
Abstract
Keywords
Bipolar I disorder is a complex and chronic brain disease associated with increased health-care costs, decreased productivity and functioning, poor quality of life, and an increased risk of suicide. The goals of treating bipolar disorder include symptomatic remission, full return of psychosocial functioning, and prevention of relapses and recurrences [1].
Bipolar disorder has at least four, and possibly six, dimensions or relatively discrete symptom areas, including hyperactivity, impulsivity, depression–anxiety, psychosis, irritability, and grandiosity [2]. The complex nature of bipolar disorder means that clinicians often use combination therapy to effectively control mood symptoms, to reduce relapse, and to facilitate socio-occupational functioning. Post et al. found in a 1-year naturalistic Stanley Foundation Bipolar Network study that patients are treated with 4.1 different medications [3]. Other naturalistic studies have also suggested that although a small subset of patients do well with maintenance monotherapy for bipolar disorder, most patients clearly do not [4].
Hospitalization is often indicated for patients who are considered to pose a serious risk of harming themselves or others [5]. Rehospitalization is an important event for the patient and their family, often indicating a relapse/recurrence of significant affective symptoms, dangerous or violent behaviour, or deteriorated function that has not responded adequately to outpatient treatment [5]. Previous studies have indicated that the 1 year rehospitalization rate for bipolar disorder ranges from 41% to 60% [6, 7]. Although rehospitalization risk is only one of the important dimensions of the outcome of bipolar disorder, and which depends on many factors other than the symptomatic course of the disorder, rehospitalization is an important event indicating that the clinical symptoms of the illness have reached an intolerable level. Rehospitalization has also been regarded as a sign of failure by the patients, the families, and the psychiatrists. Identification of predictors of rehospitalization is therefore critical in maximizing prevention and optimizing treatment strategies. If these predictors can be recognized early and adequately, their contribution to rehospitalization would diminish. The purpose of the study was therefore to examine the risk factors affecting the time to rehospitalization for Chinese patients with bipolar I disorder in Taiwan.
Methods
This study was conducted at Kai-Suan Psychiatric Hospital, a major psychiatric centre in Taiwan, under naturalistic conditions. The study was approved by the Institutional Review Board and conducted in accordance with the Helsinki Declaration.
Subjects
All inpatients with DSM-IV [8] bipolar I disorder discharged between 1 January 2002 and 31 December 2004 were screened for eligibility. The diagnosis for bipolar disorder was validated by trained psychiatrists using the Mini International Neuropsychiatric Interview [9]. The patients’ clinical status was also monitored using the Clinical Global Impressions–Severity (CGI-S) at least once a week until discharge. Patients who were discharged against medical advice [10] or transferred to another inpatient facility due to physical problems were excluded from the study.
