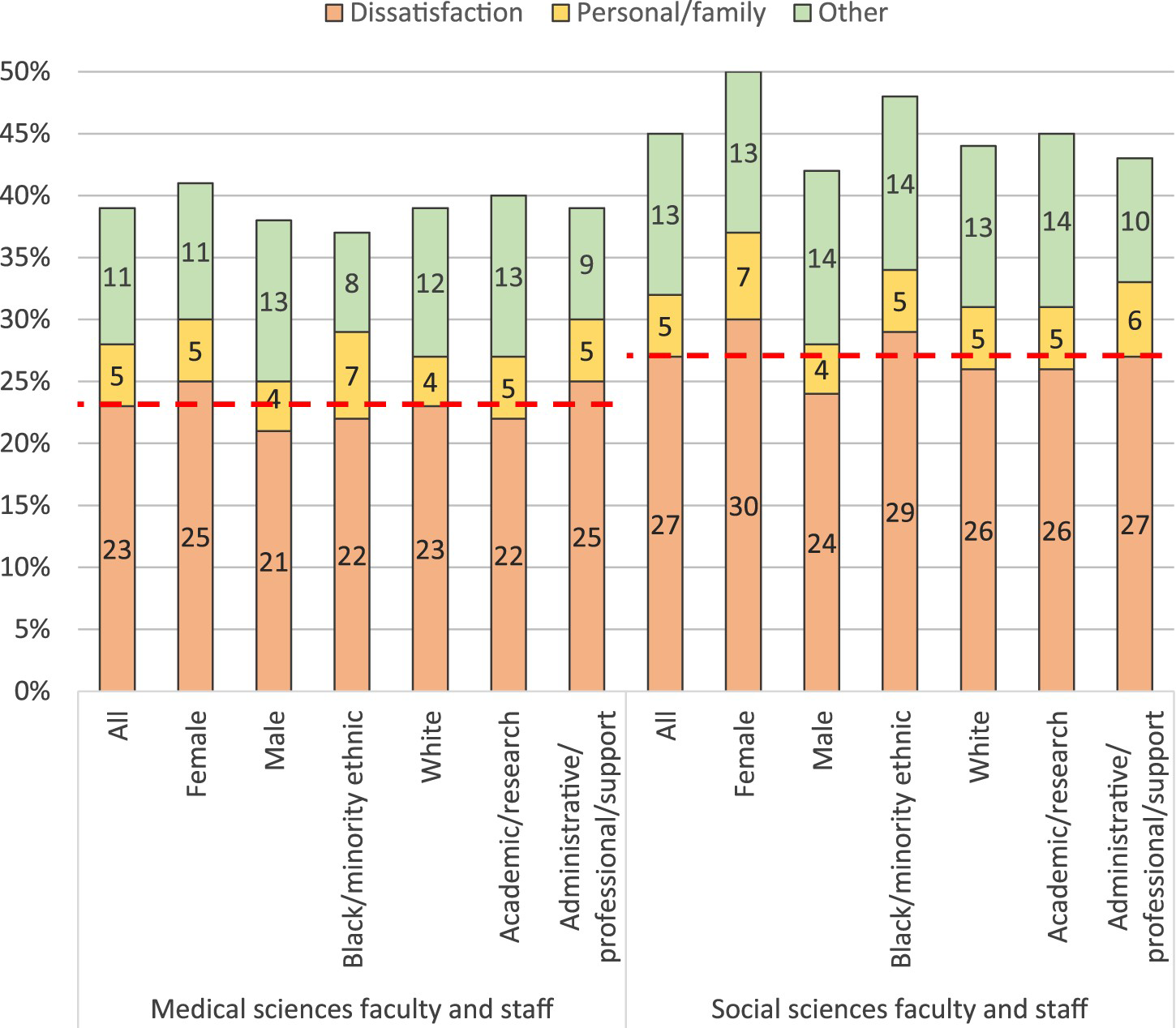
Qualitative results
In total, of 2407 respondents to the survey in medical and 770 respondents in social sciences, 523 (22%) respondents in medical and 243 (32%) respondents in social sciences provided open-ended comments. Below, we provide a range of thematically-grouped insights into the gaps between the current perceived culture and the ideal university culture together with illustrative quotations reflecting the assumptions, beliefs, values, norms, rules, and practices associated with the university culture. Illustrative quotations give voice to the critical personal perceptions and reflections by a non-statistically representative sample of the respondents who would appreciate a more supportive and inclusive culture. Illustrative quotations are presented with the respondent's socio-demographic characteristics corresponding to sex (female = F, male = M), race and ethnicity (white = W, black and minority ethic = BME), staff category (academic and research = ACAD, administrative and other professional and support = ADMIN), and the area of sciences (medical sciences = MED, social sciences = SOC); X = prefer not to say.