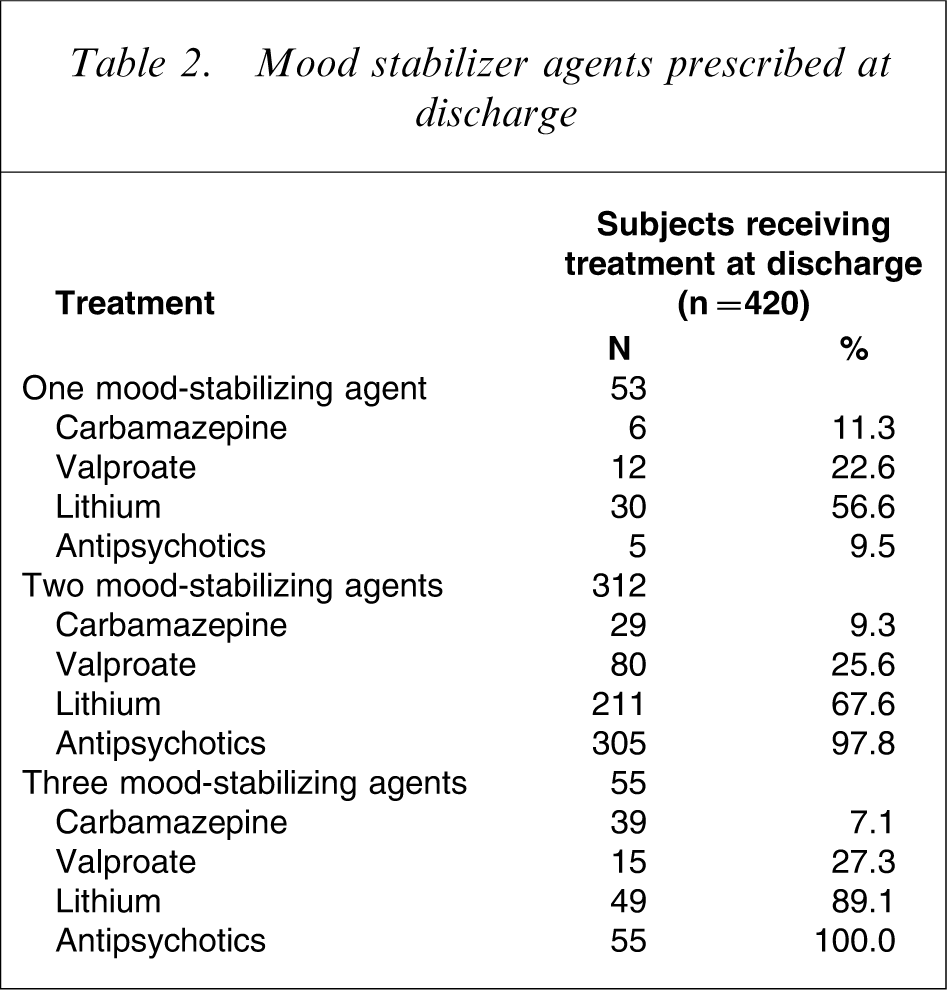
A mood-stabilizing agent is so defined if it is efficacious in the treatment of acute affective symptoms, does not exacerbate manic or mixed symptoms, or has a prophylactic effect on affective symptoms in bipolar disorder [5, 11]. According to this definition, lithium, valproate, carbamazepine, and antipsychotics (typical or atypical) were considered mood-stabilizing agents in the present study. The number of mood-stabilizing agents prescribed at discharge from index hospitalization was categorized as: one mood-stabilizing agent, two mood-stabilizing agents, or three mood-stabilizing agents.
Subjects consisted of those patients who were discharged with CCI-S scores of 1 (very much improved) or 2 (much improved), while receiving one mood-stabilizing agent (n = 53), two mood-stabilizing agents (n = 312) or three mood-stabilizing agents (n = 55).
Follow-up procedures
All subjects were followed up regularly (usually weekly, biweekly, or monthly, depending on clinical conditions) in the Outpatient Department. Lamotrigine (Lamictal; GlaxoSmith-Kline, London, UK) has been available at Kai-Suan Psychiatric Hospital since November 2006. Also, most recommendations regarding the duration of antidepressant treatment in patients with bipolar disorder suggest prompt discontinuation of antidepressants after remission of depression to avoid precipitating manic and hypomanic episodes [12–14]. Antidepressants and lamotrigine were not prescribed for any patients during the follow-up period. No special care or therapy other than routine education and counselling was provided. Subject rehospitalization status was examined within 1 year after discharge, until 31 December 2005.
Statistical analysis
Time to rehospitalization was regarded as the long-term outcome measure [15]. Other factors affecting the likelihood of rehospitalization included gender, family history of first-, second-, or third-degree blood relatives with affective illness, comorbid alcohol abuse and dependence [16, 17], psychotic features, delusions or hallucinations, at index hospitalization [18, 19], episodes (depressive or manic) at index hospitalization [20], age, the number of mood-stabilizing agents prescribed (one, two or three), age at onset of first major affective episode [21, 22], duration of index hospitalization [23], and number of previous hospitalizations [24, 25].
The Kaplan–Meier method was used to calculate the time to rehospitalization and time to loss of follow up within 1 year after discharge. The univariate Cox proportional hazards regression model was used to investigate potential factors that might have increased risk of rehospitalization. Significant factors in univariate analysis were entered into the forward multivariate Cox proportional hazards regression model to identify risk factors. All tests were two-tailed, and significance was defined as an alpha of less than 0.05. Data were analysed with SPSS version 10.0 for Windows (SPSS, Chicago, IL, USA).
Results
Of a total of 518 patients with bipolar I disorder discharged between 1 January 2002 and 31 December 2004, 420 patients (81.1%) were recruited for this study. The mean time to rehospitalization within 1 year after discharge was 231 days (SD = 7), with 211 patients (50.2%) readmitted. The mean time to loss of follow up within 1 year after discharge was 324 days (SD = 5), and the dropout rate was 11.9% (50/420).
Possible predictors and hazard ratio on univariate Cox proportional hazards regression
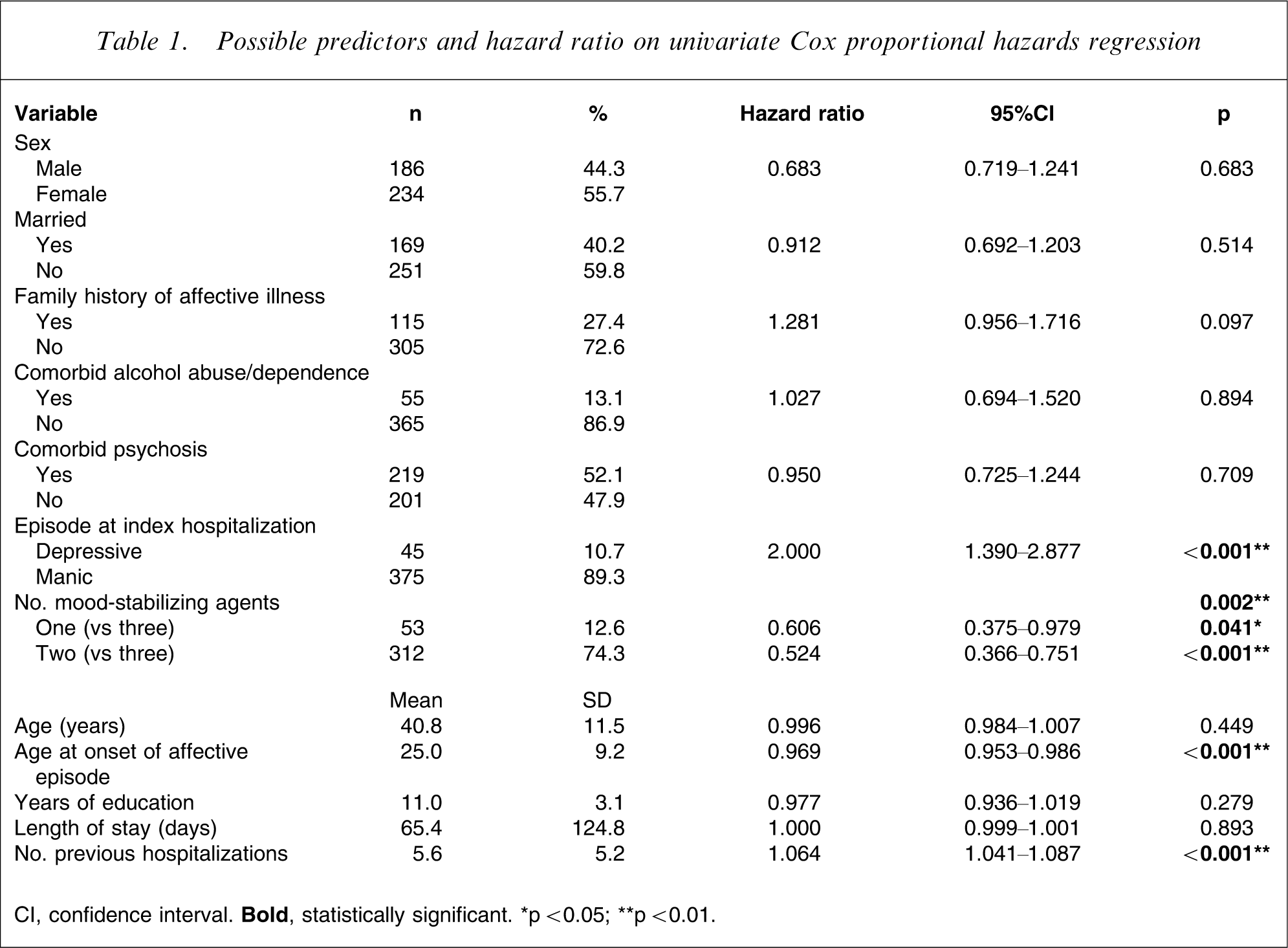
CI, confidence interval.