Gender bias
Concurring with the quantitative evidence that women experience gender equity and self-efficacy in career advancement to a significantly lesser extent than men, the majority of open-ended comments on gender equity, diversity, and inclusion came from women. A number of respondents provided instances of how perceived gender bias still manifested itself throughout the whole continuum of women's careers, from recruitment to tenure and promotion. Gender bias was implied to affect the disposition to employ women of child-bearing age at the outset:
I am not aware of a colleague being treated unfairly, but I have heard a colleague refer to employing a woman for a postdoc post who was 30 something as ‘a bit risky, she's likely to bugger off and pop some sprogs out’. (F, W, ACAD, SOC) I was recruited as a professor with a permanent position. I have also seen my wife's development … She routinely hears from admin staff that what she is asking is ‘not their job’ … I have never been told this. So, I think, male and female staff are less likely to be helpful to a female professor. (M, W, ACAD, MED) I know of more than one woman who has been told by the head of her faculty that she will need to satisfy criteria not satisfied by others if she is to be awarded the professorial title. It is impossible to say whether this is gender-based discrimination, or whether the gender of the people is a coincidence. (F, W, ACAD, SOC) Sometimes, when I (female) explain an idea, it does not create any reaction, but when a male coworker repeats it, then it is praised. This is probably unconscious, however it is highly demotivating and unsettling. (F, W, ACAD, MED) Women's approach to social science tends to be dismissed as ‘that feminism’, where other disciplines that are equally opaque to outsiders are given a free pass. (M, W, ACAD, SOC) My supervisor insisted I stopped teaching ‘because it is against his philosophy’, even though I was never doing it during the work day … all that matters here to advance in career as an academic is one's publication list. (F, W, ACAD, MED) I feel undervalued in my division and university and as if teaching and administration do not ‘count’ towards promotion or anything else. (F, W, ACAD, SOC) Women are still very poorly represented amongst those who actually make the decisions in Oxford. (F, W, ACAD, MED) Institutional knowledge and power is not shared equally and breaks down along gendered lines. We lack a culture of inclusivity, consultation and peer support in our department. (F, W, ACAD, SOC) If you aren't an ‘alpha-male’ (regardless of gender) who wants to be in charge and run everything, but rather value collaborative working, then you have no value. (F, W, ADMIN, MED) I have actually heard senior professors suggest that a good way to run a research group is to set up rivalries between postdocs, PhD students, etc. because it ‘encourages productivity’. This might not be untrue but it doesn't make for a particularly happy, collaborative working environment. (F, W, ACAD, SOC) I think women also do themselves a disservice. Women focus much more on completing tasks and are less good at the self-promotion that is sometimes required to ensure that their opinions and contributions to strategic thinking are listened to. (F, W, ADMIN, SOC) Promotion is not transparent and vehemently self-promoting individuals are given titles without going through the usual process because they have power and/or threaten to leave the university. (F, W, ACAD, SOC) These problems are structural and not exclusive to Oxford. However, it is clear that the only way to progress at Oxford is either a) get a job elsewhere in order to return with more senior experience; or b) get the offer of a job elsewhere (or secure a significant grant), and then use that as a bargaining chip to negotiate for better terms and conditions. Staying and waiting for better terms and conditions to be offered gets you nowhere. (M, W, ACAD, SOC) The university pays me half of what it pays my husband and would not support my quest to have a UK entry visa separate from my husband – although I am a professor, I am in England on a ‘dependant’ visa. I am aware of many women here who are paid significantly less than men for the same responsibilities. (F, W, ACAD, MED).
Inclusion of academic-related and research staff
Several academic-related and research staff on fixed-term contracts reported feelings of job insecurity, isolation, perceived limited support and career development opportunities, as well as intentions to leave the university. They talked about academic faculty on permanent contracts with college fellowships as ‘them’ – ‘the university’ and ‘us’ – ‘contract staff’:
I have worked in the Medical Sciences Division for over 20 years on a series of fixed-term contracts … I have never been offered a full-time contract by the University and have never been asked to become affiliated to a college. I feel that I have contributed to the reputation of the University, but have had little recognition of my efforts on their behalf … In the last year, I have been close to redundancy on several occasions, only to be reprieved by another short-term contract for three to six months. This has been extremely stressful for myself and my colleagues and I have decided to take early retirement as I do not feel that I want to continue with this situation. (M, W, ACAD, MED) I am hindered greatly by my contractual status which has low job security and prevents me from developing my research programme (I cannot be PI because my role is externally funded … One colleague put it ‘ Don't take it personally. The university has to protect itself from contract staff. I'll be PI, you get the money … and you get to do all the work … ’) (F, W, ACAD, SOC) In part, my experience is consistent with academic practice in many universities – perhaps exaggerated in Oxford due to the department/college system. I would be happy to put up with nearly all the problems if I was able to pursue my research agenda – that is, if I could own my ideas in research projects I have developed, rather than having to hand them over to a PI who is permanent member of the faculty. (F, W, ACAD, SOC) The university completely undervalues research staff and has no equivalent to staff scientist … These people (who teach, supervise, write papers, grants, do experiments, etc.) are essential for the success of units and departments and should be nurtured and promoted rather than always only relying on high fliers coming in and out of the departments. (F, W, ACAD, MED) I have come to realise that you only receive a [college junior research fellowship] if you know someone in the college. As with many things at Oxford University, it is who you know not what you know that counts. (F, W, ACAD, MED) I was asked to teach my area of special interest for very little money, and more importantly, without formal affiliation to the department. (F, W, ACAD, SOC)
Inclusion of administrative and other professional and support staff
Many administrative and other professional and support staff felt a division between themselves and academics, perceived poorly-trained leadership, and reported receiving variable treatment:
There appears to be a gulf between academic/faculty and administrative staff even at senior level. It is made very apparent that the opinion of administrative staff will only ever be subsidiary to that of academic staff whether or not the administrative staff are the experts in that area. (F, W, ADMIN, MED) University consistently appoints academics and others to leadership positions who have little skills in this area, and are not apparently required to undertake any training to improve their skills … Academic arrogance is abundant, leading to incredibly poor relationship management. (M, X, ADMIN, SOC) The support shown by academics towards administrative staff is extremely variable from very supportive, understanding and grateful through to bullying, rude and oppressive and all that is in between. There is an unfortunate culture of needing to ‘cover one's own back’ in the department, rather than working as a whole unit. (F, W, ADMIN, SOC) Oxford has a fantastic wealth of non-medically trained administrative support staff that oversee/run their large scale studies, however, there is absolutely no consideration given to their development. Administration with research trials covers a multiplicity of skills and roles and yet we appear to suffer the same stigma ‘secretarial work’ conjured up in the 1960s. (F, W, ADMIN, MED) I have been here for 14 years and have not yet had any review of my pathway. We seem to be bombarded with work/expectations with no review as to how this will be dealt with and, when small issues do not go to plan, it is a big deal for the academics in their ‘ivory towers’. To me it seems that administration staff are seen as the poor relations. (F, W, ADMIN, SOC) [Mentoring] exists in theory for all university staff, but our centre within the university does not offer support or improvement/growth unless for an academic member of staff … we are ignored. (F, BME, ADMIN, SOC)
Work-life integration
Work-life integration was seen to be hard to achieve, with the ‘need to excel’, ‘long hours culture’, and ‘sacrificing most weekends, evenings and holidays’, impacting women's career advancement disproportionally:
Sexism takes many forms, and the culture of overwork, superperformance, rampant individualism weighs more heavily on women than men. (F, W, ACAD, SOC) I'm having a very difficult time negotiating my current workload. I am working without a proper job description and without proper supervision … My physical and mental health have deteriorated rapidly over the past 6 months. I experienced my first episodes of tachycardia and panic attacks at work. (F, W, ACAD, MED). Following maternity leave, I was told by an associate head of department that having one child was a career mistake but that if I chose to have any more it would be career death. He himself had [many] children. (F, W, ACAD, MED) Being a mother and senior female has its challenges but direct colleagues are open and understanding. Although I do feel at times that I am the only one without a housewife. (F, W, ACAD, SOC) I am in my late fifties and care for my elderly mother. I think this has significantly hindered my development and progress of recent years in my contribution being undervalued. Mostly because of unhelpful attitudes towards part-time workers. (F, W, ADMIN, MED) The University as a whole still feels to me stuck in a time warp and full of old men, with college traditions fitting to Harry Potter but not reflecting society today – who prays? who prays in LATIN before dinner? … The colleges need to be far less elitist and not just the logical next step for posh boys from Eton who feel at home with all the pomp. (F, W, ADMIN, MED) I am a fellow at one of the university colleges, but find that the college makes very little effort to adapt its practices to enable a female, from a minority and with childcare responsibilities, like myself, to take an active part in college life. (F, BME, ACAD, MED)
Intersectionality of gender and minority identities
Several respondents pointed towards the intersectionality of gender and other aspects of identity, highlighting a perceived lack of racial and ethnic diversity among faculty and staff:
While I notice posters and emails about advocating diversity and promotions of minorities into higher positions, I don't actually see anyone of those origins (within my department) in those high positions. It feels like a lot of talk, but not enough action. (F, BME, ADMIN, MED) While we seem to have a diverse profile of academics in some areas these are highly privileged overseas academics and not working class [black and minority ethnic] people and although less visible this university is utterly dominated by the upper and middle classes. (F, W, ACAD, MED) I came to Oxford after 5 years teaching at an Irish University. I felt I had stepped back in time. I was toasted as the ‘first woman’ to tutor [subject] in my first college, and reminded that Oxford students would be unlike anything I had encountered before … Gender was always to the forefront, including amongst students, many of whom have attended single-sex [private] schools, and have deeply engrained gendered expectations. (F, W, ACAD, ADMIN) A senior member of the Faculty is often heard to remark amusingly on his ‘nanny’ when his children were young, assuming that all members of the Faculty have a wealthy 1950s arrangement … Have I felt excluded because I have a regional accent and grew up on a council estate and seem different to the usual Oxford don? I certainly have. (M, W, ACAD, SOC) I'm a foreigner and I think that helps to communicate across the class system in UK. (F, BME, ACAD, MED) I think the university can do more to challenge the perception that it is an exclusive club. Reviewing its admissions requirements for students from this sector is important. Thinking about how its rituals and history might serve to alienate students from more diverse backgrounds. Thinking about the forms of representation at the higher echelons important in terms of its wider public perceptions, this is especially true of class. (M, BME, ACAD, SOC) I am bisexual and bigender – this is not something I feel comfortable being open about in my working life. I feel it would be a hindrance to me. (X, X, X, SOC) Few gay people are out at work – in my department of over 100 post-doctoral researchers/associates I am the only one: If gay people can't be open, if they can't talk about their weekends/holidays/partners, their quality of work and the research output of the University suffers. (M, W, ACAD, MED) I am gay, Asian, and have health issues. I find my race to be most pertinent to how I am perceived here, especially in a college system steeped in Anglican cultural assumptions. (M, BME, ACAD, SOC) Key members of my department are secularist who are anti people with religious views. I have been told by a professor that the reason he thinks only 10% of the genome is useful is: ‘There is no God’. This is not a robust scientific argument. (F, W, ACAD, MED)
Discussion
Summary
To the best of our knowledge, this is the first study that compares the culture in medical and social sciences in large populations at the university level using an internationally validated instrument. The results presented above focus on the quantitative analysis of 12 dimensions of the culture and the qualitative synthesis of open-ended responses from two C-Change surveys in medical and social sciences conducted in 2014 at the University of Oxford. Although we cannot rule out a possibility of non-response bias, the sufficient response rates indicate that survey respondents were sufficiently statistically representative of the study populations. The high levels of reliability for the C-Change dimensions of the culture validate the use of the C-Change survey instrument in the UK context. Qualitative synthesis provides thematically-grouped insights into the differences between the perceived culture and ideal university culture. Illustrative quotations give voice to the critical personal perceptions and reflections by a non-statistically representative sample of the respondents who would appreciate a more supportive and inclusive culture.