Fifty-three patients (12.6%) received one mood-stabilizing agent, 312 (74.3%) receive two mood-stabilizing agents, and 55 (13.1%) received three mood-stabilizing agents. Mood stabilizer agents prescribed at discharge are listed in Table 2. Figure 1 presents the time to rehospitalization for bipolar I disorder patients versus number of mood-stabilizing agents as determined on the Kaplan–Meier method. The three mood-stabilizing agents group was significantly associated with a shorter time to rehospitalization and a higher rehospitalization rate (χ2=11.10, df = 2, p < 0.01) than the other groups.
Time to rehospitalization for bipolar I disorder patients taking (—) one mood-stabilizing agent (n = 53, mean time±SD = 235±18 days), (—) two mood-stabilizing agents (n = 312, mean time±SD = 242±8 days), or (—) three mood-stabilizing agents (n = 55, mean time±SD = 169±19 days; log rank = 12.88, df = 2, p < 0.01).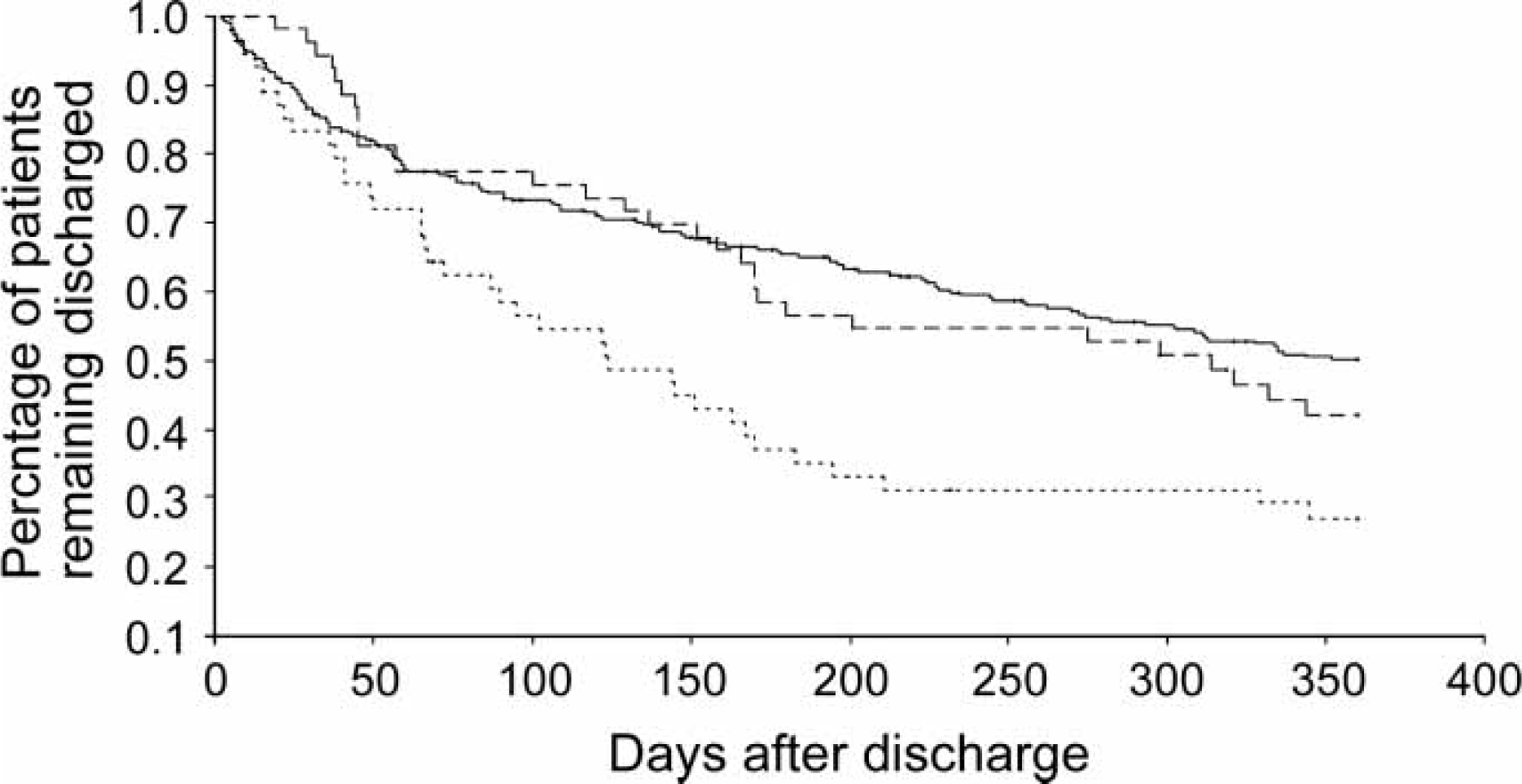
Mood stabilizer agents prescribed at discharge
Factors affecting time to rehospitalization on forward multivariate Cox proportional hazards regression model within 1 year after discharge
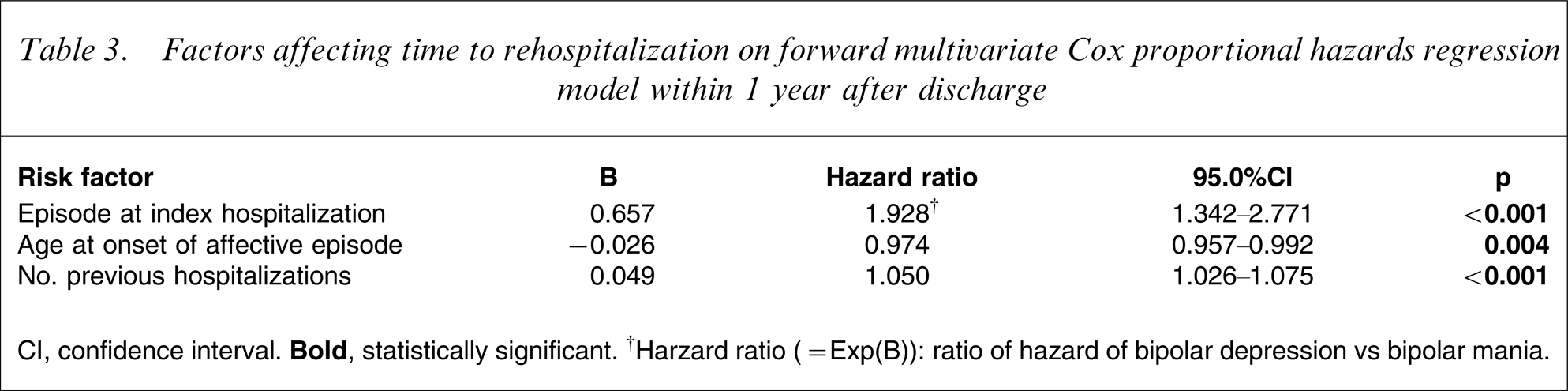
CI, confidence interval.
Discussion
As determined by the mean time to rehospitalization (231±9 days) and the rehospitalization rate (50.2%) for all patients, it has been suggested that rehospitalization is common among bipolar patients [6, 7, 26]. Patients with depressive episodes at index admission, a younger age at onset, or a greater number of previous hospitalizations are more likely to be readmitted.
In the present study patients diagnosed with bipolar depression (n = 45) at index hospitalization were significantly associated with a shorter time to rehospitalization (Table 1) and a higher rehospitalization rate (77.5% vs 46.9%, p < 0.01) than those with bipolar mania. In addition, 26 of 45 (57.8%) were readmitted due to depressive episodes, and nine of 45 (20%) were readmitted due to bipolar mania during 1 year follow up after discharge (data not shown). One possibility may be that depressive episodes are more likely to re-occur than manic episodes [20, 27, 28]. American Psychiatric Association guidelines state that following remission of a depressive episode, patients may remain at particularly high risk of relapse for a period [5].