Key findings
University culture disadvantages women
First, we found that compared to their male counterparts, women reported less positive perspectives on six C-Change dimensions of the culture in medical sciences and ten dimensions in social sciences. The highest levels of gender disparity in the perceptions of the university culture across both sciences were on gender equity and self-efficacy in career advancement. Across both sciences, a significantly higher proportion of women than men reported intent to leave the university due to dissatisfaction.
These findings align with previous research in United States academic settings suggesting that women's experiences of the culture are different to those of men and that the dominant culture usually disadvantages women (Foster et al. 2000; Schroen, Brownstein, and Sheldon 2004; Kass, Souba, and Thorndyke 2006; Pololi et al. 2012). Similar to previous research, our qualitative research indicated that women often felt isolated and disconnected from their colleagues, were considerably interested in teaching, and that the current advancement criteria predominantly based as they are on individualism and competition in research were likely to disadvantage them (Kaplan et al. 1996; Schroen, Brownstein, and Sheldon 2004; Carr et al. 2009; Pololi et al. 2009).
Our qualitative research also provided novel insights into the factors contributing to the perceived isolation and exclusion of academic-related staff from collegiate and departmental life, divisions between academic faculty and administrative, professional and other support staff, and the importance of intersectional connections between gender, race/ethnicity, sexual orientation/gender identity, and socio-economic class.
More positive culture in medical sciences
Second, our results indicated that both women and men were more positive about the culture in medical as against social sciences. There were no statistically significant differences by gender in the perceptions of the university culture on six dimensions in medical sciences compared with two dimensions in social sciences. Notably, women and men in medical sciences reported similar perceptions of work-life integration and institutional change efforts for faculty support. A significantly higher proportion of faculty and staff in medical sciences than in social sciences reported positive mentoring experiences regardless of gender. It is also the case that a significantly lower proportion of faculty and staff in medical sciences as compared with social sciences intended to leave the university due to dissatisfaction.
These findings align with the empirical evidence from systematic reviews demonstrating that mentoring can enhance personal and career satisfaction, foster career development, and increase academic productivity, grants, and publications (Sambunjak, Straus, and Marusic 2006, 2010; Kashiwagi, Varkey, and Cook 2013). Importantly, our findings contribute to the growing body of literature showing that both women and men would benefit from a more supportive and inclusive culture (Pololi et al. 2009; Pololi et al. 2012; Sadeghpour et al. 2012; Westring et al. 2012; Krupat et al. 2013; Pololi et al. 2013) and that culture change efforts towards a more positive culture increase the likelihood of more women and men staying in academia (Sadeghpour et al. 2012).
Positive impact of Athena SWAN
Third, we attribute a more positive culture in medical sciences to the wide-spread implementation of Athena SWAN gender equality action plans linked to the NIHR funding incentives. Although we cannot claim the type of causality required in experimental medical sciences on the basis of our observational study using cross-sectional data and mixed-methods analysis, we can identify the most salient variable contributing to a more positive culture in medical sciences on the basis of the Most Similar Systems Design/Mill's Method of Difference comparison commonly used in comparative social inquiry (Przeworski and Teune 1970).
Namely, medical and social sciences at the given university are most similar in a large number of cultural variables. Medical and social sciences departments and divisions use the same recruitment, remuneration, promotion, and recognition of distinction rules and procedures; they are subject to the same university equality and diversity policies, workplace norms of behaviour, and UK equality laws; and the university is equally committed to fostering an inclusive culture in all sciences, arts, and humanities. The effects of more favourable socio-demographic characteristics in medical sciences (more female, minority, and younger faculty and staff) and more favourable employment-related characteristics in social sciences (more faculty and staff employed on permanent contracts and with college affiliations) are likely to cancel each other out.
The wide-spread development and implementation of Athena SWAN gender equality action plans linked to the NIHR funding incentives in medical sciences appears to be the most salient independent cultural variable. Previous qualitative research in the given setting showed that the linkage of the NIHR funding incentives in biomedical research to Athena SWAN awards prompted medical sciences departments to introduce important structural and cultural changes, including institutional change efforts to challenge discrimination and bias, increase faculty and staff support, develop new mentoring schemes, promote work-life balance, and greater appreciate the impact of caring responsibilities in career advancement (Ovseiko et al. 2017). Cross-sectional research in other UK settings also showed that the implementation of Athena SWAN action plans is associated with increased awareness of gender equality and diversity, efforts to challenge discrimination and bias, visibility of female role models, institutional support for women's careers, appreciation of work-life balance and caring responsibilities, and new mentoring and professional development opportunities for all faculty and staff (Munir et al. 2013; Bryant et al. 2017). Other research demonstrated the positive effects of Athena SWAN, while highlighting its limitations in addressing long-standing power and leadership disparities (Barnard 2017; Gregory-Smith 2018).
Therefore, we attribute a more positive, but far from ideal, culture in medical sciences to the wide-spread implementation of Athena SWAN gender equality action plans linked to the NIHR funding incentives.
Impact on policy and practice
Prior to current publication, the findings were disseminated internally through reports to the Medical Sciences and Social Sciences Divisions, provided evidence for culture change activities in medical sciences departments, and informed decisions in social sciences departments to join Athena SWAN. The findings were presented and discussed at five action-oriented workshops attended by over 300 faculty and staff, were used to instigate a debate in the university staff magazine, were included in internal teaching materials, and were highlighted in external outreach activities with diverse audiences in the UK and internationally.
Limitations and future research
Despite its strengths and impact on policy and practice, the current study has several noteworthy limitations. One, the study highlighted that respondents in some socio-demographic groups were over-represented and in some other under-represented, but did not investigate possible effects of non-response bias on the generalizability of the survey results to the study populations. Another, the study hypothesized how differences in socio-demographic characteristics of survey respondents and study populations across sciences might have influenced their perceptions of the university culture, but did not test this hypothesis empirically. Finally, theorizing the qualitative results using existing social science theories or developing grounded theory was beyond the scope of the current study. Future research might usefully address these limitations. There is an opportunity for future research to examine longitudinal changes in the university culture in the given setting by conducting a follow-up C-Change survey and evaluating impact of continued implementation of Athena SWAN.
Conclusions
Women compared with men experienced less positively six dimensions in medical and ten dimensions of the culture in social sciences, suggesting that women's experiences of the university culture are not only different to, but are less positive than those of men. Gender disparity in the perceptions of the university culture across both sciences with regard to gender equity and self-efficacy in career advancement suggests that institutional change efforts to increase gender equity and provide more support with career advancement to all faculty and staff must accelerate.
Further efforts would yield benefit by addressing the isolation and exclusion of academic-related staff from collegiate and departmental life, divisions between academic faculty and administrative, professional and other support staff, and the intersectionality of gender, race/ethnicity, sexual orientation/gender identity, and socio-economic class. A more supportive and inclusive culture is likely to benefit all faculty and staff, increase career satisfaction, and reduce faculty and staff attrition.
Although we cannot claim causality, we attribute a more positive culture in medical sciences largely to the wide-spread implementation of Athena SWAN gender equality action plans linked to the NIHR funding incentives. Given the spread and adoption of Athena SWAN globally, including its linkage to funding incentives by three funding bodies in Ireland (Science Foundation Ireland), our results provide evidence and a degree of encouragement to other academic and research institutions in the UK, Ireland, and globally to develop, implement, and evaluate impact of gender equality plans similar to Athena SWAN. The success of UK and Irish funding bodies in introducing funding incentives linked to Athena SWAN could serve as an inspiration to other research funders globally.
Footnotes
Acknowledgements
We would like to thank the survey respondents who generously shared their experiences. We especially thank Adrienne Hopkins, Bríd Cronin, Gillian Morris, Rebecca Surrender, Roger Goodman, Sarah Rowles, Stephen Conway, Tanya Baldwin, and Trudy Coe who supported this work and culture change in Oxford.
Disclosure statement
P. V. O., M. D., and A. M. B. are employed and L. D. E. was formerly employed by the University of Oxford. P. V. O. is a member of the Environment and Culture Working Group of the Radcliffe Department of Medicine, University of Oxford.
Ethics approval and consent to participate
The study received ethics clearance through the Brandeis Committee for Protection of Human Subjects (IRB Protocol #07077Bn), the University of Oxford Medical Sciences Interdivisional Research Ethics Committee (MSD-IDREC-C1-2014-051), and the Department of Social Policy and Intervention Departmental Research Ethics Committee (DREC-2014-15-01). All survey participants provided consent for their responses to be used in presentations and academic research. No personal data were reported, only anonymized data were presented in this research article.
Data availability
Quantitative data and analyses are available on reasonable request from the corresponding author.
{kind=link}