In the present study patients with a younger age at illness onset or more frequent previous hospitalizations were more likely to be readmitted, supporting the notion that early onset bipolar disorder is associated with greater severity, sociopathy, a more chronic course, increased frequency of mood switches, resistance to medications and overall poorer outcomes elsewhere [29–32], and that more prior hospitalizations raise the risk of rehospitalization [33]. It has been confirmed that patients who frequently seek psychiatric services manifest a range of recurring and severe psychopathologies that are difficult to treat, leaving these individuals vulnerable to further exacerbations [34, 35].
Patients in the group receiving three mood-stabilizing agents had the shorter time to rehospitalization and a higher rehospitalization rate than patients receiving one or two mood-stabilizing agents, although this patient group did not remain significant after further analysis using the forward multivariate Cox proportional hazards regression model. Patients in the group receiving three mood-stabilizing agents also had an earlier age at onset of affective episode (p < 0.01) and a higher number of previous hospitalizations (p < 0.01) than other groups. One possible explanation is that this patient group may have a greater severity of illness and treatment difficulty, are more susceptible to relapse, and required more complex medications with different mechanisms of action to enhance efficacy [30]. The present findings are consistent with the results from the first year of the Systematic Treatment Enhancement Program for Bipolar Disorder study by Martinez et al., in that a greater number of medications is predictive of poor outcomes [28].
It is also important to note the negative findings, because the variables were selected based on their predictive utility in other studies. First, studies from Western countries have demonstrated that higher rates of alcohol abuse/dependence exist among patients with bipolar disorder. The Epidemiologic Catchment Area study found that approximately 46% of patients with bipolar disorder may meet the diagnostic criteria for alcohol abuse/dependence [36]. Comorbid alcohol use is typically associated with fewer and slower remissions, greater rates of suicide and suicide attempts, and poor outcome [37–39]. When compared to studies from Western countries, the relationship between comorbid alcohol abuse/dependence and rehospitalization was not significant in the present study. Some studies have stated that the rate of alcohol abuse/dependence among Chinese people has been much lower than that reported in Western countries [40–42]. One of the main reasons may be due to the marked sensitivity to alcohol and associated with high levels of acetaldehyde, during alcohol metabolism, which is suggested to be the biological protective factor [42, 43]. Other studies have demonstrated that Chinese patients with bipolar disorders have a lower comorbidity of alcohol abuse/dependence [44, 45]. This may be explained by the fact that the rate of comorbid alcohol abuse/dependence of Chinese patients with bipolar disorder appears to be lower than that of Western bipolar disorder patients. In short, relatively lower rates of alcohol abuse/dependence (13.1%) were found among the present subjects, and this may be a possible reason why alcohol abuse/dependence failed to predict time to rehospitalization. Second, there was no significant difference in time to rehospitalization between those patients with comorbid psychosis and those without. One possible interpretation is that physicians are more likely to use an antipsychotic for bipolar patients with psychosis to achieve symptom reduction and patient stabilization. The present result is consistent with that reported by Patel et al. [46].
The limitations of the present study are similar to those of previous investigations on rehospitalization of psychiatric patients [46–48]. First, the patients were not randomly assigned to the treatment groups. Second, due to patient recall bias, we could not address other potential confounding factors such as number of previous episodes [49–51], treatment adherence [52], adverse life events [53], and level of social support [54] or expressed emotion [55]. Third, continuation of the medication regimen on which the patient was discharged could not be confirmed. A large prospective naturalistic study, however, has found that most agents used in the acute phases of bipolar disorder are similarly used in the maintenance phase of treatment [56]. Fourth, although bipolar depression tends to occur more frequently than bipolar mania, most of the patients with bipolar depression receive the outpatient treatment. Like the major depressive disorder, a low percentage of patients with bipolar depression require hospitalization for their depressive illness [57]. This is the main reason that the vast majority of subjects were manic at index episode (375 vs 45) in the present study. This limits the emphasis placed on the differential importance of mood state upon admission.
Finally, the present study had a relatively small sample size, and all of the subjects were from a single treatment unit. Therefore the results may not be generalizable to other settings. Further studies in this field should test risk factors in a prospective study and be conducted in various mental health systems.
Footnotes
Acknowledgements
This study was supported by funding from the Kai-Suan Psychiatry Hospital in 2006.